
Abstract
Suicide in probation services is far higher than the general population. This paper presents secondary analysis of data previously used to evaluate the outcome of delivering psychological treatment to probationers in London. A sample of probation service users who screened positive for clinically significant symptoms of distress and were subsequently assessed and offered treatment (n = 274) were allocated retrospectively to one of three groups: those with a history of suicidal ideations but no suicide attempts (ideation group), those with a history of a suicidal act (attempt group) or a control group where suicide was not evident (no history group). Results indicate no significant difference between the ideation and the attempt groups, but significant differences between these and the no history group. The findings are discussed within the context of the suicide ideation-to-action models that have been debated in other offender settings. We conclude that a more nuanced understanding of suicidal acts and suicide attempts is required in probation services including a prospective study that tests the ideation-to-action model.
Introduction
Suicide is increasing in probation services in England. Little is known about those that either complete suicide or who experience strong suicidal ideation when they are serving a community sentence. A secondary analysis of a data set was undertaken which records the sociodemographic and clinical variables of all those screening positive for a mental health problem in probation in London. If a client screens positive for a mental health problem in the London probation service they are usually offered a manual-based psychological therapy (Fowler et al., 2020). The data analysed in this paper are drawn from a sample of 3700 probation clients during the period of July 2014 through July 2020 who all screened positive in the London service and were offered a trial of psychological therapy.
Background
It is clear from published research that suicide is a significant issue in probation. Suicide rates are increasing and there is a greater risk of death from suicide for probationers when compared with prisoners or to the general population. An early study by Sattar (2003) reviewed death certificates for 1267 offenders serving community sentences or receiving post-custodial supervision by probation in England and Wales. Standardised mortality ratios (SMRs) calculated for males showed that offenders in the community had an SMR of 378, compared to an SMR of 100 for the general population. That is, offenders in the community were almost four times more likely to die than the general population (Sattar, 2003: 21). When looking specifically at suicide, they were ‘over 9 times more likely to die than the general population in 1996 [SMR of 977 versus 100], and in 1997 community offenders were 13 times more likely to die than the general population’ with an SMR of 1307 versus 100 (Sattar, 2003: 21).
In the United States, Bingswanger et al. (2007) found highly elevated SMRs in the population released from Washington State prisons in the first two weeks after release in a group of just over 30,000 ex-prisoners. They found that the SMR, in comparison with other state residents, was 12.7. Overdoses and suicide constituted a high proportion (35%) of these untoward deaths. A similar study undertaken in Scotland (Graham et al., 2015) examined mortality data on the deaths of 4414 prisoners during an 11-year period 1996–-2007. Again, substantial excess mortality was established especially in the immediate 4-week period after release thus: In absolute terms, drug-related deaths and suicides were the single most important causes of death. (Graham et al., 2015: 881)
Philips et al. (2018) have examined suicide rates in probation more recently and shown that suicide rates of community offenders are considerably higher than the general population in England. Table 1 shows the variation in suicide by setting with probation higher than prisons and much higher than the general population. Suicide rates also vary by gender. The rate per 100,000 of the population for men 105 and for women 145 (this compares with respectively 5.6/100,000 and 29.2/100,000 for men and women in the general population). Overall, between 2010/11 and 2015/16, there were 1619 suicides by probationers. This is a high figure and one that is likely to underestimating the size of the issue (Philips et al., 2018).
Suicide rate and rate ratio of people dying by suicide under supervision, in prison and in the general population.
