
Abstract
Background
Adherence to lifestyle and dietary modifications is crucial for effective hypertension management, yet non-adherence remains a significant challenge.
Aim
This study aimed to identify determinants and perceived barriers of low lifestyle and dietary adherence among adults with hypertension attending chronic care units in Butha-Buthe and Mokhotlong districts, Lesotho.
Methods
A quantitative cross-sectional survey of 200 adults with hypertension attending chronic care units in the Butha-Buthe and Mokhotlong districts of Lesotho was conducted. Logistic and linear regression were used to identify determinants of dietary and lifestyle adherence, respectively, with statistical significance set at p < 0.05.
Summary
The mean age of participants was (48 ± 11.87 years). Only 8.0% of participants adhered to WHO dietary recommendations, while 36.5% adhered to lifestyle recommendations. Patients with low education were substantially less likely to adhere to dietary guidelines (OR = 0.18, 95% CI: 0.03–0.82, p < 0.05), and those reporting specific food preferences were likewise less likely to adhere (OR = 0.18, 95% CI: 0.03–0.88, p < 0.05). Low educational level was also a significant predictor of lifestyle adherence (β = −0.275, p < 0.05), as were food preferences (β = −0.205, p < 0.05). These findings highlight the need for patient education, nutritionist support, and context-appropriate dietary counseling to improve hypertension management in resource-limited settings.
Keywords
Introduction
Hypertension has become a significant public health issue, affecting approximately 1.4 billion adults aged 30–79 years globally (World Health Organization (WHO), 2025). It is a key risk factor for coronary artery diseases, heart failure, and cerebrovascular disease (Ayalew et al., 2023). It ranks as a major cause of premature death worldwide (Xia et al., 2022). In low- and middle-income countries, the burden is particularly high, driven by rapid urbanization, changing diets, and constrained health systems (Song et al., 2021; WHO, 2023, 2025). Lesotho faces a growing hypertension burden, with recent data showing high prevalence and concerning levels of uncontrolled blood pressure, especially among adults in rural and semi-urban districts (Lebuso and De Wet- Billings, 2022; Ogola et al., 2019).
Effective management of hypertension requires not only pharmacological treatment but also sustained adherence to lifestyle and dietary modifications. These include the Dietary Approaches to Stop Hypertension (DASH) diet, sodium reduction, weight control, regular physical activity, and the avoidance of tobacco and harmful alcohol consumption (Ingenhoff et al., 2022; Israfil and Rumambo Pandin, 2021; WHO, 2023). Collectively, these strategies have been demonstrated to lower blood pressure, improve the efficacy of antihypertensive medications, and decrease cardiovascular risk (Geremew et al., 2023). The DASH diet specifically emphasizes fruits, vegetables, whole grains, legumes, nuts, and low-fat dairy while restricting sodium, saturated fat, red and processed meats, and added sugars, creating a nutrient pattern that supports vascular health and lowers cardiovascular risk (Onwuzo et al., 2023). DASH improves endothelial function and promotes natriuresis, leading to clinically meaningful reductions in systolic and diastolic blood pressure and offering an important complement to pharmacotherapy for patients with hypertension (Lin et al., 2012). All patients with hypertension are recommended to adopt these lifestyle and dietary modifications regardless of whether they are on drug therapy (Beni Yonis, 2025; Charchar et al., 2024).
Despite clear evidence that lifestyle and dietary changes can improve blood pressure control and reduce cardiovascular risk, adherence to these recommendations remains suboptimal in many resource-limited settings (Abaynew and Hussien, 2021). Socioeconomic constraints, limited access to health information, and inadequately staffed primary care services often hinder patients’ ability to adopt and sustain recommended behaviors (Ijioma et al., 2023; Kebede et al., 2022; Kim et al., 2022). Recent population-based studies indicate a substantial burden of hypertension in Lesotho. In two districts with characteristics similar to those examined in the present study, hypertension prevalence has been estimated at approximately 25% in urban areas and 17% in rural areas, highlighting the growing need for effective hypertension management strategies in both settings (González Fernández et al., 2024). Despite this growing burden, limited research has examined the behavioral and structural factors that influence patients’ adherence to recommended dietary and lifestyle modifications in rural and semi-urban districts. Most existing studies in Lesotho have focused on hypertension prevalence, treatment coverage, and control gaps, with far less attention to the everyday barriers patients face in adjusting their diet and lifestyle (Fernández et al., 2024; Selebalo et al., 2024; Tikhute and Chattaraj, 2025). The lack of behavioral and contextual insight constrains the design of targeted interventions and policies to improve long-term hypertension outcomes in resource-limited primary care settings like Lesotho. To better understand why patients do or do not adhere to recommended behaviors, this study draws on the Capability, Opportunity, Motivation–Behavior (COM-B) model as a guiding framework (Michie et al., 2011). The COM-B model posits that health behaviors arise from the interaction of individuals’ capabilities, such as knowledge and skills; opportunities, including financial resources, social support, and access to health professionals; and motivation, such as beliefs, preferences, and stress. Guided by the COM-B model, this study aimed to assess the determinants and perceived barriers to low adherence to lifestyle and dietary recommendations among adults with hypertension attending chronic care units in the Butha-Buthe and Mokhotlong districts of Lesotho.
Methods
Study design and setting
This study employed a quantitative, descriptive, cross-sectional survey conducted across three healthcare facilities in the Butha-Buthe and Mokhotlong districts from 27 February to 27 March 2024. The selected healthcare facilities were Butha-Buthe Government Hospital, Seboche Mission Hospital, and Mokhotlong Government Hospital, the only public secondary-level hospitals in the two districts. Butha-Buthe Government Hospital and Mokhotlong Government Hospital are centrally located within their respective town centers, while Seboche Mission Hospital is situated approximately 23.6 kilometers from Butha-Buthe town. This multi-center approach was designed to capture a comprehensive representation of hypertensive patients in both urban and semi-rural settings, thereby enhancing the generalizability of the study findings to the broader populations in these districts.
Participants and eligibility criteria
The study population comprised participants with hypertension who were receiving treatment at hospitals in the Butha-Buthe and Mokhotlong districts. Only patients who had been diagnosed with hypertension for over 6 months, were 18 years of age or older, and gave written consent to participate were included in the study. Exclusion criteria encompassed patients who were hospitalized at the time of data collection, pregnant women, or those who had given birth within 6 months before data collection, and patients who were critically ill or had mental health conditions that precluded participation. Participant recruitment was conducted in collaboration with routine staff at the study facilities. Eligible patients receiving hypertension treatment at these facilities were invited to participate. The recruitment process involved providing comprehensive information about the study, explaining the purpose and procedures, and obtaining informed consent. Eligible patients who declined to participate were replaced with subsequent consenting participants until we achieved the required sample size.
Sampling method
This study utilized a multi-stage, non-probability sampling approach to recruit participants, tailored to the practical constraints and context of the research setting. Two districts—Butha-Buthe and Mokhotlong—were purposively selected based on their high prevalence of hypertension, as indicated by a recent study (González Fernández et al., 2024). In each district, hospitals with substantial hypertensive patient populations were chosen to maximize the likelihood of enrolling eligible participants. Within the selected hospitals, convenience sampling was employed. Eligible participants were approached during routine outpatient days. The use of convenience sampling is acknowledged as a limitation regarding representativeness, but it enabled efficient data collection in a real-world clinical context.
