
Abstract
The period 2010–2013 was a time of far-reaching structural reforms of the National Health Service in England. Of particular interest in this paper is the way in which radical critiques of the reform process were marginalised by pragmatic concerns about how to maintain the market-competition thrust of the reforms while avoiding potential fragmentation. We draw on the Essex school of political discourse theory and develop a ‘nodal’ analytical framework to argue that widespread and repeated appeals to a narrative of choice-based integrated care served to take the fragmentation ‘sting’ out of radical critiques of the pro-competition reform process. This served to marginalise alternative visions of health and social care, and to pre-empt the contestation of a key norm in the provision of health care that is closely associated with the notions of ‘any willing provider’ and ‘any qualified provider’: provider-blind provision.
Introduction
There are two features of the recent health care reforms in England that are striking and arguably contradictory. First, the two-year passage of the Health and Social Care Act (2012) was dominated by contestation and dissent, including very public calls for the Health and Social Care Bill to be withdrawn. The dissenters included the British Medical Association (BMA), a clutch of royal colleges, a former secretary of state for health, various think tanks, the opposition party, and even the grass roots of the minor party to the Coalition government itself (see Timmins, 2012). Objections were raised regarding the role of competition and profit in health care (a long-held objection of the BMA), linking this worry to global trends of health care privatisation (see Pollock et al., 2012), and the perceived threat to democratic accountability and the values of universalism and welfarism (see Pollock et al., 2012 and Reynolds and McKee, 2012). The second feature, though, is that despite fears that the reforms would prove to be the Coalition’s poll tax (The Guardian, 22 February 2012), critique and debate over alternative visions were decisively marginalised, allowing the Act to proceed with its principal objectives largely intact (Leys and Player, 2011; Timmins, 2012). How was this accomplished?
Drawing on the logics approach to critical policy analysis (Glynos and Howarth, 2007; Howarth, 2010; Glynos and Speed, 2012; Glynos et al., 2012; West, 2013), we suggest that the marginalisation of critical concerns and worries regarding far-reaching pro-competitive reforms in health and social care was achieved in large part through the mobilisation of a political logic organised around the idea of ‘integrated care’. We treat integration less as a concrete vision with a precise meaning and more as an ‘empty signifier’ and ‘master political logic’. As an ‘empty signifier’ it served as a receptacle for affective investments prompted by perceived threats of disintegration linked to unfettered competition. And as a ‘master political logic’ it organised a range of ‘minor’ marginalising manoeuvres. In particular, we argue that a set of political logics, both organisational and rhetorical, succeeded in policing the borders of mainstream official and popular discourse, serving to actively marginalise alternative visions of health and social care; and that their success is due in part to their capacity to act as a hinge between concrete visions on the one hand (cashed out in terms of projected norms and values) and potent affective investments on the other hand. In what follows we summarise the background assumptions and basic concepts of a logics approach to the critical explanation of practices, showing how we operationalise it for purposes of critical policy analysis through a ‘nodal framework’. We then offer a critical account of the process of marginalisation by focusing on key moments of contestation in the passage of the Health and Social Care Bill (2011) through the legislative process.
Explaining processes of marginalisation: Logics approach and nodal framework
Rooted in post-Marxist discourse theory (Laclau and Mouffe, 1985), a logics approach to critical policy analysis affirms the fundamental assumption that all social relations are in a constitutive and dynamic relation with structured fields of meaning marked by radical contingency (Glynos and Howarth, 2007). In this view the foundations of society are in a crucial sense rhetorical since discursive elements and practices are regarded as fundamentally co-constitutive. Equivalences between discursive elements and groups can be drawn into sharp friend–enemy frontiers, just as differences can be foregrounded and mobilised to break down those frontiers. In this view any existing practice or regime is understood as a product of discursively-inflected hegemonic struggles in which political, normative, and ideological dimensions are always in play. In focusing on the policy arena we draw particularly on the explanatory units of social, political, and fantasmatic logics (Glynos and Howarth, 2007) to contribute to this broader project of understanding the character and evolution of the hegemonic struggle over health care provision and delivery in the UK. In this approach, social logics help us characterise a practice or regime in terms of its dominant norms, political logics help us characterise those processes that tend to contest, de-contest, defend or transform those norms, and fantasmatic logics aim to capture the energy with which social norms retain their grip or, alternatively, are contested and transformed. The reference to fantasmatic logics indexes a concerted effort to supplement existing approaches to critical policy analysis with conceptual resources drawn from psychoanalytic theory (see also Fotaki, 2010 and Hoggett, 2006).
A stylised example drawn from health care may help draw out the character of these three types of logic and their potentially complex inter-meshing and mutually supportive relations. Consider the social logic of care, which rests on processes of negotiation, attunement, and adaptation between patient and health care professional, and in which any will to choice is trumped by the practical constraints of disease and the body’s unpredictable responses (Mol, 2008). Imagine also a different logic of health care – a social logic of choice – in which the relationship between patient and professional is understood predominantly via individual choice and market calculation. These competing logics can find expression in different material practices: while various practices of consumption and consumer research conform to a logic of choice, practices of experimentation, listening patiently to users, and adjusting advice iteratively through processes of trial and error might embody a logic of care. In normal periods, one or another of these social logics will dominate and its associated social practices will largely be taken for granted. In periods of transition, however, differences between these social logics are brought into relief, sometimes more, sometimes less, consciously.
Political logics make sense against this background, and may play themselves out in any number of modes. For example, in the mode of contestation (‘choice versus care’) a political logic that takes its bearing from the logic of choice may come to unseat the dominant logic of care. According to the logics approach, however, the efficacy of a given political logic rests not only on its normative valence (e.g., logics of choice and calculation are seen as better suited to the delivery of health care), but also on its capacity to mobilise affective attachments (its ideological valence). Here the nature and form of narratives become of key interest. What is promised and what is portended? In our illustrative example, a logic of choice has clear fantasmatic appeals: it can draw on the long-standing promise of individual self-determination and self-sufficiency, pitting itself against the image of the National Health Service (NHS) as an authoritarian, resource-hungry, bureaucratic Leviathan.