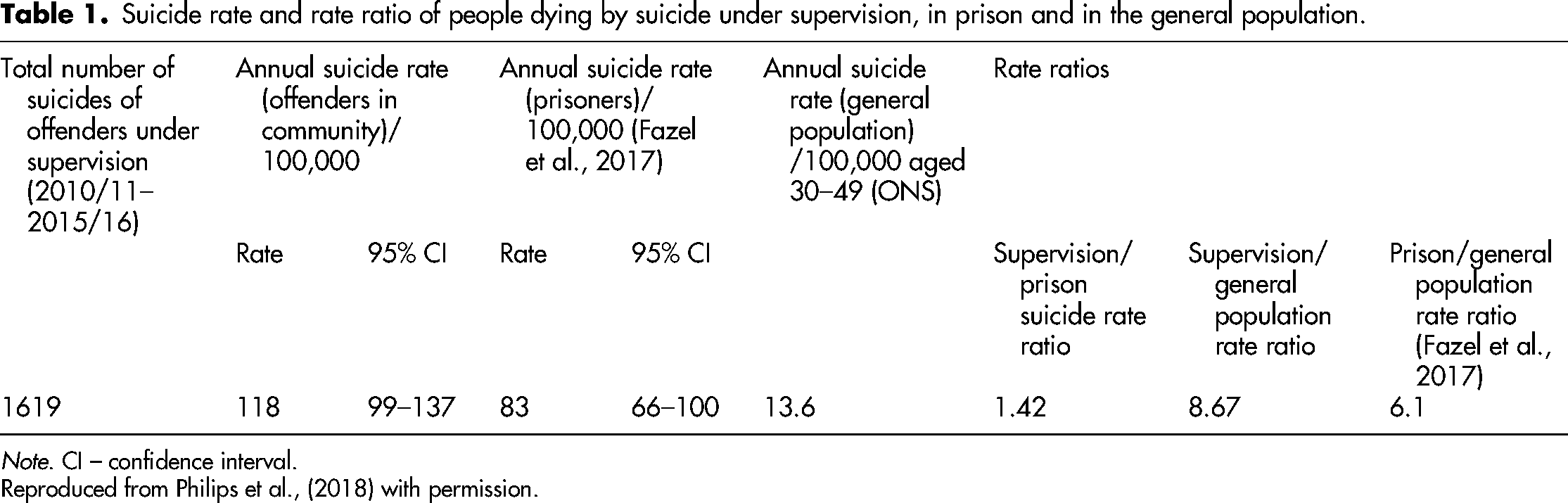
Note. CI – confidence interval.
Reproduced from Philips et al., (2018) with permission.
There has also been a systematic review of the literature concerning suicide and suicidal ideation and probation (Sirdifield et al., 2020). This includes the estimates of prevalence and possible predictors of suicide and suicidal ideation. Searches were conducted on nine databases from January 2000 to May 2017, key journals from January 2000 to September 2017 and the unpublished literature. A total of 5125 papers were identified in the initial electronic searches and were carefully double-blind reviewed. The review concluded that people on probation are a very high-risk group for completed suicide, and factors associated with this include drug overdose, mental health problems and poor physical health. There is a clear need for high-quality partnership working between probation and mental health services, and investment in services, to support appropriate responses to suicide risk.
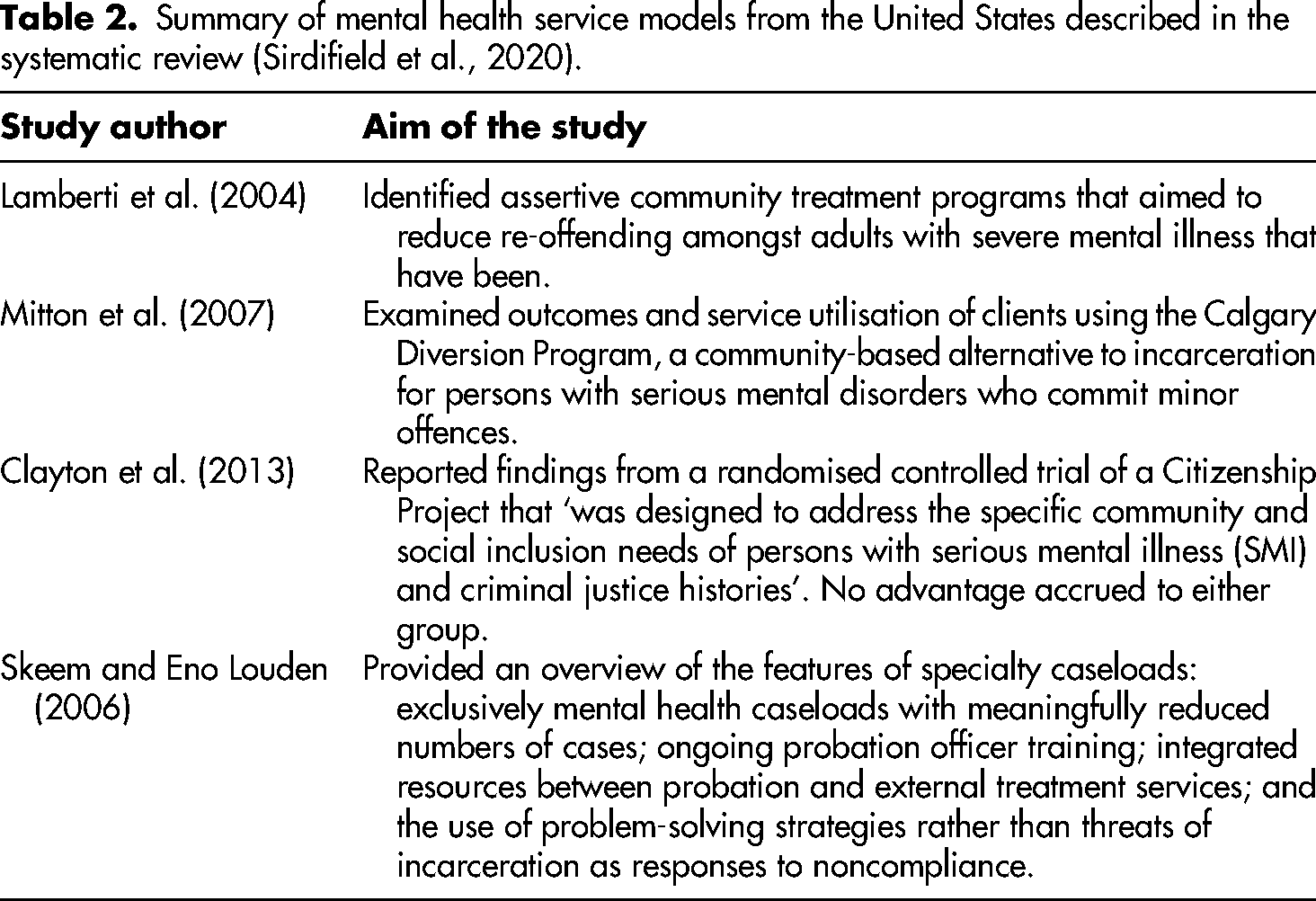
To better respond to suicide risk in probation clients, there should be an established relationship between mental health and probation service. Some examples of such a relationship have been described but mostly in the United States. Table 2 gives details of these studies.
Summary of mental health service models from the United States described in the systematic review (Sirdifield et al., 2020).
Pluck and Brooker (2014) examined past suicidal behaviour and suicidal ideation in a stratified random sample of probation clients in Lincolnshire. This sample had screened positive for a mental health problem. They found nearly one-third (32%) had attempted suicide in the past and that 9% were at ‘high risk’ of suicide