
Abstract
The Bradley report published in 2009 highlighted the diverse and complex nature of the offender population and the need for partnership working to ensure early identification of needs and diversion into appropriate treatment. Following the successful pilot of an initiative in London to identify personality disturbance and plan treatment pathways, provisions have been made for implementation at a national level. This paper seeks to draw a comparison between the original sample identified in the London pilot and those identified by the Lincolnshire Personality Disorder Pathway in the context of the Transforming Rehabilitation agenda to consider the importance of local planning.
Introduction
There is a growing body of research to suggest that within an offending population there is a high prevalence of personality disorder (PD) with a disproportionate representation in comparison to the general population (Craissati et al, 2011; Moran et al., 2006; Singleton et al., 1998). Links have been found between this recognised mental disorder and a number of challenges such as faster reconviction rates for more serious offences, community failure and increased time spent in segregation, in addition to self-harm and substance use (Coid et al., 2007; Craissati et al., 2008; Craissati et al., 2011). Provisions for offenders with personality disorders within National Offender Management Service (NOMS) and the National Health Service (NHS) have recently been reviewed (Department of Health and National Offender Manager Personality Disorder Team, 2011) and as a result some of the £69 million invested in the Dangerous and Severe Personality Disorder (DSPD) Services has been reapportioned to community and prison-based services.
As part of the reallocation of monies a pilot was implemented across four London boroughs (Lambeth, Southwark, Hackney and Tower Hamlets) to investigate how probation staff might identify offenders with problematic personality traits at an earlier point in their contact with the criminal justice system (Minoudis et al., 2012a). Initial identification was based upon the presence of 10 items in the Offender Assessment System (OASys) designed to indicate possible DSPD. However, this was soon found to not be sufficiently inclusive of all personality disorders due to the primary focus upon antisocial personality disorder (Shaw et al., 2012). In order to address this a referral system was trialled, with limited success due to inconsistencies in referral rates (Minoudis et al., 2012a). As a result a screening tool was developed, incorporating the DSPD items and four additional factors associated with personality disorder (childhood difficulties, a history of mental health difficulties, self-harm/suicide attempts and attacks or threats of attack on staff) in order to assist in the early identification of personality disorder traits. Based upon this tool offenders were identified and selected if they were: managed by probation officers (POs) and assessed as being high or very high risk of serious harm, were subject to an indeterminate or determinate sentence for a violent or sexual offence and had either the DSPD factors and/or any of the other factors. Based upon these criteria a total of 342 cases (5% of the total probation population) were selected for entry into the pathway for case discussion and pathway planning.
Further to the work of Minoudis et al. (2012a) in the London pilot, a service specification was produced to replicate the pathway nationally. It was proposed that a joint service between NHS and NOMS (NHS & NOMS, 2012) would seek to engage in the early identification of offenders with problematic personality traits and to consult on and formulate psychologically informed pathways for forward progression as per the pilot. Additionally, a key principle embedded into the pathway was, and continues to be, workforce development to be able to identify and manage offenders with personality disorder traits in a more psychologically informed way. Lincolnshire Probation Trust (LPT, the local probation organisation prior to the Transforming Rehabilitation (TR, agenda)) and Lincolnshire Partnership Foundation Trust (LPFT) were jointly awarded a contract to undertake this work within Lincolnshire and a schema-informed service implemented.
Schema theory (Young, 1990) draws upon a variety of fields, including Cognitive Behavioural Therapy (Beck et al., 1979), attachment theory (Ainsworth, 1973; Bowlby, 1969), Gestalt theory and psychodynamic theory. It provides an alternative way of understanding problematic personality traits, rather than a more diagnostic or behavioural approach. Schema theory is based on the premise that personality pathology develops from unmet core emotional needs in childhood through the presence of early maladaptive schemas (EMS). Young (1990) defines EMS as self-defeating emotional and cognitive patterns that develop early in childhood and are strengthened and elaborated throughout life. In this way maladaptive behaviours including (but not limited to) offending behaviour, substance abuse and self-harm can be understood as extreme coping responses to schema activation. EMS can be considered to be more stable trait-like entities, whilst schema modes, which are made up of clusters of schemas and coping strategies, are state-like changeable expressions of schemas that can temporarily dominate an individual’s presentation. Bernstein et al. (2007) have extended the original model to incorporate schema modes that are more commonly seen in forensic clients.
