
Abstract
This study tests the association between weight status and depression in Italy using the Second Wave of the European Health Interview Survey (EHIS2) microdata, which also provide information on weight/height and eight depressive symptoms. Using a probit regression, the empirical results show a strong positive association between weight status, proxied by body mass index, and sleep troubles and eating disorders, with females suffering more than males. In addition, low interest is negatively associated with medium and high sources of income, while depressive mood and sense of failure are negatively associated with employment status. Individuals in midlife (45–54 years old) suffer from all depressive symptoms more than those in other age classes, with females suffering more than males, with the exception of low interest and depressive mood. Furthermore, individuals with a higher level of education have a lower likelihood of suffering from all depressive symptoms. These findings suggest that policies aimed at reducing obesity rates could also reduce new and emerging types of depressive symptoms correlated with overweight/obesity, such as sleep troubles and eating disturbances.
Introduction
In recent years, weight status has played an important role among a person’s individual characteristics. The study of the causes, consequences and correlates of obesity has interested many scholars from different disciplines, including health care, sociology, psychology and economics (Assari, 2014; Cawley, 2011, 2015; Dixon, 2010; Puhl, 2011). In the economic literature, reductions in the strenuousness of jobs (Lakdawalla & Philipson, 2002; Lakdawalla et al., 2005; Philipson, 2001), technological innovation in food processing and preparation (Cutler et al., 2003), the growing availability of fast-food restaurants (Chou et al., 2004; Rashad et al., 2005), increasing urban sprawl (Ewing et al., 2003), greater discounting of the future (Borghans & Golsteyn, 2006; Fuchs, 1982, 2004; Komlos et al., 2004; Smith et al., 2005; Zhang & Rashad, 2008), time-inconsistent preferences (Cutler et al., 2003; O’Donoghue & Rabin, 1999, 2000), health insurance (Rashad & Markowitz, 2007), higher unemployment (Ruhm, 2000), maternal employment (Anderson et al., 2003; Cawley & Liu, 2012), TV viewing and advertising (Smith, 2004) have been found to increase weight status. With regard to the economic consequences of weight status, a large body of literature has analysed the lower earning potential of overweight adults in the labour market (Averett & Korenman, 1996; Brunello & D’Hombres, 2007; Cawley, 2000, 2004; Harper, 2000; Morris, 2006; Pagan & Davila, 1997; Register & Williams, 1990). The European Commission (Suhrcke et al., 2005) and the World Health Organization (WHO, 2006a, 2006b) have long stressed the importance of addressing the issue of socioeconomic inequalities, mostly in income and education, as a central element of strategies to combat weight status, emphasising the fact that food choice is determined by both individual preferences and socioeconomic factors.
Regarding the association between weight status and depression, Granberg (2011) reminds us that since Friedman and Brownell’s (1995) seminal review, progress has been made towards a better understanding of the assessed link between depression and obesity. The great majority of papers analyse this link from the perspective that obesity is a source of depression, especially among adolescents, young adults and women, with three major pathway explanations: poor body image and appearance dissatisfaction, disrupted social relationships and health problems.
More recently, with the development of high-quality longitudinal data, evidence has shown that depression is a risk factor for the development of later obesity due to increase in dietary intake, decline in physical activity or both (Liem et al., 2008) or eating disorders, genetics or biochemical interactions (Goodman & Whitaker, 2002). Physical and social contexts may also help to explain how depression may contribute to an elevated risk of obesity.
Finally, a bicausal association between depression and obesity has been proposed (Hrabosky & Thomas, 2008; Markowitz et al., 2008): depression and obesity act on each other, for example, through binge eating and self-rated health. In addition, obesity acts on depression through dieting and social stigma, while depression acts on obesity through lack of exercise, negative thoughts and isolation.
The Second Wave of the European Health Interview Survey (EHIS2) data provide the opportunity to analyse the association between weight status, proxied by body mass index (BMI) and depression in Italy because, in addition to the usual information (demographic, socioeconomic, etc.), it provides information on weight/height and depression through eight depressive symptoms: low interest, depressive mood, sleep troubles, tiredness, eating disorders, sense of failure, low concentration and slow moving/speaking. 1 Among them, sleep troubles and eating disturbances have emerged in society more recently and can be considered relatively new variables when compared to low interest, depressive mood and sense of failure.
We are conscious that there are several caveats when using EHIS2 microdata: information on height and weight are self-reported; BMI is only one of the indicators of obesity; the eight depressive symptoms and the health variables (chronic disease and chronic anxiety) are self-reported; and the data are cross-sectional. Nevertheless, we emphasise that the EHIS2 provides new and useful information in the study of the association between weight status and depressive symptoms, notably, sleep troubles and eating disturbances, as an indicator of depression. In our analysis of the link between obesity and depression, we use a probit regression to assess the probability that individual i, given his/her overweight/obesity status, suffers from depressive symptoms, also controlling for specific characteristics such as age, gender, socioeconomic status (educational attainment, employment status, income), and tighter (marital status and social network) and looser (degree of urbanisation and geographical area where the individual lives) socioenvironmental factors. In Italy, the North–South dualism, which dates back to the nineteenth century 2 and remains deeply rooted in the economic, political, cultural and social life of these two macro areas of the country, provides the incentive to analyse the link between obesity and depression separately.
This study is structured as follows. In the next section, we outline the literature on the association between obesity and depression. In the third section, we describe the data and variables. In the subsequent section, we focus on the empirical design. In the fourth and fifth sections, we present the main empirical findings and robustness checks. A discussion of the results and conclusions is presented in the last section, emphasising the main policy evaluation.
Previous Studies: A Brief Review of the Literature
The World Health Organization (WHO) includes both physical and psychological components of well-being in the definition of health (WHO, 1946). In this view, health is positively defined as an individual’s fitness.
According to the economic approach to health production (Grossman, 1972, 2000), individuals simultaneously produce both physical and mental health by combining their own time for healthy activities with market goods such as nutritious foods and medical care. In this view, while health capital generally declines over time, individuals can alter the rate of decline by investing in their own health capital through health-related behaviours. Overeating, for example, leads to obesity, which contributes to a rise in the rate of decline of health capital.
In the economic approach to health production, a large role is played by the socioeconomic conditions of the individual: better socioeconomic conditions are expected to produce better health at both physical and mental levels.
Before outlining the literature on the role of socioeconomic conditions in the obesity–depression link, it is worth noting that in this link, gender has a key role. Some authors have underlined that because individuals have given characteristics, gender is expected to have an influence on physical and depression. Blehar and Oren (1995) show that women suffer from depression approximately twice as often as men, while men seek help less often than women and mask their depression with other lifestyle disorders. Costa-Font and Gil (2006) also found evidence of significant gender differences: depression and obesity in women are associated with household size and lifestyle, while depression in men is directly linked with the extent to which they are involved in personal interactions, their marital status and their occupational attainment.
Regarding socioeconomic conditions, we first consider educational attainment. In the literature, there is evidence that educational attainment can have positive effects on health through the better health information that an individual can acquire through education (Kenkel, 1991). However, the level of educational attainment can have negative effects, and highly educated individuals are relatively more exposed to higher risks of depression (Propper et al., 2004).
With respect to employment status (employed/unemployed), there is an evidence in the literature that unemployed individuals may be relatively more exposed to risks of depression than employed individuals (Farrè et al., 2018).
Costa-Font and Gil (2006) found that income does not increase the likelihood of obesity and socioeconomic position plays a less important role than socioenvironmental factors, especially family interactions, in explaining the obesity–depression association.
Regarding socioenvironmental factors, we first consider tighter factors, such as family interactions. In the literature, there is evidence that marriage leads to higher female obesity (Costa-Font & Gil, 2004) and parents clearly play a key role in the obesity of their children (Averett & Kohn, 2018; Cawley & Liu, 2012; Fielding-Singh, 2017).
Finally, there are looser socioenvironmental factors, such as unemployment rate and work pressure (Ruhm, 2000), high food and restaurant prices (Chou et al., 2004), level of urbanisation and geographical area. These factors may influence individual lifestyle choices, producing both physical and depressive symptoms.
From previous studies, it is interesting to observe that historically, depressive mood has mainly received attention, although currently, as EHIS2 demonstrates, sleep troubles 3 and eating disorders deserve to be analysed.
Data and Variables
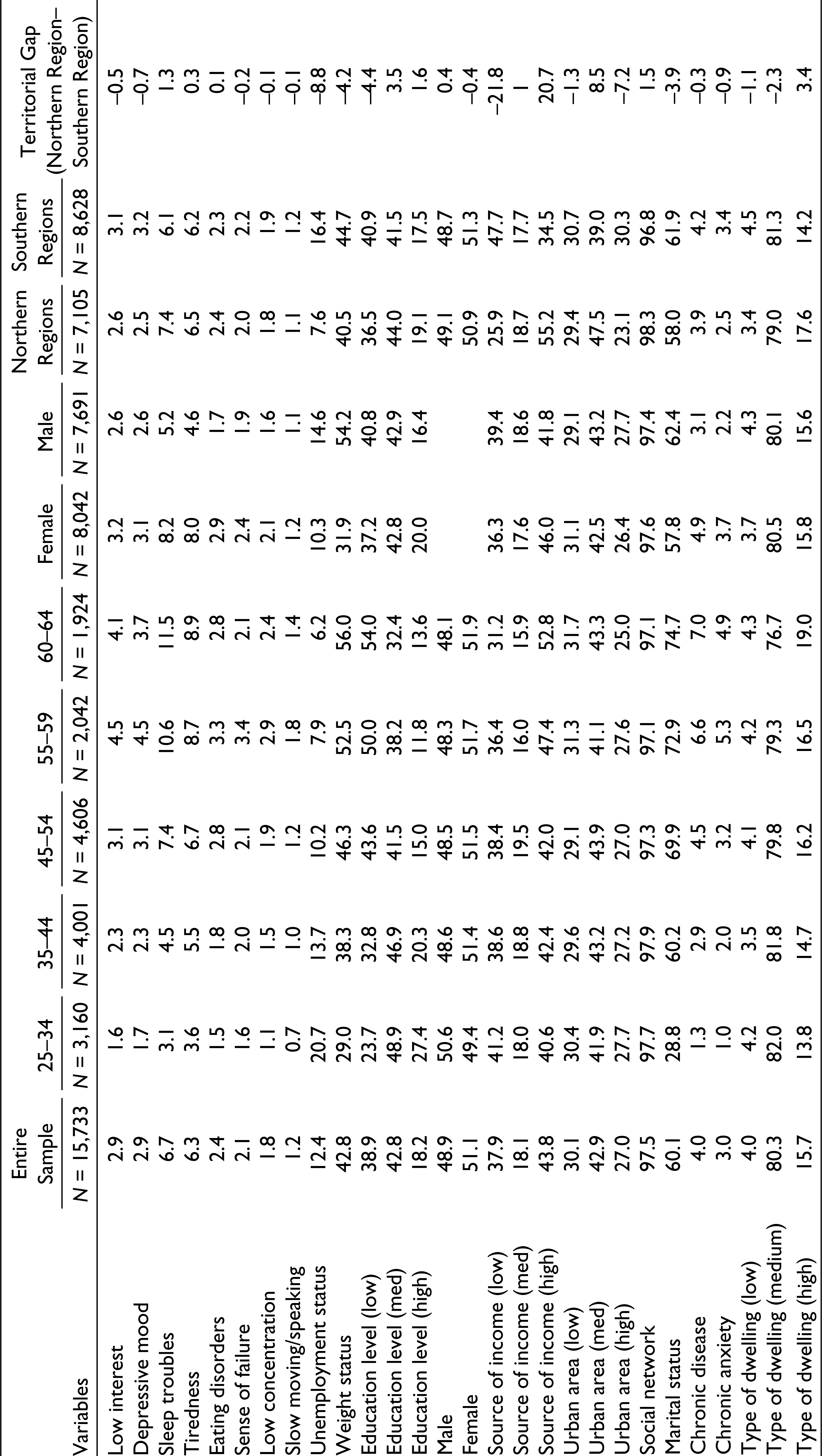
Table 1 describes the EHIS2 4 variables used in our empirical analysis, while Table 2 reports the main statistics divided by all samples, gender, macro area and age class.
