
Abstract
The focus of this article is on how musical interaction can contribute to bonding and early interaction. This article is based on a music therapy project in a pedagogical institution for people with visual impairment. The study is qualitative and exploratory, where children with visual impairments (aged 1–4 years) and their caregivers participated in music therapy sessions over 10 weeks. Data have been collected by participant observation, video recordings, and interviews. Moments of positive interactions in music were selected and analyzed, and the selections were triangulated by interviews with the caregivers. The data material indicates that music therapy promotes positive bonding patterns and enhances early interaction. Musical interaction facilitates elements of early interaction that can be challenging for children with visual impairments and their sighted caregivers. Both caregivers and children seemed to experience one another as a source of joyful interaction. This article discusses the findings in the broader perspective of disability studies and community music therapy and argues that music therapy promotes positive interactions and empowerment of children with visual impairment and their caregivers.
Introduction
Human beings are social in nature (e.g. Buber, 1923/1965) and they need companionship for development. Companionship links to mutuality, recognition, bonding, and belonging (Baumeister & Leary, 1995; Inclusion International, 2012). Children with visual impairments and their caregivers often face several challenges in the first years of the child’s life. These challenges may both be linked to their relationships and everyday life and to broader structures in the community (Barnes & Sheldon, 2010; Bigelow, 1995; Brambring, 2006). Larssen and Wilhelmsen (2008) consider vision as a motor for the development of social and practical knowledge, body awareness, as well as space and direction sense. Bonding, the deep emotional connection between caregiver and child, and early interaction are especially challenging due to the different perception styles and the vulnerable situation (Corneliussen & Skjærseth, 2003; Fraiberg, 1977; Hobson, 1993). Vision seems to promote social interaction and bonding as it facilitates joint attention (e.g. mutual focus on an activity) (Fraiberg, 1979; Stern, 1985/2000). However, interaction and bonding are totally possible if parents and others can adjust themselves to the child with visual impairment and use touch and their voices to establish a relationship and attend to, for example, body movements and the child’s sounds instead of the face (Bigelow, 1995; Preisler, 1991).
Other challenges for families with a child with visual impairment can be caused by societal structures (Vision 2020, 2007) such as access to education and health services. Children with visual impairments and their families are, depending on the socioeconomical context, considered to be one of the most marginalized groups in the world (Vision 2020, 2007). Brambring (2006) and Jantzen (2002/2004) have elaborated on stigmatization and the loss of social and cultural capital of families with children with disability. As the World Health Organization (2004) states, social and economic issues also influence the quality of the relationship between child and caregiver. However, it is important not to generalize families that have children with disabilities as dysfunctional families (Read, 2000). Alternatively, it is good to be conscious about their challenges in the society we live in.
Music therapy can be seen as “the relationship between music and health” (Stige, 2002, p. 198) and has been proposed as a resource for bonding, attachment, and early interaction for families in challenging life situations (Edwards, 2011; Jonsdottir, 2008; Trevarthen & Aitken, 2001). Music therapy has been defined as an effort “to increase the possibilities of action” (Ruud, 1998, p. 32). These “possibilities of action” are not only challenged by individual preconditions but also by societal barriers (Ruud, 1998). In this project, one assumption was that music therapy could provide a space where caregivers and children could mutually interact and experience turn-taking, attunement, and bonding.
The anthropologist Blacking (1973) proposed that all humans are “musical” from birth. We all have an innate capacity for communication through music, and early parent–infant communication is intrinsically musical (Malloch, 1999). Research on early interaction between children and caregivers has shown that children are born to be sociable, to communicate, and to share meaning with others (Trevarthen & Malloch, 2000). Trevarthen and Aitken (1994) point out that the human being is born with what they call a system for intrinsic motive formation (IMF). This system seeks intersubjectivity and makes cultural learning in companionship possible (Trevarthen & Aitken, 1994, 2001). There is a similarity between forms of musical interaction between client and music therapist and early caregiver–infant interaction (Edwards, 2011; Tønsberg & Hauge, 2008), and both forms of interaction are built on rhythm, attunement, and turn-taking. As Edwards (2011) points out, music therapists can offer a musical space or container in order to help caregivers and their children in a non-intrusive way. For Jonsdottir (2008), musicking, 1 in the context of early intervention, is possibly the most effective way of providing help to families.
