
Abstract
The association between attributional style (AS), problem-solving orientation (PSO), and gender on depressive symptoms was investigated in Egyptian adolescents with visual impairment (VI). After being written in Braille, measures of AS, PSO, and depression were administered to 110 adolescents with VI, ages 12–17 years, from a residential school for pupils with VI. Regression analyses showed that gender, negative general (NG) attributions, and negative problem-solving orientation (NPSO) were the strongest predictors of depressive symptoms in adolescents with VI, whereas negative internal (NI) attributions and avoidant problem-solving orientation (APSO) were weak predictors. The findings are discussed in relation to different perspectives and models of depression, particularly the stress-diathesis model. The theory that these cognitive variables are core constituents of a cognitive diathesis model of depression in individuals with VI is not supported by this study.
Introduction
Psychosocial adjustment to disability is determined by disability-related psychological/personality characteristics (Bishop, Smedema, & Lee, 2009; Livneh & Wilson, 2003). Interest in affective, cognitive, and behavioural personality characteristics of individuals with visual impairments (VIs) among educators and rehabilitation specialists is long standing. Some scholars insist that there is no special psychology of blindness (Adrian, Miller, & De l’Aune, 1982; Bak, 2012; Foulke, 1972). Some scholars believe that those with VI display the broad range of personality traits that are found in the general population (Bak, 2012; Oakland, Banner, & Livingston, 2000).
Adults with VI seemingly display more depressive symptoms and less well-being than individuals without disabilities (Cimarolli, 2006; Guerette & Smedema, 2011). Different theoretical perspectives have dominated depression research, including biological, cognitive, life-stress, interpersonal, and developmental psychopathology perspectives (Hammen, 1992; Rudolph et al., 2000; Spence, Sheffield, & Donovan, 2002). Each perspective has contributed despite its limitations.
For those with VI, depressive symptoms are thought to result from the social support and overprotection they receive together with the psychosocial stress associated with trauma incurred as a result of having a disability (Cimarolli, Reinhardt, & Horowitz, 2006; Livneh & Antonak, 2005). Negative life events (NLEs) are associated with the development of depression in typically developing adolescents (Spence et al., 2002). The presence of a disability has been viewed as a major NLE that may increase the risk for psychological problems and poor social and emotional adjustment in early adolescence (Bak, 2012; Celeste, 2006). Thus, one may expect that those with VI are at greater risk of developing depressive symptoms than their non-VI peers (Rudolph et al., 2000).Similarly, compared to other individuals with disabilities, those with VI may be more vulnerable to depression due to its greater negative impact on well-being compared to other disabilities (Bishop, 2005; Horowitiz, 2004; Wallhagen, Strawbridge, Shema, Kurata, & Kaplan, 2001). In addition, environmental events (e.g., parents’ marital conflict, separation, divorce, poverty, abuse, and high levels of daily hassles) have been shown to increase the risk of adolescent depression (Goodyer & Altham, 1991a, 1991b). Adverse events (e.g., teasing, rejection, and humiliation), all of which may apply to those with VI, may be more likely to contribute to the development of negative attributional styles (ASs) than would other types of life events (Rose & Abramson, 1992). However, the impact of disability is not specific to depression and increases the risk of a wide range of emotional and behavioural difficulties (Celeste, 2006, 2007). Furthermore, not all young people with VI show elevated levels of depression due to disability conditions or NLEs associated with their disability. Therefore, identification of the characteristics that influence the impact of disability and associated conditions on the psychological adjustment of VI remains important for researchers as well as practitioners.
Such characteristics include cognitive, behavioural, and emotional aspects of individuals with VI. According to cognitive diathesis–stress models, intrinsic cognitive characteristics may contribute to negative affective states or reduce the person’s ability to cope with or remove stressful events (Abramson, Alloy, & Metalsky, 1988). Such cognitive characteristics include, among others, AS and problem-solving orientation (PSO), and have been argued to represent a diathesis that may increase the development of depression (Abramson, Metalsky, & Alloy, 1988). Most research on cognitive models of depression has focused on AS as a cognitive diathesis as proposed by the hopelessness theory of depression (Abramson, Metalsky, & Alloy, 1989). The hopelessness model proposed that the tendency to attribute negative events to stable and global causes and positive events to unstable and specific explanations is associated with increased risk for the development of depression, but only in the presence of NLEs.
