
Abstract
Institutional births increased in India from 39% to 79% between 2005 and 2015. Drawing from 17 months of fieldwork, this article traces the shift from home to hospital births across three generations in a hamlet in Assam in Northeast India. Here, too, one finds that most births have shifted from home to hospital in less than a decade, aided by multiple factors. These include ‘free’ birthing facilities and financial incentives offered by government schemes, idiosyncratic changes within the hamlet, such as the introduction of biomedical practices through home births where oxytocin was used, and changes in cultural belief systems among local people. The exploration reveals significant transitions between (and fluidities of) categories such as local/global, tradition/modernity, past/present and nature/technology, creating a complex and ambivalent narrative of change, in which the voices of mothers should not be ignored.
Introduction
In recent decades, concerted efforts by state and non-state actors to improve maternal health outcomes in India have resulted in incentivising and improving access to institutional deliveries, ante-natal care and immunisations. The National Family and Health Survey (NFHS-4) of 2015 found that institutional births in India doubled from 39% to 79% between 2005 and 2015. In this context, we explore changes around birthing practices over several decades through narratives of older and younger mothers in a rural hamlet in Assam in Northeast India. We also map the trajectory of changing sites for birthing, situating this within an altered political economy where the state is increasingly visible in reproductive governance that goes beyond family planning to reduction of maternal and child mortality, in consonance with global discourses and indicators.
Older women in the study hamlet reported that about 60 years ago, births occurred with minimal interventions, gradually in the presence of a dai-ma [midwife] who administered oils and massages. In the 1990s, women in this hamlet began using the services of an informal health provider, who administered injections and saline drips to speed up births through oxytocin. We conjecture that this intermediary stage of change and local women’s prior use of injections and oxytocin made them more amenable to institutional births under the government’s National Rural Health Mission (NRHM) launched in 2005. The NRHM, renamed the National Health Mission in 2017, is among the largest state-funded health programmes in the world. Through its cadre of community health workers, called ASHAs (Accredited Social Health Activists), it encourages women to visit Primary Health Centres (PHCs) for ante-natal care, advice on institutional deliveries and immunisations. In 2005, the government also introduced a conditional cash transfer programme for ASHAs and mothers, Janani Suraksha Yojana, which provided financial incentives for institutional births.
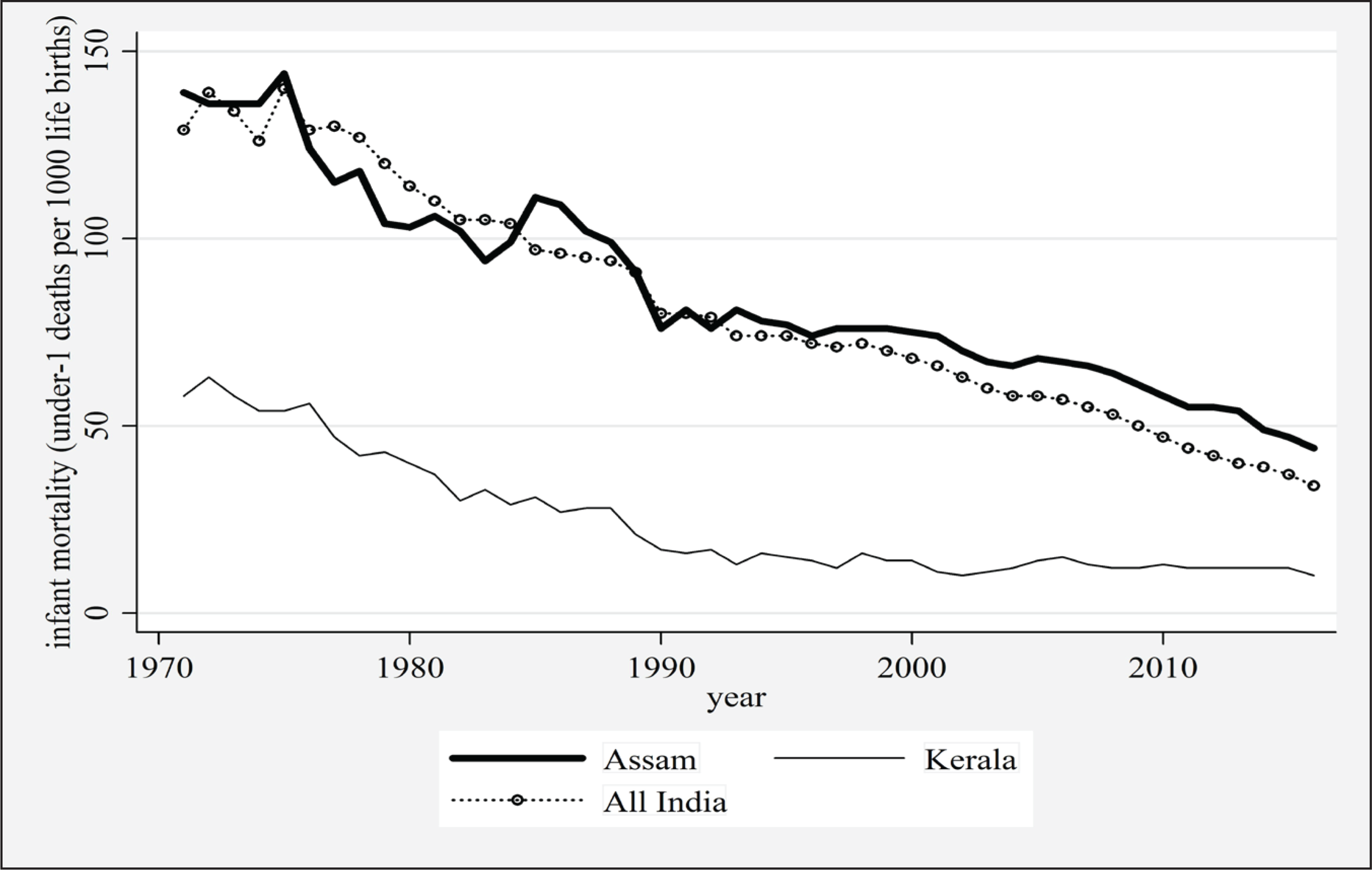
Assam provides an interesting backdrop to examine changing birthing sites because institutional births in this state more than tripled between 2005 and 2015, from 22% to 71%, with 60% of births occurring in state facilities. Assam’s mortality rate has significantly dropped in recent decades (Figure 1). Nonetheless, for the latest years for which data were available (2014–16), Assam still had the joint second highest infant mortality rate (IMR) in India, 44 out of 1,000, almost 30% higher than the country’s average of 34 out of 1,000, and over three times higher than Kerala, which at 10 per 1,000 births had the lowest IMR in India. Assam also had the highest maternal mortality rate (MMR) in India, at 237 per 100,000 births, almost double the figure for India (130 per 100,000) and almost five times more than Kerala, the state with the lowest MMR at 46 per 100,000. Several reasons, including terrain, the presence of historically disadvantaged tribal and religious minority groups and intra-state disparities in health infrastructure seem to explain this scenario in Assam.