A review of different literature 2 reveals that the field of music therapy in the context of visual impairment is rather under-developed. Although there is no literature that involves caregivers in the music therapy process, there are comments that emphasize the relevance of music therapy for parent–infant bonding (Codding in Kern, 2006). 3 The reviewed literature shows a rather individualized view of disability. As the challenges of children with visual impairment and their caregivers need to be seen in their sociocultural context (e.g. Tellevik, 2008), a community music therapy stance is useful. Community music therapy provides a perspective that reaches beyond the dyad of music therapists and clients in a music therapy room, is sensitive to context and culture, challenges structures in society, and explores the relationships between society, the individual, music, and health (Ansdell, 2002; Pavlicevic & Ansdell, 2004; Stige & Aarø, 2012). Therefore, community music therapy provides a theoretical background on how musical interaction within the family relates to culture and social participation.
The aim of this article is to contribute to the literature where research is lacking on music therapy, bonding, and families with visual impairment. This article will also explore how making music together contributes to bonding patterns and quality of social interaction for children with visual impairment and their caregivers. Based on the literature review, personal clinical experience, and the identified literature, the research question for this study was defined as follows: What can joint music-making afford 4 children with visual impairment and their caregivers in terms of bonding and social interaction?
Methodological approach
This project was anchored in qualitative research with a research approach informed by ethnography and emancipatory disability research (Barnes, 2003). Qualitative research is often used in exploratory studies (Hammersley & Atkinson, 2007). As it is not the first time I am writing about this topic (Metell, 2011; Metell & Stige, submitted), having personal interest and pre-understanding, I need to use an approach that is reflexive (Alvesson & Sköldberg, 2000/2009). Reflexivity is a characteristic of qualitative research (Hammersley & Atkinson, 2007). Reflexivity is especially important, as I am researching my own practice and need to reflect upon the different roles of researcher, music therapist, and visual impairment pedagogue. To research one’s own practice is a common approach in music therapy, although the double role of researcher and music therapist can be challenging and calls for critical reflection (e.g. Rickson, 2009).
This study was approved by Norwegian Social Science Data Services (NSD 5 ; project number 31102), and each of the caregivers provided written informed consent regarding research participation. A letter that explained the objective of the study and detailed information on confidentiality, treatment of the video recordings, and possible publications was handed over.