The TR agenda changes came into force on 1 June 2014. TR has resulted in a move from local area probation trusts to the nationally controlled National Probation Service (NPS, which retains management of cases assessed as being either high or very high risk and/or eligible for registration for a Multi-Agency Public Protection Arrangement), and Community Rehabilitation Companies (CRCs) (CRC, which retain management of offenders assessed as medium or low risk of serious harm). Since TR the pathway contract is now between the NPS in Lincolnshire and LPFT. However, at the time of the initial identification process LPT was still in existence, and thus it is referred to throughout this article. The TR agenda has presented the pathway team both with opportunities and challenges, which will be discussed.
Since the implementation of the personality disorder pathway in Lincolnshire from April 2013 to June 2014 all cases held within LPT were screened and this paper seeks to provide a comparison of those offenders identified within the Lincolnshire area with the London sample reported by Minoudis et al., 2012a.
Lincolnshire is a large, mainly rural, English county, with an approximate population of 713,653 (Lincolnshire Research Observatory, 2012). The London pilot (Minoudis et al., 2012a) worked across four London boroughs with a significantly smaller area but significantly bigger population of approximately 1,091,000 (Office of National Statistics, 2012a) and much greater population density. The areas also differ in ethnic diversity (Office of National Statistics, 2012b), with Lincolnshire’s white population approximately 97.6%, and the four London borough’s white population approximately 53.0%.
LPT was managed in two local delivery units (LDUs): west and east, with the west having 25 offender managers working in three offices, and the east having 35 offender managers working across six offices. At the time of the initial screening (July to September 2013) there were 1717 offenders who had supervision with LPT. Both areas included an Integrated Offender Management office dedicated to the management of prolific acquisitive offenders.
Whilst it is recognised that the areas are geographically and demographically very different, it was felt that it was important to draw a comparison with the London sample as this was the basis for the national implementation and useful in the consideration of local differences and the challenges that unique differences may present.
Hypotheses
Based upon findings published by Minoudis et al. (2012a), it was hypothesised that:
Hypothesis 1: Offenders identified by the pathway will be more likely to have an index violent or sexual offence, compared to the total LPT caseload
Hypothesis 2: Offenders who are identified by the pathway will be more likely to have received a custodial sentence for the index offence, compared to the total LPT caseload
Hypothesis 3: Offenders who are identified by the pathway will be more likely to be assessed as high or very high risk of serious harm, compared to the total LPT caseload
Hypothesis 4: A significantly higher proportion of POs caseloads will screen in, compared to probation service officers’ (PSOs) caseloads
Hypothesis 5: There will be a high prevalence of childhood problems amongst the offenders identified by the pathway
Method
During the national implementation process a flowchart based upon the pilot screening tool (Minoudis et al., 2012a) was identified within the service specification from the NHS and NOMS (2012). This was used by the pathway to begin the screening process in July 2013 when all offender managers (both qualified POs and PSOs) were tasked with screening their caseload. It was hoped that early screening would enable case consultation, formulation and workforce development (training on personality disorder traits, the schema model and consultation and formulation) to begin as soon as possible.
The primary focus for screening in the pilot were offenders in custody, those who were assessed as high or very high risk and those with violent or sexual offences. This focus was incorporated into the guidance provided for the national implementation in order to help sift through a large number of individuals for a more focused approach to service provision. However, based upon anecdotal evidence and previous experience of the pathway’s POs from within both general offender management and the prison estate, it was recognised that individuals currently assessed as being low or medium risk with no convictions for violence can and do sometimes go on to commit a serious violent or sexual offence. Further, due to size and culture within Lincolnshire, the pathway team were keen not to exclude individuals based upon a current risk assessment level and at the time of screening the team had capacity to support this. As a result it was decided to screen all cases held within probation based upon the personality disorder factors, as this could facilitate the identification of possible personality disorder traits at an earlier point than initially planned by the pilot. Furthermore, the pathway team did not limit itself to only assisting with individuals with custodial sentences (either life, indeterminate public protection or determinate), and it was decided that they would work with both custody and community cases where need was identified.