Sample size
The sample size was determined using Yamane's finite population correction formula for a known population size:
Operational definitions
Hypertension (HTN)
Hypertension was defined as a prior clinical diagnosis of high blood pressure recorded in the patient's medical file, consistent with World Health Organization criteria of systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg on at least two different days, or current use of antihypertensive medication for blood pressure control (WHO, 2025).
Blood pressure (BP)
Blood pressure is defined as the pressure of circulating blood against the walls of the arteries, measured in millimeters of mercury (mmHg) as two values: systolic and diastolic (Asayama et al., 2021). For this study, blood pressure was defined as standardized clinic measurements documented in participants’ medical records at the chronic care units.
Blood pressure control status
Blood pressure control status was defined as a binary variable indicating whether a participant's average clinic blood pressure was below or above the treatment target.
Controlled blood pressure
Controlled blood pressure was defined as the most recent clinic measurement <140/90 mmHg, in line with WHO and international guidelines for hypertension control in adults (WHO, 2025).
Uncontrolled blood pressure
Uncontrolled blood pressure was defined as the most recent clinic blood pressure measurement≥140/90 mmHg among participants with a prior diagnosis of hypertension (WHO, 2025).
Lifestyle modification
Lifestyle modification refers to non-pharmacological behaviors recommended for hypertension management, including engaging in regular physical activity, maintaining a healthy body weight, limiting dietary sodium intake, abstaining from tobacco, and avoiding harmful alcohol use, as recommended by the WHO and other hypertension guidelines (Kaplan, 2004; WHO, 2025).
Lifestyle adherence
Lifestyle adherence was operationalized as self-reported engagement in all six WHO-recommended lifestyle behaviors adopted in the questionnaire (regular physical activity of at least 30 min per day on most days of the week, weight-control behaviors, avoidance of smoking, avoidance of harmful alcohol use, reduced dietary salt intake, and consumption of a generally healthy diet for hypertension) (WHO, 2025). Participants who reported engaging in all six behaviors were classified as adherent to lifestyle modification; those who missed one or more behaviors and had a total score of <6 points were classified as nonadherent.
Dietary modification (DASH-style diet)
Dietary modification refers to the adoption of a DASH–style eating pattern characterized by high intake of fruits and vegetables, whole grains, and low-fat dairy products, with limited intake of saturated fat, red and processed meats, and added sodium, as recommended for hypertension control (Onwuzo et al., 2023).
Dietary adherence
Dietary adherence was defined as self-reported engagement in all five WHO-recommended dietary modifications adapted for this study (increased consumption of fruits and vegetables, reduced intake of processed foods, reduced intake of fatty foods, reduced intake of fatty dairy products, and reduced use of added/raw salt), measured using five modified items from WHO dietary guidance. Participants who reported engaging in all five dietary practices were categorized as adherent to dietary recommendations; all others with a total score of < 5 points were categorized as non-adherent.
Harmful alcohol use
Harmful alcohol use was defined as a self-reported history of drinking more than 7 standard drinks per week in the past 6 months (Musto et al., 2025; Paradis et al., 2023).
Perceived barriers to adherence
Perceived barriers were defined as self-reported factors that participants believed made it difficult to adhere to recommended lifestyle and dietary practices, including limited knowledge, financial constraints, limited access to health facilities, absence of a nutritionist, low education, food preferences, food intolerances, lack of social support, and stress.
Financial constraints
Financial constraints were defined as self-reported difficulty affording recommended foods or activities for hypertension management, consistent with literature identifying cost as a major barrier to DASH-style diets and lifestyle modification in low-resource settings (Tyson et al., 2023).
Limited knowledge
Limited knowledge was defined as self-reported inadequate understanding of hypertension, its complications, and recommended dietary and lifestyle changes, consistent with studies linking health literacy to adherence behaviors (Geremew et al., 2023).
Low educational level
Low educational level was defined as having no formal education or only primary education, as reported in the sociodemographic section.
Educational level
Educational level was defined as the self-reported, fully categorical distribution of participants’ schooling, as reported in the sociodemographic section.
Social support
Social support was defined as self-reported emotional, informational, or practical support from family members, friends, or community networks that could facilitate adherence to dietary and lifestyle recommendations.
Food preferences
Food preferences were defined as strong likes or dislikes for specific foods or preparation methods that influenced participants’ willingness to follow recommended diets, consistent with literature emphasizing cultural and taste preferences as determinants of dietary adherence (Jayasinghe et al., 2025).
Food intolerances
Food intolerances were defined as self-reported adverse reactions to specific foods, such as gastrointestinal discomfort, that limited the ability to consume recommended items.
Stress
Stress was defined as self-reported psychological distress related to life circumstances, illness, or treatment, recognized as a barrier that can trigger unhealthy eating and reduce adherence to lifestyle recommendations.
Absence of a nutritionist
The absence of a nutritionist was defined as the lack of an on-site nutrition professional at the health facility providing chronic care, as perceived by participants, which limited access to individualized dietary counseling.
Comorbidity
Comorbidity was defined as the presence of at least one additional chronic condition, such as diabetes or cardiovascular disease, documented in the patient's record or reported by the participant (Geremew et al., 2023).
Duration of hypertension
Duration of hypertension was defined as the time since the first clinical diagnosis of hypertension, categorized as less than 5 years or 5 years or more, as recorded in medical files or self-reported by participants.
Instruments and procedures
Data were collected using a structured, interviewer-administered questionnaire developed in English and guided by World Health Organization recommendations for hypertension management and lifestyle modification (WHO, 2025). The tool comprised five sections: sociodemographic characteristics, clinical characteristics, adherence to recommended diet, adherence to lifestyle modifications, and perceived barriers to adherence. Items assessing dietary and lifestyle practices were adapted from WHO-recommended dietary and lifestyle guidance and from previous studies (Geremew et al., 2023; WHO, 2025) and were anchored on behaviors during the preceding 6 months.
On clinic days, trained research assistants worked alongside routine clinic staff to identify potentially eligible patients from medical booklets. After verification of eligibility and a brief explanation of the study aims and procedures, interested patients were invited to a private area within the clinic, where written informed consent was obtained. Each consenting participant was then assigned a unique code, and their most recent clinic blood pressure reading and clinical details, such as duration of hypertension, comorbidities, and number of antihypertensive medications, were recorded in the questionnaire from the medical record.
The questionnaire was administered face-to-face in the local language (Sesotho) by trained interviewers, who read each item aloud and recorded responses to minimize literacy-related barriers. For dietary adherence, participants were asked about the consumption of processed foods, adding salt at the table, intake of fruits and vegetables, intake of high-fat foods, and full-fat dairy products, and an overall dietary adherence status (yes/no) was coded according to pre-specified criteria. Lifestyle adherence items covered engagement in physical activity (meeting the recommended duration of at least 30 min on most days), smoking history, current smoking, attempts to quit, and heavy alcohol use, followed by an overall lifestyle adherence classification.
Perceived barriers were captured using a checklist of potential reasons for non-adherence, including financial constraints, limited access to health facilities, low education, limited knowledge, lack of social support, cultural or religious beliefs, food preferences, food intolerances, stress, and lack of access to a nutritionist. Data were collected using a structured, pre-tested questionnaire administered via face-to-face survey interviews.
