
Abstract
A structured literature review concerning the design of living environments for people with dementia and sight loss was conducted. Following systematic searching, 33 items were included and quality was assessed. Findings are described covering colour and contrast, lighting, fixtures and fittings, entrances and exits, gardens, and outdoors. The discussion highlights the poor quality of evidence, combined nevertheless with useful suggestions for design; the tendency for the literature to be fragmented; and the need for improvements in terms of study focus, study quality, and an emphasis on independence and individual needs. The review was subsequently used to inform the development of design guidelines.
Background and aims
A growing literature focuses on how environmental design can either enhance or inhibit independence for people with impairments. This includes research on design for people with sight loss and design for people with dementia, and design guidance which has been produced for each of these groups.
Advancing age is a well-evidenced risk factor for sight loss as well as for dementia. Dementia can compound and complicate sight loss, as memory and understanding may become impaired. Furthermore, some forms of dementia may entail physical damage which can produce additional sight problems. Despite this, researchers have been slow to consider the impairments together, and the scientific literatures have tended to remain largely separate.
The existing guidance also appears to have some limitations. Reviewing selected design guidance publications for people with sight loss and people with dementia, Goodman and Watson (2010L 1 ) suggest that while there are many similarities, there appear to be some areas of potential conflict: for example, recommendations of curved paths and corridors for people with dementia and straight ones for people with sight loss (p. 4) and recommendations of multiple objects placed around environments for people with dementia to support reminiscence and reduced clutter for people with sight loss (p. 4). Furthermore, they identify that the evidence base for the guidance is not always clear, and they raise reliability issues.
Given the common co-occurrence of dementia and sight loss for older people, the apparent contradictions in the existing guidance, and the questioning of the evidence base, this article reports on a literature review of research on design of living environments for people with dementia and people with sight loss, which aimed to explore the evidence base for design recommendations. The literature review was subsequently used to inform the development of new design guidelines for people with dementia and sight loss (Greasley-Adams, Bowes, Dawson, & McCabe, 2014).
Methods
The structured literature review involved systematic searches conducted in December 2012 of a wide range of databases, complemented by consultation with expert informants who were asked to recommend materials (such as reports) that the searches might not have identified. Table 1S (Supplement) lists the search terms used, Table 2S (Supplement) lists the electronic databases searched, Figure 1S (Supplement) summarises the results of the searches and the process of identifying relevant materials for review, and Table 3S (Supplement) provides the scoring system used as a final filter to select items for full text review. These were systematically evaluated using a pro forma which enabled assessment of the quality of the research reported and assembled key information regarding the subject matter, results, and conclusions of each item. Reviewers identified the research design of the item being reviewed, and then responded to a series of questions relating to that specific research design. Table 4S (Supplement) lists the quality criteria used to assess different types of research. These were drawn from standard protocols widely used in reviewing, including Centre for Research and Development (CRD) Report No. 4 used for randomised controlled trials, Cochrane Effective Practice and Organisation of Care (EPOC) checklists used for controlled before and after studies, and Critical Appraisal Skills Programme (CASP) assessment criteria used for literature reviews and qualitative studies (CASP, n.d.; Cochrane Effective Practice and Organisation of Care (EPOC), 2002; NHS CRD, 2001). In addition, a section for ‘other types of study’ sought information about design and quality of these in a structured manner. Having responded to detailed questions about the design of the study, its conduct, and conclusions, reviewers were asked to rate it as of high, medium, or low quality and to record their reasons for doing so. Table 5S (Supplement) lists all the evaluations and the reviewers’ summary reasoning. Thus, each study was quality assessed according to specific criteria relating to studies using the same approach, and assessments were therefore structured and consistent within study type. A total of 33 items were included in the review. In total, 28 of these were identified by the searches and met the inclusion criteria, that is, they focused on how people engaged with environments, described or reviewed a number of research studies, and related to people with dementia, people with sight loss, and/or people with both. A further five items included were suggested as relevant by the panel of experts.