Following the screening process each offender subject to supervision under LPT obtained a score from the five personality disorder factors developed by Minoudis et al. (2012a), with a score of seven DSPD items counting as one of the five items. An algorithm (Figure 1) was then developed to determine the level of team involvement for male offenders. Similar challenges in comparison to the pilot in terms of reliably identifying borderline, paranoid and narcissistic personality disorders were noted by the pathway team when interpreting the screening tool based primarily upon the DSPD items and so equal weight was given to each of the five factors on the screening tool in an attempt to account for and include a variety of personality disorder traits. Based upon local knowledge and experience, and analysis of the screening tool returns, an entry criteria of three or more of the five factors on the screening tool was implemented. In order to manage and prioritise the service consultation, formulation and planning delivery this was further tiered so that males scoring three items would be offered case consultation and those high or very high risk cases scoring four or five of the criteria would be offered full case formulation. Additional monies were awarded to the pathway to specifically investigate the needs of females and in partial fulfilment of this key performance indicator all women with a personality disorder trait score of three were automatically identified for full case formulation rather than imposing the additional cut-off tiers.
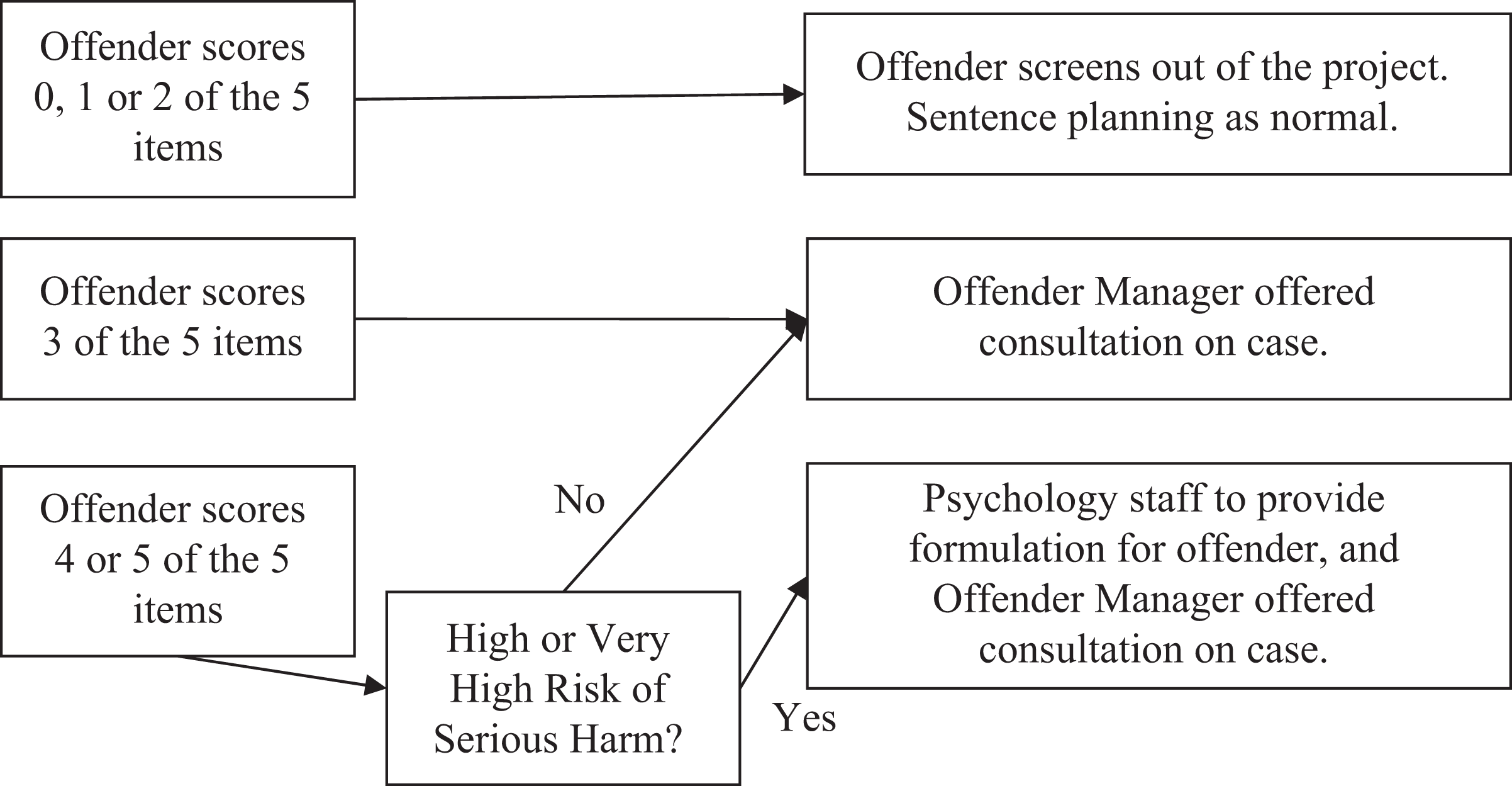
Algorithm showing male offenders entry into the pathway for consultation or formulation.