Cognitive factors contributing to depression
Cognitive diathesis models of depression highlight the role of cognitive vulnerability to depression. According to the reformulated theory of learned helplessness (RTLH), a pessimistic AS (i.e., a habitual pattern of interpreting the causes of negative events as internal [locus of control is within the person], stable [not likely to change over time], and global [affecting more than one domain of life]) creates a vulnerability to helplessness and depression in the face of NLEs (Abramson, Seligman, & Teasdale, 1978). The hopelessness model of depression, a revision of the RTLH, similarly addresses a cognitive diathesis to depression and predicts increases in depression for those with a maladaptive cognitive style through increasing hopelessness (Abramson et al., 1989). The negative cognitive style in the hopelessness theory of depression includes stable and global attributions for negative events as well as negative inferences for the future and self.
According to the hopelessness theory of depression (Abramson et al., 1989), the internal attributional dimension was associated merely with one particular symptom of depression (i.e., low self-esteem), while the global–specific and the stable–unstable dimensions by themselves were posited to be related to the risk for the development of hopelessness and depressive symptoms. Supporting this position, Joiner and Rudd (1996) report that while the attributional dimensions of stability and globalism reflect the same underlying factor, internality does not. A stable attribution helps explain the cause of a negative event in terms of long-lasting, constant factors, whereas an unstable attribution is transient. A global attribution helps explain that negative events can affect a wide range of situations. In contrast, a specific attribution generally has a more circumscribed impact. The stable and global dimensions combine to form a general composite dimension. The tendency to attribute bad events to stable and global causes is described as a depressogenic AS (Reijntjes, Dekovic, Vermande, & Telch, 2008).
The results of a number of studies that investigated various diathesis–stress theories in children have been neither consistent nor conclusive. Support for the diathesis–stress–hopelessness model of depression has been reported in several studies involving non-disability populations, including adults (Reilly-Harrington, Alloy, Fresco, & Whitehouse, 1999; Vickers & Vogeltanz, 2000), children, and adolescents (J. F. Dixon & Ahrens, 1992; Gibb et al., 2001; Rueger & Malecki, 2011; Vines & Nixon, 2009). Two meta-analyses reported strong and consistent support for an association between AS and depressive symptoms (Gladstone & Kaslow, 1995; Joiner & Wagner, 1995). However, support for the diathesis–stress component of the RTLH has been inconsistent (Joiner & Wagner, 1995). For example, Hammen, Adrian, and Hiroto (1988) and Nolen-Hoeksema, Girgus, and Seligman (1992) found only partial support for the model. One explanation for inconsistent results involves the developmental level of the samples. When young, children’s cognitions are developing and influenced by events and feedback. A cognitive diathesis is thought to become operative only after the development of abstract reasoning and formal operational thinking (Cole, as cited in Turner & Cole, 1994). Several investigations have demonstrated support for this explanation (Abela, 2001; Gibb et al., 2006; Nolen-Hoeksema et al., 1992; Turner & Cole, 1994). Tests of a cognitive diathesis that focus on samples in early adolescence or older people may add importantly to this literature.
Gender differences also may account for the inconsistent findings. Although gender differences were not apparent on measures of AS (Hankin & Abramson, 2002; Thompson, Kaslow, Weiss, & Nolen-Hoeksema, 1998), they may be apparent in the association between AS and depression (Gladstone, Kaslow, Seeley, & Lewinsohn, 1997). In addition, the results of a few studies that have examined possible gender differences in the cognitive diathesis model suggest that AS operates differently for boys and girls when stressful conditions vary (Abela & Payne, 2003; Morris, Ciesla, & Garber, 2008).
Problem solving (i.e., attitudes, skills, and abilities that enable a person to find effective or adaptive solutions to specific everyday problems) constitutes another cognitive factor (E. Chang & D’Zurilla, 1996; D’Zurilla, Chang, Nottingham, & Faccini, 1998). Similar to findings from AS research, poor problem-solving processes may represent a diathesis, interacting with NLEs in the development of depression (Adams & Adams, 1993; Cheng & Lam, 1997; Goodman, Gravitt, & Kaslow, 1995; Spence et al., 2002). For example, the display of a PSO that utilizes self-destructive or passive/avoidant solutions to life problems was found to predict future depression in the presence of NLEs among typically developing adolescents (Adams & Adams, 1996).