Following review, a descriptive and qualitative analysis of the findings was conducted. This was guided by design themes which are used to guide the presentation of findings. The themes were identified through consultations with 19 people experiencing dementia and/or sight loss and 10 staff who worked with them: the consultations reviewed initial findings and helped inform the thematic analysis of the findings. A full account of the consultations and the development of the guidelines, which took place throughout the process, will be published elsewhere (please contact authors). A flowchart of the process of the literature review demonstrating where consultation was used is provided in the Supplement (Figure 2S).
Quality and coverage of literature
Table 1 summarises the nature of the literature evaluated in the review and indicates the quality assessments.
Included items and quality assessments.
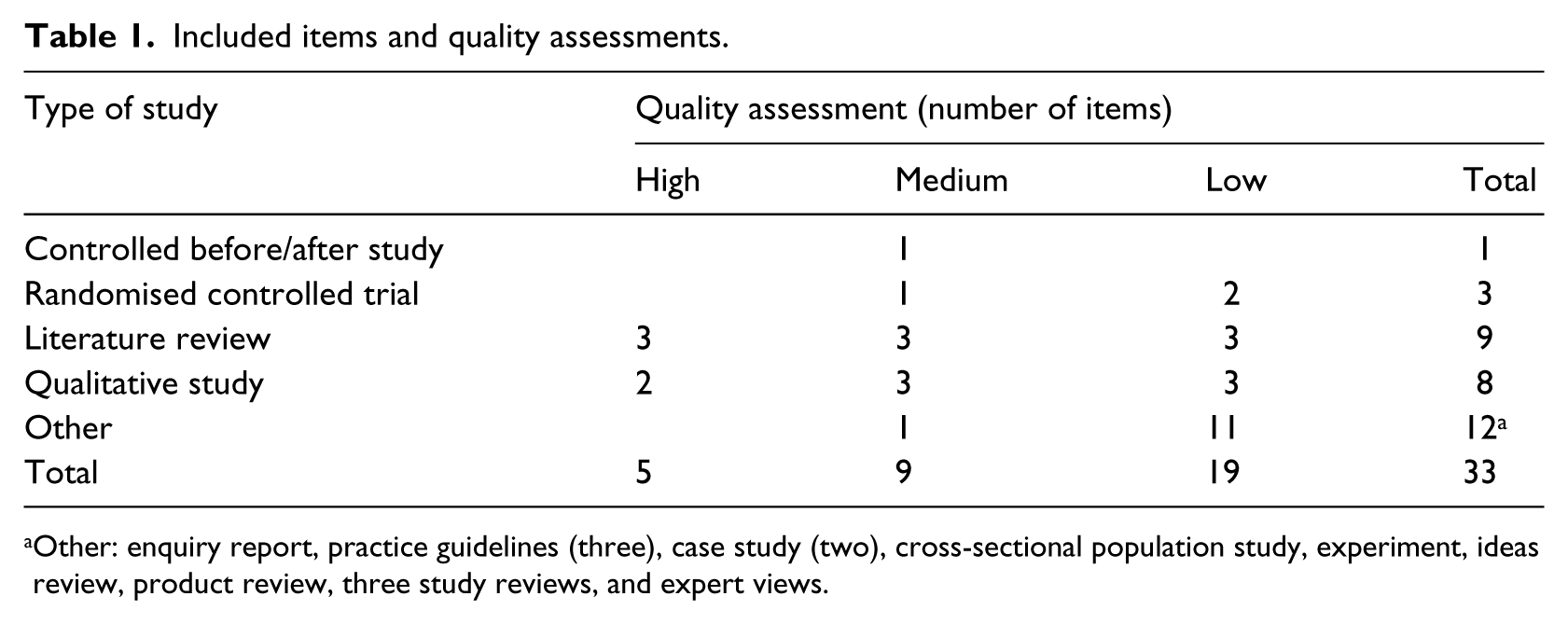
Other: enquiry report, practice guidelines (three), case study (two), cross-sectional population study, experiment, ideas review, product review, three study reviews, and expert views.