The project was conducted in a pedagogical institution where the families participated in an early intervention program conducted by special teachers 6 once a week. Music therapy sessions conducted by the author were offered over 10 weeks. The number of sessions varied from one to seven, and the sessions lasted around 25 min.
Participants
The choice of participants 7 was done in collaboration with the special teachers working in the early education program. This generated a form of purposeful sampling (Tracy, 2013, p. 154) as they chose participants who would probably contribute to the initial research question. The inclusion criteria were as follows: (a) the child had to be between 0 and 3 years 8 and diagnosed with a visual impairment, and (b) they had to have one caregiver interested in participation. I did not exclude children with additional special needs (Table 1).
Overview of the participants.
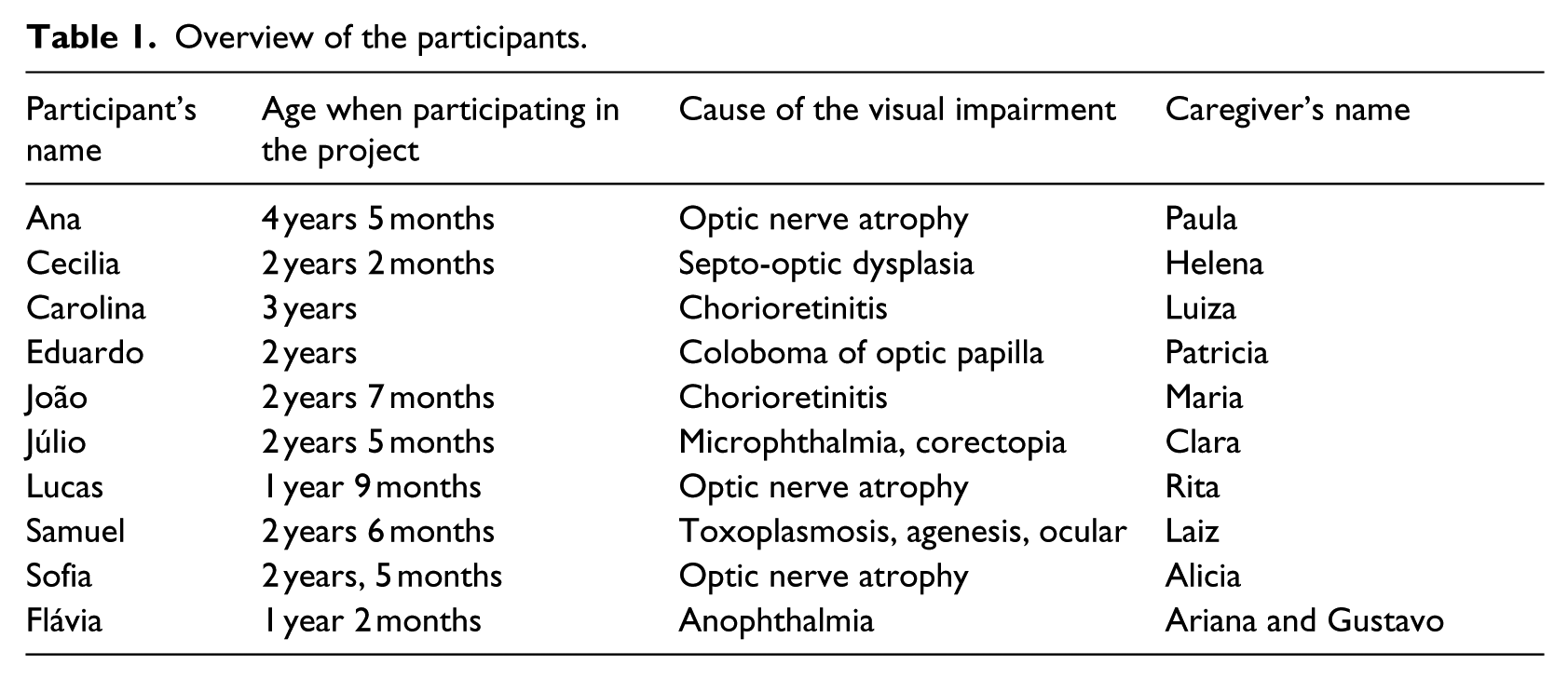
Four children were congenitally blind. All children had additional diagnoses of conditions such as cerebral palsy, syndromes, and epilepsy.
Two children had some verbal speech (Cecilia and Eduardo). The background of the participating caregivers varied. Most were young, single mothers from socioeconomically disadvantaged backgrounds.
Data collection
Four sources of data are used in this study: field notes (Stige & Aarø, 2012), participant observation (e.g. Davies, 1999/2002; Stige & Aarø, 2012), interviews with caregivers and professionals (Tracy, 2013), and video footage of the music therapy sessions (Galaasen, 2010; Packer, 2011).
Data selection
The data material consists of 48 session notes, 29 field notes, three interviews with caregivers, and one interview with two special teachers. The video footage of the moments that were identified as special in terms of companionship and mutuality were micro-analyzed. Micro-analysis means to focus on “minimal changes in relationships or interactions between people or minimal changes in the music and in dynamic forces” (Wosch & Wigram, 2007, p. 14). I selected one to four moments of each participating child with its caregivers. I selected moments where caregiver and child were mutually interacting and seemed engaged positively and moments that contrasted this quality of interaction.
To provide a broader picture, the initial selection of moments was triangulated, and I showed the chosen video recordings to the caregivers and conducted interviews that focused on their experience of the moments. I only had the opportunity to interview three caregivers during the fieldwork period. Furthermore, I conducted an interview with two special teachers on their view of music in early intervention and chose field notes, session notes, and comments referring to the moments I selected.
Data analysis
Data analysis is the search for patterns in the collected data (Riemer, 2012). In qualitative research, data collection and fieldwork are intertwined, and my pre-understanding, clinical experience, and previous studies shaped my data analysis.