Guided by the COM-B model, the survey was designed to capture key constructs related to patients’ capability, opportunity, and motivation regarding lifestyle and dietary adherence behaviors. Before the main study, the instrument was reviewed by nutrition and health experts for content validity and piloted with a small group of 10 hypertensive patients in a different hospital to assess clarity and reliability; feedback from this pilot informed minor revisions to the questionnaire.
Quality assurance and data management
All researchers underwent comprehensive training on study protocols, data collection techniques, and ethical considerations. The principal investigator reviewed completed questionnaires for completeness and accuracy. Double data entry was employed to minimize errors, and all identifiable information was anonymized to protect participant confidentiality.
Data analysis
The statistical analysis for this study was conducted using the Statistical Package for Social Sciences Version 29.0.2.0. Data were analyzed using descriptive and inferential statistics. Descriptive statistics summarized sociodemographic characteristics, clinical variables, adherence outcomes, and perceived barriers. Frequencies and percentages were calculated for categorical variables, while means and measures of dispersion were computed for continuous variables. Inferential analyses were used to identify factors associated with dietary and lifestyle adherence, with statistical significance set at p < 0.05. Logistic regression was fitted with dietary adherence (adherent vs nonadherent) as the dependent variable, and linear regression was fitted with the lifestyle adherence score as the dependent variable. Potential confounding was considered during model development; however, because of the modest sample size, the very low number of dietary-adherent participants, and limited precision in some self-reported covariates, fully adjusted causal models were not fitted. Including many weakly measured covariates could have produced unstable estimates and overfitting, particularly in the dietary adherence model. The estimates are therefore presented as exploratory associations between measured determinants and adherence outcomes, and residual confounding is explicitly acknowledged as a limitation.
Results
Sociodemographic characteristics of participants
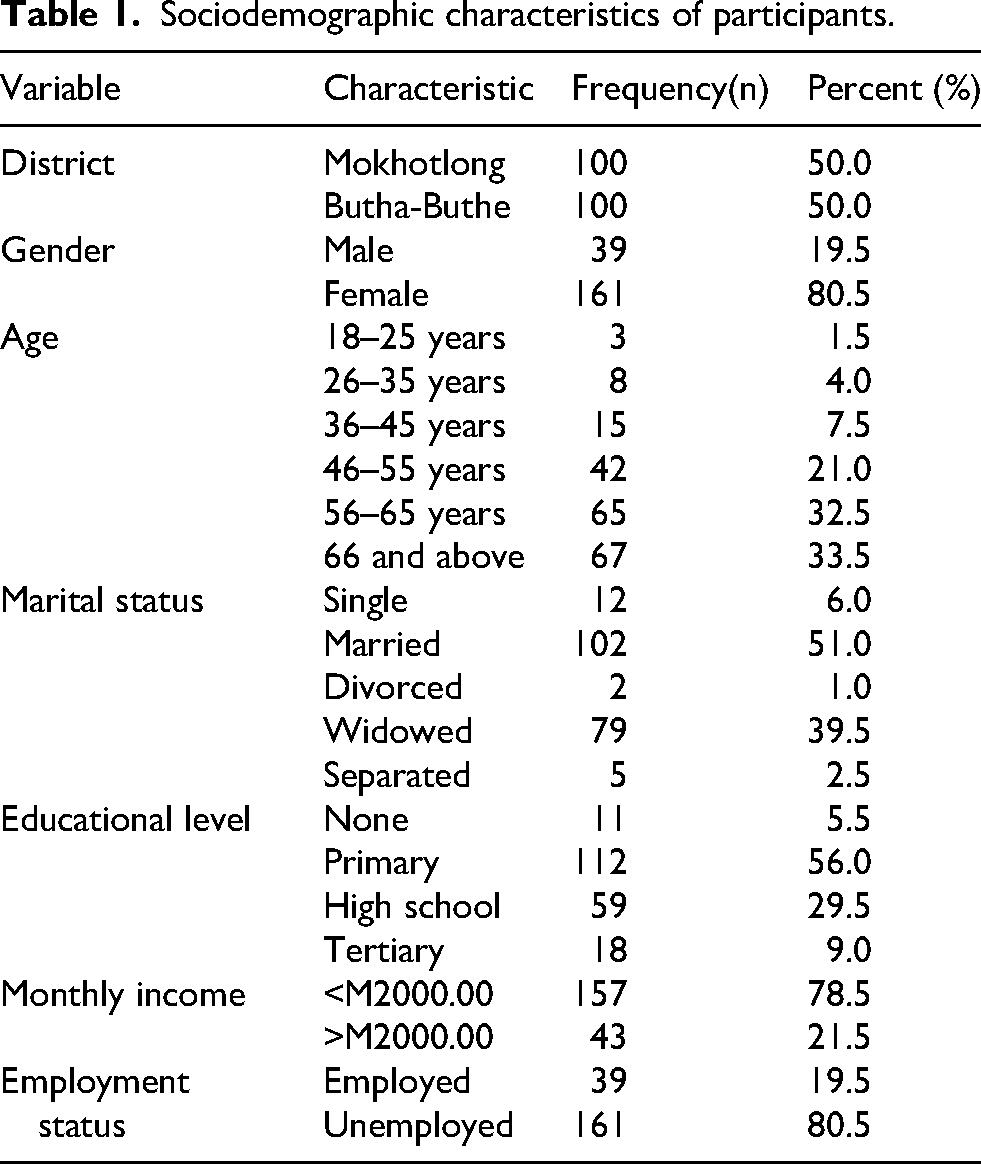
Table 1 presents the sociodemographic characteristics of the 200 participants enrolled from February to March 2024. The participants were evenly distributed between the two districts, with 50% from Mokhotlong and 50% from Butha-Buthe. The majority of participants were female (80.5%), while males accounted for only 19.5%. The mean age of respondents was 48 years (±11.9), with the largest age groups being those aged 66 and above (33.5%) and those aged 56–65 years (32.5%). Younger participants aged 18–25 years constituted only 1.5% of the sample. Most (51.0%) of the respondents were married, 39.5% were widowed, and the remaining (9.5%) were single, divorced, or separated. About half (56.0%) of the respondents had only attained the primary level as their highest academic level. Out of all the respondents, only (9.0%) had attended college or university, while 19.5% of respondents were employed. Also, 78.5% of respondents reported a monthly household income of less than M2000.00 (122 USD).
Sociodemographic characteristics of participants.