Overall, there was little high-quality research, consisting of three literature reviews and two qualitative studies. This means that our discussion can produce only indicative conclusions. Unlike some review procedures, we do not exclude lower quality work: especially in a new field of enquiry, this may provide useful indicative material. This contrasts with, for example, Anttila, Samuelsson, Salminen, and Brandt (2012H), whose review of the evidence base for assistive technology (AT) interventions for people with disabilities only included systematic reviews. We note that the strict inclusion criteria used by Martin, Kelly, Kernohan, McCreight, and Nugent (2008H) produced no relevant studies about smart home technologies, despite initially identifying 2380 citations.
Table 2 indicates the populations covered in the literature. It is notable that the searches identified very little work relating to populations with both dementia and sight loss, supporting the need to focus specifically on this group in future research.
Literature relating to which populations.
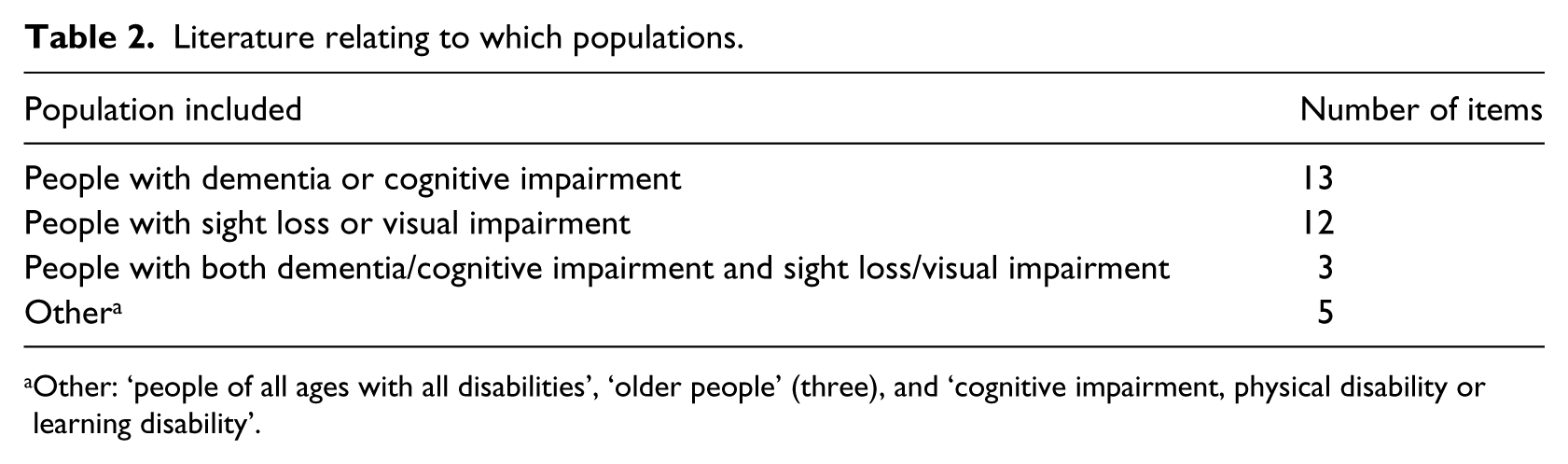
Other: ‘people of all ages with all disabilities’, ‘older people’ (three), and ‘cognitive impairment, physical disability or learning disability’.
Particular types of dementia or sight loss were rarely distinguished, with only two studies identifying type of dementia (both Alzheimer’s disease) and only one specifying a single type of sight loss (age-related macular degeneration) and one identifying a specific group of conditions (retinitis pigmentosa, diabetic retinopathy, and glaucoma).
The large majority of sources focused on private spaces, including general housing stock, care homes, or sheltered/extra care housing. There was a particular emphasis on care homes, with 17 items covering these. Where public buildings were considered, sources tended to cover a wide range, considering in general terms how places that people visited outside their homes could be more accessible by design.
Table 3 lists the wide range of design features considered, and Table 4 lists the design properties.
Design features covered in the literature.