Although in practice social, political, and fantasmatic logics are all operative at any one time, each being in a relation of over-determination with the others, it is often useful to foreground the role of one type of logic to help sharpen the analysis. Accordingly, in this paper we foreground integrated care as a political logic that operates in such a way as to marginalise critiques of the government’s imagined pro-competitive policy reform proposals. Nevertheless, in order to adapt the above-described logics approach to the critical analysis of this policy reform process, we have found it helpful, as a first step, to draw a distinction between social logics and projected social logics. Technically, social logic are meant to capture the patterns of self-interpretations of subjects engaged in a concrete practice. Logics of care and attunement might capture the way health professionals understand their relation to users, but they also help characterise the way they interact with one another. Social logics embody certain norms of behaviour, and for this reason we often use the terms social logic and norm interchangeably. However, when it comes to policy reform, the focus of analysis is not health practices as such, but rather ‘imagined alternative practices’. For this reason, then, we tend to talk about ‘projected’ social logics since, strictly speaking, these social logics or norms of behaviour have not yet been materialised in concrete practices (see Figure 1).

The arena of public discourse.
Drawing a distinction between social logics and projected social logics helps us better understand the political and ideological significance of instances of contestation and non-contestation in the reform process. As is suggested in Figure 1, we use the distinction to devise a research strategy that focuses on elite policy discourse and debates, tracking the health and social care reform process through a series of critical interventions taking place at key moments which we will briefly outline in the next section: firstly, the initial responses to the White Paper and opposition to the Health and Social Care Bill; and secondly, the ‘listening exercise’ and subsequent work of the Future Forum. By elite discourse we simply mean to capture the discursive utterances of actors occupying positions within the formal policy-making orbit, including governmental, party-political, think-tank, campaign group, and broadsheet productions. Popular discourse, by contrast, would denote a series of discursive productions by actors acting outside this orbit or acting in an informal capacity, and would invariably comprise a rich source of fantasmatic narratives and investments that help account for the inertia of existing regimes or the energy with which regimes undergo transformation (for a particularly insightful discussion of this relation in the context of health care policy in a choice regime, see Fotaki, 2010).
In terms of our methodological tactics, we have focused our analysis around a small set of key policy-making actors, in particular the King’s Fund, the Nuffield Trust, and the Future Forum, as well as the government itself. It is important to stress here that while we focus on the discursive productions of these prominent actors, it is not their specific interests and objectives that interest us so much as the logics they project, and the political logics of marginalisation evident in their discursive productions. In other words, in this paper we are interested primarily in the overall pattern or effects of a series of interventions by a range of agencies rather than their underlying motivations. As we will go on to show, we argue that rhetorical strategies combined in complex ways around the trope of integration to produce sufficient consensus to forestall revolt against the main thrust of the proposed health and social care reforms.
However, in order to better understand how exactly the integration imperative can be understood as a master political logic that has marginalised more radical critiques and alternative visions of the provision of health and social care, we supplement the above-described logics approach with an analytical framework that identifies four nodes along the health and social care service chain: provision, distribution, delivery, and governance (drawing on Glynos and Speed, 2012) (see Figure 2).
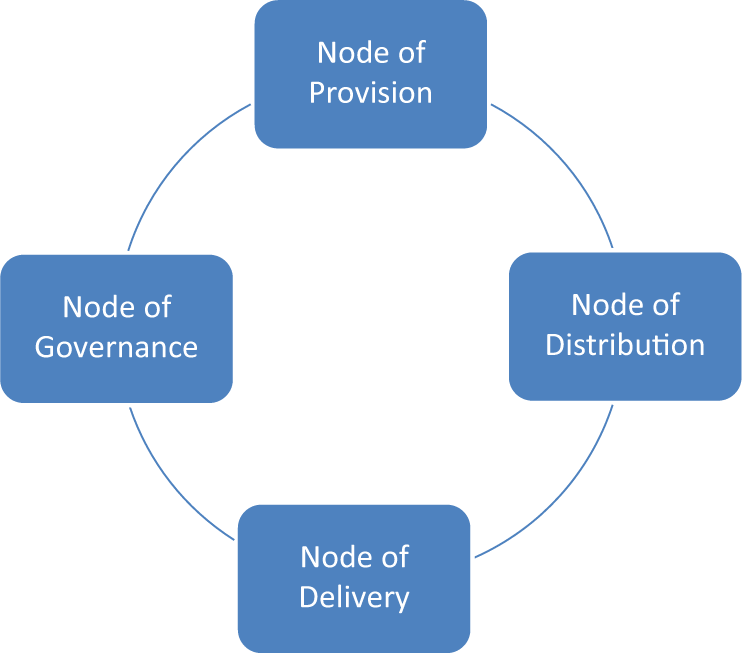
Nodes along the health care service chain.