Results
In using a pathway entry cut-off of a score of three or above 307 offenders were identified, representing 17.9% of the total caseload within Lincolnshire as compared to the 5% identified in the pilot (Minoudis et al., 2012). There was no significant difference between those identified for entry to the pathway based upon the LDU or office.
Hypothesis one
There was partial support for hypothesis one. A larger proportion of those identified by the pathway had a violent index offence (Z=2.56, p<0.01), compared to LPT’s total caseload. This was a comparable finding to the London pilot sample. However, unlike the pilot, there was no significant difference between the proportion of individuals with sexual offences identified by the pathway and those within LPT’s entire caseload who were more likely to have convictions for drug offences (Z=−3.50, p>0.001), fraud and forgery offences (Z=−2.23, p<0.01) or motoring offences (Z=−2.40, p<0.01).
Hypothesis two
There was no support for hypothesis two. In contrast to the pilot sample, there was no significant difference in the proportion of offenders given a custodial sentence identified by the pathway, compared to LPT’s entire caseload. However, a significantly greater percentage of offenders identified by the pathway were currently in custody after being recalled (Z=2.40, p<0.01) or were detained under the Mental Health Act (Z=3.09, p<0.001).
Hypothesis three
Hypothesis three was supported as a larger proportion of those assessed as very high risk (Z=2.92, p<0.01) and high risk (Z=8.08, p<0.01) met the criteria for the pathway compared to LPT’s total caseload, matching the findings within the pilot. Of note, there was no significant difference for those assessed as medium risk of serious harm, with only results for those assessed as low risk of serious harm being in the expected direction (Z=-6.87, p<0.0001). Demographic comparisons, concerning hypotheses one to three, are made below (Table 1).
Comparison of offenders identified by the pathway to the total LPT caseload.
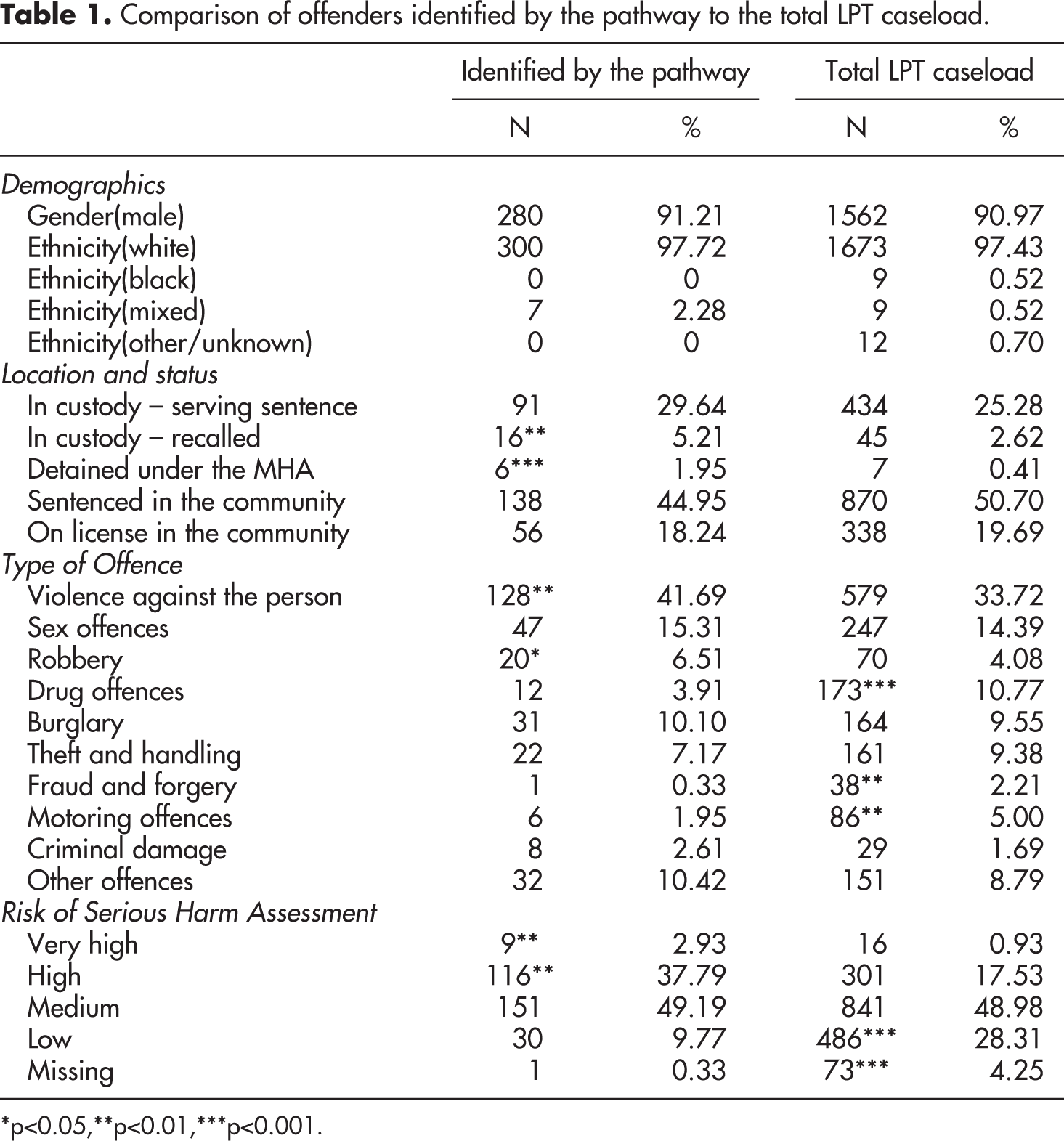
*p<0.05,**p<0.01,***p<0.001.
Hypothesis four
A significantly larger proportion of POs’ cases were identified by the pathway (25.63%) compared PSOs’ cases (12.91%) (Z=8.135, p<0.0001) providing support for hypothesis four. Despite this significant difference almost half (44%) of cases identified were held by PSOs.
Hypothesis five
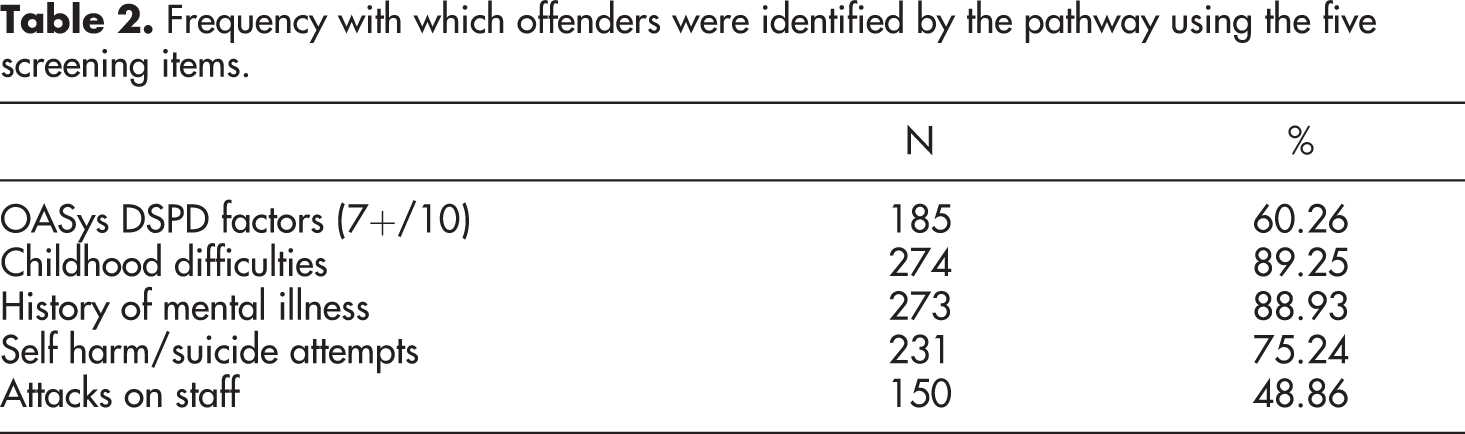
Childhood difficulties were the most reported screening tool factor in the identified sample (Table 2) providing support for hypothesis five and matching the results found in the London pilot (Minoudis et al., 2012a).