Although institutional births are associated with reduced mortality rates (Campbell et al., 2006), there are concerns over access to care and abuse during childbirth in institutional contexts (Chattopadhyay et al., 2018; Devi & Kaur, 2020). A shift from home to institutions as the site of childbirth involves a paradigmatic change that shapes, and is also shaped by, cultural practices around birthing. Davis-Floyd (2017: 5) describes the underlying biomedicalisation as the continuing separation of ‘the individual into component parts, the process of reproduction into constituent elements, and experience of childbirth from the flow of life’. While some scholars argue that such changes efface women’s autonomy and make them passive receptacles of interventions that embody institutional power, others emphasise both the coercive and emancipatory dimensions of power underlying these changes (Unnithan, 2019: 71–9). We find that while biomedicine is attaining prominence, there continues to be active engagement with medical pluralism and non-allopathic approaches, using herbs, massages, special foods and rituals in the management of care during pregnancy, childbirth and the post-partum period (Withers et al., 2018), challenging the state-driven homogenising practices and discourses around biomedical interventions during childbirth.
This article begins with a short history of modern biomedicine and policy interventions around birthing in India, followed by a discussion of the literature on birthing practices and the role of informal healthcare providers who significantly shape pliancy towards biomedical interventions. Next, we present the methodology and details of the study site. Our findings are structured around three different ethnographic accounts that reference the ‘oils, oxytocin and obstetrics’ of the sub-title. The first is Bahagi’s narrative about home births without biomedical interventions. The second presents Kanchani and Bakuli, who had home births with oxytocin injections. The third features Junu and Rupali, who had biomedicalised, institutional births. The final section summarises the processes that have transformed childbirth from a cultural practice into a biomedically managed event. While the transitions may seem chronological, especially in our presentation, we acknowledge that this process is marked by multiple slippages, where the modern is not far from the traditional and the nature/technology split is never neat.
Historicising Practices and Policies on Childbirth in India
Three key issues emerge from our review of childbirth in colonial and early postcolonial India: place of birth, the disappearance of the traditional birth attendant or TBA (dai/dai-ma) and the role of (often) male informal health providers, who administer oxytocin injections to hasten births.
In pre-colonial India, births were private affairs that occurred at home, mostly facilitated by a traditional midwife (dai). Since the colonial period and extending to postcolonial times, increasing interventions modified these patterns along with subsequent vernacularisation of modern practices (Guha, 2018; Hodges, 2006; Mukharji, 2009; Qadeer, 1998). Colonial biomedical doctors and their postcolonial counterparts viewed dais as ‘dirty’, ‘unclean’ and ‘ignorant’, posing risks to mothers and neonates (Jeffery et al., 1989). Consequently, colonial-era interventions focused on ‘modernising’ healthcare practices, moving childbirth from dais to trained midwives and doctors, establishing ‘lying in’ hospitals through the Dufferin Fund, designing modern nursing and midwifery training courses and embedding rational, scientific and sanitary practices of allopathic medicine in Indian birthing practices. As these efforts found traction among many Indian reformers and upper-class Indians, slowly a dominant discourse privileging Western medicine emerged (Guha, 2018; Guha, 1998).