Specific problem-solving skills (e.g., problem definition and formulation, generation of alternative solutions, prediction of consequences, solution monitoring, and evaluation) together with a cognitive orientation that the individual takes to the occurrence and management of problems seemingly help to account for depression (Haaga, Fine, Terrill, Stewart, & Beck, 1995). Problem orientation refers to the cognitive, emotional, and behavioural variables that reflect a person’s awareness of, beliefs in, appraisals of, and expectancies for relating to both the occurrence of problems and ability to solve them. A negative problem-solving orientation (NPSO) relates to those cognitions and emotions that are proposed to inhibit adaptive problem solving. Several studies have demonstrated strong associations between a NPSO and depression (D’Zurilla et al., 1998; Sadowski & Kelly, 1993).
This study was designed to examine the association between cognitive variables represented in AS and PSO and depressive symptoms in adolescents with VI. Additionally, the study aimed to examine whether the cognitive diathesis–stress model of depression can account for the presence of depressive symptoms in Egyptian adolescents with VI.
Method
Participants
Participants originally included 110 middle and high school pupils aged 12–17 years. This number was later reduced to 91 due to attrition (56 males and 35 females). The sample was drawn purposefully from a residential school for children with VI in the largest city in Upper Egypt. This region is located in a southern part of the country, one that typically is seen as being less modernized than Lower Egypt located in the northern part of the country. The school provides institutionalized education service for children aged 6–18 years with VI from different regions and villages. The type of VI (i.e. acquired vs congenital) and the severity of the vision loss were not considered in the selection of the participants. Thus, the participants included both types and varied with regard to the severity of the vision loss. School officials agreed to participate in this study following its approval by the ethical committee at the university with which the researcher was affiliated.
Procedures
The researcher informed the school principal and teachers about the rationale of the study and its aims. Participant approval was obtained from either their parents or them personally. Participants were informed that they would be filling in questionnaires about their personal views, feelings, and attitudes. The chosen scales were adapted through translation to the Arabic language. The translation process uses consecutive and back-translation methods (Hambleton, Merenda, & Spielberger, 2005) by the authors. A third translator who had background in educational psychology conducted the back-translation while having no access to the original questionnaires. Two translations were sufficient to achieve a desired adaptation. The study instruments were then written in Braille in order to avoid misinterpretation by the participants if they were to have the statements read to them by their teachers. Each scale was labelled with a pupil code in order to ensure confidentiality.
Instruments
The following instruments were administered: the Beck Depression Inventory for Youth (BDI-Y), Depression subscale of the Adolescent Psychopathology Scale (APS, long form; Reynolds, 1998), Social Problem-Solving Inventory–Revised (SPSI-R) Short Form, and Children’s Attributional Style Questionnaire–Revised (CASQ-R). An overview of these instruments is presented in the following:
BDI-Y
BDI-Y is part of the Beck Youth Inventories that contain five scales that may be used separately or in combination to assess a child’s depression, anxiety, anger, disruptive behaviour, and self-concept (Beck, Beck, & Jolly, 2001). Reliability estimates indicate that the BDI-Y has moderate internal consistency (α = .75).
Depression subscale
The depression subscale from the APS (long form; Reynolds, 1998) was administered in order to obtain criterion validity of the BDI-Y. APS is a 346-item self-report that assesses psychopathology, personality, and social–emotional problems. It is used to assess psychological problems and behaviours that may interfere with an adolescent’s psychological adaptation and personal competence. The depression subscale consists of 20 statements that measure depressive symptoms by asking the respondents to rate how often each item occurs for them on a 3-point scale ranging from 0 (almost never) to 2 (almost every day). The APS was standardized on a large Egyptian sample. Its alpha internal consistency reliability estimates are good for its different scales (Cronbach’s alpha ranges were as follows: α = .79−.82) (Elbheary & Emam, in press). Alpha internal consistency estimates for the depression subscale were good (α = .80) (Elbheary & Emam, in press). Correlations between the BDI-Y and APS’s depression scale are moderate (r = .72, p < .01), reflecting the validity of the BDI-Y.