Frequency with which offenders were identified by the pathway using the five screening items.
Discussion
Despite the significant difference between Lincolnshire and the four London boroughs covered in the pilot, the caseload demographics were examined and compared to ascertain how well the London pilot could be replicated in other areas as part of the national implementation of the offender personality disorder pathway. Cases identified by the pathway were similar to the pilot in terms of the proportion of violent offences, risk assessment ratings and experience of childhood difficulties recorded for identified individuals as compared to the total probation caseload. Differences were found between the pilot and pathway in terms of the proportion of sexual offences and sentence type for individuals identified by the pathway as compared to the total probation caseload. Further, more cases were identified as a proportion of the total probation caseload in Lincolnshire than compared to the pilot.
The number of cases identified as meeting criteria for entry into the pathway in Lincolnshire was over three times greater than was found in the London pilot. As noted previously, the method used to screen offenders for personality disorder traits and enter them into the pathway in this study differed from the London sample. POs were asked to assess their own caseloads, allowing the team to provide consultation and training from the onset of the pathway. Furthermore, within the pathway PSOs, who manage low and medium risk cases, were also asked to assess their caseloads due to the anecdotal evidence of POs in the pathway team, local culture and team capacity, whereas the London pilot initially only assessed POs’ caseloads. This resulted in the inclusion of community orders. The variation in screening process and inclusion criteria due to local sensitivity may go some way to account for the larger identification percentage as compared to the pilot; more individuals were screened resulting in a higher likelihood of increased identification and so a greater proportion of entry into the pathway.
Similarly to the pilot, there were statistically more individuals assessed as high or very high risk of harm identified and entered into the pathway than in LPTs total caseload. This suggests that individuals assessed as high or very high risk are more likely to present with problematic personality traits. Interestingly, there was no statistical difference in the proportion of individuals assessed as medium risk of harm identified by the pathway but there was a significant difference in the proportion of individuals assessed as low risk of harm. In keeping with the idea of assessed risk being associated with likelihood of personality disorder trait presence, there were statistically more cases held by POs than by PSOs identified by the pathway. This can be partly accounted for by the nature and risk level of the caseloads traditionally held by the officers, with the more complex cases who may be more likely to have problematic personality traits being held by POs. Despite this difference, almost half of the pathway’s identified caseload were supervised by PSOs, possibly indicating a prevalence of problematic personality traits in cases assessed as being lower risk. This highlights the benefits of including this group in the screening process as risk level does not, in this instance, seem to be an indicator for likelihood of personality disorder trait presence. In not screening this group there is the potential for overlooking possible personality disorder and therefore need.
Following the TR agenda changes and the probation split in June 2014, medium and low risk cases are now held by the CRCs, and there is no remit for the pathways involvement with them. This is an unfortunate consequence of the TR agenda, and given the number of medium risk or serious harm cases who were identified by the pathway before the split, it is potentially worrying. Clearly resources should be targeted where there is the greatest need, in keeping with the principles of the risk-needs-responsivity model (Andrews & Bonta, 2006). However, these findings suggest that there may be an area of need for individuals assessed as medium risk that would benefit from further exploration.