After independence, many women especially in rural areas, continued to have home births with the help of dais. Recognising this, in the 1940s, the government’s Bhore Committee recommended integration of dais into India’s nascent modern healthcare system. Nevertheless, as part of the major push for development planning after independence, policy gravitated towards Western medicine, with concerns over family planning crowding out concerns around childbirth practices and shaping reproductive reforms (Qadeer, 1998). With time, as part of the emerging development discourse, the focus has increasingly been on the safety of children and mothers, also with an eye on international indicators.
While institutional births increased, recent Indian childbirth reforms have projected hospitals as ‘safe’ sites for birthing instead of homes, recommended deliveries conducted by doctors rather than family members or TBAs, and offered prenatal care, particularly managing widespread anaemia through providing iron folic acid (IFA) supplements. Unsurprisingly, the second phase of India’s Reproductive and Child Health Programme excluded TBAs from birth reforms and stopped TBA training altogether (Saravanan et al., 2012; Sharma et al., 2013). Reforms favoured formally trained doctors and nurses through skilled birth attendant (SBA) training programmes, as well as increasing access to emergency obstetric care. However, it is not clear that health infrastructure has kept pace with this increased demand, that rights have been adequately safeguarded, or that there is either equity or quality in care during institutional childbirths (Chattopadhyay et al., 2018; Jungari et al., 2021). In Uttar Pradesh (UP), mistreatment and abusive behaviour, especially directed towards poor rural Muslim women, lack of privacy, hygiene and space in state hospitals are reported as major reasons why many women in rural UP still preferred home births (Devi & Kaur, 2020).
Further, in both home births by informal healthcare providers and in institutional births, oxytocin is used to speed up labour, which is dangerous if not monitored by specialists (Brhlikova et al., 2009; Iyengar et al., 2009; Sharma et al., 2013). The transition from TBAs and home deliveries to SBAs and hospitals has thus brought change that often translates into a more negative experience of childbirth. Iyengar et al. (2008) note that in rural Rajasthan, while the dai massaged the pregnant woman and provided an attentive birth experience, which included performing various ancillary tasks, nurses and doctors in hospitals took a ‘hands-off’ approach, asking women to bear down while pushing or simply administering oxytocin injections to augment labour. Longitudinal ethnographic studies from rural UP (Jeffery et al., 2007: 174) note the wide use of oxytocin in the 1990s by untrained male pharmacists and find greater oxytocin use among women with more education and higher socio-economic status, ‘suggesting that oxytocin was used less because of need and more because of ability to pay and an association with “modernity”’ (Jeffery et al., 2007: 174). These findings resonate with our study.
Regarding informal healthcare providers, within the ambit of biomedicine but outside formal public and private institutions with doctors, nurses and related personnel, there is a large class of non-institutional health providers officially categorised as Registered Medical Practitioners (RMPs). They are typically middle-aged men with little post-secondary education or formal training, although Devi & Kaur (2020: 371) also note the presence of women. Functioning outside the regulatory framework, they do not keep detailed records of medical interventions or payments and use kinship networks to set up private practices in medically underserved areas (George & Iyer, 2013; Nahar et al., 2016; Pinto, 2004). Despite their lack of recognised training and limited skills, RMPs play an important role where the formal health system is weak (Al Dahdah et al., 2018). They are popular because they are affordable, locally accessible and familiar to users (Nahar et al., 2016). RMPs are often called ‘English Doctors’ because they provide ‘allopathic’ care. Pinto (2004: 337) describes RMPs as neither ‘quacks’ nor legitimate doctors, but those who invent roles for themselves as medical authorities and representatives of development. They deliver babies, administer injections for abortions, issue hormonal pills for delaying periods and remove placental remains after childbirth. Jeffery and Jeffery (2008) note that in rural UP, folk methods, which were popular in the early 1980s, had mostly disappeared by the early 2000s. Male RMPs were called during prolonged labour by birthing women and their female kin to administer injections to ‘increase pain’ or contractions for faster deliveries. The presence of such a figure in our study hamlet suggests that pliancy towards biomedicine may have followed a similar trajectory.