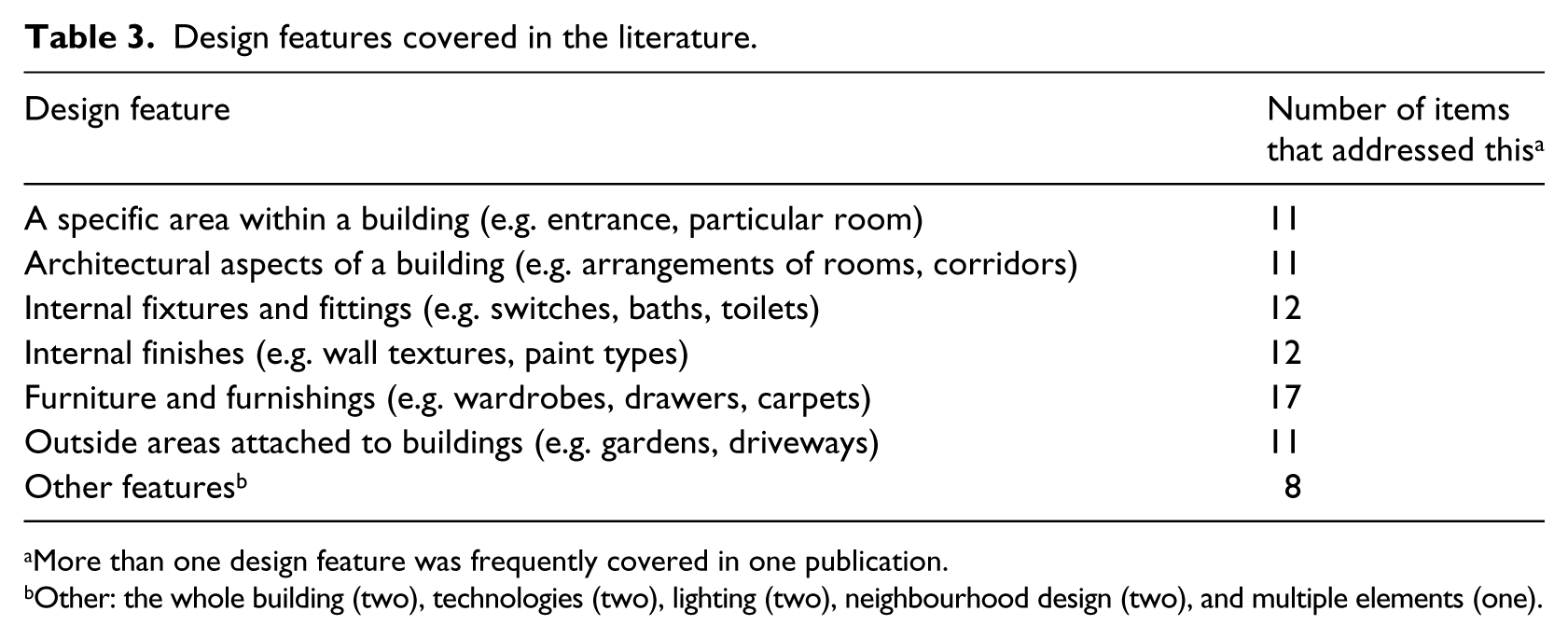
More than one design feature was frequently covered in one publication.
Other: the whole building (two), technologies (two), lighting (two), neighbourhood design (two), and multiple elements (one).
Design properties addressed in the literature.