Medical history
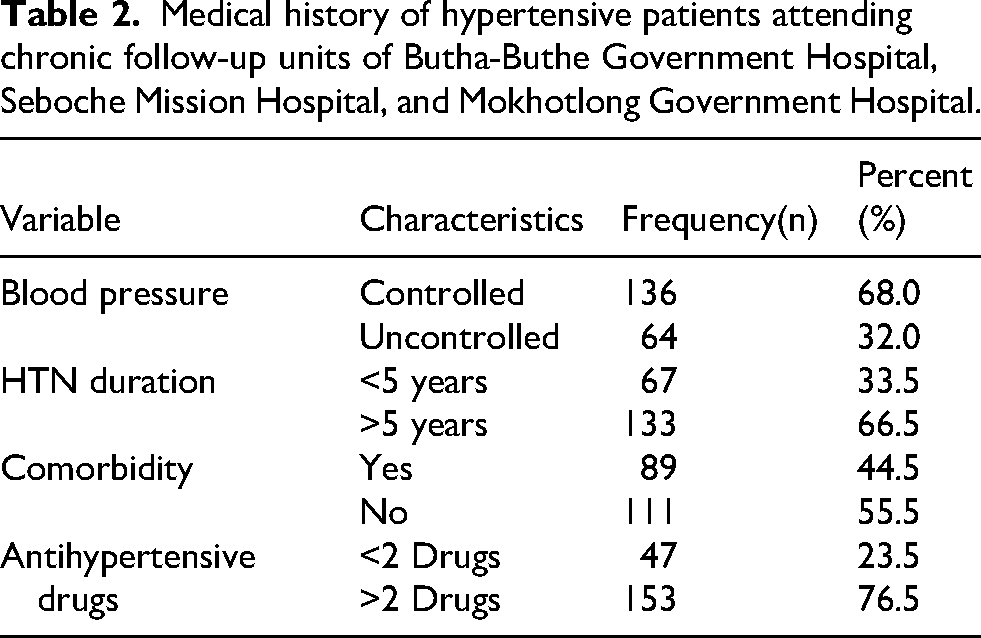
Table 2 presents the medical history and characteristics of the hypertensive patients in the study. Of 200 participants, 64 (32.0%) had uncontrolled high blood pressure (> 140/90 mmHg). Most participants (66.5%) had been hypertensive for more than 5 years and had all been on hypertension treatment for the same period. Most of the respondents (76.5%) were on two drugs per day. Eighty-nine (44.5%) had a comorbidity, meaning they had the presence of at least one additional chronic condition such as diabetes, HIV, or other cardiovascular disease, documented in the patient's record alongside hypertension (Geremew et al., 2023).
Medical history of hypertensive patients attending chronic follow-up units of Butha-Buthe Government Hospital, Seboche Mission Hospital, and Mokhotlong Government Hospital.
Dietary intake
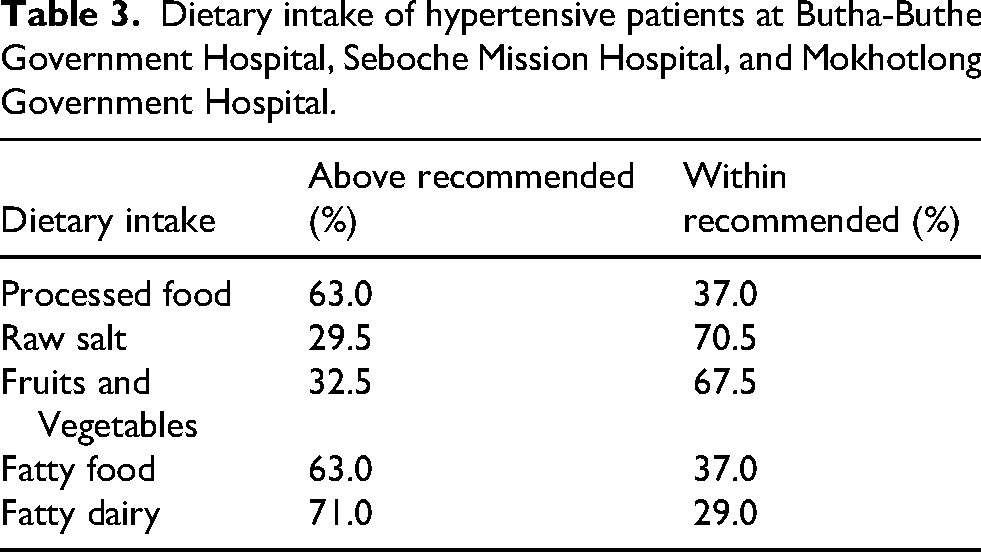
About 70% of the respondents have included fruits and vegetables in their diet since their hypertension diagnosis. Since the diagnosis, participants rarely consumed processed foods (37.0%), high-salt foods (70.5%), fatty foods (37.0%), and fatty dairy products (29.0%) (Table 3).
Dietary intake of hypertensive patients at Butha-Buthe Government Hospital, Seboche Mission Hospital, and Mokhotlong Government Hospital.
Lifestyle factors
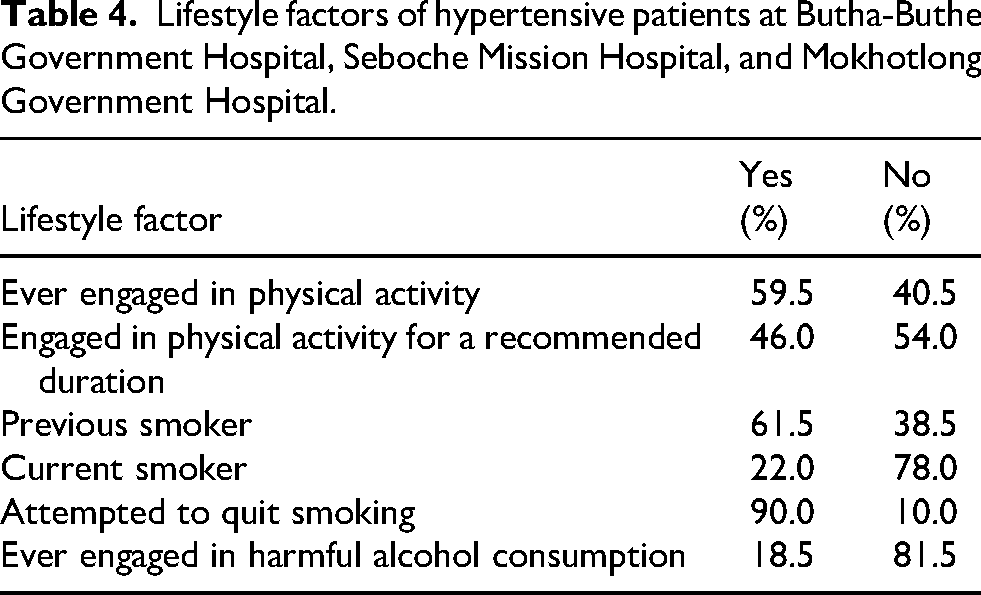
Table 4 shows that most participants reported engaging in some physical activity (59.5%), but less than half (46.0%) met the recommended duration, indicating that many are insufficiently active despite being ever active. A majority had a history of smoking (61.5%), and a small proportion were still current smokers (22.0%), although most of those who had ever smoked reported attempting to quit (90.0%). Harmful alcohol use was less common, with 18.5% having ever engaged in harmful alcohol consumption and 81.5% reporting no history of such drinking behavior.
Lifestyle factors of hypertensive patients at Butha-Buthe Government Hospital, Seboche Mission Hospital, and Mokhotlong Government Hospital.
Dietary adherence
The majority (92.0%) did not adhere to the WHO dietary recommendations, as depicted in Figure 1.