Description of the Variables
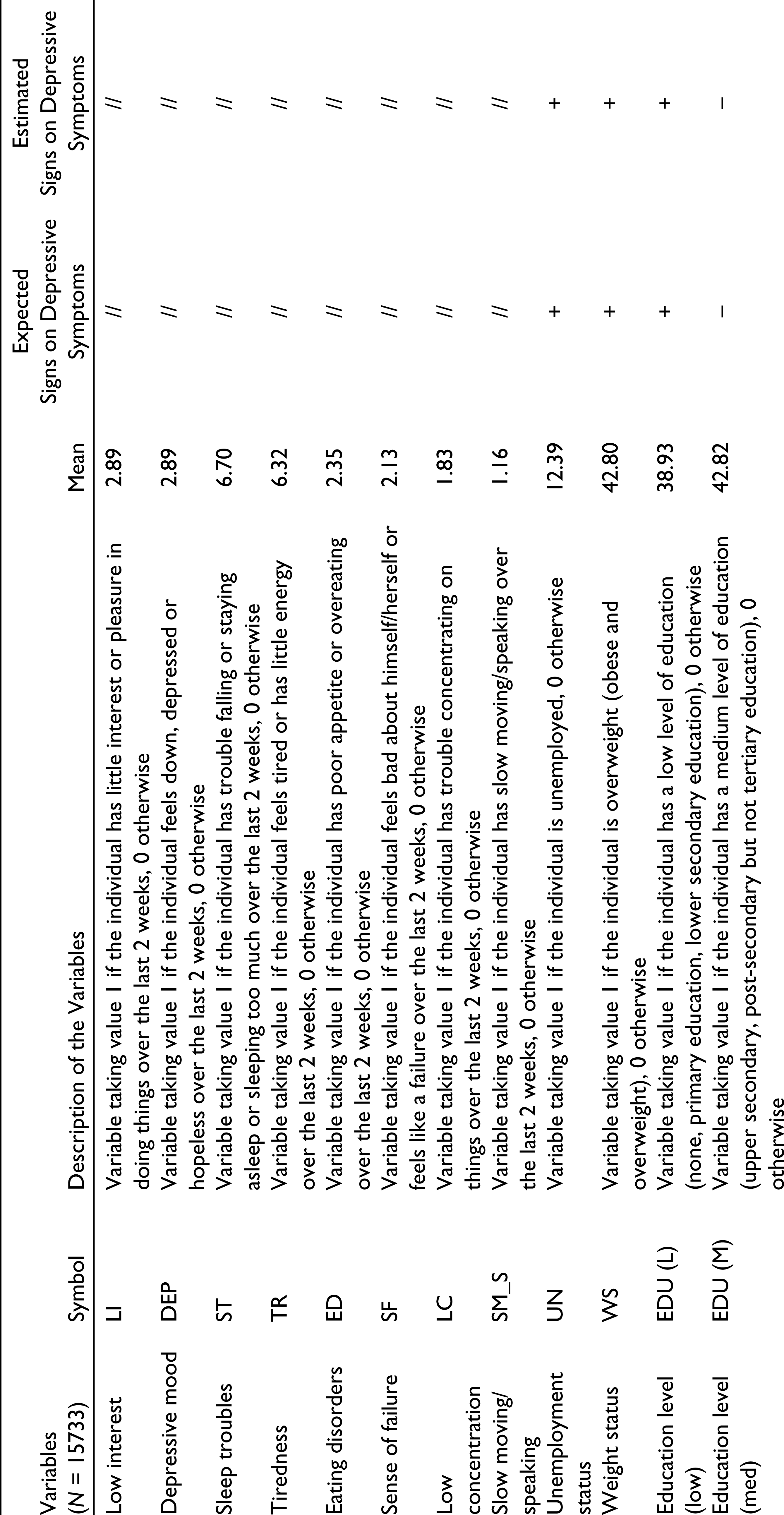
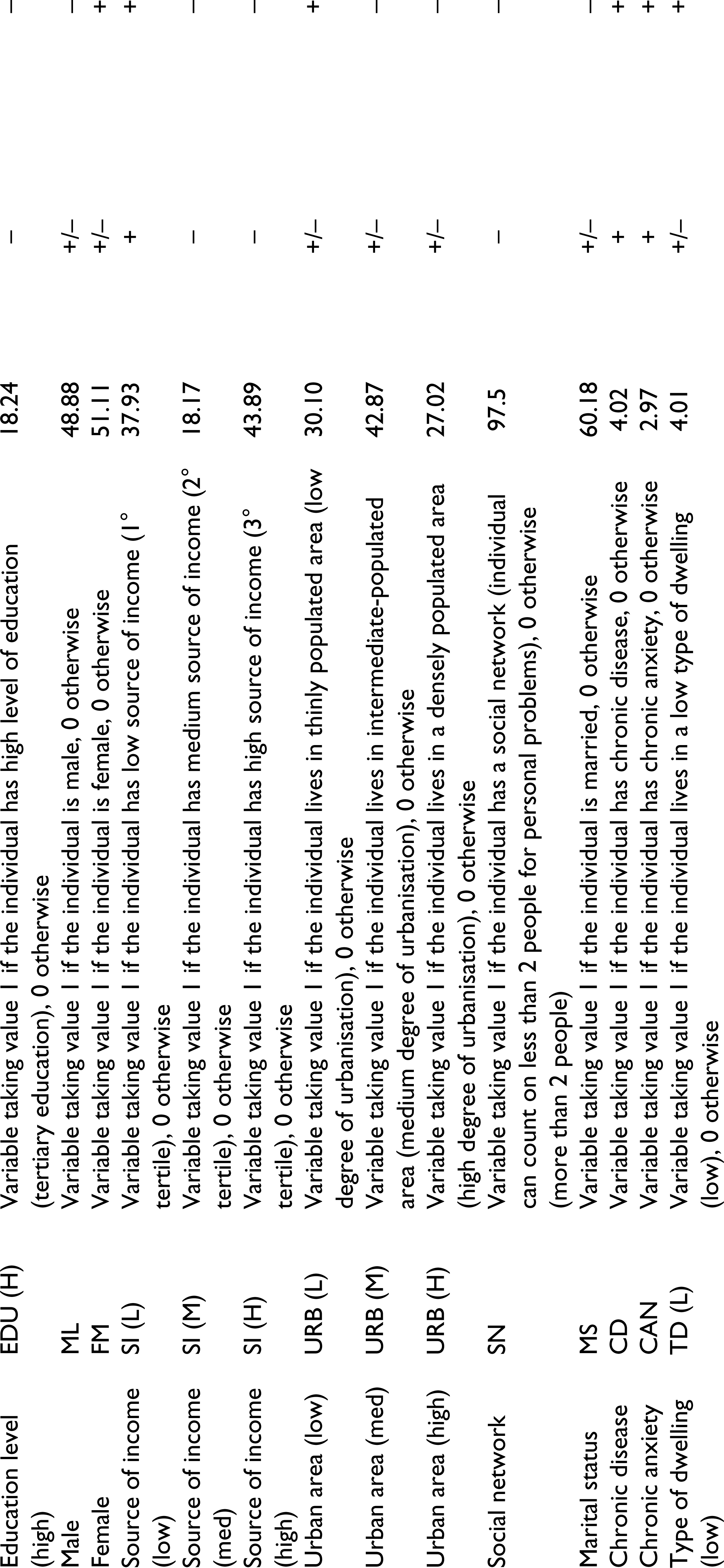
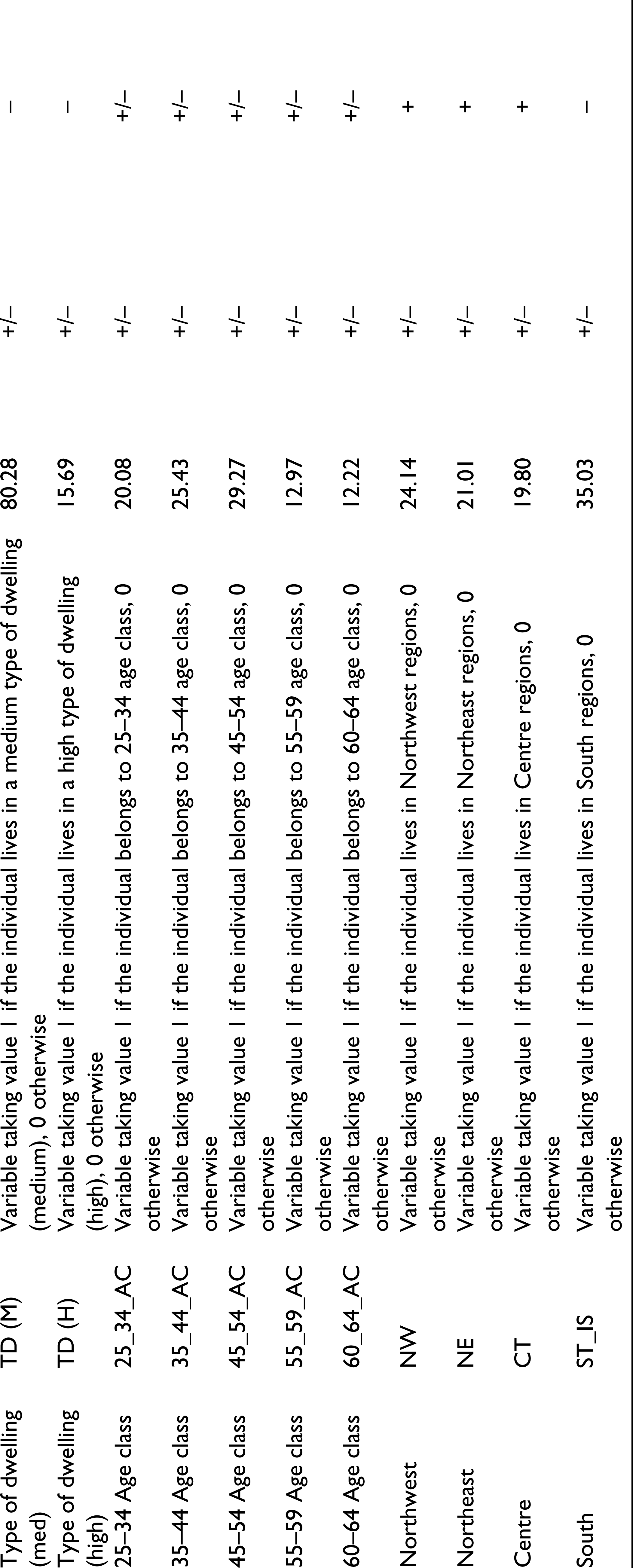
For the sake of clarity and brevity, we illustrate only the statistics that consider the entire sample of individuals between 25 and 64 years (see Table 2, column 1). The statistics confirm that in Italy, a low percentage of individuals, ranging from 1% to 6%, have depressive symptoms, and 13% declare that they are unemployed. It is interesting to note that approximately 43% of individuals are overweight and experience obesity problems. Only 18% attained a high level of education, while 43% have a high family income. Most individuals (43%) live in medium-level urbanisation areas, while 97.5% declare that they have been helped by multiple persons (more than 2) with their personal problems, thus establishing very strong social networks. Finally, 60% of individuals assert that they are married; a very low percentage, ranging from 3% to 4%, claim serious anxiety and chronic disease problems; and 80% live in medium-type dwellings.