Study Setting and Methodology
As noted, although MMR figures in Assam are still the highest in India, they have more than halved over a decade due to better ante-natal care and the expansion of institutional deliveries over the last few years. Our study is located in the hamlet of ‘Lalkhuti’ in Assam’s Kamrup region, where 90% of the population is rural. Lalkhuti has 99 households and approximately 500 individuals from the Karbi and Bodo communities, two of the larger indigenous groups in Assam (Andersen & Soren, 2015; Srikanth, 2014). The local primary occupation is farming, though some households have diversified to poultry and pig-rearing, combined with circular labour migration to other parts of India. The village has a government primary school and an early childcare centre (anganwadi). While Lalkhuti offers limited local employment, except for a pork processing plant supplying organic meat to Europe and North America, its relative proximity to the state capital Guwahati translates into potential job opportunities for youth. The village is well-connected to Guwahati through a national highway with a newly constructed 200-bed district hospital located in its vicinity, which was established just as we commenced fieldwork in December 2015.
Two research assistants trained in social sciences collected most of the data in conjunction with six visits of varying durations, ranging from three weeks to one week, by the authors, spread over about 17 months of fieldwork. The material presented here includes in-depth interviews and conversations with women and their families, doctors, nurses and ASHAs, as well as observations in health facilities. Interviews were conducted primarily in Assamese, with occasional use of Karbi language by older participants. They were transcribed and translated into English, coded using OpenCode 4.0 software, and analysed for emerging themes. The study was reviewed by the relevant ethics committee at the first author’s home institution. We secured written or oral informed consent from all participants, and all names have been anonymised to protect confidentiality.
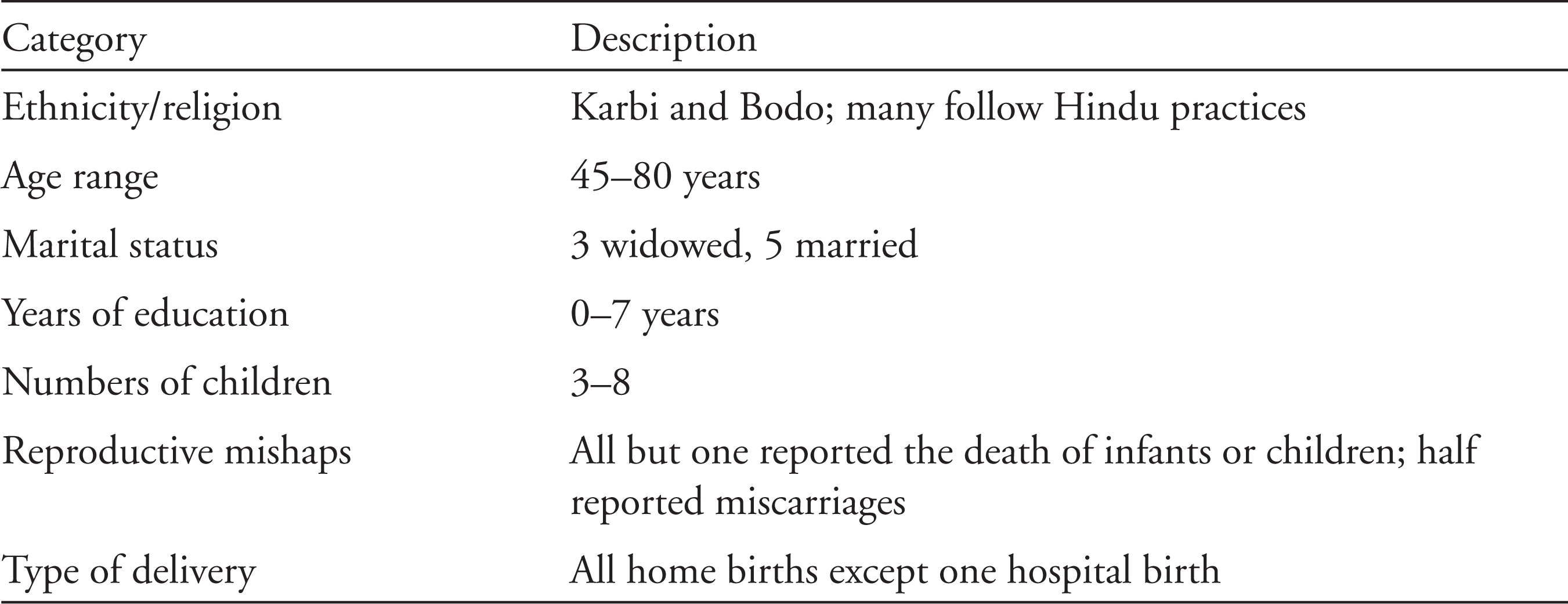
Initial fieldwork in 2015 focused on women who gave birth in 2013–15. Later fieldwork in 2017 focused on older women who had children in previous decades. We used snowball sampling to recruit women for multiple in-depth interviews. Data gathering techniques were informed by ethnographic and oral history methods, including repeat interviews with women (in private and sometimes with family members present), conversations with key informants such as ASHAs and anganwadi workers, and hanging out in the village with families. Table 1 presents a profile of our older participants. The majority of interviewees were Karbis, and two of the women were Bodos married to Karbis. There are nearly half a million Karbis in Assam, mostly residing in the autonomous Karbi Anglong district. Traditional Karbi religious beliefs are largely animist in nature. Illnesses are often believed to be supernatural in origin, and goats, pigs or fowls are sacrificed to ensure well-being, depending on the severity and nature of the illness. Births and deaths as important rites of passage are marked through animal sacrifices, even among families of younger women.