currently. Younger people were more likely to have deliberately self-harmed in the previous month (15% vs. 2%). The study concluded that: The National Confidential Inquiry into Suicide and Homicide collects data annually on all suicides throughout the whole of the UK and has monitored trends in prisons and health services. It is time to attend to community supervised offenders too.
It has been suggested that the lack of training for probation officers in either mental illness or substance misuse means that mental health issues are often missed by offender managers (Sirdifield et al., 2010). Suicidal ideation, in particular, is difficult to identify without specific education in this aspect of mental health (Brooker et al., 2014). Indeed, it has been shown that offender managers only recognise 64% of cases with depression and 36% of those with psychotic disorders in a large community random sample of probationers formally identified with a mental health disorder (Brooker et al., 2012).
In England, the recent National Probation Service Health and Social Care Strategy 2019–2022 (National Probation Service, 2018) has included a commitment to raising awareness and understanding of suicide prevention and risk of suicide and to develop the workforce to address these vulnerabilities. Intensely training a subset of probation staff in mental health seems to make perfect sense, not least of which would be to reduce the seriously high suicide rate amongst this group. However, it still requires a good relationship with a local mental health service/general practitioner if clients are to pursue an appropriate pathway once suicidal ideation has been detected. Progress with the overall implementation of the national probation health strategy has, as yet, not been described.