Descriptive Statistics of Variables Divided by Gender, Macro Areas and Age Class (Values in Percentage)
Because of methodological problems (i.e., measurement problems, omitted variable bias and reverse causality), the causality mechanism is not clear. Because of the unavailability of longitudinal observations and reliable instrumental variables, we first analyse the correlation among weight status and depressive symptoms taking into account the individual characteristics and socio-economic conditions of the individual. The correlations between study variables are shown in Table 3. Obese individuals differ from normal weight individuals in regard to their eating behaviour and sleep patterns; as expected, we found a strong positive association between them, as reported in Table 3. In other words, obesity problems are associated with sleep troubles and eating disorders, which could become more problematic, for example, when individuals are still investing in their education (Stroebele et al., 2013).
Correlation Matrix for Study Variables (EHIS2)
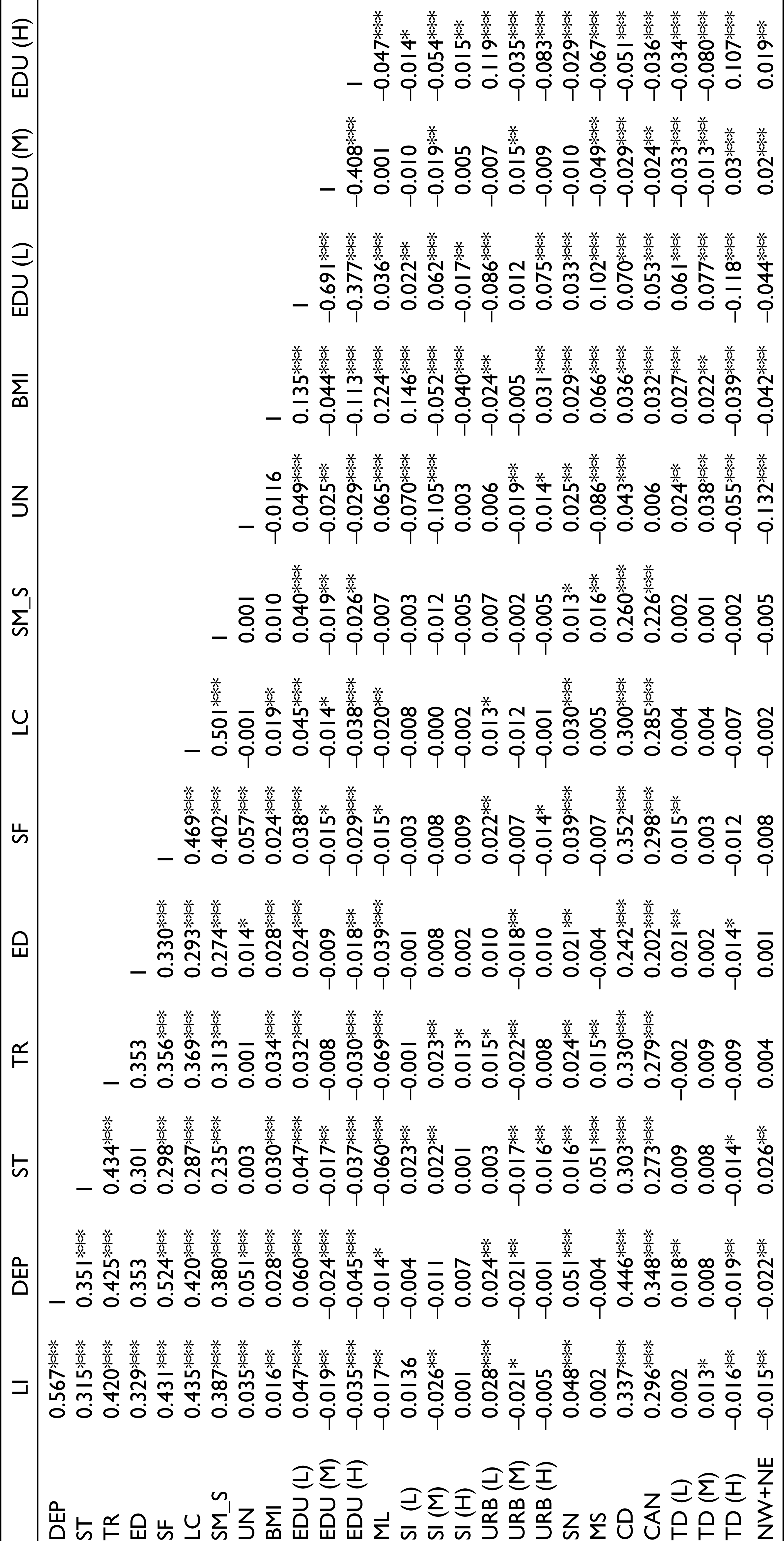
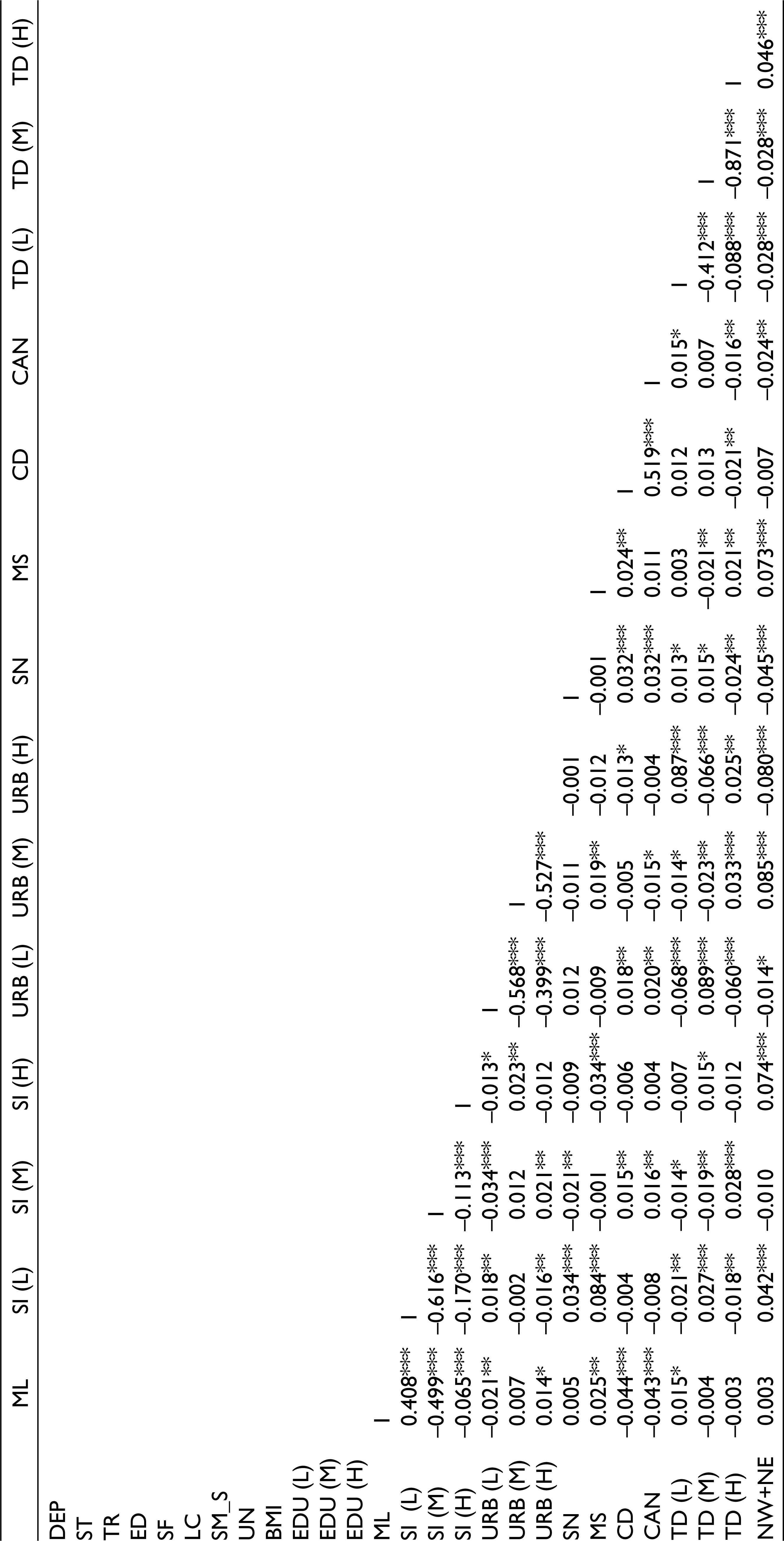
Moreover, we found a strong positive association between weight status and other depressive symptoms 5 (low interest, depressive mood, tiredness, sense of failure, low concentration), except for slow moving/slow speaking.