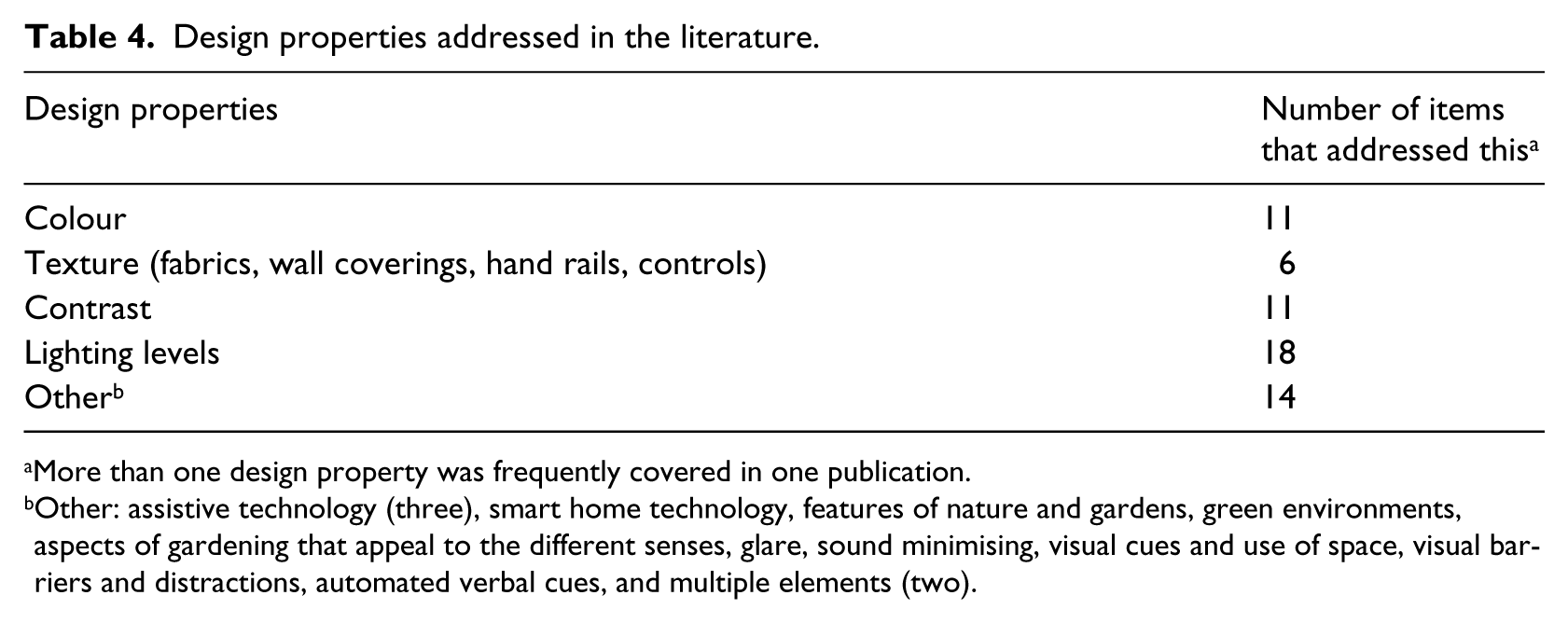
More than one design property was frequently covered in one publication.
Other: assistive technology (three), smart home technology, features of nature and gardens, green environments, aspects of gardening that appeal to the different senses, glare, sound minimising, visual cues and use of space, visual barriers and distractions, automated verbal cues, and multiple elements (two).
Findings of literature review
We summarise the findings of the literature review under the headings that emerged from the thematic analysis of finding.
Colour and contrast
Research relating to colour and contrast was mainly of low quality, but a number of consistent findings and recommendations did emerge. The balance of views suggested that contrast rather than colour per se was of particular significance.
For example, for people with dementia, Goodman and Watson (2010L) suggest using colour to define spaces, such as those for dining, relaxing, or activity areas. Marquardt (2011M) supports this by suggesting that vivid colour coding might help improve functional ability and short term-memory, since people with dementia may have impaired ability to discriminate colour. Kelly, Innes, and Dincarslan (2011M) suggest that the use of colour can aid way-finding and enhance visibility of features. Calkins (2002L) argues that colour should be used to emphasise what is important (e.g. signage, orientation cues, stair edges, and level changes) and de-emphasise that which is not. She suggests using brighter colours and higher contrast with background, adding that varying colour value by at least two levels on a 10-level scale will help people with dementia to distinguish between colours.