In this study, data were analysed from the Psychological Treatment service offered to clients in the London Community Rehabilitation Company (CRC). The aim was to examine variables that might be associated with suicidality in probationers assessed as needing, and accepting, psychological intervention.
Method
Ethics
Ethical approval for the previous study (Fowler et al., 2020) was granted from two committees in 2016 – one represented the London CRC and the other represented St Andrew's Healthcare. Ethics approval was granted on the basis that each service user entering the programme signed a consent form demonstrating their understanding of how data regarding their treatment would be handled. That form also described how their information may be used for research purposes. This same consent granted access for our staff to their relevant offending history through the nDelius database. In the case of this study, St Andrews Healthcare provided us with further approval through their research governance processes.
Sample
Our sample was obtained from service users of the London CRC (a private probation provider working alongside the National Probation Service in the England and Wales). Participants in this study were those individuals on probation deemed to be in need of psychological intervention by probation staff by scoring over 12 on the Kessler 6 (K6) psychometric test (Cornelius et al., 2013). The Kessler screening tool consists of six items all scoring 1 to 5. An example of one of the Kessler items is ‘During the past 30 days how often did you feel hopeless?’ All offenders on probation were administered the K6 during their intake interview, the results of which informed probation officers as to whether or not an individual was in need of intervention. Between the establishment of the service in 2014 and the time of this study (July 2020), there were 3700 service users registered with the service.
After referral, a consultation is provided and advice is given as to whether or not an assessment should be offered as part of the service. There are various outcomes 1 of the assessments where some individuals are offered and complete treatment (291/3700; 7.9%), although a small number are advised not to proceed due to being in crisis (45/3700; 1.2%).
A total sample of 336 records were investigated for this study, which consisted 291 completing treatment and 45 individuals who were assessed but advised not to proceed due to being in crisis at the time. Of the total, 61 (18%) were subsequently excluded because they had no suicide assessment available. Therefore, the final sample in this study was 274.
Measures
Participant notes were analysed to determine the current and/or past suicidal ideation or action of each individual. The threshold used to determine the presence of ideation was that of one or more clinical notes recording suicidal ideation in the opinion of the clinician working with the service user. Suicidal action was determined by a recorded example of an attempt in which medical attention was required, differentiated from self-harm through risk assessment at the time of the attempt, conducted by the clinician working with the individual at the time of the attempt. In addition, demographics (age, gender, ethnicity, postcode), crime (order and offence type) and psychometric measures which included: K6 [Cornelius et al., 2013]; Generalized Anxiety Disorder 7-item (GAD-7) [Spitzer et al., 2006]; Public Health Questionnaire (PHQ-9) [Kroinke et al., 2001]; and the Work and Social Adjustment Scale (WSAS) [Mundt et al., 2002].
Analysis
Three groups of suicidal intent were identified: those with current suicidal ideations (ideation group), those who had made a previous suicidal attempt (attempt group) and those where suicide was not indicated (no history group). Descriptive analysis was undertaken initially to compare the three groups.
Results
Within the study group, 100 (36%) had ever attempted suicide, 111 (41%) had suicide ideation at some time and 63 (23%) had no history of suicide attempt or ideation (Table 3). There was no statistical difference between the groups in gender, age, ethnicity, order type or local area deprivation score (indices of multiple deprivation).
Descriptive results of demographics between suicide groups (a) ever attempted suicide, (b) suicide ideation and (c) none indicated.

Chi square p < 0.05. IMD: Indices of multiple deprivation.
For all measures, there was no statistical difference between the attempt or ideation in the proportions in each category (Pearson's Chi square) or the mean scores (analysis of variance [ANOVA] post hoc Bonferroni multiple comparisons).