There is a positive association between weight status and education when the level of education is low and a negative association when the level is high. This could be due to the positive effects on weight status through better health information that an individual can acquire through education (Kenkel, 1991).
Gender plays a role because females have more depressive symptoms than males, as reported in most of the literature (Blehar & Oren, 1995; Costa-Font & Gil, 2006; Granberg, 2011).
The association between weight status and the source of income is positive for low sources of income and negative for intermediate and high sources of income. The association between weight status and the degree of urbanisation is negative for low and intermediate degrees of urbanisation and positive for a high degree of urbanisation.
There is a positive association between weight status and two socioenvironmental variables: being married and having a social network to count on, in case of difficulty.
Moreover, weight status, as expected, is positively associated with chronic diseases and chronic anxiety. 6
The association between weight status and the type of dwelling, a proxy of the wealth of individuals, is negative in the case of high type of dwelling: individuals with lower weight status live in luxury homes. Finally, considering looser socioenvironmental variables, a negative association emerges between weight status and living area for individuals (the North, i.e., Northwest and Northeast).
Empirical Design
To study the association between weight status and depression, we assessed an econometric model using a probit regression. 7 In particular, our model aims to assess the probability that individual i, given his/her overweight/obesity status, suffers from depressive symptoms, also controlling for some specific characteristics.
Formally and using a general framework, the probit model is described as follows:

where DSi denotes the eight depressive symptoms (for more details about the eight depressive symptoms included in the regression as dependent variables, see Note 4); WS stands for weight status, proxied by BMI; Z represents the vector of individual characteristics (demographic [age, gender], education [high vs. low; low as benchmark group], economic variables [employment status, source of income (high vs. low; low as benchmark group), type of dwelling (high vs. low; low as benchmark group)], health [chronic anxiety, chronic disease], social network, type of living environment [densely populated area, medium-populated area, low-populated area; low as benchmark group]) and macro regions of Italy (Northeast, Northwest, Centre, South; South as benchmark group) where the individual lives (see Table 1 for more details and descriptions of these variables and Table 2 for the main statistics divided by gender, macro areas and age class);
b1 and ci are parameter vectors, and εi is error term, which is assumed to be jointly normal with the unknown correlation coefficient.
In non-linear form, the probit model becomes

Finally, following a linear form, the probit model is

Empirical Evidence: The Nexus Between Weight Status and Depression in the Entire Sample
We begin to interpret the estimates considering the entire sample of individuals, that is, those belonging to the age group of 25–64 years. The coefficients and marginal effects of the probit regression are reported for various depressive symptoms in Table 4 (columns A1–A8). The standard errors of the coefficients have been clustered around the macro regions in which the individuals are located.
Obese individuals differ from individuals of normal weight in eating behaviour and sleep patterns, and, as expected, we found a strong link between them. Weight status is positively associated with sleep troubles (column A3) and eating disorders (column A5). In other words, overweight/obesity is positively associated with sleep troubles and eating disorders, which could become more problematic if individuals, for example, are still investing in their education (Stroebele et al., 2013).
Gender plays a role because females have more depressive symptoms than males, as reported in most of the literature (Blehar & Oren, 1995; Costa-Font & Gil, 2006; Granberg, 2011).
Education clearly emerges as a key characteristic: there is a lower likelihood of suffering from many depressive symptoms (low interest, depressive mood, sleep troubles, sense of failure (p < .10), low concentration, slow moving/speaking) associated with a high level of education. Considering only the estimates that are statistically significant, the results show that depressive symptoms decrease as the level of education increases from medium to high.
Table 4 demonstrates, for the whole sample, that while weight status is associated with sleep troubles, tiredness and eating disorders, unemployment is associated with depressive mood (column A2) and sense of failure (column A6). In terms of magnitude, we find that sleep troubles and eating disorders are positively associated with weight status, while low interest and depressive mood are associated with socioeconomic variables: low interest is positively associated with medium and high sources of income, while depressive mood and sense of failure are negatively associated with unemployment status.
Weight Status and Depression (Entire Sample)
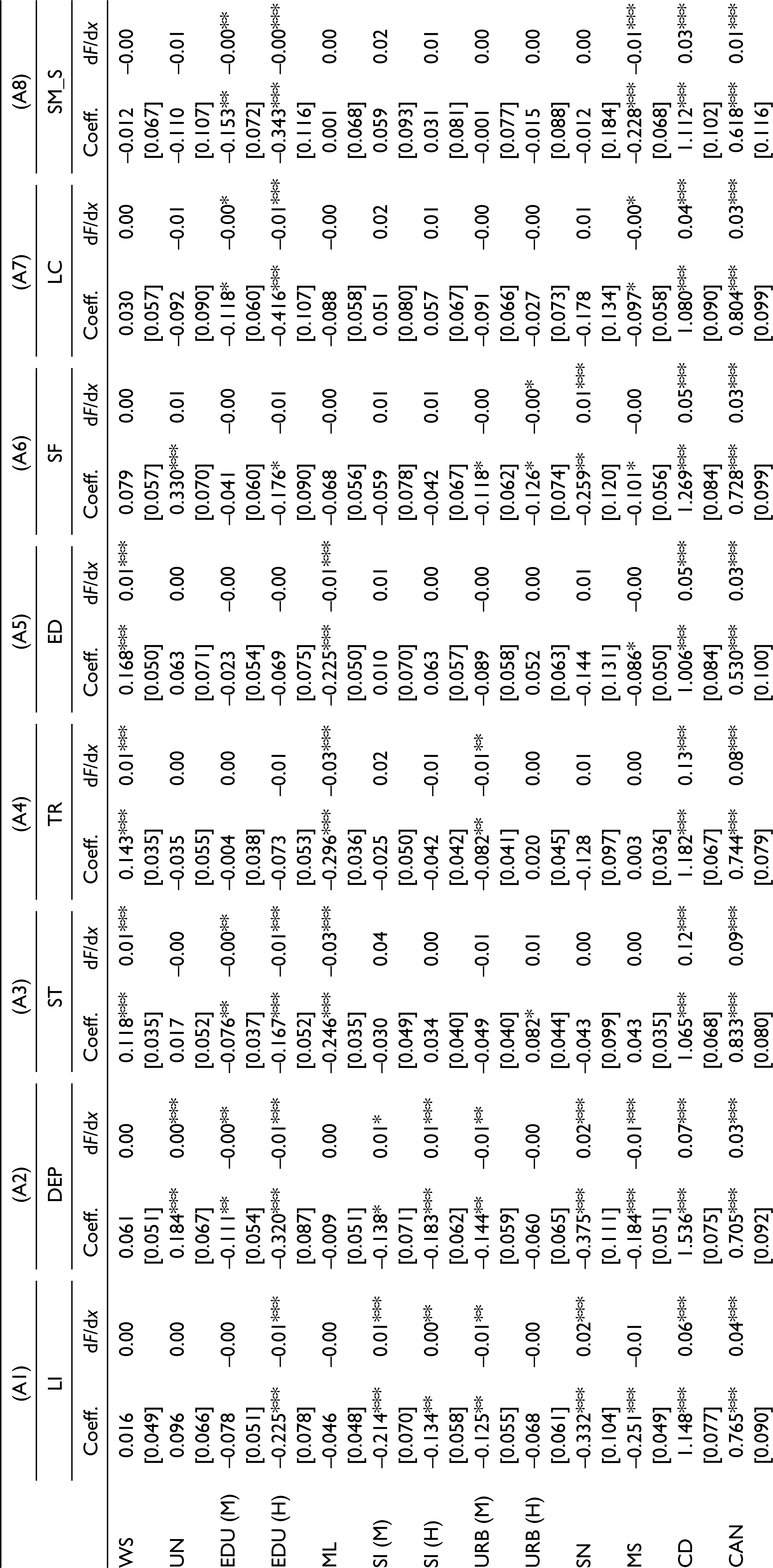

Individuals who are married and have a social network to count on in case of difficulty have a lower incidence of low interest and depressive mood. Individuals who live in luxurious homes have a lower incidence of eating problems, where the type of dwelling could be considered a proxy of wealth: the wealthier an individual is, the lower the probability of having eating disturbances.
Moreover, health variables, as expected, explain part of the variability of depressive symptoms: individuals with chronic disease and severe chronic anxiety have an increased likelihood of suffering from both sleep troubles and eating disorders.
Finally, considering looser socioenvironmental variables, it seems that individuals living in the North have a higher likelihood of suffering from sleep troubles. Moreover, only two depressive symptoms—low interest and depressive mood—are associated with urbanisation levels: the lower the level of urbanisation, the higher the probability that an individual feels low interest and depressive mood.
The results show, first, that weight status is associated more with physical disturbances such as sleep troubles, tiredness and eating disorders, while unemployment is linked to depressive mood and sense of failure. Second, that there are interesting strong and positive gender differences in the association between weight status and sleep troubles/eating disorders: females suffer more than males. Third, education, as expected, is a key characteristic: with a high level of education, the likelihood of suffering from many depressive symptoms is lower.