SPSI-R Short Form
SPSI-R Short Form (D’Zurilla & Mayday-Olivares, 1995) was used to assess PSO. The SPSI-R was originally developed to assess both PSO and interpersonal problem-solving skills. The SPSI-R Short Form is a 25-item self-report questionnaire on which respondents rate how true each item is for them on a 5-point scale ranging from 0 (not at all true of me) to 4 (extremely true of me). Five subscales, each containing five items, are contained within the SPSI-R Short Form. These scales relate to positive problem-solving orientation (PPSO), NPSO, avoidant problem-solving orientation (APSO), impulsive problem-solving orientation (IPSO), and rational problem-solving orientation (RPSO). Although research studies on psychopathology showed that there is an association between NPSO and depression as well as suicidal ideation (D’Zurilla et al., 1998; Sadowski & Kelly, 1993), the study explored the association between other problem-solving styles that were not highlighted in previous studies. Alpha reliability estimates of the five subscales were found to be good (PPSO, α = .76; NPSO, α = .80; RPSO, α = .74; IPSO, α = .78; and APSO, α = .79).
CASQ-R
CASQ-R (Seligman et al., 1984) was used to assess the ASs. The CASQ-R consists of 24 items with six subscales that provide internal, stable, and global scores for both positive and negative events. Each item consists of a hypothetical event for which respondents are required to choose the most likely explanation from a choice of two alternatives. Each subscale contains four items with scores ranging from 0 to 4. A composite positive event score is calculated by adding together the internal, stable, and global scores for positive events. Similarly, a composite negative event score is calculated by adding together the internal, stable, and global scores for negative events. An overall composite score for AS may also be calculated by subtracting the composite negative event score from the composite positive event score, with lower scores indicating a more depressive AS. The psychometric properties of the CASQ-R have been shown to be acceptable yet not strong, with moderate internal consistency and fair test–retest reliability (Thompson et al., 1998). Scoring was based on the following scores that comprise the CASQ-R: positive internal (PI), positive stable (PS), positive global (PG), negative internal (NI), negative stable (NS), and negative global (NG). Alpha reliability estimates of the six subscales are good except for the PG that is relatively low (PI, α = .72; PS, α = .79; PG, α = .65; NI, α = .73; NS, α = .76; and NG, α = .69).
Analysis