The selected moments were transcribed in a notation system that includes musical notation, the infant’s behavior, the caregiver’s behavior, and the music therapist’s behavior. The interviews were transcribed. For publication, I translated the caregivers’ comments and quotes from Portuguese to English. My data analysis followed the steps for thematic analysis as described by Braun and Clarke (2006): “1. Becoming familiar with the data. 2. Generating initial codes. 3. Searching for themes. 4. Reviewing themes. 5. Defining and naming themes. 6. Producing the report” (p. 87)
Findings
The categories are the results of a cyclical process between the data gathered from fieldwork and my professional background and experience. This process resulted in the selection of three main categories:
Early interaction and bonding in music
Music’s affordances for children and their caregivers
Musical interaction as resource in everyday life
Early interaction and bonding in music-making
“A great moment . . . because of the music.”
Across the selected video sequences, there were visible elements such as synchronization, responsiveness, turn-taking, and attunement. These elements are associated with early interaction and bonding.
Togetherness
A common topic in the analysis was to share something on a mutual basis and to do something pleasurable together. Being together in rhythm seems an important part of togetherness for the dyad: Ana sits in front of her mother and bounces a tambourine on the floor. Her mother Paula starts singing. After a few seconds, Ana turns her head in direction of her mother and seems to pay attention to her mother. She starts rocking in rhythm of her mother’s singing.
The feeling of being together in rhythm and music can be linked to the concept of synchronization. Responsiveness appeared as another important concept whereby it is possible for caregivers to demonstrate to the children that their initiatives are perceived and understood: Carolina reaches out for her mother with her right hand and claps in her hands. Luiza looks at Carolina and turns her body to her daughter. Carolina smiles and Luiza starts to dance and to laugh, still looking at Carolina. Carolina leans forward to Luiza and Luiza responds immediately leaning forward to Carolina. Both are moving in rhythm, smiling, and lean forward until they noses touch. They laugh and both turn back to playing.
This moment is not only an example of responsiveness and turn-taking but also a moment of intimacy. Responsiveness and intimacy are linked to bonding (Papousek, 1996) and are concepts not only relevant for Carolina and Luiza. The quality of Paula’s voice changed a lot depending on Ana’s positive responses, and this attunement to Ana’s emotional state seemed closely linked to experiences of bonding and attachment. Compared to situations outside music when Paula talked to Ana, there was much more affection in her voice. Another sequence with Sophia and Alicia highlights attunement: Sophia sits on Alicia’s lap and seems agitated. I improvise on the guitar and she calms and starts rocking in the rhythm of the guitar play. Alicia moves together with Sophia and Sophia realizes that. Sophia starts to vocalize in the harmony of the guitar play.
Often, I noted that responsiveness seems to be a difficult interactional element, as the children’s movements are not interpreted as initiatives: We are playing a Brazilian childhood song. Sophia reaches out for the drum in front of her, but Alicia lifts her up and takes her on her lap.
However, the findings of the analysis showed that caregivers who participated in more sessions showed an increase in the frequency of mutual interaction.
Joint attention
“He was sharing something with me,” said Clara when I asked her about how she experienced the sequence I showed her. From what I understand, she had the experience that Júlio and she were doing something together, paying attention to the same action, and being conscious about sharing something – in my view, sharing links to the experience of sharing attention or having joint attention. According to the video material, familiar songs seem to facilitate joint attention: Clara is singing a Brazilian lullaby to Júlio and I am accompanying her on the guitar. As she sings “he will pick up Júlio” Júlio starts laughing, shakes his head and vocalizes “Dedede.” Clara laughs at Júlio and continues singing. All three of us are smiling.
In the sequence with Alicia and Sophia described above, joint attention was established when Alicia accompanied Sophia’s rocking and Sophia realized that. Besides using the voice, physical contact appeared as a facilitator. In all analyzed moments, the caregivers used touch in order to establish joint interaction.
Happiness
Happiness is the topic that most clearly goes through interviews, field notes, and video footage. Happiness is visible in the recorded moments through smiling and laughter and appears frequently in the interview data. The three interviewed caregivers reported that they were happy in those moments I showed them and linked this to the happiness of their children:
“Together with him music is perfect. He likes when I sing to him and I like it, too. Both are happy . . . happiness. He is together with me dancing, happy with me, and I am happy with him. Both happy.”
Body contact and movement
Touch and physical contact emerged as an important theme in order to establish or maintain contact: Flávia (14 months) sits on her mother’s lap. Flávia is moving her feet, her mother comments on this movement immediately and I start to play in rhythm of her movement. Flávia starts smiling and starts to move with her whole body held by her mother, who smiles and joins her in movement.