The results we found are slightly different from those reported by Costa-Font and Gil (2006), in which socioeconomic position (education, employment, income) plays a less important role than socioenvironmental factors, especially family interactions, in explaining the obesity–depression association.
More generally, the results show that improving socioeconomic and socioenvironmental factors could contribute to counteracting the increasing phenomenon of obesity and depressive symptoms in Italy. These results can also be found in the US social situation, although there are significant differences in the mortality rates between Europe and the US due to their different health systems. According to Case and Deaton (2020, ch. 8), in the past two decades, deaths of despair from suicide, drug overdose and alcoholism have risen dramatically among midlife, white, non-Hispanic working-class people in the United States. As in the case of deaths, worsening health (overweight, smoking, drinking, pain, serious mental distress and difficulty going about their day-to-day lives) seems to be isolating people of working age with less education. As colleges become healthier and wealthier, adults without a degree literally die from pain and despair (Case & Deaton, 2020, ch. 6). In addition to growing inequality, Case and Deaton tie the crisis in the US to the weakening position of labour, the increasing power of corporations and an overpriced yet inadequate health system, which cast shadows on the functioning of capitalism itself.
Robustness Checks
How Does Gender Influence the Estimation?
As a result of the heterogeneity problem in our sample, we estimated the model described in Equation 1 grouping by gender, that is, males and females. As before, the standard errors of the coefficients have been clustered around the region in which the individuals are located.
We begin to interpret the results considering only the female group (columns B1–B8, Table 5). Once again, we find a strong link between weight status and depressive symptoms as an indicator of depression. As expected, weight status is positively associated with sleep troubles (column B3), eating disorders (column B5) and tiredness (column B4).
Weight Status and Depression (Female Group)
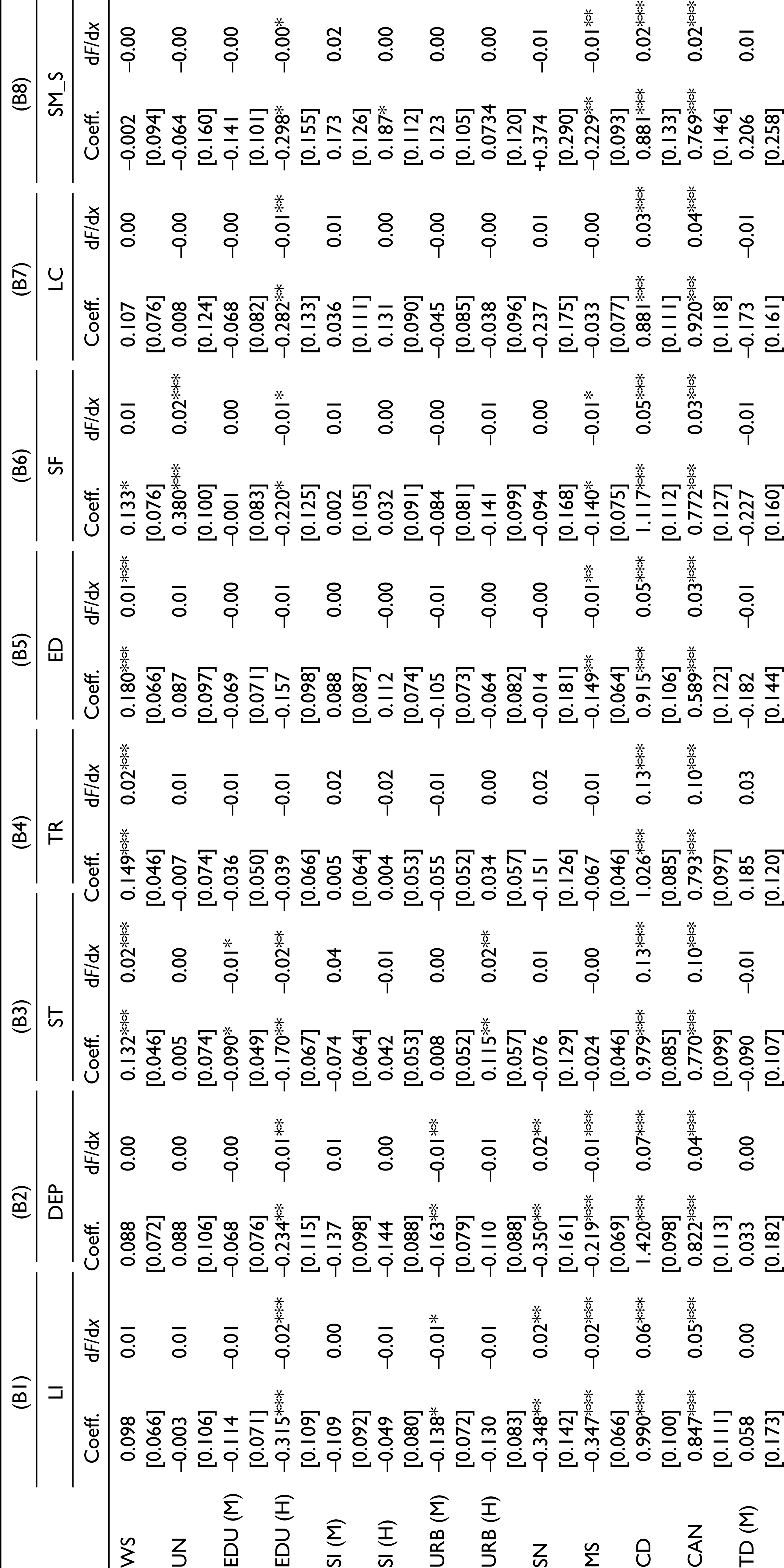

With respect to the entire sample, for females, there is an evidence of a link between unemployment status and sense of failure (column B6), although there is no evidence of its role in depressive mood (column B2). Among individual socioeconomic variables, it is interesting to observe that with high levels of education, there is a lower probability of suffering not only from sleep troubles but also from all other depressive symptoms except eating disorders (column B5).
Among the tighter individual socioenvironmental variables, it is worth noting the positive role played by marriage: married females have fewer eating disorders and lower degrees of problems with low interest and depressive mood.
Among the looser individual socioenvironmental variables, the level of urbanisation is associated with low interest and depressive mood; the lower the level of urbanisation is, the higher the probability that an individual feels low interest and depressive mood. Moreover, the health variables, as expected, explain part of the variability of depression. Chronic disease and severe chronic anxiety are positively associated not only with sleep troubles and eating disorders but also with the other six depressive symptoms. Females with chronic disease and severe chronic anxiety have an increased likelihood of having depressive symptoms; this result is in line with the existing literature on the issue (Blehar & Oren, 1995; Costa-Font & Gil, 2006; Granberg, 2011). Finally, females in the North experienced more sleeping troubles.
Now, let us interpret the results considering the male group (columns C1–C8, Table 6). Once again, we find a strong link between weight status and depressive symptoms. As expected, weight status is positively associated with sleep troubles (column C3) and eating disorders (column C5).
Weight Status and Depression (Male Group)
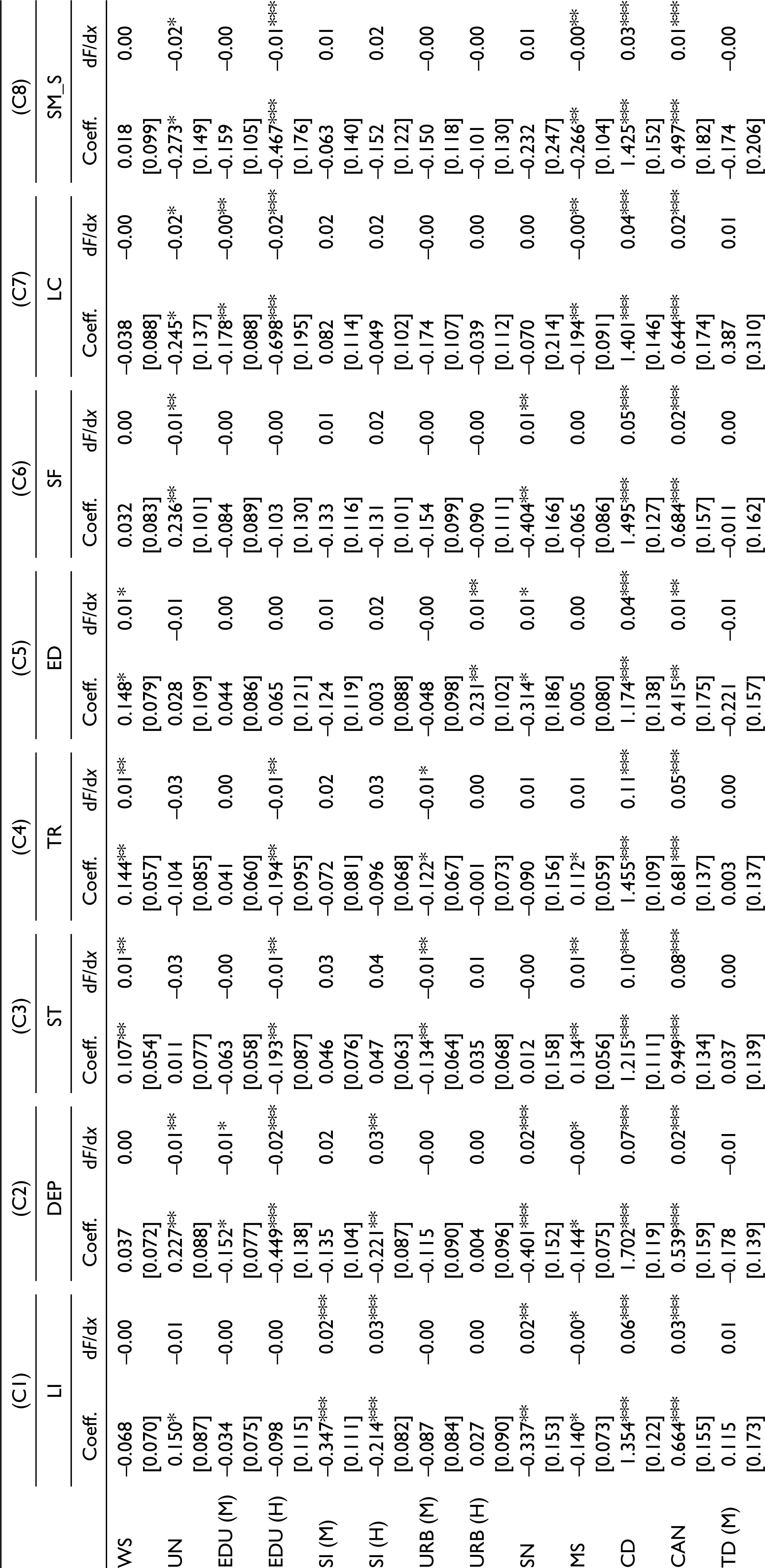

The health variables, as expected, explain part of the variability of depression. Chronic diseases are positively associated with sleep troubles and eating disorders. Males with chronic disease problems and severe chronic anxiety have an increased likelihood of having depressive symptoms.