However, for some of the measures (K6, GAD-7, PHQ-9 and SAPAS), both the attempt and the ideation group were significantly more likely to have a higher score than the no history of suicide group:
38% of the attempt group and 36% of the ideation group had a psychological distress score (K6) of 25+ compared with 15% of those with no history (Pearson's Chi square p < 0.01). The mean K6 score was also significantly lower in those with no history (ANOVA p < 0.001);
60% of the attempt group and 52% of the ideation group had a generalised anxiety (GAD-7) score of 15+, indicating severe anxiety, compared with 37% of those with no history (Pearson's Chi square p < 0.05). The mean GAD-7 was also significantly lower in those with no history (ANOVA p < 0.01);
38% of the attempt group and 35% of the ideation group had PHQ-9 score of 20+ indicating severe depression, compared with 12% of those with no history (Pearson's Chi square p < 0.01); The mean depression (PHQ-9) score was also significantly lower in those with no history (ANOVA p < 0.001);
Where it was recorded (n = 161), 94% of the attempt group and 92% of the ideation group had a personality disorder (SAPAS 3+), compared with 83% of those with no history (Pearson's Chi square p < 0.05). The mean personality score (SAPAS) score was also significantly lower in those with no history (ANOVA p < 0.001);
32% of the attempt group and 24% of the ideation group had had some previous engagement with services compared with just 5% of those with no history (Pearson's Chi square p < 0.001).
For other measures such as functional impairment (WSAS), there was a gradient from most severe in the attempt group through a medium in the ideation group to lowest in those with no history, such that the only significant difference was between the attempt group and those with no history:
54% of the attempt group had severe or moderately severe functional impairment (WSAS > 10) compared with 34% of those with no history (Pearson's Chi square p < 0.05). The mean WSAS score was also significantly higher in the attempt group (22.3) than in those with no history (17.2; ANOVA post hoc p < 0.05). Those in the attempt group had a significantly lower self-regard and optimism (22.6), that is, less self-efficacy, than those with no history (26.5; ANOVA post hoc p < 0.01) using the General Self-efficacy Score measure. Those in the attempt group had a significantly lower The Social Problem-Solving Inventory – Revised Scale score (5.2), that is, lower social problem-solving ability, than those with no history (score 10.9; ANOVA post hoc p < 0.05).
Discussion
Overall, the literature on effective interventions for suicide and suicidality in probation is scant as a recent systematic review reveals (Sirdifield et al., 2020). There have been papers published, however, on the epidemiology of suicide in probation. For example, Philips et al. (2018) have shown that, compared to the general population, the rate of suicide in probation is eight times higher. Pluck and Brooker (2014) examined suicide in a secondary analysis of data from a prevalence study of mental disorders in the Lincolnshire Probation Service (Brooker et al., 2012). They found that 25% to 40% of offenders serving all, or part of, their sentence in the community, had a lifetime history of self-harm and that 30% had, at some time, attempted suicide.
In this study, a secondary analysis of data was undertaken that has already been reported (Fowler et al., 2020). All of the probationers in the London CRC who scored over 12 on the K6 screening instrument were offered a psychological treatment package. The records (n = 274) of this group were identified, and the sample was classified into three groups; namely controls (n = 63), those with only suicide ideation (n = 111) and those who had attempted suicide (n = 100). Few significant differences were found between those with suicidal actions and those with suicidal ideation. When those who had attempted suicide and those with suicidal thoughts were compared to the control group, a range of variables significantly differed including general anxiety, severe depression, severe functional impairment, self-efficacy, lower problem-solving scores and use of mental health services (particularly referral to a psychologist).