Touch was often used to establish contact and to reaffirm that the caregiver was paying attention. Similarly, the children used touch in order to seek attention or involve their caregivers in a new action. Touch and movement highlight the relevance of amodal perception, the capacity to process and translate a sensory impression across modalities (Stern, 1985/2000), for interaction of the dyad. So, in one selected moment Ana transfers rhythm, intensity, and structure of a refrain into physical movement. Paula sees her engagement and motions, then in turn smiles and sings with more intensity.
Reflections on the music therapist’s role
From the analyzed moments, it was possible to identify how my own participation and role in facilitating interaction differed a great deal. In the cases of Clara and Júlio and Paula and Ana, I was accompanying their songs. The most important aspect of my role at that time was to support the mother and to encourage her to sing and interact by playing and smiling, further, to support all the child’s initiatives. In the case of Sophia and Alicia, I improvised based on Alicia’s rocking and her vocalization. With Carolina and Luiza, I played and sang a children’s song while they interacted. Across all moments, the main aspect of my role was to facilitate interaction between caregiver and children and to provide a musical and social space. This requires the allocation of meaning to the initiatives of both of them and to engage them both in an activity. In general, I experienced the triadic work as very meaningful in the context of children with visual impairment and their caregivers. However, there was one dyad that had so many interactional challenges that I gathered the impression that the child would benefit a lot from additional individual sessions, and probably the mother too.
Music’s affordances for children and their caregivers
Affordances for the caregivers
For Clara and Paula, seeing their children as being able to take part in play and interaction appeared important:
“It was great – he knew what to do.”
“And when she does the things I am feeling happy.”
To see the resources of their children seemed an important aspect for all caregivers. The things the children managed to do in the sessions surprised the caregivers. Music therapy sessions seemed to facilitate the caregiver’s ability to wait for initiatives of their children.
The special teachers emphasize the importance of working with the emotional relationship between caregiver and children in terms of accepting the disability:
“I think (musical interaction) is a form of communicating, a form of paying attention to your child. To really try to interact and to accept the situation. There in music, you focus there. I think it facilitates the acceptance.”
My own impression was that the caregivers were in a challenging situation and that positive moments and happiness therefore seemed to be important for their relationship. They emphasized that they felt happy when they saw their children happy. Paula described how happy she felt to see her daughter playing and smiling as they had been through a very challenging period.
Affordances for the children
“She is playing and getting smarter. She is expanding into the world.”
According to the caregiver’s comments in the interviews, all children showed progression through music therapy. Paula explained that Ana did not like loud sounds and could not stand to be in the group with the other children. For Paula, it seemed that through music therapy Ana’s relationship to sounds changed. Sophia stated that Alicia was better in better mood and Clara stated that Júlio showed progress in general.
The most important affordance for the children according to the analysis of the video footage is for them to take part in pleasurable interaction and to experience bonding as this leads to positive experiences and to more activity. Moments that engaged the children and their caregivers caused prolonged interaction. The children seemed to experience their caregivers being responsive to their communicative initiatives.
In contrast to these positive findings, there were also patterns between the children and their caregivers that highlight limitations and the extent to which the children were able to experience this positive progression. One example is the use of sound and instruments to develop an idea of physical space, which links closely to possibilities in social interaction. Carolina made clicking noises with her mouth in order to gather spatial information about the room. Several children enjoyed letting egg shakers fall on different surfaces, while listening carefully. This behavior was not necessarily considered as useful behavior by the caregivers and it was therefore difficult to take into account the children’s initiatives and the caregiver’s needs:
“She sleeps with a shaker in her hand. And sometimes when she doesn’t find an instrument she takes off her shoe, just to find out how it sounds.”
According to the caregivers, their children have a strong relationship to music and sound. The participation in music therapy sessions is therefore potentially empowering, as the children can make use of their own capabilities
Musical interaction as a resource for bonding and interaction in everyday life
“What music means in my house? Everything.”
Paula and Clara emphasize that music plays a very important role in their lives. They describe that they often use music in their children’s different everyday activities. These activities involve waking up, feeding/eating, taking a bath, calming, and sleeping. Both Júlio and Ana have a strong relationship with sounds and music, and their caregivers describe their children’s affinity for music:
“ . . . and now she will try out how her pacifier sounds on the guitar.”