Similar to females, we found that for males, there is a negative association between high levels of education and sleep troubles, but there is no link with eating disorders. Males show evidence of a link between unemployment status and depressive mood and sense of failure. Among the looser socioenvironmental variables, married males have more sleeping problems than eating problems. There is no link between social networks and sleep troubles/eating disorders. Furthermore, it seems that males living in the North have more sleep troubles than those living in the South. Finally, in contrast to females, there is a positive association for males between medium urbanisation levels and sleep troubles.
How Does Territorial Diversification Influence the Estimation?
To validate our empirical analysis, we estimate the model described in Equation 1 for different geographical areas, that is, Northern and Southern regions. This allows us to control for territorial differences and test which areas drive the results. As before, the standard errors of the coefficients are clustered around the region in which the individuals are located.
First, we interpret the results only considering the subsample of individuals who live in Northern Italy (columns D1–D8, Table 7). With respect to the cases analysed above, we do not find a strong link between weight status and depressive symptoms.
Weight Status and Depression (Northern Regions)
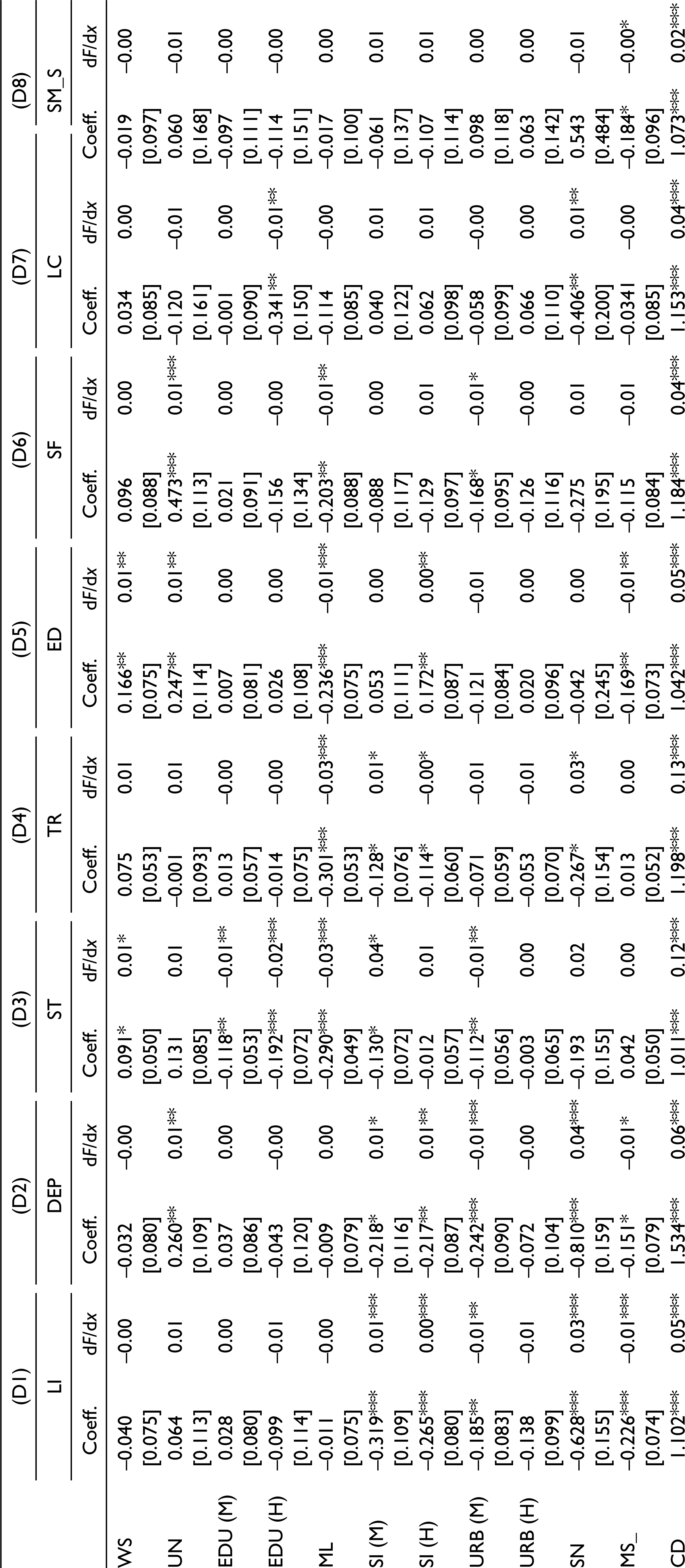

Females have more depressive symptoms, including sleep troubles, tiredness, eating disorders and sense of failure.
The health variables, as expected, explain part of the variability of depression. Chronic disease and severe chronic anxiety are positively associated with depressive symptoms.
High levels of education are negatively associated with sleep troubles (albeit weakly, 10% significance).
We find that there is evidence, albeit weak, of a positive link between employment status and depression. In other words, unemployed individuals have more depressive symptoms.
There is a negative association between the source of income and low interest, depressive mood and eating disorders: the higher an individual’s income is, the lower his or her probability of feeling low interest, feeling depressed or having eating disorders. Individuals who lived in luxurious homes did not report depressive symptoms.
The social network is negatively associated with two depressive symptoms: low interest and depressive mood. The stronger the network, the lower the probability that the individual feels low interest and has a depressive mood. Being married also lowers the probability of feelings of low interest and depressive mood.
Finally, no association was found between low urbanisation levels and depressive symptoms.
Second, we interpret the results considering only the subsample of individuals who live in Southern Italy (columns E1–E8, Table 8). With respect to individuals located in the North, we find a strong link between weight status and depression: weight status is positively associated with sleep troubles (column E3) and eating disorders (column E5), demonstrating that high levels of obesity in individuals who live in the South are positively associated with depressive symptoms.
Weight Status and Depression (Southern Regions)
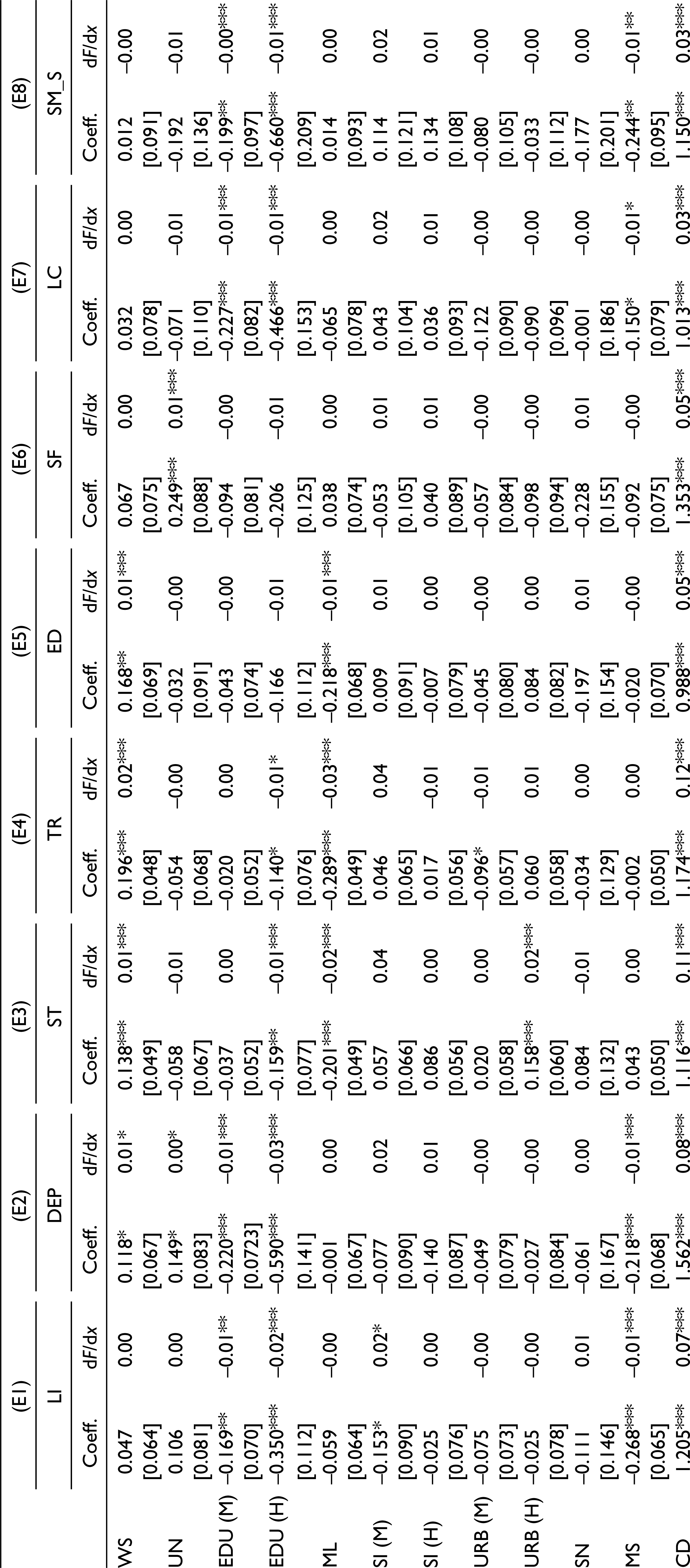

With respect to gender, females show more depressive symptoms.
The health variables, as expected, explain part of the variability of depression. As before, chronic disease problems and severe chronic anxiety are positively associated with the likelihood of having depressive symptoms.
High levels of education are negatively associated with sleep disorders (albeit weakly, 10% significance). The source of income seems not to be associated with depression issues. Individuals living in luxurious homes show more depressive symptoms than similar individuals living in the North. Both marital status and social networks are negatively associated with low interest and depressive mood. Finally, there is a positive association between higher levels of urbanisation and sleep troubles.