Participant Information
We also interviewed 24 younger women using snowball sampling in the first phase of our fieldwork. Most were first-time mothers and had an institutional birth by choice. These mothers constituted a mixed group of tribal, Hindu and Muslim women. Many had finished schooling and their characteristics reflect the current demographic profile of women in that cohort in the village. A detailed analysis of their experiences is found in Chattopadhyay et al. (2018).
Situating Births in Lalkhuti
Exploring changes in birthing practices through older women’s narratives and memories of giving birth, we have chosen five women, three older and two younger, to illustrate the arc of change. The oldest, Bahagi, had her births with no biomedical interventions, followed by Kanchani and Bakuli who had homebirths with the use of oxytocin, and lastly Junu and Rupali, who had starkly different experiences with modern obstetrics. The reproductive and life histories of the women narrated below help trace these changes and identify larger local, national and global forces that have shaped their lives.
Bahagi: Birth as a Rite of Passage with Little Intervention
Bahagi Kathar was a widowed Bodo grandmother [aita] in her late seventies, the oldest woman we interviewed. She lived with her eldest son, daughter-in-law and two grandchildren. Bahagi had six children, born about two years apart. Three of them died, two as adults and one as an infant. The experience of loss of infants and children characterises the narratives of seven of the eight older women in our study. The only woman who had not lost an infant was the youngest of the eight, suggesting that expanded immunisation and public health programmes reduced the once near-universal experience of this loss experienced by previous generations (Figure 1). Bahagi was less poor than other women in the hamlet and had access to some land, which she used to cultivate vegetables, but paddy cultivation was no longer the mainstay of the household economy as in the past.
In stark contrast to the younger women we interviewed, Bahagi had all her births at home. In some of her births, like others of her generation, she gave birth alone and used only village medicine or herbs [goalia oukhod]. She said that although her mother-in-law was present, she ‘did not take care of her’. In many parts of India, female kin such as the mother-in-law, sisters-in-law or fictive kin (close neighbours) often help during childbirth (Unnithan, 2019). Bahagi and two other respondents, both in their sixties, reported similar experiences of giving birth alone, using a strong string to cut off the umbilical cord. She said that women of her generation had the knowledge to take care of these things. Bahagi was afraid and suspicious of injections and had never used them. For her last two births, the dai-ma helped her eject the placenta.
Bahagi said that traditionally husbands would be called only once the child was born. The act of giving birth was considered not just ritually polluting, but also embarrassing for women, and they were responsible for washing bloodied clothes near a well [dong] the next day. For the first night, the mother and the baby used to stay alone. Bahagi was doubtful whether younger women today were capable of doing all that women of her generation did when giving birth, including having a very short post-partum period of rest. Iyengar et al. (2008: S27) report similar findings for rural Rajasthan, where older women thought that although a healthy young woman should have the ‘heat’ and strength [taakat] to deliver by herself without interventions, this was not the case anymore.
Kanchani and Bakuli: From Oil Massages to Oxytocin
Kanchani Rongson was a Bodo woman like Bahagi, married to a farmer. Aged about 50, Kanchani was much younger than Bahagi and had two daughters and one son. One of her daughters died in infancy, while the other died at the age of 12 from complications arising from jaundice, which the family suspected was because of negligence on the part of the hospital where she was admitted. Kanchani reported a life of extreme hard labour, with no opportunity to access even primary schooling. She also had multiple health complaints, which posed a great financial burden to the family.
Analysing Kanchani’s childbirth experiences suggests she belongs to that cohort of women who started off with minimal interventions such as oil massages by the dai and then graduated to home administration of oxytocin to speed up labour by Thulen, a male informal health provider with no formal medical training but addressed as ‘doctor’ by the older women. We learnt that for this generation of women, if they were in labour for 2–3 days, they would ask the dai-ma to help with the delivery and also remove placental remains. While there were some Western medical facilities, there was a stated cultural preference for home births. An informant who had all her births at home prior to 2005, and the establishment of NRHM, commented: ‘Yes, there was a doctor, a nurse, a medical facility. But they did not go to the doctor, because as people from the village they thought delivery is a normal process. So why would they go?’ She said there was no ASHA or auxiliary nurse midwife when she was pregnant. Kanchani had a second trimester miscarriage between the birth of her second and third child but did not take any medicines to expel the foetus.
Unlike Bahagi, Kanchani did not reject modern biomedicine and actually wondered whether her current poor health was because of lack of interventions like injections during pregnancy, which she believes is the norm now, as well as immunisation schedules for pregnant women or blood tests. During her first two pregnancies, there were no doctors or nurses that she could consult, although the village PHC was operational by the time her third baby was born. She said that only during her third pregnancy she was given injections on a monthly basis by the PHC nurse. When she asked Thulen to help during labour, he administered what appears to have been oxytocin to augment labour. She gave birth to a boy, her only surviving child.