Paula describes that Ana uses music herself to fall asleep, humming until she sleeps. Both caregivers see music as something that will be important for their children throughout their entire lives:
“This pandeiro 9 got even famous at home; so much I talked about it.”
During our sessions, a pandeiro turned out to be Ana’s favorite instrument. She would often play with it in the early intervention section outside of our sessions. For Clara and Júlio, a Norwegian song (Vi er alle sammen elleville) that I translated and introduced to them turned out to be an activity at home and in the bus:
“But then we were on the bus, and I was humming this song we always sing with you. And Júlio calmed down, started to laugh and to move, and we suddenly had a good time.”
In the interview, Clara told me that they sing the song at home regularly. They have found their own way to sing it and use a shorter version.
Discussion
Music-making as a space for development of bonding and interaction
Music therapy in the context of early intervention has been described as space or container for parent–infant bonding (Edwards, 2011; Jonsdottir, 2008). All elements (as for instance joint attention and mutuality) observed in the selected moments are related to positive parenting and “healthy” bonds (e.g. Edwards, 2011). The interaction in the space of music is possible through protomusicality (Malloch, 1999), and therefore, both partners have the similar capacities for participation.
The findings of this study correspond with the literature and indicate that music-making can be considered as a space for social interaction and bonding for children with visual impairments and their caregivers. The findings add to previous literature that musical interaction facilitates elements of early interaction that can be challenging for children with visual impairments and their sighted caregivers. This applies especially to joint attention.
The necessity for attachment in early childhood is well documented in the literature (e.g. Bowlby, 1951). Theorists from biopsychology (Trevarthen, 2001) and critical special education (Feuser, 1989; Jantzen, 1976) point out that early interaction links to the acquisition of culture. For Jantzen (1976), the isolation from processes of acquisition of culture as well as societal heritage is the core element of disability.
“She is expanding into the world,” said Paula about her daughter participating in music therapy. The possibility to experience participation in early childhood links closely to possibilities for participation in later life. Working with caregivers and their children with visual impairment can therefore promote possibilities for participation in music and social interaction.
The affordances of joint music-making
The findings suggest that music-making affords different things for the children and their caregivers. For the caregivers, one important aspect is acknowledging the resources of their children. Both Clara and Paula emphasize that their children understood what they should do. I interpret these statements as meaning that they do not often get this experience outside of musical interaction. This can be interpreted in the context of the challenges linked to the different perception styles of children with visual impairments and their sighted caregivers.
The narratives of the caregivers support the literature that states that caregivers are in a very challenging situation during the first months and years of the child’s life. The participation in music therapy affords the experience of being a “good enough” mother, as Levinge (2011) emphasizes for mothers with maternal depression.
For the children in the project, the most important aspect seems to be the promotion of individual capacities for interaction and bonding or, rather, the experience of being capable to interact and that their caregivers are capable to interact too. Children with visual impairments do not easily get the experience that their actions have an effect in the physical world. Therefore, experiences like Flávia playing guitar with her foot and her mother commenting on her action immediately are very important.
One shared affordance seems to be the experience of happiness and pleasure. I suggest that happiness and joy is an underrepresented focus in early intervention for children with visual impairments and their caregivers. The importance of this affordance is supported by Schore (2010), who outlines how the absence of early interaction and attunement is traumatic for brain development. Another aspect is the absence of vision and the potential vulnerability of children with visual impairments. For Schore (1994), smiles and positive looks stimulate the brain to growth of the “social, emotionally intelligent brain.” The pleasurable arousal that triggers a biochemical response promotes brain growth (Schore, 1994). Schore (1994) describes this as being linked to visual contact when smiling. How does a child with a visual impairment perceive whether the caregiver is smiling? As described above, the quality of Paula’s voice changed when she was smiling, as she suddenly communicated more affection through her voice. In other moments, happiness was expressed through touch and responsiveness).
Other affordances link to everyday life. The caregivers describe that they use music in order to calm their children, to feed them, and to have a good time with them. Music seems to afford different things during the day. Different artifacts, such as instruments, songs, or activities, afford different things depending on the appropriation (DeNora, 2000; Stige, 2002). In the presented findings are two examples. The pandeiro gave Ana a large amount of attention in her family and neighborhood and a song that turned into an activity for Clara and Júlio at home and on the bus. These examples show also that music is not limited to the music therapy room, but links to the everyday life of the participants and in some ways interacts with the context of the participants.