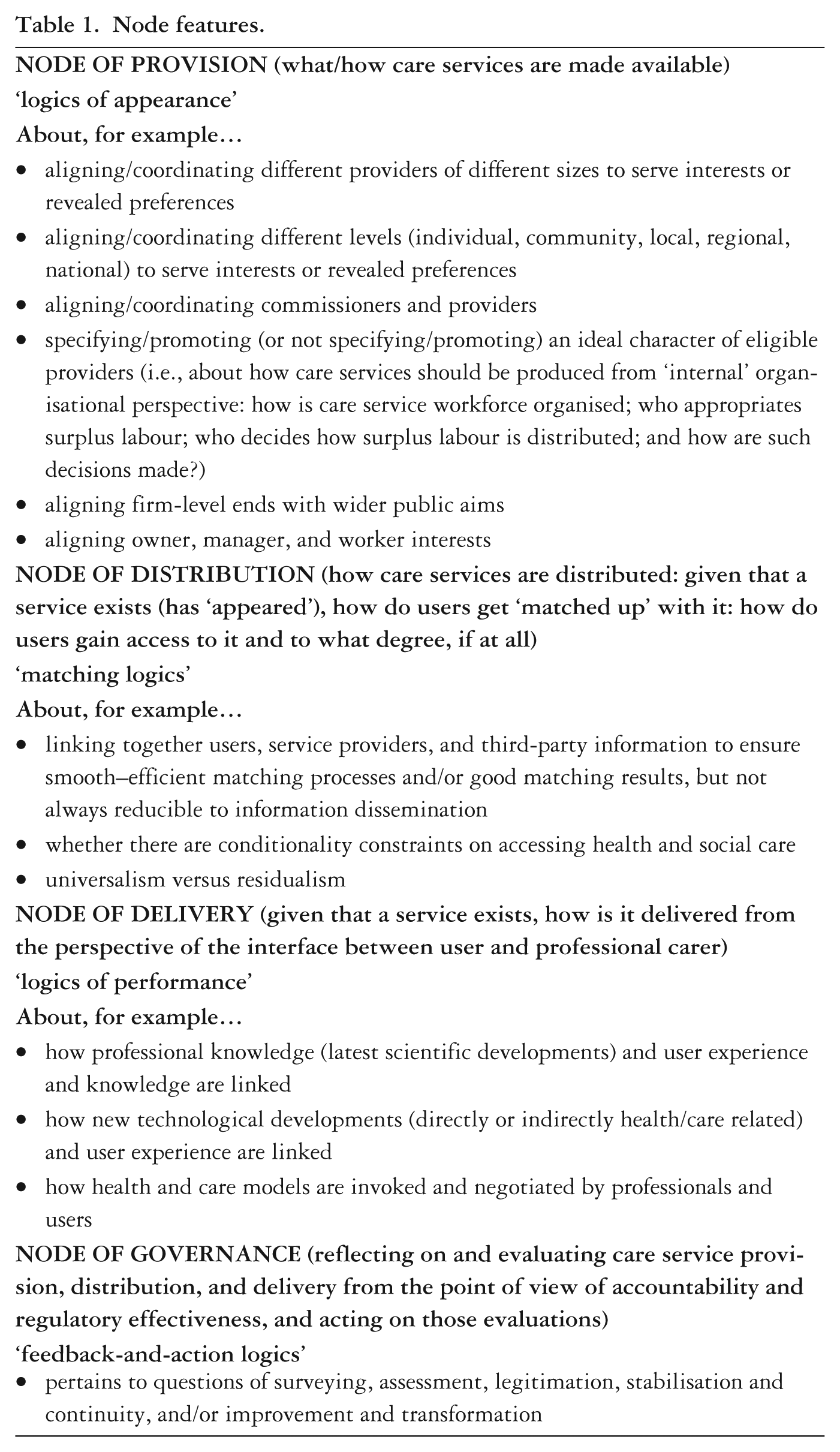
We can now be more precise about the role particular social logics (or projected social logics) play because we can situate them in relation to particular nodes along the whole service chain. Each node foregrounds distinct sets of questions and concerns regarding service reform. The node of provision is largely about which services need to be provided and the conditions under which such provision can be instituted, the node of distribution is about how users find out about such services and their conditions of access (e.g., universal access, co-payments, etc.), the node of delivery is about the norms that shape the relationship between health professionals and users (e.g., concerning the treatment process, the exchange of knowledge, the role of technology, etc.), and the node of governance is about how the norms characterising the node-specific practices are evaluated, maintained, or transformed (see Table 1 for a more complete sketch of this range of emphases).
Node features.
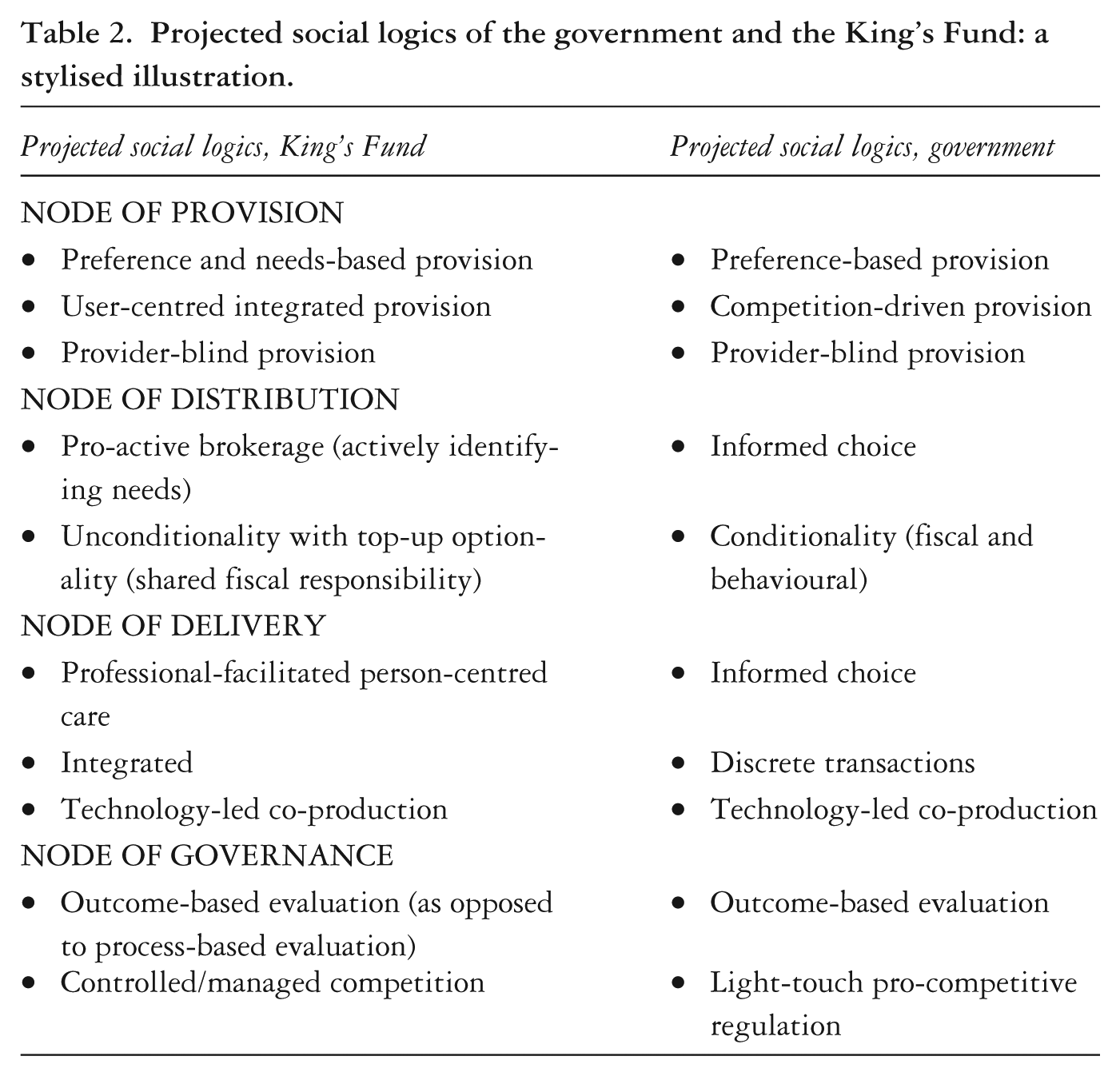
The benefit of this nodal framework is that it allows us to distribute identified social logics across the nodes depending on which are more relevant to our analytical focus, and enabling us, in particular, to be much more precise about the norms in relation to which one can understand logics of marginalisation. Table 2 offers a stylised illustration of what such a set of projected social logics might look like as a function of nodes.