How Does Age Class Influence the Estimation?
We estimated the model described in Equation 1 for different age classes, that is, 25–34, 35–44, 45–54, 55–59 and 60–64 (columns F1–F8, Table 9). For the sake of space, we focus only on the weight status coefficient for all age classes. From the probit regression, we find that in both the North and the South, two age classes suffer more than the others from their weight status: young adults (25–34 years old) and those in midlife (45–54 years old). However, in the South, young adults suffer more than those in the North: five of the eight variables in the South are significant compared to three in the North. In both regions, eating disorders and sense of failure are significant; in the South, depressive mood, sleep troubles and tiredness are also significant. With respect to the 45–54 years age class, tiredness is significant in both regions, albeit with a higher rate of significance in the North. Interestingly, in the South, sleep troubles and eating disorders are significant, while in the North, sense of failure is significant.
Weight Status and Depression (Age Classes)
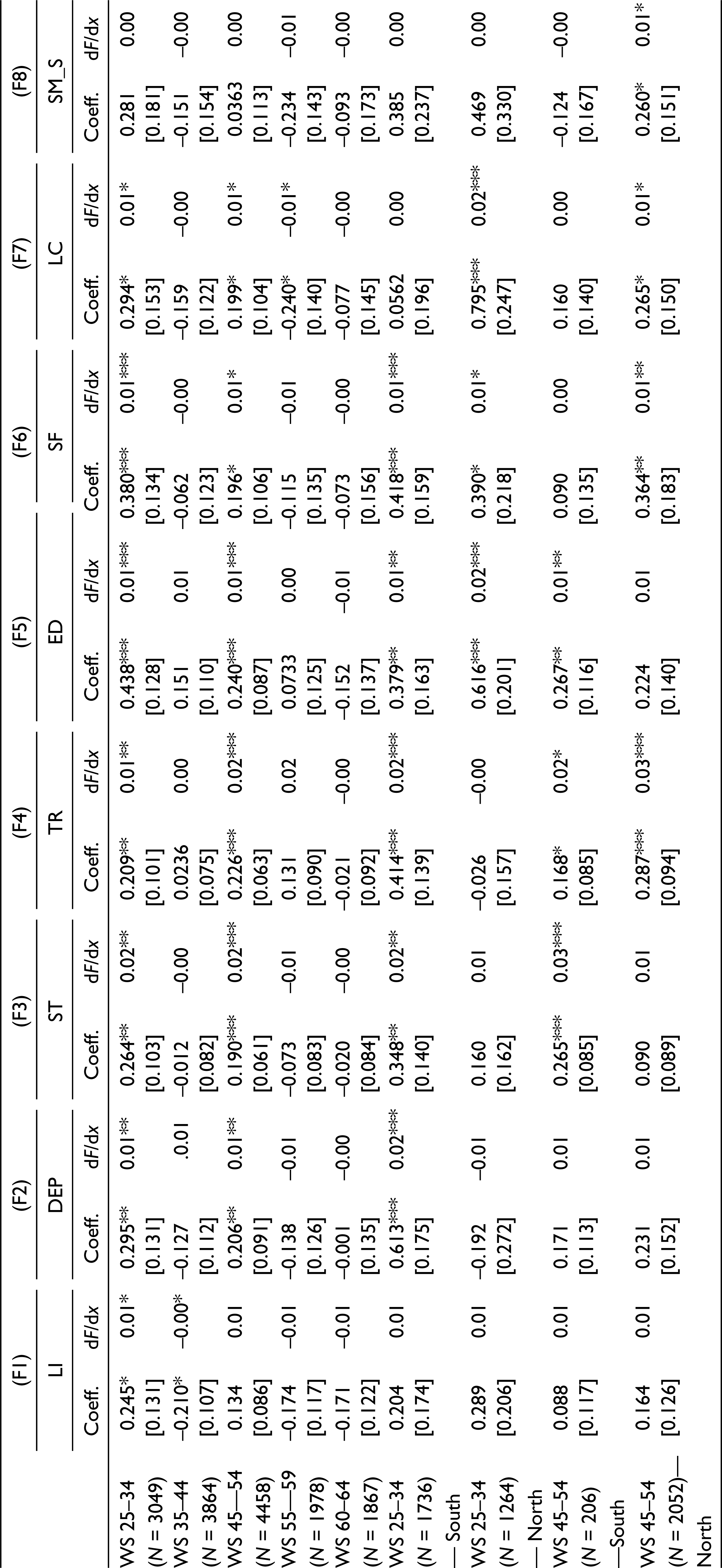
For robustness, we repeated the regression only for these two classes and for different geographical areas (Northern and Southern regions). The results show that weight is positively associated with depression, especially in the Southern regions, underlining the fact that in the Northern regions, fewer depressive symptoms are associated with weight status.
How Does an Alternative Estimator Influence the Estimation?
Finally, as an additional robustness check, we estimated the model described in Equation 1 using a multinomial logit model to measure the association between weight status and depression by gender (columns G1 and G2, Table 10), territorial heterogeneity (columns G3 and G4, Table 10) and the entire sample (column G5, Table 10). In this model, the depression variable takes the value of 0 when an individual claims to not have depression symptoms, 1 when an individual has little interest or pleasure in doing things (low interest), 2 when an individual feels down, depressed or hopeless (depressive mood), 3 when an individual has trouble falling or staying asleep or sleeps too much (sleep troubles), 4 when an individual feels tired or has little energy (tiredness), 5 when an individual has poor appetite or overeating (eating disorders), 6 when an individual feels bad about himself/herself or feels like a failure (sense of failure), 7 when an individual has trouble concentrating on things (low concentration) and 8 when an individual has slow moving/speaking (slow moving/speaking) (for more details about the definition of these variables, see Table 1).
Weight Status and Depression: A Multinomial Logit Model
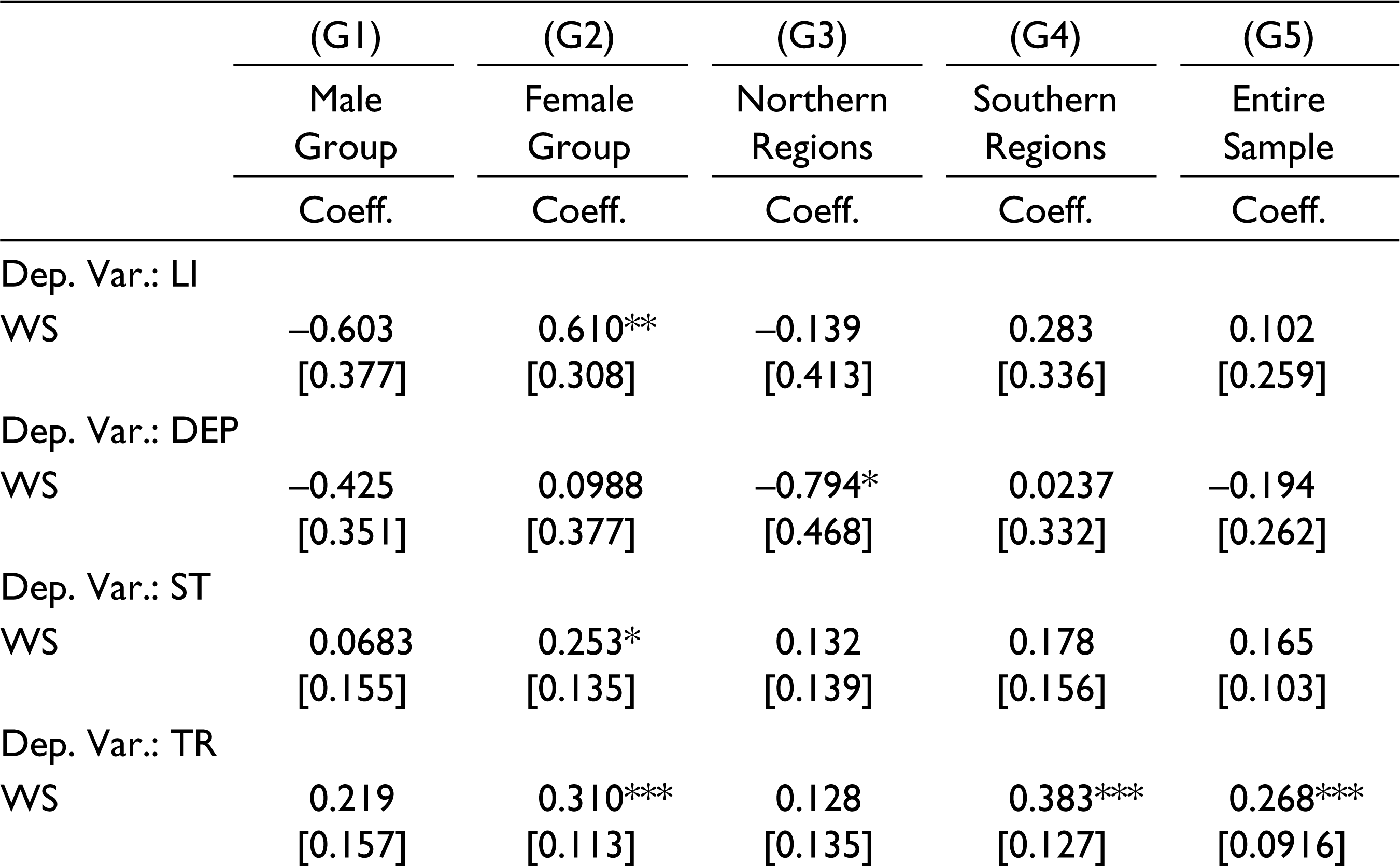
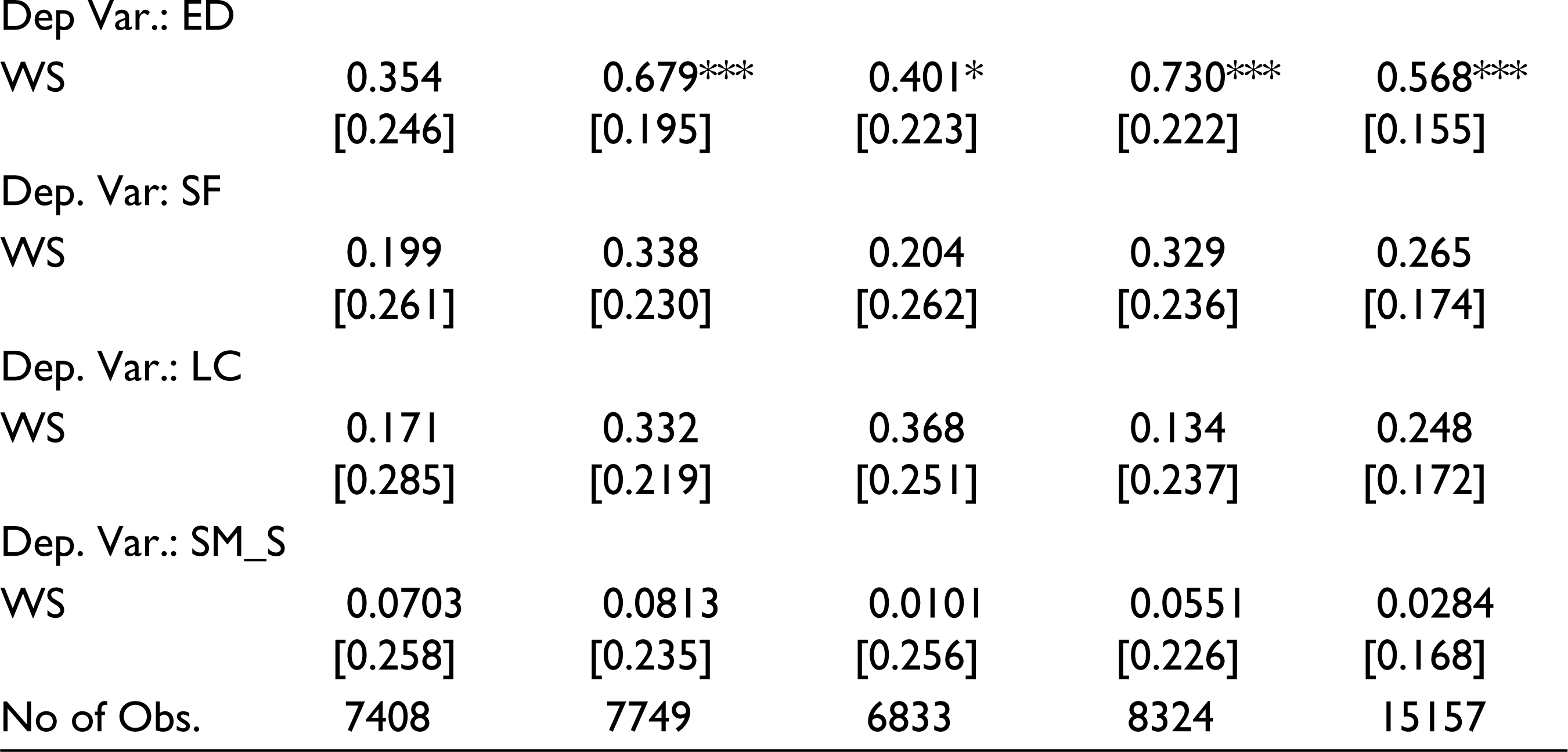
BMI classification has a nonlinear relationship between BMI and depression. For example, low BMI is associated with one set of depressive symptoms, and high BMI is associated with a separate set of depressive symptoms, leaving behind the ordinal ranking associated with a probit and indicating the likelihood of being classified as one BMI classification versus another without a prespecified functional form.
The results confirm that females suffer more from low interest, sleep troubles, tiredness and eating disorders than males. In addition, the empirical findings are mainly driven by the Southern regions as we find that tiredness and eating disorders are more present in this area than in the Northern regions.
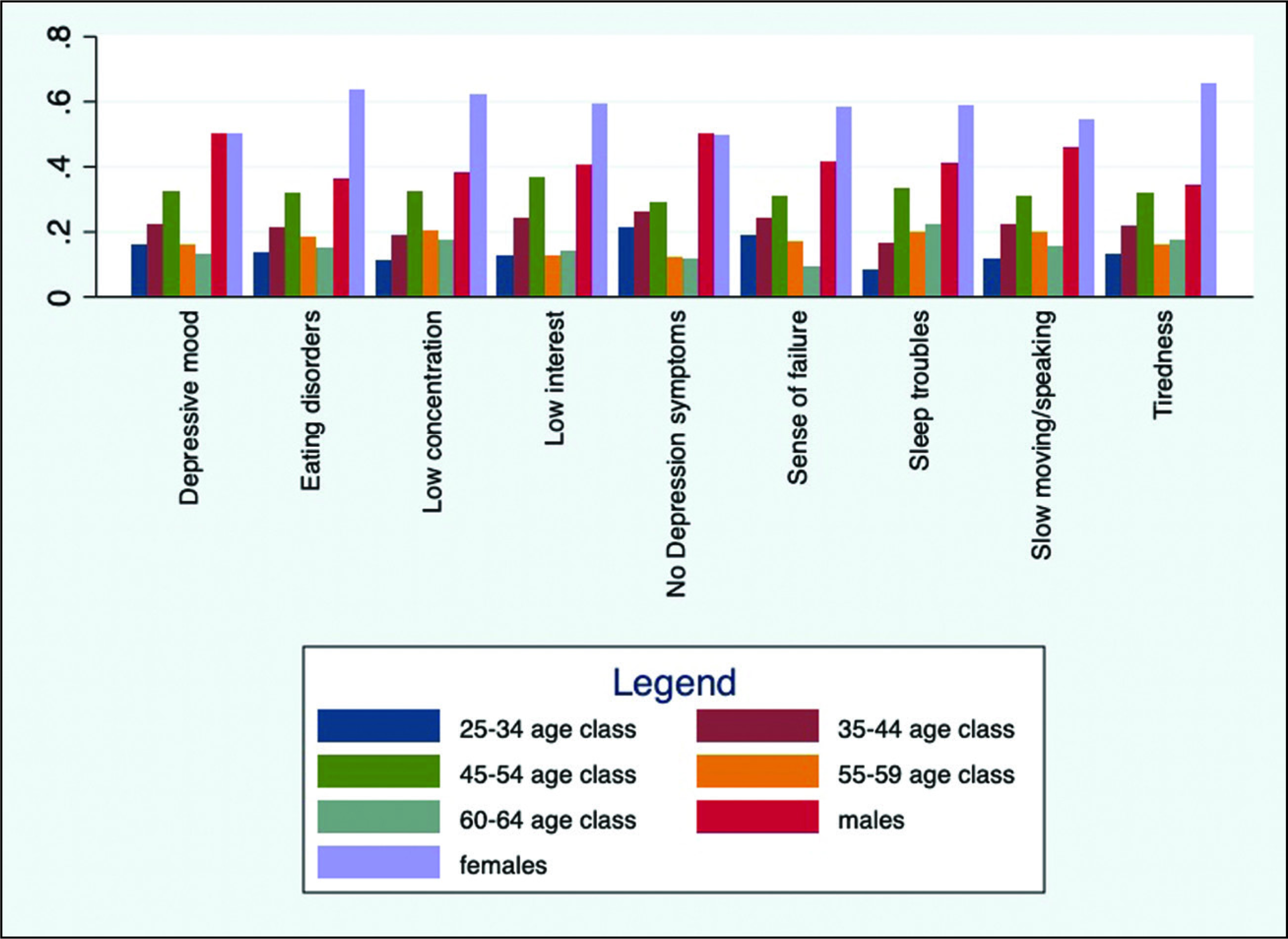