Music-making, social capital, and empowerment
As pointed out above, disability intersects with exclusion, poverty, and limited access to health and education systems. Procter (2011) links musical interaction (musicking) to the generation of social capital. He suggests that music-making affords, if not the generation of social capital, the generation of proto-social capital. I consider this idea as important for two different reasons. On one hand, the generation of proto-social capital links to the idea of repairing communicative musicality. This is important for those, through exclusion and disability, who did not have the chance to develop communicative musicality in early childhood. Music therapists can have an important role in assisting in this process (Procter, 2011). The other aspect links to the cultural aspect and the importance that music has in society. Both Clara and Paula emphasize how important music is to them and in their lives. This points to the possibilities of music therapy as music is linked to culture and social life (Ansdell, 2002; Stige & Aarø, 2012). One important aspect in this project was the focus on use of music that the participants use in everyday life. This highlights the relevance of culture-centered music therapy (Stige, 2002).
Through the project, I became more and more engaged with the caregivers’ life stories as I experienced that their stories closely linked to their relationship to their child. Landsman (2010) emphasizes that motherhood is challenged by the concepts of disability in society. As described earlier, the caregivers participating in the project had many challenges in the first years of the child’s life. For me, one important aspect of music therapy in an early childhood context is therefore empowerment. Music therapeutic work can be empowering in different ways. An approach to music therapy that is based on values as mutuality and equality can reduce professional dominance. This is supported by scholars from the fields of music therapy and special education. For Procter (2002), music therapeutic work is an enabling and empowering process “building on people’s experiences of who they are and what they can do” (p. 96). A resource-oriented approach to music therapy (Rolvsjord, 2010) implies recognition and development of the client’s resources and goals. In the context of special education, Lassen (2008) discusses how principles of empowerment can be used in consultation. Both children and caregivers in the project may be empowered in their relationship and possibilities for participation. However, the work with caregivers and their children ideally would be supplied by working with the community of the family. Possibilities for participation are determined by societal structures (Ruud, 1998; Stige & Aarø, 2012), and the concepts of disability have an impact on the life of families with children with visual impairments. Music therapists need, therefore, to be aware of the structures within which they are practicing and work actively toward more inclusive structures in society.
Implications for practice
This study reveals the need for access to music therapy. Access can, however, be difficult, and it is important to pass music therapeutic knowledge to other people, especially to caregivers and professionals. At the same time, this cannot substitute qualified music therapists in this area, and I consider the training of music therapists in the context of visual impairment as very important. Ideally, family-centered music therapy that takes into account the caregivers’ voices would be implemented in early intervention programs in the community of the families.
Practitioners could use insights from this study to reflect upon and reinforce their use of music in the context of direct work with children with visual impairment and supervision. The practical implications of this project include the promotion of awareness for the conscious use of music and music therapy in early childhood. Music needs to be used with care, as it can also be over-stimulating. As children with visual impairment commonly use their auditory sense for orientation, a permanent musical background disturbs their capacity for orientation.
Implications for research
The findings of this study contribute to the growing interest in empowering research that takes into account the caregivers’ voices. Other studies in this area should observe the longitudinal impact. There is a need for further multi-disciplinary investment in practice and research in the area of children with visual impairment and music therapy. Furthermore, the study revealed the need for providing an audio version of invitation and information letters for non-reading members of society.
Concluding thoughts
What can joint music-making afford children with visual impairment and their sighted caregivers in terms of bonding and social interaction? The data material suggests that music therapy promotes positive bonding patterns and enhances early interaction by providing experiences of togetherness, joint attention, and happiness. “A great moment . . . because of the music,” said Clara. Musical interaction seemed to facilitate elements of early interaction that can be challenging for children with visual impairment and their sighted caregivers. These findings support the notion that music is important in the life of children and their caregivers. Music therapists can have an important role when the natural ability to interact musically may have been challenged. Further research is needed to explore the relationships between music-making, empowerment, and everyday life of families with a child with visual impairment.
Footnotes
Acknowledgements
I would like to thank the children, caregivers, and staff members who took part in this Master’s thesis project as well as the supervisors Dr Simon Gilbertson and Dr Per Frostad for their suggestions and comments.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.