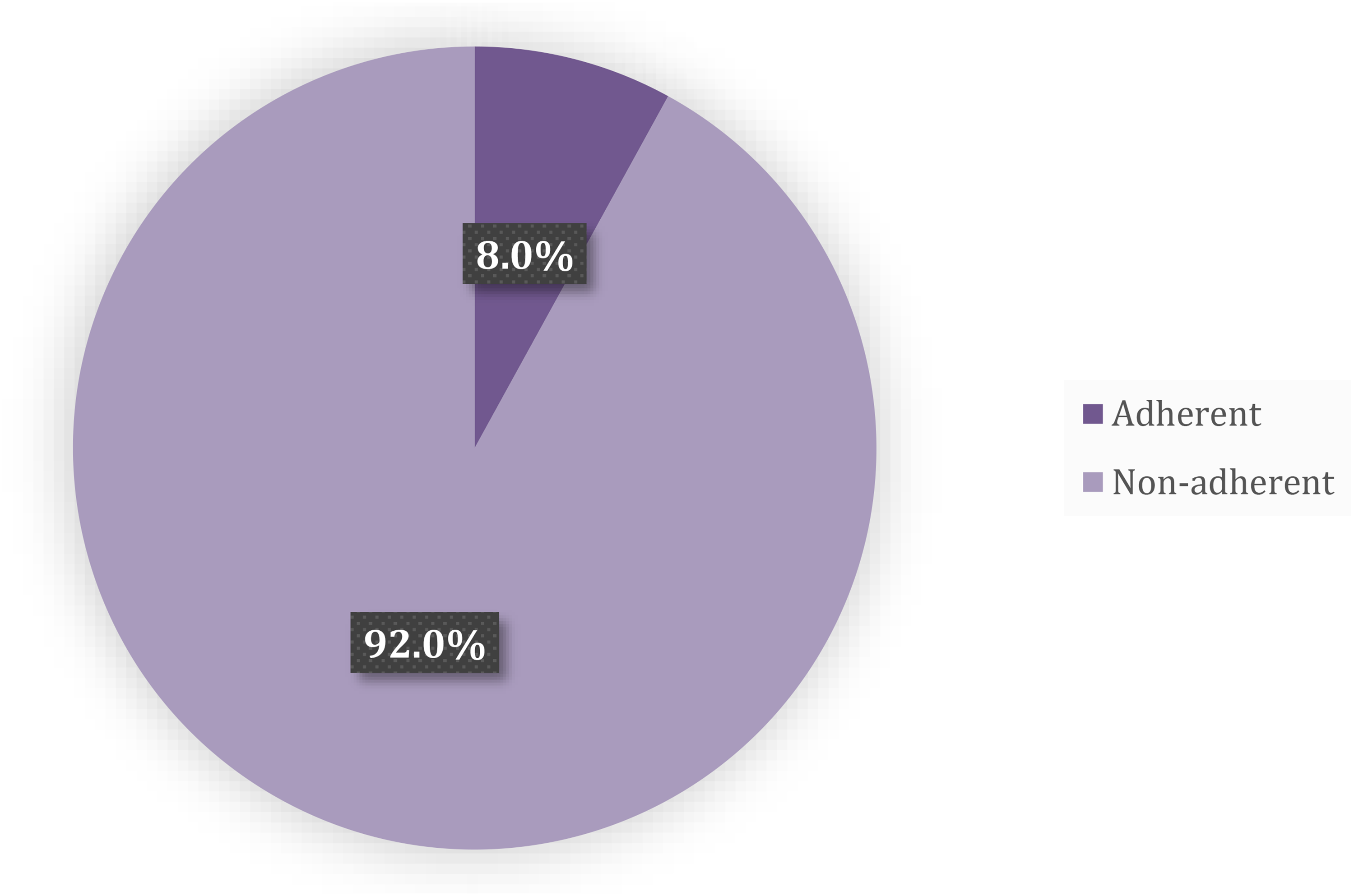
Adherence to dietary recommendations.
Lifestyle adherence
Most participants (63.5%) did not adhere to the lifestyle recommendations, as shown in Figure 2.
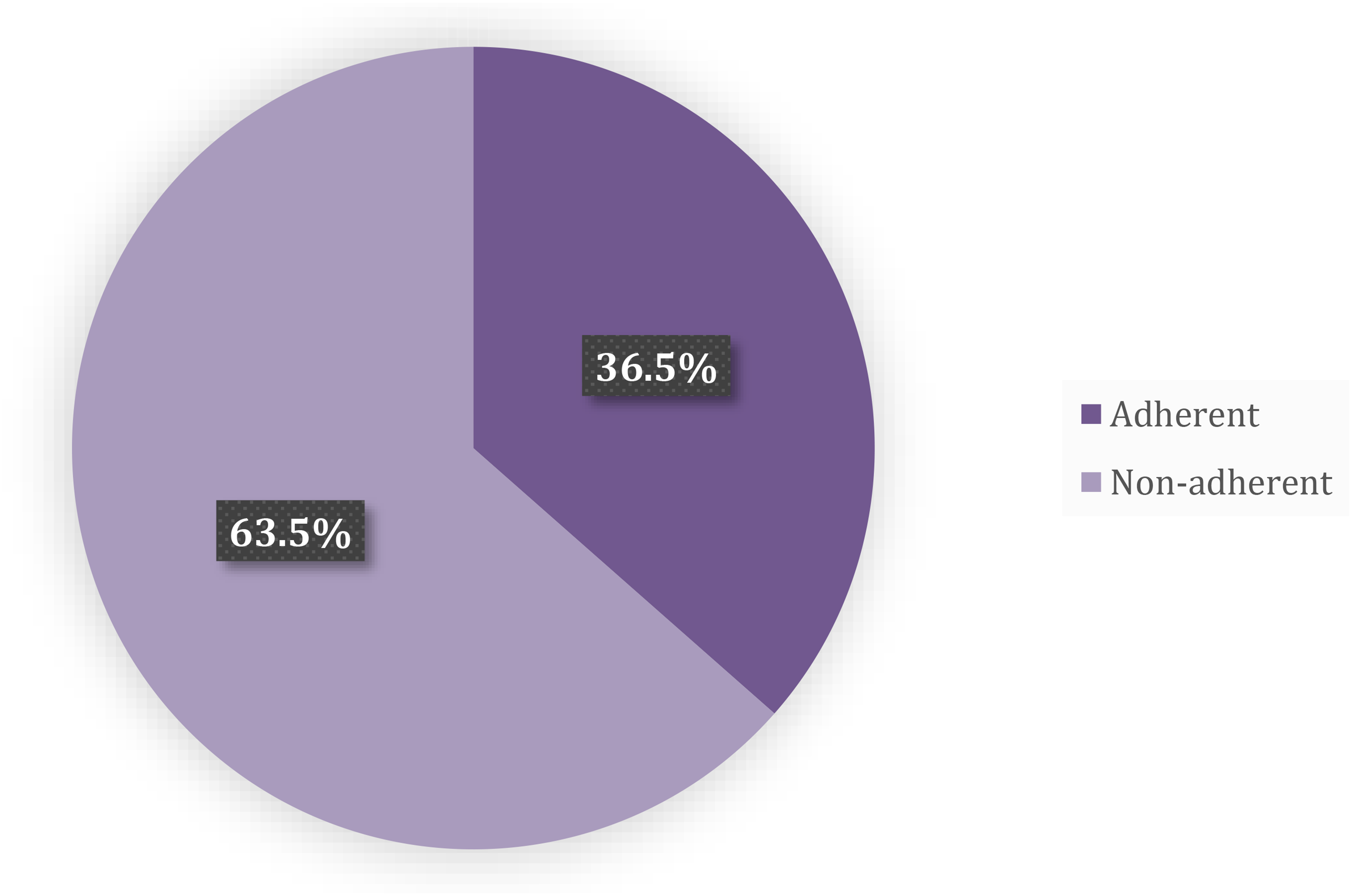
Lifestyle adherence of hypertensive patients at Butha-Buthe Government Hospital, Seboche Mission Hospital, and Mokhotlong Government Hospital.