The London pilot used risk and sentence type to focus screening and identification. The team screened individuals who had been assessed as high risk and/or those who had a determinate or indeterminate sentence for a violent or sexual offence. As a result, a large proportion of those identified were in custody. This was not the case within the Lincolnshire pathway, where less than a third were in custody and, as previously noted, this may be accounted for by the total caseload screen rather than the focused screen. The pilot findings may have been replicated in Lincolnshire if a more focused screen had been conducted. However, it is of note that a larger proportion of offenders identified had been recalled to custody compared to LPT caseload, in line with theories around personality disorder and the difficulties such individuals have with completing an order/licence period (Department of Health 2011).
Of particular note was the difference between the pathway and pilot for the identified number of individuals convicted of a sexual offence as a proportion of the whole areas caseload. Within Lincolnshire there was no difference between the number of individuals identified and the general caseload. It is not clear why this difference exists. One possibility is that individuals who have committed sexual offences may present differently to the factors listed on the screening tool, which seems to reflect more borderline and anti-social personality disorder presentations than any other type. It may be that traits associated with other personality disorders such as schizoid or narcissistic presentations are not adequately captured. Since the initial screening process, the screening method used by the pathway has evolved. The pathway team have found that more individuals with convictions for sexual offences have been identified with lower scores on the screening tool through a clinical over-ride decision based on presentations more in line with a narcissistic personality disorder (i.e. prolific writing of complaint letters to managers and local MPs, litigation, excessive proofreading of OASys assessments for grammatical errors, self-representation for parole hearings etc.).
Minoudis et al. (2012a) noted that most of the cases identified in London had reported childhood abuse and/or behavioural problems. The pathway found a similar link between childhood problems and identification. This is consistent with the understanding of the importance of childhood provided by the schema model that informs the pathway. It is noted that almost as many offenders had a history of mental health problems as childhood problems. In line with schema theory, mental health problems can be considered in terms of an individual’s childhood, suggesting that the childhood factor is particularly crucial in screening.
One limitation of the current paper is that whilst the entire caseload within Lincolnshire was used, the sample is small and the generalisability of the findings is limited as a result. Additionally, whilst comparisons were drawn between the Lincolnshire pathway and the pilot, these are limited due to the different screening criteria and process used and therefore direct comparisons and conclusions are difficult to draw. Further, it is acknowledged that Lincolnshire has a very different geography and population to London, where the pilot took place, and results from the study of one Midlands county may not be generalisable to other counties across the UK. However, given the differences between the two sites and the screening methods, it is encouraging that similarities exist and provide some confidence that the screening process is identifying a similar group of individuals.
The screening process is dependent upon the current OASys. As noted by Minoudis et al. (2012b) one limitation of asking offender managers to screen their own caseloads based on their OASys was the differences in frequency and quality to which offender managers complete an OASys. The pathway was not immune to this challenge and despite quarterly quality audits conducted by LPT, variation is still likely. There is a minimum expectation that the OASys is reviewed on a yearly basis. However this is a long time in the course of an individual’s life and important things may be missed during this period. As a result, some of the screening may not have been as accurate and up-to-date as would have been preferred.
Another problem noted was that OASys layer one and layer two assessments only hold minimal offence and personal information. This lack of information meant it was impossible for an offender to be identified for the pathway using the screening tool. However, after discussion with probation staff, it was noted that professional judgement only allows a layer two OASys to be completed when there are no concerns and a minor offence has been committed. Individuals would therefore be unlikely to be identified by the pathway had a layer three OASys been completed. Arguably then, any individual for whom there is only a layer one or two OASys should not need identification for consultation, formulation and pathway planning as a lack of concerns would suggest that the individual is functioning well and progressing through their sentence and there is no remit for the pathway.
Current situation and future direction
The pathway is continuing to formulate complex offenders with personality disorders and consult on all cases identified, in addition to providing training to probation staff and allied services. A small number of the offenders identified by the pathway are managed directly by the POs who are based within the pathway team, upon a complexity and needs basis, so that the ‘critical few’ are managed by POs with more time and support than is possible within general offender management.