After conducting correlation analyses, the data were examined separately for cross-sectional set using linear hierarchical regression analyses. Significant correlations between depression scores and predictor variables ranged from .25 (p < .05) to .32 (p < .01). For regression analyses, gender was entered in the first step of each regression analysis, given that female gender has been shown to be a risk factor for depression in previous research (Lewinsohn, Hops, Roberts, Seeley, & Andrews, 1993).
Results
Regression analyses
The results of the hierarchical regression analysis predicting BDI-Y scores through AS subscales, β values, and significance levels are reported in Table 1. Gender was entered into the equation first. The NI, NS, NG, PI, PS, and PG scores were entered into the equation second in one block. The final equation explained 23% of the variance in BDI scores and was significant, F(7, 90) = 3.56, p < .001. Gender, NI, and NG were significant predictors of BDI score.
Standardized beta values for cross-sectional hierarchical regression analysis examining predictors of depression symptoms through attributional styles.
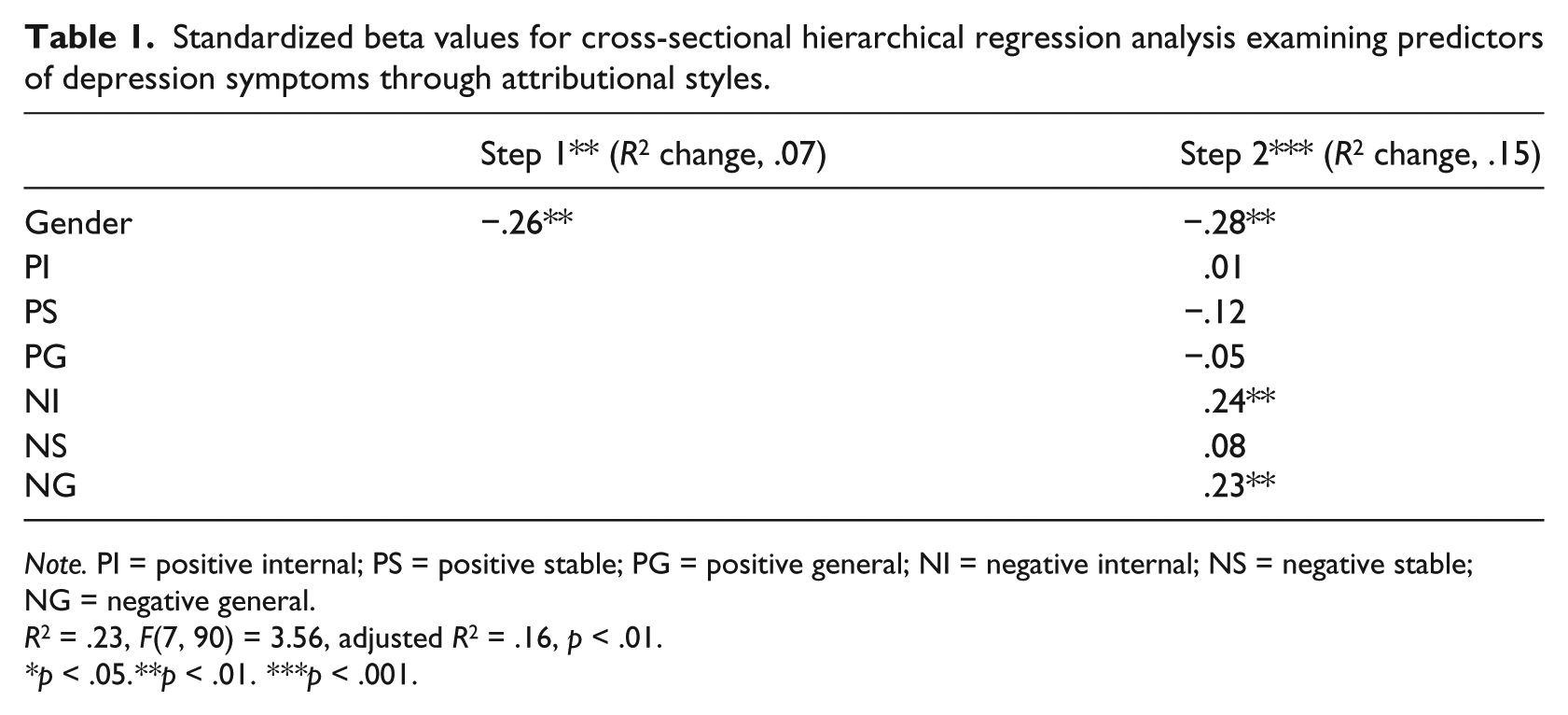
Note. PI = positive internal; PS = positive stable; PG = positive general; NI = negative internal; NS = negative stable; NG = negative general.
R 2 = .23, F(7, 90) = 3.56, adjusted R 2 = .16, p < .01.
p < .05. **p < .01. ***p < .001.
Thus, participants who reported higher levels of depressive symptoms were more likely to adopt an AS that can be described best as being negative and subject to internal or global explanations. Both NI and NG attributions show that participants tend to display pessimistic AS and to have negative or unconstructive attitudes and beliefs relating to life events. Gender was also significantly associated with depression scores. Girls reported higher depression scores than did the boys and therefore are more vulnerable to depression.
The results of the hierarchical regression analysis predicting BDI-Y scores through PSO subscales, β values, and significance levels are reported in Table 2. Gender was entered into the equation first. The PPSO, NPSO, RPSO, IPSO, and APSO scores were entered into the equation second in one block. The final equation explained 21% of variance in BDI-Y scores and was significant, F(6, 90) = 3.71, p < .001. Gender, NPSO, and APSO were significant predictors. Thus, there is an association between NPS as well as APS and depression score among adolescents with VI.
Standardized beta values for cross-sectional hierarchical regression analysis examining predictors of depression through problem solving orientation.