Perceived barriers to dietary and lifestyle adherence
Most participants identified the absence of a nutritionist in the facility (94%), limited access to health facilities (85%), and financial constraints (80%) as key barriers to adhering to both lifestyle and dietary modifications. Two-thirds (66%) reported that a low educational level hindered their ability to follow recommended dietary and lifestyle changes, and 75% believed that stress negatively affected their adherence. In addition, 71% reported inadequate knowledge about dietary and lifestyle recommendations as a barrier to adherence. Only 3% reported cultural beliefs as a barrier to adherence, as shown in Figure 3.
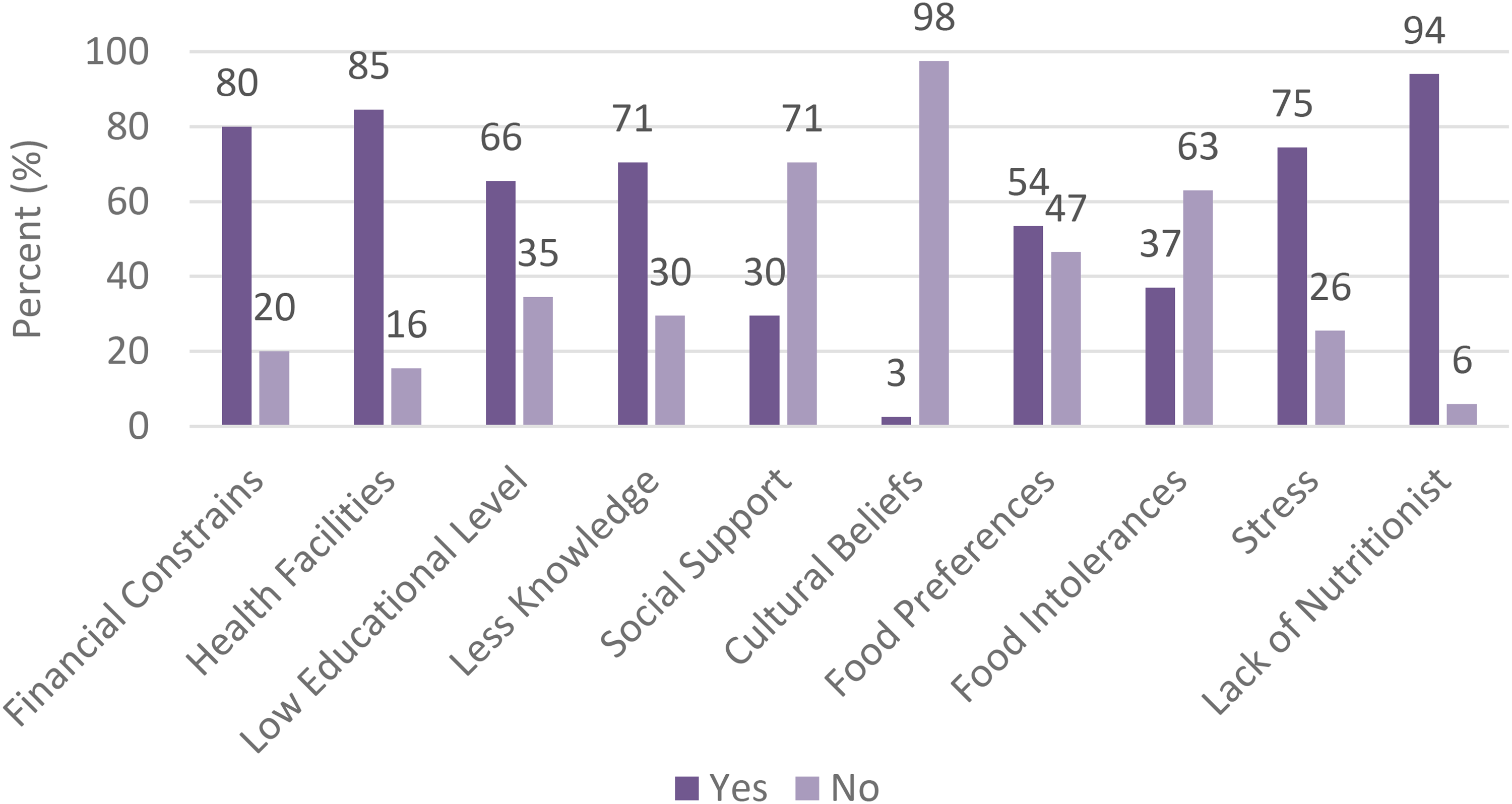
Perceived barriers to dietary and lifestyle adherence.
Factors affecting dietary and lifestyle adherence
The logistic regression analysis of factors affecting dietary adherence among hypertensive patients presented in Table 5 revealed several significant findings. Education level emerged as a crucial determinant, with patients with lower education approximately 82% less likely to adhere to dietary recommendations than those with higher education (OR = 0.18, 95% CI: 0.03–0.82, p = 0.02). Similarly, food preferences significantly affected adherence, with patients with specific preferences about 82% less likely to follow dietary guidelines (OR = 0.18, 95% CI: 0.03–0.88, p = 0.03). Other variables, including age, marital status, blood pressure status, and employment status, did not demonstrate statistically significant associations with dietary adherence.
Logistic regression summary of factors affecting dietary adherence of hypertensive patients at Butha-Buthe Government Hospital, Seboche Mission Hospital, and Mokhotlong Government Hospital.