Kelly et al. (2011M) suggest that in care homes, strong contrasting colours can help draw attention to areas that will be used by residents. For example, contrasting doors and doorframes might be beneficial, as might toilet seats that contrast with toilets. Other lower quality examples include McNair, Cunningham, Pollock, and McGuire (2010L), who employ the same principle when suggesting that dining rooms in care homes for people with dementia should ‘use white dishes with a contrasting coloured dark rim’. Calkins (2002L) suggests the use of contrasting colours may be helpful in a range of settings, including chair seats; sinks and washstands; for toilets or toilet seats; and for table settings, using pale plates on darker tablecloths. High contrast markers may also help people with dementia identify hazards (Lawrence & Murray, 2009L).
Contrast may also present difficulties. For example, Goodman and Watson (2010L) call attention to the potential for the sudden changes in contrast at floor level to be seen by some as a barrier and potentially to discourage movement. They note that some guidance considers the use of such contrast to deter people from entering certain spaces, arguing that the ethical aspects of such measures require careful attention: they could be seen as a form of restraint.
For people with sight loss, good contrasts are reported to be important (Brunnström, Sörensen, Alsterstad, & Sjöstrand, 2004L) and contrasting colours can aid object recognition (Unwin, Andrews, Andrews, & Hanson, 2009L). For example, pull cords for blinds, and light switches could be high contrast with surroundings (Littlefair, 2009L) and chairs could be contrasted with walls to help people see them (Torrington & Lewis, 2011M). Littlefair (2009L) suggests that light coloured window frames and window walls reduce contrast between the window and its surroundings and might help in reducing glare. However, Cooper (1999M) found that people disagreed that they needed supports using colour and contrast.
Den Brinker et al. (2005M) and Unwin et al. (2009L) suggest that for people with sight loss, contrasting strips placed on the edge of stair-treads can help reduce the risk of falls. Littlefair (2009L) suggests that lighting which creates contrast between tread and risers on stairways and which casts shadows can help to highlight the three-dimensional form of stairs and adds that natural lighting from the side is best for stairways. East or west facing windows at the top and bottom of stairs should be avoided due to increased risk of glare from the rising or setting sun (Goodman, 2008, referred to in Littlefair, 2009L).
For people with both dementia and sight loss, Lawrence and Murray (2009L) recommend using bold colour and contrast to aid vision and independence: for example, they may assist with identifying objects and distinguishing them from their background more easily.
Lighting
Several low- and medium-quality publications refer to the need for adequate lighting levels in home environments for people with dementia (e.g. Calkins, 2002L; Calkins and Brush, 2002L; Kelly et al., 2011M; Marquardt, 2011M; McNair et al., 2010L; Van Hoof, Kort, Van Waarde, & Blom, 2010M). McNair et al. (2010, p. 9L) argue that there is a clear link between appropriate lighting and supporting independence.
The type of light may be important, although evidence in this area is not strong. Natural light is said to have beneficial properties for people with dementia, including improving health and well-being (Bossen, 2010L), lowering incidence of falls and sleep disturbance (McNair et al., 2010L), and assisting with way-finding and thus independence (Marquardt, 2011M). For people with dementia living in care homes, Marquardt (2011M) argues that sensory stimulation through natural light and views to the outside are beneficial, and long internal corridors lacking these will negatively affect vitality.
Several studies find benefits from bright light. Marquardt (2011M) points to studies which have demonstrated that bright artificial lighting and natural light can improve sleep duration, reduce agitation and aggressive behaviour, and assist with way-finding. Lawrence, Murray, Ffytche, and Banerjee’s (2009H) high-quality work which also focuses on care homes suggests that dim lighting is associated with challenging behaviour in people with dementia. Van Hoof et al.’s (2010M) literature review notes that improving lighting is often mentioned as a means to increase safety and poor lighting has been identified as an environmental hazard in the homes of older people. They suggest that good lighting can increase overall quality of life and prevent falls; it might be able to help modify behavioural symptoms and improve cognitive function; it can make hazards more visible; and in dining rooms, it can enable people to eat better.