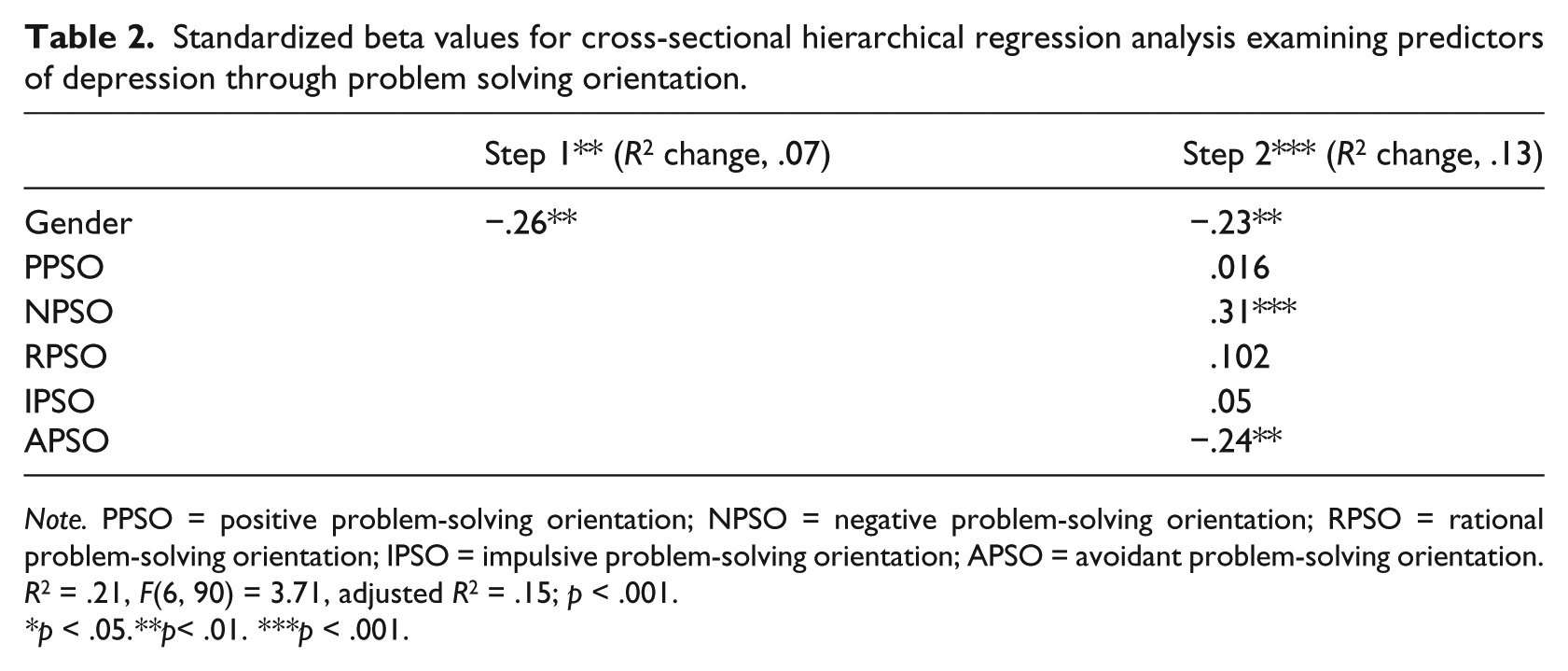
Note. PPSO = positive problem-solving orientation; NPSO = negative problem-solving orientation; RPSO = rational problem-solving orientation; IPSO = impulsive problem-solving orientation; APSO = avoidant problem-solving orientation.
R 2 = .21, F(6, 90) = 3.71, adjusted R 2 = .15; p < .001.
p < .05. **p< .01. ***p < .001.
Thus, participants who reported higher levels of depressive symptoms were more likely to have NPSO in dealing with life issues, including their disability-related conditions. The association corresponds to their NI as well as NG attributions. It is more likely that the participants behave negatively when faced with various problems in life. They may also adopt an avoidant style that suggests that they may manoeuvre rather than confront the problems.
Relative contribution of significant variables
The significant variables that resulted from previous hierarchical regression analyses were combined into one final model to test their contribution to the participants’ depression composite scores. The results of the hierarchical regression analysis predicting BDI-Y scores through the five contributing variables, β values, and significance levels are reported in Table 3. Gender was entered into the equation first. The NPSO, APSO, NI, and NG scores were entered into the equation second in one block. The final equation explained 26% of the variance in BDI-Y scores and was significant, F(5, 90) = 6.20, p < .001. Gender was a strong predictor of BDI-Y score. The NPSO and NG remained good predictors of BDI-Y score. However, NI and APSO became insignificant predictors of BDI-Y score.
Standardized beta values for cross-sectional hierarchical regression analysis examining the relative contribution of the predictor variables of depression symptoms.

Note. NPSO = negative problem-solving orientation; APSO = avoidant problem-solving orientation; NI = negative internal; NG = negative general.
R 2 = .26, F(5, 90) = 6.20, adjusted R 2 = .22, p < .001.
p < .05. **p < .01. ***p < .001.
Discussion
The study examined whether individual characteristics of AS and life problem-solving skills can predict their depressive symptoms among Egyptian adolescents with VI. The study also examined whether those cognitive variables that are essential components of the cognitive diathesis model can account for the presence of depression in Egyptian adolescents with VI. The model posited that AS and PSO represent a cognitive diathesis that operates in the presence of NLE such as the presence of a disability. More specifically, the model proposed that the negative dimensions (i.e. negative AS, NPSO) directly influence the presence of depressive symptoms (Abramson et al., 1989).