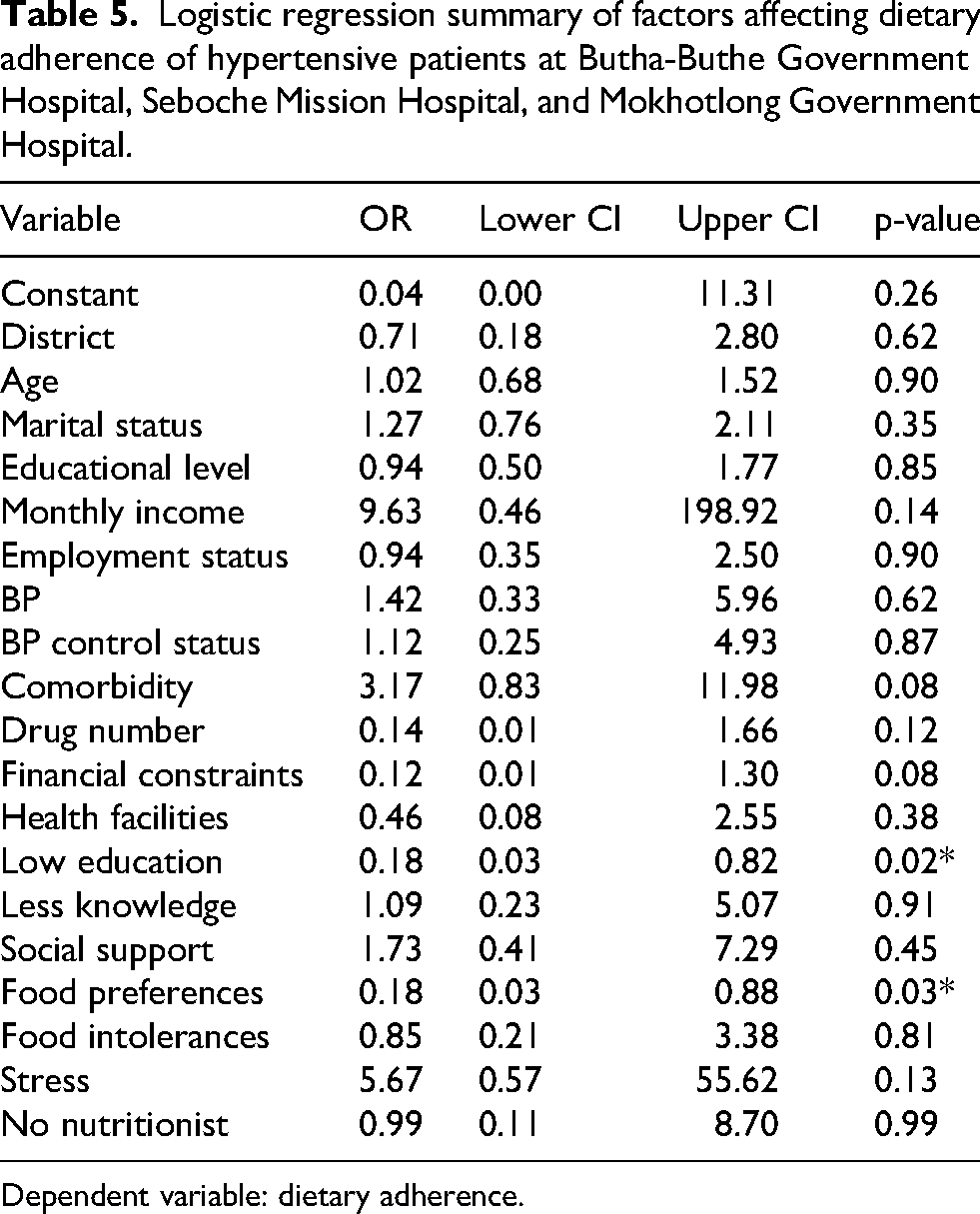
Dependent variable: dietary adherence.
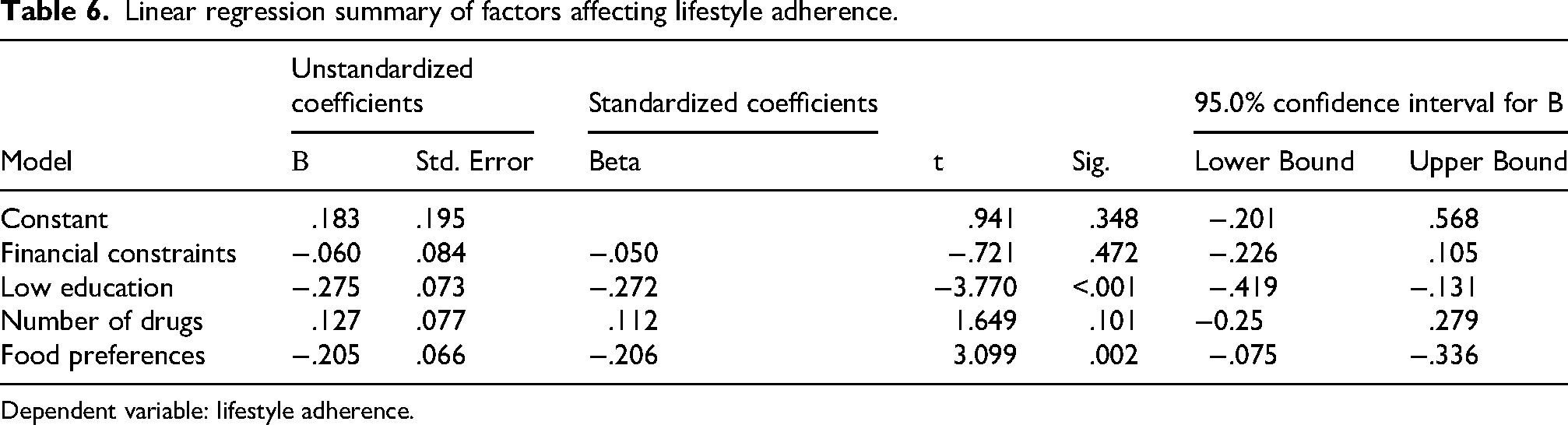
Table 6 presents the results of a linear regression model examining factors influencing lifestyle adherence. Low education was significantly associated with lower lifestyle adherence (β = −0.275, t = −3.770, 95% CI: −0.419 to −0.131, p < 0.001). Food preferences were also significantly associated with lower lifestyle adherence (β = −0.205, t = −3.099, 95% CI: −0.075 to −0.336, p = 0.002).
Linear regression summary of factors affecting lifestyle adherence.
Dependent variable: lifestyle adherence.
Discussion
This cross-sectional survey aimed to assess barriers and factors influencing adherence to lifestyle and dietary recommendations among adults with hypertension in the Butha-Buthe and Mokhotlong districts. Low education and individual food preferences were significant determinants of dietary non-adherence, while low education and food preferences were associated with poorer lifestyle adherence. Because the models were exploratory and not designed to estimate fully adjusted causal effects, these associations should be interpreted as signals of important contextual and behavioral barriers rather than proof of independent causality. Perceived barriers to adherence were highly prevalent, particularly limited knowledge, financial constraints, stress, and limited access to nutritionists in health facilities. Cultural beliefs were reported by only a small minority of participants (3%) and therefore did not emerge as a major determinant of adherence in this study.
Dietary adherence and determinants
The low dietary adherence observed in this study is consistent with reports from other low- and middle-income countries, where patients struggle to follow DASH-style diets due to cost, limited availability of healthy foods, and competing household priorities (Abera et al., 2024; Khan et al., 2014; Ninsiima and Lubogo, 2023; Thinyane et al., 2015). The strong association between low education and non-adherence suggests that limited health literacy and difficulty interpreting dietary advice may hinder effective self-management of hypertension (Olstad and McIntyre, 2025). Educational interventions may therefore significantly improve adherence to the DASH diet (Firdaus Al-Ghifari Atmadja et al., 2025; Geremew et al., 2023; Kim et al., 2022; Tam et al., 2020). The influence of individual food preferences indicates that dietary counseling must go beyond generic recommendations and engage with culturally embedded eating patterns and taste preferences to be effective (Altawili et al., 2023; Faraz et al., 2023; Subramaniam et al., 2022).
The extremely low dietary adherence observed in this study should also be interpreted within the broader socioeconomic context of the study population. Most participants had low educational attainment, limited income, and high unemployment rates, factors strongly associated with reduced access to healthy foods and health information. Rather than reflecting measurement bias, the observed associations between education, food preferences, and adherence likely represent structural barriers faced by patients in rural and peri-urban settings. In resource-limited contexts such as Lesotho, international dietary recommendations, such as the DASH diet, may not fully align with patients’ economic realities, who may rely on inexpensive staple foods that are often high in salt or fat. As a result, adherence challenges may arise not from unwillingness to follow recommendations but from structural constraints related to food availability, affordability, and health literacy.