Projected social logics of the government and the King’s Fund: a stylised illustration.
In this paper, however, our analysis centres on the node of provision, giving our analysis of the documents from the government, the King’s Fund and the Nuffield Trust a clear focus. We read these documents with the following question in mind: what do these documents have to say about existing (or projected) norms with which service provision is (or can be) organised?
The development of this nodal framework helps us better understand the marginalisation process in terms of political logics. This is because the sense and significance of qualifying a logic as political emerges only in relation to particular norms embodied in identified social logics. Political logics marginalise efforts to contest and debate norms that many consider worthy of contestation, and as we will see later, a key norm we identify as worthy of contestation is embodied in what we term the social logic of provider-blind provision: the idea that our decision to choose a service should be governed by its capacity to provide a good service, not the type of provider-organisation offering that service. This enables us to see how the discourse of the King’s Fund and the Nuffield Trust, while not wholly uncritical of government policy, nonetheless works very much with the grain of official discourse – that health care reform in the UK demands we create opportunities for a wide range of organisations to provide services under conditions of formal equality. The integration imperative appears as a master political logic because its invocation has tended to pre-empt or narrow the scope of debate around the contestation of the provider-blind norm in the node of provision; and that this, in turn, is because integration has been understood predominantly through the wider hegemonic discourse of choice (as opposed to ‘care’, for example).
In what follows we situate the integration imperative in a wider discursive terrain, particularly the regime of market choice, in order to better understand the political and ideological significance of instances of contestation and non-contestation in the reform process. To anticipate briefly, we could say that the regime of choice places the user at the centre of health and social care and, in this view, choice is understood to be motivated by the prospect of users’ preference satisfaction and materialised via discrete transactions. We begin, however, with a brief overview of the health and social care reform process.
A brief sketch of the health and social care reform process
On 9 May 2010 an agreement was reached between the Conservative Party and the Liberal Democrat Party to form a coalition for the next UK parliamentary term. Neither party had an electoral mandate for restructuring the National Health Service. Indeed, part of the Coalition agreement was an explicit statement that there would be no more top-down restructuring of the NHS. Yet, just a few months later, in October, the then Conservative Secretary of State for Health and Social Care, Andrew Lansley, had produced a complete White Paper detailing what have come to be labelled the most far-reaching reforms of the National Health Service in its sixty-five year history (DH, 2010; Timmins, 2012). The Secretary of State for Health and Social Care was clearly keen to press ahead with reform, immediately implementing what he could without primary legislation (such as the re-organisation of Primary Care Trusts and the Strategic Health Authorities [Timmins, 2012]), whilst also seeking to lock key elements of the reform into statute – the removal of the state from day to day management of the NHS, the introduction of general practitioner commissioning, and the fashioning of a new regulatory panoply (Speed and Gabe, 2013). However, dissent quickly arose. The Health and Social Care Bill was introduced to the House of Commons in January 2011, but its passage through Parliament was far from smooth. In March 2011, the largest doctors’ union, the British Medical Association (BMA) called for the Bill to be scrapped, and in early April the government announced an almost unprecedented ‘listening exercise’ – a ‘pause’ in the legislative process – to allow the government to ‘listen, reflect and improve’ (Hawkes, 2011) the proposals. This would enable the Prime Minister and the Secretary of State ‘time to try to find compromise amendments’ (Leys and Player, 2011: 70) and to enable them to demonstrate they had listened to public and professional opinions (Leys and Player, 2011).
As part of this ‘listening exercise’, the NHS Future Forum was set up to investigate proposed reforms and consult widely and then report back to the Secretary of State – a forum largely sympathetic to the general direction of the reforms (Timmins, 2012). One key theme it was asked to probe was ‘the role of choice and competition [could play] for improving quality’ (DH, 2011). Choice and competition were the central elements of Lansley’s ambition to create a self-regulating health service: market-based incentives would be set in train and Monitor, as the arm’s length statutory regulator, would ensure that commissioning decisions respected the competition imperative, obviating the need for the government to be involved in the day to day management of the NHS. Giving up on choice and competition would have meant abandoning the reform project of self-regulation and the idea of a ‘restructuring to end all restructuring’. Although the twin ideals of choice and competition were already present in the NHS before Lansley’s reforms, elevating competition to the status of regulatory principle was always bound to be controversial. Something was needed to lend legitimacy to this reform. In our view, the appeal to integration forms a key part of this story, and in order to appreciate the rhetorical and political role integration played during the ‘pause’, we turn to the initial reactions to the White Paper and Bill.