In contrast to Bahagi, Kanchani believes that hospital births are a better choice for women because ‘they are well taken care of … they give injections and saline, and the baby is delivered properly’. Kanchani reported prolonged labour during each of her births and said that she suffered a lot. Initially, the dai-ma and her husband’s sisters had assisted her. Kanchani’s positive view of hospital births is built on an imagination of what hospitals births could be, in stark contrast to the frequent poor treatment that younger women reported while giving births in facilities. Despite her husband’s critique of the absence of doctors in the hospital, the high costs of medical care and his belief that biomedical intervention caused the premature death of their daughter, Kanchani feels that her health needs would have been better served by modern biomedicine. Perhaps her current state of poor health, rendered bearable by the miracles of modern biomedicine and the free care that she sees pregnant women receiving from the ASHA, may explain why she is more positively disposed towards biomedical interventions. Hospital births have certainly brought a decline in infant and maternal deaths. In our interviews with younger women, we found few instances of infant deaths and no accounts of maternal deaths.
Possibly, Kanchani’s positive view of biomedicine derives partly from the experience of her last childbirth. As noted, administration of oxytocin by individuals like Thulen is not uncommon. Thulen is a Karbi from Lalkhuti, related to some of the villagers. Although he has no formal medical education, he acquired some practical training in the military, enabling him to administer first-aid and give injections. After retiring from the military, he managed to accumulate enough wealth to build an ostentatious home in the village and also established a small medical shop in Lalkhuti. A divisive figure, his wealth and consequent arrogance was a source of friction and envy among his relatives.
We learned that until 8 years ago, Thulen had a more active practice, which changed when an elderly patient died under his care and the government became suspicious of his involvement in childbirth. Now his interventions were limited to providing medications (allopathic, ayurvedic and homeopathic) and massages when residents complained of aches and pains. During our interactions with him, he was prone to embellishing his claims of medical prowess to impress us, often in a state of intoxication, which made coherent conversations difficult. Much of what we learned about his involvement derives from directly speaking to him on occasions when he was sober, from our prolonged interactions with an ASHA who knew him well, and three women, including Kanchani, who had sought his help.
The younger women in our study had a clear preference for institutional births, supported by engagement of the local ASHA. None of the 24 younger women interviewed reported assistance by Thulen, despite two of them having accidental home births. Among our cohort of eight older respondents, three reported that Thulen had assisted with delivering babies during prolonged labour at their homes. Some women welcomed his interventions and giving a saline drip which hastened contractions and enabled them to deliver the baby more quickly, though painfully, while other women found his ways ‘rough’.
The use of oxytocin during childbirth requires a medical monitor that indicates maternal and foetal distress, careful calibration of dosage and hourly pelvic exams to prevent uterine rupture through over-stimulation (Brhlikova et al., 2009). While oxytocin use is specifically contraindicated in women who had previous births, because of the high risks of uterine rupture, it is recommended and widely used during first births, especially to control post-partum haemorrhage, a leading cause of maternal deaths in India (Say et al., 2014).
Thulen assisted three women with home births. All were given oxytocin without the requisite medical infrastructure. For Bakuli, it was her first birth. At 44, Bakuli was the youngest of our eight older respondents, and she had two sons aged 15 and 20 years. While her older son was born at home, the younger one was born in 2003 in the PHC. She describes her homebirth experience thus, contrasting it with her hospital birth experience:
Bakuli: The dai-ma was very good, but sadly she died a few years ago. She used to tell me that the [baby’s] hand was somewhere else, so it was hurting me. She would put oil [tail] on my stomach and massage it. Later, when I had to work, I needed to bring bricks, needed to fetch water, and the malik [husband] was also not there. I would be in pain. The dai-ma would come and massage my stomach and back. Eight months passed in this way. She said that if it [the baby] wants to come out at eight months, let it come. She kept massaging me and like that it came down [the baby descended], and it was born. Interviewer: But didn’t you say that Thulen delivered your baby? Bakuli: Yes, he did, the dai-ma massaged and brought the baby down. And when it pained, Thulen came to give saline, and then the baby came out. I suffered a lot during that time [kosto paiso moi tatia]. I didn’t know anything during my elder son’s time, unlike for the small one. In the hospital, after getting two saline bottles, I got pain [contractions], then I forced myself and he came out. After birth, there was no sickness, no problems. Before the birth, I had pain. Interviewer: Was the ASHA with you in your younger son’s time? Bakuli: Yes, she was there, we like her a lot. She came with me, but the nurse wanted to go home early since it was festival time. She told me: ‘You hurry up and push because I want to go home and sleep’. I was admitted to the hospital in the morning. The baby came out at night, and I was sent home. It is not like it is now, where they keep you [for observation] for at least 24 hours.