Lifestyle adherence and determinants
Lifestyle adherence was higher than dietary adherence but remained suboptimal, echoing findings from other African settings, where patients often report engaging in some physical activity but fall short of comprehensive lifestyle recommendations (Ogola et al., 2019; Song et al., 2021; Xia et al., 2022). The association between low education and poor lifestyle adherence underscores the role of educational and socioeconomic disadvantage in shaping daily health behaviors, including exercise and avoidance of harmful alcohol and tobacco use (Firdaus Al-Ghifari Atmadja et al., 2025; Tam et al., 2020). Greater influence of food preferences, such as a tendency towards processed foods, which are often energy-dense and high in sodium, further highlights how environmental and market factors constrain patients’ ability to adopt recommended lifestyle changes. In resource-limited settings, these preferences are frequently shaped by palatability, cost, and satiety, for example, reliance on traditional high-sodium staples or inexpensive processed items versus limited access to fresh produce and nutrient-dense alternatives.
Perceived barriers to adherence
Perceived barriers to adherence emerged prominently in this study and help explain the low levels of dietary and lifestyle adherence observed among participants. The most frequently reported obstacles were limited knowledge about hypertension management, financial constraints, stress, and the lack of access to nutritionists within health facilities, all of which map closely onto the capability and opportunity domains of the COM-B framework. Patients with low educational attainment may struggle to understand and apply complex dietary and lifestyle advice (Firdaus Al-Ghifari Atmadja et al., 2025; Tam et al., 2020). At the same time, financial hardship restricts their ability to purchase healthier foods or engage in recommended activities (Appiah et al., 2022; Ingenhoff et al., 2022; Israfil and Rumambo Pandin, 2021), and the absence of nutrition professionals reduces the support available to translate recommendations into practical, culturally appropriate routines. The finding that 94% of participants reported an absence of a nutritionist in the facilities highlights a major structural gap in the health system. Their absence suggests that nutrition services are either deprioritized or inadequately integrated into primary health care. This structural issue likely contributes to fragmented service delivery, reliance on non-specialist staff for nutrition-related tasks, and limited capacity to address complex dietary needs. High levels of stress further erode motivation to sustain behavior change (Abaynew and Hussien, 2021; Cotter and Kelly, 2018; Kalinowski et al., 2021), suggesting that effective interventions in this context must address psychological and structural barriers alongside traditional health education.
Implications for practice
Our findings underscore the urgent need for multifaceted interventions that address both individual and systemic barriers to adherence among hypertensive patients in Lesotho. Educational programs should be prioritized to improve knowledge about hypertension management and empower patients to make informed decisions about their health. Culturally tailored dietary recommendations and increased access to nutritionists could further enhance adherence rates. Additionally, addressing financial constraints through subsidies or community-based programs could mitigate economic barriers and improve access to healthy foods and opportunities for physical activity (Appiah et al., 2022). Stress management interventions should also be integrated into hypertension care plans to address psychological barriers effectively.
Study strengths and limitations
The present study has several strengths. It addresses a critical gap in hypertension research in rural and semi-urban settings of Lesotho, where dietary management and lifestyle adherence remain underexplored.
The use of structured questionnaires based on WHO guidance provided a standardized approach to measuring adherence and perceived barriers. In addition, the study identified practical barriers, including financial constraints, low educational attainment, stress, and food preferences, that can inform targeted adherence-support interventions.
However, this study also has limitations, and the findings should be interpreted with caution. The cross-sectional design limits the ability to establish causal relationships between identified factors and adherence to dietary or lifestyle modifications; longitudinal studies would be needed to clarify temporal relationships. Participants were selected using convenience sampling, which may introduce selection bias and limit the generalizability of the findings to all hypertensive patients in Lesotho. Dietary and lifestyle adherence were assessed using interviewer-administered, self-reported questionnaires. Although this approach minimized literacy-related barriers, it may be affected by recall and social desirability biases, with some participants potentially overreporting recommended practices or underreporting nonadherent behaviors. When interpreting the regression findings, it is also important to recognize that the models were not fully adjusted for all potential confounders. The modest sample size, the low number of dietary-adherent participants, and the limited precision of some self-reported covariates increased the risk of unstable estimates if extensive adjustment was attempted. Consequently, the associations reported here may partly reflect differences in unmeasured or imprecisely measured participant characteristics rather than independent effects of the exposures.
Future studies with larger samples should pre-specify confounders and use more comprehensive adjusted models to confirm whether the relationships observed here persist after controlling for sociodemographic, clinical, and behavioral factors. Adherence was defined according to WHO-based criteria requiring participants to meet all selected dietary or lifestyle criteria. This strict definition strengthens comparability and identifies patients achieving comprehensive adherence, but it may also underestimate partial adherence and contribute to the low overall dietary adherence rate observed (8%). Future research should consider reporting graded adherence categories in addition to binary adherence status to capture partial improvements. The achieved sample size (n = 200) was lower than the initially calculated minimum of 304 participants due to time, staffing, and clinic attendance constraints during the data collection period. This reduction increased the margin of error and may have reduced statistical power, especially for detecting small associations and for the dietary adherence model, where the number of adherent participants was small. Despite these limitations, this study provides valuable context-specific evidence on barriers and determinants of dietary and lifestyle adherence among adults with hypertension in Butha-Buthe and Mokhotlong districts.
Conclusion
The findings of this study highlight the need for multifaceted, context-appropriate strategies to improve lifestyle and dietary adherence among adults with hypertension in Butha-Buthe and Mokhotlong districts. Priority should be given to simple, literacy-sensitive education programs that strengthen patients’ understanding of hypertension and its management, particularly for those with low educational attainment. District hospitals and chronic care clinics should integrate nutrition counseling into routine services, either by deploying nutritionists or training existing staff to provide culturally appropriate, low-cost dietary advice that accommodates patients’ food preferences. In addition, interventions that address financial barriers, for example, through the promotion of affordable, healthy foods, and community-based support, and incorporate basic stress-management and behavior-change support could help patients translate recommendations into sustainable daily practices. Policymakers and program planners should use these insights to design and test comprehensive adherence-support packages tailored to resource-limited settings such as Lesotho.
Footnotes
Acknowledgments
This research was partially funded by SolidarMed through the COMBACAL project. The authors gratefully acknowledge Dr. Mamakhala Chitja, Dr. Gerber Felix, and the entire SolidarMed team for their invaluable field support. The content of this work is solely the responsibility of the authors and does not necessarily reflect the official views of the funding organization.
Ethics approval and consent to participate
Ethical approval for this study was obtained from the Nutrition Department at the National University of Lesotho Institutional Review Board (NUL IRB), the Ministry of Health Ethical Committee, and the management teams of Butha-Buthe Government Hospital, Seboche Mission Hospital, and Mokhotlong Government Hospital. Written informed consent was obtained from all participants prior to their inclusion in the study.
Consent for publication
Not applicable.
Author contributions
The study was conceptualized and designed by MGS, LVH, and LSP, who also contributed to drafting the original manuscript. TKL and BM reviewed and provided critical feedback on the manuscript. Data collection was conducted by LVH and LSP, while MGS performed data analysis and contributed to the final draft. TKL and MGS reviewed the manuscript for intellectual content. All authors approved the final version of the manuscript for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by SolidarMed through the COMBACAL project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
All data generated or analyzed during this study will be made available upon request.
Clinical trial registration
Not applicable.