First reactions to the White Paper and Bill: Competition, fragmentation, and the promise of integration
The reforms outlined in the White Paper can be understood to further institute and deepen a liberalisation and marketisation trend set in motion during the Thatcher and New Labour eras, resonating with ideas like the ‘provider/purchaser split’ and the ‘third way’. It is clear, however, that important though competition was to New Labour, the White Paper and Bill made competition, and the accompanying notion of ‘any willing provider’, the cardinal organising principle of reform. Competition would – via the ‘any willing provider’ stipulation – ensure that user choice would be maximised at most levels and sectors of health care:
Our aim is to free up provision of healthcare, so that in most sectors of care, any willing provider can provide services, giving patients greater choice and ensuring effective competition stimulates innovation and improvements, and increases productivity within a social market. (DH, 2010: 37)
A clear but rather familiar frontier was being rhetorically constructed, separating the efficiency of market competition in generating choice for the user on the one hand, from the inefficiencies of state provision and unaccountable medical professionals on the other hand. Market competition would unleash creativity and innovation and thereby increase productivity. It would also maximise efficiencies for the taxpayer and multiply choices for the user. But the reaction to the White Paper and Bill was both swift and direct. The renewed boost to the competition imperative and the introduction of ‘any willing provider’ into the lexicon of health care reform raised the spectre of privatisation, and associated fears of disintegration, fragmentation, and a general undermining of cooperation and quality of services in many areas of health care.
The NHS Support Federation (2010), a campaign group aimed at ‘protecting and promoting the founding principles of the NHS’, criticised the ‘flawed vision’ of the market-based model. Fragmentation was seen in terms of a diminishing capacity to pool risks, as providers would compete against each other for the most ‘lucrative’ services and seek to divest the most costly. Health Emergency (2010: 1), another campaigning organisation, voiced concerns about ‘the fragmentation and privatisation of the NHS’ and the promise of ‘£20 billion of spending cuts by 2014’. Similarly, the NHS Consultants Association (NCA), together with Keep Our NHS Public (KONP), were instrumental in organising a letter from the BMA to the Times and Financial Times newspapers, dated 13 December 2010:
BMA policy is to uphold the founding principles of the NHS (which are held dear by British citizens) that health care should be on the basis of public provision not private ownership, co-operation not competition, integration not fragmentation and public service not private profits. Four out of five doctors believe the reforms will not benefit patients. (http://abetternhs.wordpress.com/2010/12/13/letters-to-times-and-financial-times/)
Formal consultation on the White Paper closed in October 2010 and despite widespread objections, the Health and Social Care Bill was introduced to the House of Commons in January 2011. Opposition from professional groups continued to mount, however, and the highly influential British Medical Journal published a roundup of concerns related to the Bill (BMJ, 2011b). These included worries expressed by the Royal College of General Practitioners and the Royal College of Physicians among others, linked to ‘fragmentation and unnecessary duplication’, threats to ‘quality of service’, and the spectre of ‘less choice and fewer services’ as well as ‘increase[d] bureaucratic costs’ (BMJ, 2011b). The BMA was especially worried about how ‘[f]orcing commissioners of care to tender contracts to any willing provider … could … allow large commercial companies to enter the NHS market and chase the most profitable contracts, using their size to undercut on price, which could ultimately damage local services’ (BMJ, 2011b).
These responses show how, early on, there was a clear and vocal effort to contest moves to turn competition (and the accompanying notion of ‘any willing provider’) into a master principle with which to organise the provision of health care services in the NHS. Advocate organisations marshalled a series of rhetorical and political logics aiming to break down the equivalence between competition, efficiency, and maximisation of choice, instead constructing a different equivalential frontier linking competition and fragmentation. Drawing on precisely these rhetorical logics, the Labour shadow health spokesman Andy Burnham, speaking at a fringe meeting of the Labour Party Conference in the autumn of 2012, dubbed the reforms as ‘the fast track to fragmentation’ (The Guardian, 3 October, 2012). Already, however, the idea of integration was emerging as a master counter-principle to affirm in quelling worries associated with the competition imperative. While the Coalition’s proposals for reform were seen as risking fragmentation, integration was now widely understood to be ‘the thing that was needed’ and ‘the thing that must be protected’. 1
The contestation of competition was thus forcefully and overwhelmingly established by linking competition to the spectre of fragmentation. It was unclear, however, whether competition was necessarily incompatible with integration. Much would depend on the meaning attributed to integration. However, beyond its possible concrete meanings, we wish to emphasise how integration functioned as a term that attracted high levels of affective investment and allegiance in the wider domain of public discourse, largely on account of its ‘empty’ oppositional status (it is clearly against fragmentation, but it is less clear what it stands for more positively and concretely). Nevertheless, as we will see now, a logic of compatibilisation was available for rhetorical deployment by a number of policy-making actors in the domain of policy discourse.
Responses to the initial reactions: Competition serves integration
Given the mounting opposition to the Bill, an almost unprecedented halt in the legislative process was called in April 2011. Here we focus on the government-endorsed responses issued through the Future Forum reports. Given the frontier now separating competition and integration and the emerging rhetoric of ‘competition versus integration’, the task facing supporters of the pro-competition reforms was to render these compatible. But how exactly? As Leys and Arnold (2011) point out, there is nothing intrinsic to the idea of integrated health care that suggests a need for competition. Integration is fundamentally about coordination and planning (Leys and Arnold, 2011), and perhaps this is why the trope of competition versus integration resonated so powerfully. The job of rendering the two compatible, whether knowingly or not, fell to the Future Forum.
As indicated earlier, one of the Future Forum’s key remits was to publish a formal report on the controversial topic of choice and competition (Future Forum, 2011b). That controversy, as we have discussed, tended to centre on the fragmentation that competition would produce, but the Forum had no specific instructions to examine integration as such. It nonetheless commissioned a joint report on integration in health and social care from the King’s Fund and the Nuffield Trust (Goodwin et al., 2012) – both highly influential health think tanks (see Shaw et al., 2014) – which was published in January 2012. The King’s Fund in particular, under its Chief Executive, Professor Chris Ham, had already produced a considerable body of work on integration. Thus, as integration was already a key concept in the work of the King’s Fund and the Nuffield Trust, the legislative ‘pause’ served as an opportunity to remobilise the concept to allay fears of fragmentation.