The results did not support the cognitive diathesis–stress model. In the hierarchical regression analysis, all NI, NG, NPSO, and APSO attributions were associated with depressive symptoms. Adolescents were more likely to report higher levels of depression when they held a pessimistic AS. This finding is consistent with the conclusions of a meta-analytic review of the literature reported by Joiner and Wagner (1995) on typically developing adolescents. However, the contribution of the constituent variables of the model explained a small proportion of the BDI-Y scores (23% for NI and NG, and 21% for the NPSO and APSO). In addition, the p values reported in Tables 1 and 2 for these variables do not reflect their paramount role in the participants’ display of depressive symptoms. Additionally, the hierarchical regression analysis of these significant variables, including gender, explained 26 percent of the BDI-Y scores. When the significant variables were combined into one model for analysis, NI and APSO became insignificant predictors of BDI-Y scores in adolescents with VI.
These findings can be compared with those from other research with individuals without disability. Joiner (2000) noted the conflicting results emerging from studies examining the cognitive diathesis–stress model of depression with children and adolescents. The findings of this study, with respect to AS, are inconsistent; Joiner’s results found that AS contributed importantly to depression in a clinical sample. Similarly, the findings by Hilsman and Garber (1995) provided support for the cognitive diathesis model in relation to the prediction of depressive symptoms by negative attributions. As previously noted, other studies have not supported the cognitive diathesis–stress model involving AS. Given the marked variation in methodology used across different studies, such as sample size, sample characteristics (age and clinical vs community samples), and measures used to assess cognitive styles, such variation in results is not surprising.
Despite evidence for the correlational link between negativistic thinking and depressed mood, the diathesis model was argued to have several shortcomings. Although the diathesis model purports to explain aetiology of depression, a number of research studies that tested causal predictions have indicated relatively weak support (e.g. Hammen et al., 1988; Rudolph et al., 2000). These studies report that cognitions that represent alleged underlying vulnerability factors are, in fact, concomitants or even consequences of depression, and their status as underlying vulnerability factors is unclear.
Given these shortcomings of the cognitive diathesis models, alternative explanations were offered to account for depression. Most of these explanations gained support from empirical studies on typically developing adolescents. Rueger and Malecki (2011) posit that models based on social support literature can provide some explanation for the display and development of depression by individuals. The main-effect model, which suggests that social support offers a positive effect through an increased sense of well-being under all conditions, and the stress-buffering model, which suggests that social support provides greater benefit under the negative effects of stress, are examples of social support–based models, which can provide us with clearer understanding of depression shown by individuals. The role of parental support is a good example in this respect. Rueger and Malecki (2011) found that there is an interaction between AS and perceived parental support and the development of depressive symptoms with noteworthy gender differences in typically developing adolescents. Unfortunately, none of the social support–related variables were included in this study despite the significant role of social support in the lives of individuals with disabilities (S. Chang & Schaller, 2000; Cimarolli & Boerner, 2005).
The social and interpersonal domain for depression vulnerability may similarly be another viable explanation for adolescents’ display of depressive symptoms. Vulnerability to depression is based on interpersonal factors, interpersonal skills and behaviours of the depressed person, and consequences of depression on interpersonal relationships. These areas, none of which were explored in this study, can increase our understanding of depression in adolescents with VI if they are examined at the levels of family and peer relationships (Rudolph et al., 2000).
The finding that NPSO remained a significant predictor of depressive symptoms is of interest. Although the model, including the significant predictor variables, explained a small proportion of the depression scores, NPS can increase the risk for depression in individuals with VI. There are various theoretical interpretations that may explain this finding. D’Zurilla et al. (1998) stressed the importance of cognitive and emotional components of problem solving, particularly with regard to a person’s appraisals, beliefs, and expectancies relating to the occurrence of problems and his or her ability to solve them. These authors also discuss the self-efficacy component of PSO and the association between hopelessness and low self-efficacy expectations for problem solving.
An NPSO also could be hypothesized to fit within the hopelessness theory of depression. According to the hopelessness theory of depression (Abramson et al., 1989), a range of attributions, inferences, and expectancies relating to the occurrence of NLEs are suggested to lead to hopelessness and thereby increase in the risk for developing depressive symptoms. These variables include inferences relating to negative characteristics about the self that was shown to apply to individuals with VI (D’Zurilla et al., 1998). Variables such as low self-efficacy or low self-confidence expectations for problem solving could fit within this model. Unfortunately, this study did not include a measure of such variables to examine their mediating role in the presence of depressive symptoms.