Lighting recommendations for particular rooms for people with dementia are made. In bathrooms for people with dementia, McNair et al. (2010L) suggest multiple ceiling-mounted lights to ensure no dark corners, task lighting at wash-basins, light-transmitting material for shower cubicles or an appropriate ingress-protected light mounted directly above the cubicle, and a movement detector at the door to turn lights on automatically. However, Van Hoof et al. (2010M) with stronger evidence caution that automatic lights switching on can cause distress to people with dementia.
In kitchens, McNair et al.’s (2010L) specific suggestions include using long light sources (i.e. fluorescent tubes) for general lighting rather than spotlights; low-profile strip lighting under cabinets for task lighting, protected from direct view by pelmets; similar lighting on top of the wall-mounted cupboards to avoid dark areas, protected from direct view by cornices; and providing specific task lighting over the sink. Similarly, Van Hoof et al. (2010M) mention the need for greater task illumination for food preparation.
For people with sight loss, lower quality research such as Littlefair (2009L) reports that natural day lighting is generally more comfortable than electric task lighting. Long (1995L) supports this, reporting that people with sight loss acknowledge the desirability of natural light throughout their homes. The variation in natural daylight can help with sleep and add to interest in the visual environment, and windows can help with way-finding (Littlefair, 2009L).
Poor lighting can compromise home safety for people with sight loss, whereas good lighting can bring benefits beyond simply improved safety. In a randomised controlled trial of a home safety intervention for people with visual impairment, La Grow, Robertson, Campbell, Clarke, and Kerse (2006L) found that nearly 40% (77 of 194) homes visited presented safety hazards related to indoor lighting. Calkins and Brush (2002L) and Kelly et al. (2011M) note that care homes also tend to fall short in these aspects. Brunnström et al. (2004L) found that having good quality lighting in a living room can benefit quality of life and that improving the quality of lighting in bathrooms and kitchens could lead to improvements in activities of daily living (ADLs). This is supported by Van Hoof et al. (2010M), who note that people with visual impairments may have impaired ability to adapt to changing light conditions.
These recommendations differ from other literature relating to lighting for people with sight loss which highlights the preferences of people themselves and their individual requirements. For example, Littlefair (2009L) notes that people with visual impairments may appreciate a degree of variation in light in rooms and will organise tasks according to lighter or darker areas. Similarly, Long (1995L) points out that people with sight loss have unique lighting requirements depending on the type of vision loss, sensitivity to glare, and the task being undertaken. His study emphasises both the need to increase sources of natural and artificial lighting in people’s homes and to be able to control lighting. Increased availability of lighting could include strip lighting under kitchen cabinets, lights within shower areas, well-lit exterior doors and lighted keyholes (see also Unwin et al., 2009L), and sound- or motion-activated external entrance lighting. Increased control could include the use of rheostats on all light switches, adjustable blinds, and tinted large windows/skylights to reduce glare. Long (1995L) and Percival (2007M) both argue that control of lighting is particularly important for people with sight loss – more so than colour and contrast – and is relatively simple to achieve.
Considering kitchens for people with sight loss, Long (1995L) discusses the need for additional lighting including strip lighting under cabinets (a recommendation also supported by Unwin et al., 2009). Brunnström et al. (2004L) found that providing ceiling-mounted fluorescent tube light fittings together with under-cupboard lighting on working surfaces led to significant improvement in ADLs for tasks carried out on the working surface in the kitchen. Littlefair (2009L), however, noted the preference of people with visual impairments for daylight in kitchens, especially for task areas.
For people with both sight loss and dementia, Goodman and Watson (2010L) state that there is a need to maximise natural light, supported by the Homes and Communities Agency (2009L). Edgerton and Ritchie (2010L) suggest that lighting should be at a level that helps to compensate for poor eyesight in people with dementia to aid with way-finding. Goodman and Watson (2010L) also suggest that stark differences in lighting levels, such as areas of excessive light and shadowed areas, should be avoided. They too highlight the need to be able to adapt or adjust the lighting levels to suit individual needs. The need to couple appropriate intensity of light with good contrast conditions and absence of glare has been noted both for those with sight loss (Brunnström et al., 2004L) and for people with dementia (McNair et al., 2010L).