Here we focus on a corpus of texts centred on the King’s Fund/Nuffield Trust/Future Forum nexus. One report in particular, Curry and Ham (2010), is liberally cited in both the King’s Fund/Nuffield commissioned report (Goodwin et al., 2012) and the Future Forum’s later survey (2012) of integration across English health and social care, this intertextual-citational feature making it worthy of special focus. The report is technical in tone, seeking to clarify the many meanings of integration and the various levels in the health care system at which it operates (macro, meso, micro), but it also has political import in that it places the theme of integration on an equal footing with, in its view, the ‘even greater emphasis being placed on choice and competition’ since the change of government (Curry and Ham, 2010: 1). For the King’s Fund, it was not so much that choice and competition were problematic, but that the government’s view of unfettered competition needed to give way to a more ‘nuanced debate about the direction of reform that recognises the possibility of integration and competition both having a part to play in improving performance’ (Curry and Ham, 2010: 1). Having taken issue throughout the report with the government’s vision of commission-led competition, the authors seek common ground with the government on the centrality of patient choice in articulating what (from a patient’s perspective) is a very attractive vision of future health care:
If competition between clinically integrated systems evolves in England, patients would choose both their practice and the consortium that commissions their care. They would also have choice within the integrated provider network or networks under contract to the consortium. In addition, patients could be offered the choice of specialist providers outside these networks to create an incentive for network providers to offer care that is responsive and high quality. (Curry and Ham, 2010: 46)
Competition and patient choice were thus not ruled out. It was, rather, a matter of educating the government on the difference between the means and the ends of competition. In their view, competition can and should be put in the service of integration. Thus, ‘competition between integrated systems is likely to be more effective … than competition between fragmented systems’ (Curry and Ham, 2010: 46).
The Future Forum’s report on choice and competition, for its part, was more bullish on the question of the compatibility of competition and integration. It states:
We have … heard many people saying that competition and integration are opposing forces. We believe this is a false dichotomy. Integrated care is vital, and competition can and should be used by commissioners as a powerful tool to drive this for patients. (Future Forum, 2011a: 6)
This is reiterated in the Forum’s final summary report (Future Forum, 2011b) presented to the government on 13 June 2011. Its broad conclusion is that while the provisions of the 2012 Health and Social Care Act need to make the objective of integrated care explicit, there is no necessary or inevitable incompatibility between integration and competition. Competition must be managed to avoid the worst excesses of ‘cherry picking’ and market dominance (see Future Forum, 2011a: 5–6, section on ‘managed competition’), but is, in fact, necessary for integration and, indeed, for the very survival of the NHS (Future Forum, 2011b: 25). Its recommendation was that Monitor take its primary duty to be not the promotion of competition, but rather the safeguarding of ‘the best care for patients’ through ‘the delivery of integrated care’ (Future Forum, 2011b: 25).
In this way, the Future Forum corpus brought a degree of discursive closure on the question of the role and place of competition in the health and social care reforms. But it did not convince everybody. Julian Le Grand, Tony Blair’s former choice tsar, and Alan Millburn, former Blairite health secretary, were concerned that this change of emphasis would weaken the competition imperative (Timmins, 2012). But there were still plenty of misgivings in the opposite direction – that untrammelled competition would reign and that more needed to be done to protect and promote integration (expressed, notably, by some of the Royal Colleges and the BMA).
The report from Goodwin et al. (2012), commissioned by the Future Forum and following a series of workshops on integration in the October and November of 2011, proceeds with studied caution on the question of the compatibility of competition and integration. It argues:
choice and competition policy … appears at times to run contrary to the desire in many sites for more integrated care (Ham and Smith 2010). The key issue here is the unit of competition and whether this is defined narrowly (eg, for an annual foot check) or broadly (eg, for a year of care to a diabetic). It also begs the question as to how competition should operate – should it be competition for the market (ie, tendering to providers) or within the market (ie, patient choice of location and caregiver). (Goodwin et al., 2012: 8, emphasis in the original)
The question of ‘the right unit of competition’ is not answered but, as with the earlier King’s Fund report (Curry and Ham, 2010), we are left in no doubt that, provided that the end is integrated care, there ought to be choice and competition. 2
Indeed a further Future Forum report, instigated during a second phase of ‘the listening exercise’ reinforced the compatibilising logic that makes competition serve integrated care via the rhetoric of choice. An emblematic figure stalks this report – a fictitious octogenarian – ‘Mrs Crabtree from number 3’ – and it is on her outcomes (along with others – Jim and Ben and his mum) that we are entreated to focus. This figurative device leads on to the assertion that patients know best what their everyday needs are and that the choices they make can drive efficiencies through competitively structured systems and thereby ensure integrated outcomes (Future Forum, 2012: 15).
In a series of rhetorical moves, then, integration was elevated to the status of overriding objective of the NHS and competition had come to be seen as essential to its realisation. If the rhetoric of reaction analysed earlier can be characterised in terms of ‘Integration versus Competition’, we have now shown how a compatibilising rhetoric enabled the response ‘Competition serves Integration’. Rendering integration and competition compatible was made possible through an appeal to choice: competition is about choice (the choice of commissioners, but ultimately the choice of users), but integration is also about choice (the user can choose the best integrated package of care, or can herself construct-integrate a bespoke package of care). In other words, competition and integration are rendered compatible by situating both within a regime of choice. What we see is the operation of a compatibilising rhetoric of choice. Competition and integration are no longer seen as opposites, but allies in the fight to pull the NHS back from the brink of collapse. Moreover, competition now appears to have acquired a clearer rationale that was arguably lacking in Lansley’s White Paper.
The rise of integration to an overarching imperative has served to mobilise and organise a range of moves and logics, of which the compatibilising rhetoric of choice was one of the most energetically performed. What is not clear, however, is how and why we should understand the appeal to integrated care and the compatibilising rhetoric of choice as a specifically political logic. In order to appreciate why, we need to return to our earlier discussion of social logics, more specifically the norms that they embody and that we consider worth contesting.