Recent research with offenders (on much larger samples than ours) has shown that there are clear differences between those who have suicidal thoughts and those who may have suicidal thoughts and then actually attempt suicide (Favril and O’Connor, 2019; Favril et al., 2020a; Favril et al., 2020b). Favril and colleagues (2020a) examined 1212 adult prisoners, mostly men, in 13 prisons across New Zealand. The prisoners were divided into three groups: those with no suicidal history, those who thought about suicide but had never made an attempt and prisoners who had suicidal thoughts who then acted on them. A third of this total sample had thought about suicide at some point in their lives and just over half of these had attempted suicide (one in five of all in the sample). This, in comparison to our sample, where the figures are much higher; however, Favril et al. (2020a) had studied the general prison population, whereas the sample in our London study had already screened positive for a mental health problem. Favril and his colleagues found that some particular mental disorders were more associated with suicidal acts than others, these included: drug dependence (odds ratio [OR] 1.65), alcohol dependence (OR 1.89) and post-traumatic stress disorder [PTSD] (OR 2.09). The authors comment on these findings as follows: …disorders characterised by increased distress (anxiety) and decreased restraint (poor impulse control) are especially pertinent in predicting the transition from suicidal ideation to action (Favril et al., 2020a: 1151)
The authors of the study then discuss ‘ideation-to-action’ theories in the light of their findings. Ideation-to-action theories have been reviewed by Klonsky et al. (2016), and there are probably three main theoretical positions. Joiner (2005) described the interpersonal model where the perception of being a burden combined with ‘thwarted belongingness’ leads to an increased capability for suicide. In this paradigm, ‘increased capability’ is defined as overcoming fears of death and pain. O’Connor (2011) proposed an integrated motivational–volitional model. Here, it is argued that defeat and entrapment lead to suicidal ideation which prompts action when there is an acquired capability, for example, impulsivity or access to lethal means. Finally, Klonsky and colleagues propose a three-step theory of suicide (Klonsky and May, 2015). The key components here are pain/hopelessness, connectedness and suicide capacity. At the first step, ‘pain’ can be of any kind: social isolation, physical suffering and negative self-image, for example. However, the pain, to a great extent, must be irresolvable thus hopelessness is a key factor alongside pain. Step 2 on the path to a suicidal act occurs when there is a lack of connectedness, this can mean a lack of connection with a role or work, in short, those areas of life that give meaning. Once connectedness is disrupted, and pain/hopelessness is present then a suicidal act is more likely.
The findings from the New Zealand study (Favril et al., 2020a) have been replicated in a large sample of Belgian prisoners (Favril et al., 2020b). Again, it was found that mental health disorders featuring anxiety and poor impulse control, such as PTSD and/or substance misuse, were key factors in the reduced inhibition that might lead to a suicidal action. Propensity to be violent towards others and self-harm with important variables too.
Compared to the general population, this study showed high levels of suicidality in those screening positive for a mental health problem in the London Probation Service. We have also shown that there are few significant differences between those with suicidal ideation and those attempting a suicidal act in this small sample. Indeed, it is possible that the ideation group is a discrete blend between the no history and the attempt groups. The data we had access to in our study on suicide in probation did not allow the testing of hypotheses within the ideation-to-action model discussed above. This is because, unlike Favril's two studies, in this secondary analysis, we did not have access to key variables such as diagnosis, level of substance misuse, history of self-harm and level of violence towards others. The K6 screening tool only allows a statement about the likelihood of a mental health disorder above a certain score. The PHQ-9 focuses largely on aspects of depression. The GAD-7 aims to assess the severity of generalised anxiety. Specific details about alcohol and drug consumption were not available as part of our data set nor was their information about post-traumatic disorder. However, Favril and colleague's research in prisons is very encouraging and has applicability to probation settings. The prevalence studies of probationers have shown that anxiety, personality disorder and substance misuse are high (Brooker et al., 2012). These are all key predictive variables for suicide acts found in Favril's research. Also, we also know that social isolation, physical ill-health, unemployment and negative self-image are common features of the probation population from a health needs assessment undertaken using the Short Form-36 a global measure of health status (Brooker et al., 2009; MacKenzie et al., 2015; Power, 2020). Thus, the ‘pain’ and ‘hopelessness’ discussed by Klonsky and May, as a key first step along the path to a suicide act, would be commonly experienced by probationers.
Conclusion
A prospective large study of suicide in probation services, embedded in the ideation-to-action model, would be of great value in identifying interventions in probation services aimed at reducing the high suicide rates. The study would need to obtain diagnosis, levels of substance misuse, self-harm history and social status.
Footnotes
Acknowledgements
The authors are grateful to St Andrews Healthcare Research and Development Office for providing them with the research governance approval to conduct this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.