Figure 1 allows us to clarify the pattern of depressive symptoms by age class and gender. This figure indicates that for all the depressive symptoms, individuals in midlife (45–54 years old) suffer more than individuals in the other age classes. This evidence is in line with the hill-shaped relationship between unhappiness and age found by Blanchflower (2020). In addition, for the same age class (45–54 years), females suffer more than males from all depressive symptoms except for low interest and depressive mood.
Discussion of the Results and Conclusions
The empirical results show that in Italy, there is a strong positive association between weight status and two depressive symptoms, sleep troubles and eating disorders. There is also an interesting gender difference in this association in that females suffer more than males. Moreover, while sleep troubles and eating disorders are positively associated with weight status, the empirical results show that low interest, depressive mood and sense of failure are negatively associated with socioeconomic variables (unemployment status, economic resources).
Finally, the empirical findings indicate that two age classes in both geographic regions suffer from their weight status more than the others: young adults (25–34 years old) and middle-aged adults (45–54 years old). Young adults in the South suffer more than those in the North.
The results show that individuals in midlife (45–54 years old) suffer from all depressive symptoms more than those in other age classes, with females suffering more than males from all depressive symptoms except low interest and depressive mood. People in midlife suffer more from sleep troubles and eating disorders in the South and more from a sense of failure in the North.
As expected, health variables explain part of the variability of depression (individuals with chronic disease and severe chronic anxiety have an increased likelihood of having all depressive symptoms). Furthermore, education is a key characteristic: the higher an individual’s education, the lower the individual’s likelihood of suffering from all depressive symptoms.
These results suggest some policy considerations. First, policies aimed at reducing obesity rates could reduce new and emerging types of depressive symptoms such as sleep troubles, tiredness and eating disturbances. Second, educational policies could also help individuals establish barriers against the eight types of depressive symptoms analysed in the EHIS2.
There are more general considerations suggested by these results on depression. Among individual socioenvironmental variables, there are two interesting factors that seem to protect against low interest and depressive mood: being married and having a social network on which to rely in case of difficulty. The same result occurs when source of income is taken into account. Considering looser socioenvironmental variables, it seems that individuals living in the Northwest and Northeast have a higher likelihood of having sleep troubles. Moreover, taking into account urbanisation levels, the results show that the lower this level is, the higher the probability that an individual feels low interest and depressive mood.
These results suggest that in Italy, socioeconomic factors other than education (i.e., unemployment status, economic resources) and socioenvironmental factors (i.e., marital status, individual social network, environment in which the individual lives) involve low interest, depressive mood and sense of failure more than sleep and eating disturbances, suggesting that all depressive symptoms have deep roots in economic mechanisms and social relationships that require ad hoc economic and social policies.
Footnotes
Acknowledgements
We thank two anonymous referees for their comments on this article. Nevertheless, any remaining errors are the authors’ responsibility.
Declaration of Conflicting Interests
The authors declares no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.