Integrated care as a political logic: On the contestability of provider-blind provision, and the critical potential of provider pluralism
Integrated care can be conceptualised in concrete terms as a particular vision, which – in turn – we can understand as a function of the different nodes along the service chain. In relation to the node of provision, this might appear as a way of coordinating different providers to serve the interests (or revealed preferences) of users and the public at large, for example by aligning firm-level ends with wider public aims, including allowing commissioners to be providers themselves under certain conditions. Lansley’s idea of a self-regulating system offers one such vision of integration – a vision that relies heavily on competition, information dissemination, and user choice, to do this coordinating work. In the node of distribution, integration might appear as a way of linking together users, service providers, and third-party information to ensure that users are well-matched with services. In the node of delivery, integration might appear in the different ways professional, scientific, and technological developments and knowledge are integrated to enhance user experience, particularly in complex needs cases where issues of health and social care over-determine one another. In relation to the node of governance, integration can refer to the way the evaluation of service provision, distribution, and delivery informs and lends legitimacy to ongoing practices and their transformation.
But integrated care need not be understood only in terms of a concrete vision. We have thus emphasised how integration also functioned as a site of affective investment and source of hope, particularly when set against the spectre of fragmentation. Here integration can be understood as an ‘empty’ signifier – that is ambiguous as to its content. We argue, however, that we can also understand the appeal to integrated care as a political logic. In order to transform our understanding of the integration imperative and its associated choice-based compatibilising logic from rhetorical device to political logic, it is essential to bring it into explicit relation with a norm (or norms) we consider worthy of contestation (or defence). The political dimension of the rhetoric of integration appears against this background, because it is only with reference to the contestability of one or another projected social logic that we can identify its political role in instituting, defending, or – in this case – pre-emptively marginalising processes of contestation and critique. Since the focus of our textual analysis so far has been on the node of provision, we will consider the projected social logics of this node in more detail, the norm of provider-blind provision in particular.
As noted earlier the node of provision is organised around the question of how services – here health services – appear on the scene. We can begin by focusing on a key problem outlined in the White Paper: the lack of good quality services in some areas and a lack of innovation and efficiency. One-size-fits-all state monopoly provision is seen as inefficient, delivering poor results. This leads to the argument that there should be a much wider range of firms providing services, since different organisational structures may work better than others to quality and efficiency standards in different times and environments (DH, 2010). The White Paper’s projected social logics in the node of provision tend to take their cue from the preferences revealed in potential user choices, and in this context competition among ‘any willing providers’ holds out the hope of dispensing with government interference in the affairs of the NHS.
But the government was not alone in problematising the social logic of monopoly state provision and regulation. The King’s Fund’s projected social logics in the node of provision also take their cue from potential user preferences, but extend their scope to include potential user needs. In this view competition must be structured so as to be sensitive to these needs too. According to the King’s Fund, the solution is to be found in integrating services around the needs of the patient and striking a balance between competition and planning. However, and crucially, it need not necessarily be the state doing the planning since this could be contracted out to independent integrated care providers: ‘integrated care organisations could be in the vanguard of the … innovations needed to improve performance, especially if there is competition among integrated care organisations’ (Curry and Ham, 2010: 1).
A key projected norm we have thus identified across both the White Paper and the King’s Fund report, is what we have termed a social logic of provider-blind provision: the idea that our decision to choose a service provider should be governed by the organisation’s capacity to provide a good service, not the type of organisation offering that service. While this finds itself expressed as ‘any willing provider’ in the White Paper, we could say that the idea of ‘any willing integrated care provider’ can express the equivalent King’s Fund view. For neither is it any longer a case of the state being default monopoly or dominant provider. We have named this social logic provider-blind provision because it makes more explicit the steer given to commissioners to treat all contenders as formally equal in the competitive bidding process: commissioners are supposed to be ‘blind’ as to contenders’ size or internal organisational structure, caring only about the quality of services they promise to provide. 3
Our argument is that the political dimension of the master logic of integration can be appreciated when it is understood in relation to a norm considered worthy of contestation and/or defence. Once we have a fix on norms worthy of contestation, tactics and strategies can be qualified as political logics in relation to them. Integrated care and the accompanying compatibilising rhetoric of choice can thus be understood as a political logic because it naturalises the social logic of provider-blind provision and marginalises or pre-empts efforts to open up for serious debate and discussion a series of questions linked to this norm.
The most obvious question raised by the emphasis placed on provider-blind provision can be evoked by contrasting it with a possible alternative social logic: provider pluralism. It is, of course, true that official government documents, the Future Forum reports, as well as the King’s Fund and Nuffield Trust papers, talk about the virtues of pluralism. The Future Forum report on integration devotes a section to the need to ‘[f]ree up voluntary and community sector organisations’ (Future Forum, 2012: 27), noting the ‘widespread support for expanding the role of voluntary and community sector organisations in designing pathways and providing services’ (2012: 27). The King’s Fund/Nuffield Trust report, for its part, acknowledges the role that the independent and community sectors can play in ‘developing new models of care’ (Goodwin et al., 2012: 2). The Future Forum’s report on Choice and Competition also talks of the need to ‘promote a diversity of providers’ (Future Forum, 2011a: 9). What is notable across all documents, however, is the rather considerable faith placed on choice-based competition among willing providers to deliver pluralism, particularly in the government-sponsored Future Forum reports. There is little to no guidance on how integrated health care systems can be oriented towards provider pluralism, nor do the Future Forum’s recommendations indicate how Monitor might maintain or promote provider pluralism in the application of competition rules.