Notably, the initial attempt was to deliver the baby with the help of the dai-ma; only when that was unsuccessful was Thulen invited. While his background and administration of oxytocin injections and ‘saline’ would have imbued a sense of medical authority, we believe that may not be the only reason why he was trusted by the villagers. His identity as a Karbi, and relations of kinship and reciprocity with the villagers, would have made him less of an outsider. Further, his practical skills acquired during military service perhaps helped consolidate his position as a medicine-man in the village.
Thus, the transition from an absence of intervention (Bahagi’s example) to acceptance of some forms of biomedical intervention to finally hospital-based births unfolds in a gradual fashion. Women use some of the state-provided ante-natal services like initial urine tests to check for gestational diabetes, and blood tests to check for anaemia, but births are still a cultural rather than a biomedical event and hence take place at home. For some women like Bakuli and Junu (discussed below), this transition from the cultural to the biomedical was more pronounced.
Junu and Rupali: Contrasting Experiences of Modern Obstetrics
Junu was a 55-year-old widow who had her first hospital birth not in Lalkhuti, but in an army hospital in Punjab, where her husband was posted as part of the Assam Rifles, a paramilitary force controlled by the Indian Army. Army service is a common choice of occupation among some Karbi groups. She had a second birth at home, not by choice, but because her older son was too ill at that time for her to go to the hospital to give birth. Junu had been initially admitted to an army hospital near Guwahati but had to return after a week’s stay because of her older child’s illness. Although there was a state-wide curfew prohibiting movement of all vehicles, she managed to get a seat on an army truck and travelled 35 kilometres to her home in Lalkhuti. She said a hospital birth would have been her preference, because of her prior experience at the army hospital:
[In the Army hospital,] food and lodging are free, medicine is free. During delivery, there is no need for family members to stay there. The people in the hospital take care of everything. Family members are allowed to visit only in the morning. The hospital took good care of me, and the nurses also behaved well with me. Only during my elder son’s birth, I suffered a bit because although he was born fine, half an hour later he lost consciousness. Then he was given oxygen and after that he regained consciousness. As a whole, it was good; treatment was free.
Junu’s experience in the army hospital is a far cry from state-run facilities near Lalkhuti and also the GM Hospital in Guwahati, the largest in Assam. Often poor women from Lalkhuti and their relatives are reluctant to go to the GM Hospital because it lacks support facilities such as food and stay, not just for relatives but also for ASHAs. Large out-of-pocket expenses for families and ASHAs, and the overall poor and disrespectful treatment they receive during childbirth discourage them from having births in GM Hospital. Junu’s home birth was facilitated by her mother-in-law. She reports that it was uncomplicated, despite the fact that the army hospital had earlier decided to admit her a week ahead of time in order to closely monitor her pregnancy.
Rupali, a first-time mother, was 24 years old. Her experience of giving birth in a large state-run hospital is representative of the experiences of many younger women in our study. She reported being scolded and subjected to fundal pressure to hasten the birth. She said the doctor at the hospital reprimanded her, claiming that she did not have problems and had ‘come just like that’, when in fact the PHC personnel had sent her there, because it was erroneously thought that she might need a caesarean section, as they had miscalculated the child’s weight from images in the sonogram.
Research indicates that it is not uncommon for smaller health centres to refer patients to tertiary care hospitals in rural locations for a host of complicated reasons, including not having an obstetrician on call, absence of medical equipment and not wanting to take risks that might potentially lead to the death of the mother or the child (Chattopadhyay, 2022). The PHC staff had pressurised Rupali into immediately transferring to the tertiary care hospital, but once she got there, the doctor blamed her for visiting the overburdened state facility. While her baby was delivered normally, she reported poor quality of care at the facility.
Birth as a Medically Managed Event
The narratives of younger women, as well as older women like Junu who had hospital births, suggest that what was earlier viewed as a family-/community-managed scenario has become transformed into a professionally managed event. With institutional deliveries and the disappearance of the dai-ma, family members now rely on hospitals to perform the polluting tasks of cleaning after birth instead of having to defile themselves and the home. With the death of the dai-ma in Lalkhuti and Thulen stopping his involvement in childbirth, hospitals have become the only and preferred site of childbirth. Along with this, the availability of imaging technologies such as sonograms even in small rural clinics, the regular monitoring of blood pressure and laboratory tests for blood and urine, the ubiquitous administration of vitamin injections, often purchased from the private sector and an emphasis on IFA supplementation due to high rates of anaemia during pregnancy, have given pregnancy and childbirth a distinctly biomedical character.