Limitations
Several methodological issues should be considered when interpreting the findings from this study. First, the study relied on self-reports of the individuals with VI, which could have affected the findings due to the reporter bias. Replications of the study should consider obtaining data by direct observation as well as teachers’ observations on externalizing behaviours, which are known to associate with the internalizing depression symptoms. Second, given the small sample size of this study, the study findings cannot be generalized. Therefore, future replications of this study should include larger representative samples and different age groups, including adults, to give support to the findings of this study. Third, the translation of the measures into Arabic and presenting the measures in Braille could have produced minor variation in the psychometric properties of the measures. A related point concerns the use of the 24-item version of the CASQ to assess AS, and not the 48-item version that was used by Joiner (2000) and Hilsman and Garber (1995). The difference between the two versions was believed to account for differences in the study variables with adolescents without disabilities (Spence et al., 2002). Fourth, this study did not consider the duration of the VI, as it included participants with both acquired and congenital VI as well as with varying degrees of the severity of the vision loss. Dissection of the participants in future studies is also recommended. Such dissection may help identify whether the cognitive diathesis model accounts for the development of depression in certain types of VI. Fifth, this study was also limited in that it restricted the investigation to depressive symptoms. Therefore, conclusions cannot be drawn as to the specificity of the findings in relation to depression versus other forms of psychopathology, such as anxiety. In line with Joiner (2000), it would be valuable if future studies examined whether the cognitive diathesis–stress effect of NPSO is specific to depression or is also relevant in the development of anxiety and externalizing problems. Finally, in this study, gender sample sizes were too small to run separate multiple regression analyses for boys and girls. Such analysis could have provided insight into how gender contributes to depression in individuals with VI in the presence of other cognitive factors such as PSO and AS.
Conclusion and implications
NG attributions and NPSOs were found to predict depressive symptoms in Egyptian adolescents with VI. The findings are inconsistent with a cognitive vulnerability model of depression for adolescents without disabilities, which reports that cognitive variables explain the presence of depression when individuals experience NLEs. The findings of this study found that these cognitive variables explained a small proportion of the presence of depressive symptoms in participants. However, findings may have implications for preventive interventions for individuals with VI. The results suggest that, in addition to enhancing AS, attention should be paid to PSO as a component of programmes designed to prevent depression for adolescents with VI.
The importance of the role of gender in the study of depressive symptoms should not be overlooked. The current findings supported similar findings from previous research, which reports that gender plays a paramount role in the cognitive diathesis model of depression and how it interacts with both AS and PSO (Abela & Payne, 2003; Hankin & Abramson, 2002; Morris et al., 2008; Spence et al., 2002; Thompson et al., 1998). Girls were more vulnerable to be affected by their NI attributions and NPSO in relation to depressive symptoms.
The findings may have a number of implications for the education of and service provision for adolescents with VI in Egypt. Most notably, the Arabic versions of the measures used in the study were shown to be reliable and valid when used in Egypt for research and practice purposes. Several components of the data provide support for its reliability and validity. The findings extend our understanding of adjustment problems among Egyptian adolescents with VI by capturing the association between PSO and AS and how they interact and increase their risk for depression. Information from the study allows teachers and service providers to compare the role of these cognitive variables with other perspectives in their contribution to the development of depression in individuals with VI. These may include the study of social support and coping with the disability condition in those with VI whether they are in residential or inclusive settings. In addition, replication of this study is recommended on different community and age samples with specific types of VI to compare with other similar studies in Western cultures and within the Egyptian culture. Although the study did not prove a causal relationship between the cognitive variables of AS and PSO and the presence of depression, these variables can be useful in planning interventions for Egyptian adolescents with VI. Attribution training- and problem solving–based interventions can target Egyptian adolescents with VI who are at risk of developing depression. The application of the cognitive diathesis model of depression may be replicated with larger samples with specific types of VI as well as with other types of disabilities in the Egyptian culture to validate the model cross-culturally.
Footnotes
Acknowledgements
The author would like to thank Professor Thomas Oakland at the University of Florida for his editorial remarks on the final draft of this article. The author would also like to thank the British Journal of Visual Impairment and the reviewers for their comments on the earlier drafts of the article.
Declaration of conflicting interests
The author declares that there is no conflict of interest.
Funding
This research was funded by Assiut University Research Fund for Humanities Studies (AURFHS).