What is striking, therefore, is the absence of serious and sustained scrutiny of an alternative norm organised around provider pluralism. If patterned state monopoly provision is the target of critiques coming from the government and from the King’s Fund and Nuffield Trust, the move to provider-blind provision appears to be too quick, missing out a whole spectrum of alternative patterned provision options, of which provider pluralism would be one. Of course, provider pluralism is patterned in the rather minimal sense that a broad ecology of providers would need to be actively monitored and maintained to avoid the dominance of specific providers or types of providers. Yet when viewed from the perspective of even this ‘minimal’ alternative projected norm, provider-blind pluralism can appear uncomfortably silent along a number of dimensions:
the number of organisations that would make an adequate pool within which competition could properly take hold;
the range of organisation types that would make up a robust and resilient organisational ecology of providers;
whether specific organisation types should be championed in the delivery of health care (e.g., mutuals or cooperatives), or on the contrary, should be presumed to be unsuitable (e.g., for-profit organisations subject to the shareholder value imperative);
whether the system capacity to pool risks is protected from selective ‘cherry-picking’ tendencies;
the broader economic context and trends, elite networks, and power nexus within which particular organisations or types of organisations come to compete and operate in the existing and projected regime of health and social care. 4
The rationale for treating integrated care as a political logic should be clear now. Integrated care has certainly been given renewed impetus and status in the light of fears about unfettered competition in health care. In our reading, however, it functions as a political logic insofar as it reinforces, and pre-empts the contestation of, the norm of provider-blind provision. Taking our lead from the above-mentioned ‘silences’, we can be more specific about how appeals to integrated care and choice-based compatibilising logics push to the margins inquiries that might explore a further range of issues:
the justice of any one organisation’s economic process, particularly concerning the appropriation of surplus labour and workers’ capacity to shape the decisions of their organisation, including their working conditions;
whether the economic logics at the site of production/delivery are conducive to norms of good health and social care.
Drawing a distinction between provider-blind provision and provider pluralism opens up these sorts of questions to critical normative scrutiny, enabling us to draw productively on the work of a range of normative political theorists, critical political economists, and critical health care researchers. The sense and significance of integration, for example, may shift as we situate it in relation to regimes other than a choice regime: care, paternal care, or recognition, for example. Instead of placing the emphasis on the choice or preferences of the user, a regime of care might emphasise the good of the user as it is expressed and developed dialogically with health care workers; a regime of paternal care might emphasise the good of the user as judged by the state, the organisation, or by any one of a number of health professional bodies; and a regime of recognition might emphasise the good of the user and health worker.
What we have sought to do in this paper is explain how choice-based integrated care acts as a political logic to normalise provider-blind provision, obscuring wider contextual features linked to the landscape of power relations, hegemonic struggle, and ideological investments. When choice-based integrated care is allied with the norm of provider-blind provision, we can see that even the presentation of only non-profit exemplars of integrated care in the government’s White Paper and the Future Forum’s reports could be understood as a political logic. The appeal to non-profit organisations as privileged or paradigm illustrations deflects attention away from the considerable resources at the disposal of for-profit global health conglomerates. But, choice-based integration is also a master political logic, insofar as it gives a range of minor political logics a principle of articulation and suasive power, linking together what might otherwise appear as rather disparate elements: choice, personalisation, austerity, the demographic ‘time bomb’, or professionalisation. The political dimension of appeals to personalisation and choice-driven integrated care is also foregrounded when they serve to marginalise issues linked to the status, identity, and conditions of health and social care workers. But other rhetorical manoeuvres too can appear as political logics of marginalisation when viewed from the point of view of the projected social logic of provider-blind provision, for example, the often-repeated assertion by government that the pro-competition reforms were ‘merely’ the completion of a project instigated by the previous New Labour government. 5
Two final points are worth making. First, one key implication of this type of logics-cum-node analysis is that the intention of the parties involved is not essential to our capacity to characterise particular logics as political or not. Qualifying a logic as political serves as a critical device for identifying what discursive-rhetorical moves have political and ideological significance. Second, it is worth noting here that political logics are energised by fantasies operative at both policy level (e.g., market fantasies) and popular level (e.g., fantasies of personal independence and mastery). The persistence of integration as a long-standing and highly invested organising ideal in health care already attests to its fantasmatic appeal, but it is beyond the scope of this paper to explore the fantasmatic dimension of integration fully. Suffice to say that this is also key to its hegemonic grip: it mobilises anxieties linked to fragmentation and complexity in everyday life, but also holds out the promise of regaining control over our fate.
Concluding remarks
In the past, state monopoly provision was seen as a huge improvement over the previous regime in which there was no collective health insurance mechanism in place; but 60 years later, the NHS is faced with many modern challenges. We do not seek to deny those challenges, but only to point out how the present context has been problematised in such a way as to steer policy makers too quickly away from state monopoly provision to provider-blind provision. The quick move to a regime of choice-based competitive provision clearly leaves out other possible patterned forms of provision, particularly provision-pluralism. The move is also highly seductive because it resonates with wider discourses and fantasies linked to choice, autonomy, personalisation, independence, and the potential of telecare systems of care. Integrated care has worked as a master political logic of marginalisation in this move, and its success is partly due to its capacity to act as a master political logic or conduit through which a set of wider discourses and fantasies can play themselves out. The most troubling aspect of this political logic is the way crucial considerations are shuffled to the margins of substantive debate in both policy and media domains. It is thus important to bring fully into view how integrated care and its associated ‘minor’ political logics are (or are likely to be) performed in and outside the policy arena by key actors embedded in specific institutional and power networks. But it is not just that protecting the norm of provider-blind provision tends to direct attention away from broader ideological contexts and power dynamics. Just as important is the related tendency to not look too closely into the internal dynamics of organisations that seek to provide and deliver health services, particularly from the point of view of wider efforts to democratise the workplace.
Footnotes
Acknowledgements
We are grateful to anonymous reviewers for their helpful comments. We would also like to thank Sara Shaw and Gemma Hughes for their comments on earlier drafts of the paper. The thinking in terms of logics and nodes that underpins this paper is also part of a broader effort to develop this framework, and we would like to acknowledge Robin Klimecki and Hugh Willmott in this regard. All errors and omissions are our own.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Notes
Author biographies
![]() ), a blog on the sociology, economics and politics of health and health care. His current research explores the changing relations between citizen and state in the context of ongoing health and welfare reform.
), a blog on the sociology, economics and politics of health and health care. His current research explores the changing relations between citizen and state in the context of ongoing health and welfare reform.