As noted, older women viewed younger mothers as having diminished capacities and felt that their inability to ‘suffer’ means that technological interventions during childbirth have become necessary. Similar findings are reported from rural Rajasthan and Tamil Nadu (Iyengar et al., 2008; Van Hollen, 2003), with practices like fundal pressure and oxytocin use justified because of the belief that younger women needed ‘external force to help expel the baby and placenta’. Shortening the duration of labour with more intense pain aided through oxytocin use became a ‘status passage’, while institutional births symbolised a more desirable way of birthing associated with modernity and development. In Assam, a similar process is underway, although still leaving out and thus ‘othering’ rural, poor or indigenous women who accidentally have home deliveries or are unable to access hospitals because of difficult terrain or other impediments (Chattopadhyay, 2018). Home deliveries in many parts of rural and tribal India have now become synonymous with backwardness and symbols of resistance to modernity and development.
Further, in Lalkhuti, the state has made itself omnipresent in recent years through several visual and discursive strategies in the area of reproductive governance. There are billboards of smiling mothers with their families who have ostensibly delivered ‘happily’ at state facilities. We found multiple visual and textual sources, including posters outside doctors’ rooms, noticeboards and billboards that described the role of ASHAs, including provision of contraception, immunisation and assistance during births as well as several advertisements for spacing devices such as intrauterine devices (IUDs) and pills. These images and accompanying texts emphasise the (ostensibly) free and quality care that women receive at hospitals. Simultaneously, Lalkhuti has a primary school and an anganwadi to provide free early childcare education and supplemental nutrition for infants and toddlers along with pregnant women, all of which builds expectations of the state as a provider of health and education. The reality is rather different, though, as there are out-of-pocket expenses for giving birth in government facilities. Also, women are given post-partum IUDs without choice or counselling about other spacing devices, and hospitals often lack basic supplies such as gloves and analgesics.
Despite such drawbacks, there is a continued irrevocable shift from home to hospitals for childbirths in the hamlet, suggestive of the homogenising power of biomedical technologies disbursed and supported by state institutions and the private sector. Changes in birthing practices are consonant with changes in the larger political economy, including proactive governance of reproduction, the proliferation of biomedical technologies and their consumption by pregnant women and their families, indicating the shift from births as a cultural rite of passage to a biomedical event.
Conclusions
The normalisation of hospital births in Lalkhuti has been facilitated by multiple factors identified in this article. Economic development has provided expanded access to modern medicine. The tangible presence of the state through its infrastructure and symbolic embodiment through direct messages and indirect signalling of free and better care, combined with stories of ‘safe’ births in hospitals is prominent. The introduction of biomedical practices through home births where oxytocin was used prepared the shift towards institutional deliveries. Financial incentives offered by government schemes are connected to international and national discourses around maternal health indicators, equating safety with institutional births. Socialisation into modern medical practices through the state’s free public health interventions such as immunisation and prenatal care has been a factor. Deskilling of TBAs that made communities feel less empowered to manage childbirths, and changes in cultural belief systems that medical interventions are necessary for safe births, followed by real reduction in mortality rates, have all had an impact.
Many of these changes such as medicalisation of births accompanied by high levels of interventions during childbirth may be detrimental to women’s and children’s well-being in the long-run, while also simultaneously reducing health-promoting cultural practices. Although not all traditional practices are health promoting, such as those that ask pregnant women to eat less to ensure easier births, others such as giving birth in non-dorsal positions, use of massages, being mobile while labouring and presence of female kin may have led to a more positive experience of childbirth in the past (Withers et al., 2018). The Government of India, recognising that quality of care during labour was a problem in many state facilities, launched the Labour Room Quality Improvement Initiative or LaQshya in 2017 to improve the care for women delivering in state facilities and incorporated some of these into best practice checklists for hospitals.
While it is clear that the main locations for births are now hospitals, whether private or public, we end with some questions for future exploration. In time, is it likely that the memories of giving birth alone or at home will disappear, so that hospital births will seem to be the way that women have always birthed? What implications does this have for women’s relationship with their bodies and for childbirth as a life event? Will the introduction of the LaQshya programme, which seeks to improve quality of care in labour rooms in India, improve women’s experience with modern obstetrics? Within such interventions, will there be space to accommodate cultural practices which were health promoting such as massages, consumption of specific items and attentive care?
Footnotes
Acknowledgements
We thank the Azim Premji University’s Research Centre for funding our research project in 2015 to 2017, titled ‘Exploring Factors Affecting Maternal Health in Assam’, and two research assistants (Riniki Dutta and Rijumoni Chetia) who helped collect data. We also thank Professor Arima Mishra, whose collaboration was invaluable. We thank the women of ‘Lalkhuti’ and surrounding hamlets for sharing their lives and stories with us. Also, thanks are due to the staff of the District Hospital who permitted us to recruit study participants and the doctors, nurses and health workers who shared their experiences with us. We benefited from feedback received on our findings from papers presented at the American Anthropological Association Annual Conference (Minneapolis, 2016), a dissemination workshop attended by local scholars in Guwahati, Assam in 2017, and drafts of this article presented at the Institute for Social and Economic Change (ISEC, Bangalore), and the Centre for Contemporary South Asia at the Watson Institute, Brown University in 2018.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.