Since the initial screening process, the identification of cases entering into the pathway has evolved and adapted in the wake of experience and the realisation of the TR agenda within probation. The use of an algorithm to provide cut-off points was based upon the notion that the more traits that were reported for an individual identified by the pathway the more complex or sever the individuals difficulties may be. The algorithm was perceived as a way to best manage a limited resource and a means of making a seemingly large and potentially daunting task manageable. However, there is a sense that the pathway was overly reliant upon categories and numbers and therefore the process lacked some of the clinical sensitivity often required when working with people. Following the initial screen, the ownership of the screening was retained by the pathway in order to support offender managers through the split, and this resulted in a consistent 100% screening rate.
Following the move from LPT to the NPS and CRCs the pathway’s remit has narrowed to working only with the NPS, and thus with individuals assessed as being high risk. Within this process the task of screening was returned to the offender managers and the screening rate has significantly reduced, to the extent that from June to August no screening took place. The impact of the TR agenda was significant upon all probation staff members within Lincolnshire and many seemed to struggle to have the space or time to complete what was felt by many to be yet another task.
Whilst there was an impact upon contracting and delivery of service for the pathway, this was relatively tempered as a result of the significant early progress that was made in case identification. This meant that the pathway was well established before the split. Whilst this was clearly a challenging time for all involved, the pathway team sought to use the change as an opportunity to review the screening process. As a result the algorithm was retired and a more sensitive, clinically based approach introduced to jointly identify and decide upon pathway entry on a need-responsive basis. This seems to have been well received and screening tools have begun to be returned more frequently. This return rate still falls far short of the 100% target, however, and it remains an area of focus for the pathway.
One significant impact of the TR agenda upon the delivery of the pathway has been the contracting shift to working with the NPS and only female CRC cases. This is in part due to the funding stream for the pathway, which requires the money to be directed towards individuals assessed as high risk. In this regard the screening tool has functioned as a rudimentary personality disorder screen, which is then discussed though consultation with the offender manager. However, NPS caseloads are now all high risk offenders who, based upon the initial findings presented here, are more likely to have personality difficulties and have more complex needs. The impact of this upon staff is likely to be particularly challenging. There were concerns that supporting staff to think about cases when they had high caseloads full of complex individuals would be increasingly difficult. Whilst there have undeniably been some problems, the biggest challenge has seemed to be the screening rate rather than engagement with consultations and formulations.
Looking forward, the demarcation of risk as prescribed by the TR agenda to designate the service that an individual receives is a cause for concern. Risk is a dynamic construct and as highlighted in the pathway screening process, it is argued that individuals are more complex than is implied by arbitrary cut-off points on a scale. Further, risk (or dangerousness) is not necessarily the same thing as difficulty. It is of concern that, based upon this unitary factor, offender managers do not have access to a service to support the understanding of an individual and therefore support risk and difficulty management. It is particularly concerning that males within the CRCs assessed as being medium risk appear in this sample to have relatively equal rates of personality difficulties. Whilst personality difficulties do not automatically equal an increased risk, the additional support to help understand any possible functional link between personality difficulties and offending is an important risk management strategy. Unfortunately, this is the nature of the probation service following the TR agenda and arguably the limited resource must follow risk. If an individual case within the CRC is deemed to be increasing in risk level, they can be escalated up to the NPS and then screened as part of the pathway. Equally, should an NPS case no longer be assessed as high risk they may remain an identified case but the offender manager can access consultation on a needs basis. It is maybe a task for the pathway team to demonstrate the efficacy of this way of working so that it could be extended into the CRCs.
It is unclear what the future will be for the NPS and the personality disorder pathway. However, when fully staffed, the Lincolnshire Pathway team has a high ratio of team to offenders supervised compared to other areas. This has allowed the team to consult with more staff, train more staff (including external agencies) and complete more formulations to date than other areas are likely to have had the capacity to do. The feedback from both commissioning bodies and local staff has generally been very positive and whilst TR presents a risk of this changing, the pathway team are committed to supporting psychologically informed pathway plans for all individuals. It is hoped that the model used could be emulated across the NPS.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.