The many recommendations about lighting made in this literature are not wholly consistent, and not generally well evidenced. Nevertheless, it is possible to identify the importance of individual choice and the ability to control one’s environment by, for example, adjusting lighting according to one’s own preferences.
Fixtures and fittings
The literature makes multiple recommendations about fixtures and fittings, often in relation to particular rooms in the house, notably kitchens and bathrooms. Under this heading, there was relatively little literature relating specifically to people with dementia and most of the recommendations relate to people with sight loss. The quality of this literature is not generally high.
In care homes, Calkins and Brush (2002L) discuss the use of soft furnishings such as curtains and acoustic panels to absorb noise which might otherwise distract diners in dining rooms. Edgerton and Richie’s (2010L) brief literature review suggested creating the perception of choice for care home residents with dementia using low-level dividers or partitions to create smaller spaces in larger rooms, research having shown that providing choice could improve quality of life and have a calming influence on residents.
In people’s own homes, Unwin et al. (2009L) present a list of potential modifications which might allow people with dementia to remain there for longer. Many of these relate to fixtures and fittings including grab rails in the bathroom, room-darkening curtains in the bedroom, bannisters on both sides of stairs, and removing rugs without non-skid backing. Kiata et al. (2008L) however find that people do not necessarily want to remove rugs, preferring to protect the carpets underneath.
For people with dementia, fixtures and fittings in bathrooms are encouraged to be visible, using contrast (Kelly et al., 2011M). Unwin et al. (2009L) warn of a potential issue regarding mirrors in bathrooms for people with dementia, who may not recognise their reflections and find this distressing: this presents a contrast with recommendations for people with sight loss (Long, 1995L) to have an accessible mirror available.
Regarding people with sight loss, several points made about fixtures and fittings relate to the provision of hand rails or grab rails (Dahlin-Ivanoff and Sonn, 2004M; La Grow et al., 2006L), the use of rugs and mats (Kiata et al., 2008L; La Grow et al., 2006L), electrical outlet sockets and switches (Long, 1995L), appliance controls generally (Kondo, Mann, Tomita, & Ottenbacher, 1997L; Littlefair, 2009L; Long, 1995L), and kitchen cupboard doors and handles (Long, 1995L). More generally, Lawrence and Murray (2009L) refer to bold colour and contrast in fixtures and fittings as a means of promoting independence through aiding vision.
Goodman and Watson (2010L) suggest that with respect to fixtures and fittings, there may be different requirements for people with dementia and people with sight loss and make several related points. They note first fittings and equipment made or adapted for people with sight loss may need to incorporate less ‘traditional’ and less familiar types of controls (e.g. more tactile controls). Second, the ‘old fashioned’, more familiar, design of fittings, and fixtures often recommended for home environments for people with dementia may promote an ‘institutional’ image that accommodation providers for people with sight loss would be keen to avoid and which might deter interaction/visits from the wider community. Third, fixtures and fittings which assist with reduced functional abilities often experienced by people further into their dementia journey would not be necessary in homes of people with sight loss. Fourth, some items suggested as providing memory stimulants might present hazards to people with sight loss (they use the example of traditional clothes lines with stretchers). Mihailidis and Fernie (2002L) identify that assistive technology that can respond to individual requirements and wishes is increasingly feasible, suggesting increasing potential for flexibility.
Entrances and exits
The literature on entrances and exits relating to people with dementia tends to emphasise control. For example, Edgerton and Richie (2010L) suggest that unobtrusive and disguised exits and safety features can reduce ‘exit attempts’ by people with dementia. Letts et al. (2011H) also comment on how visual barriers are effective in reducing attempts at exiting. To facilitate people using entrances and exits, Kelly et al. (2011M) again suggest that strong contrasting colours, such as between doors and doorframes, can help draw attention to areas that will be used by care home residents.
Control of use of exits, whether deliberate or inadvertent, can have unintended consequences. For example, where difficulties exist in accessing gardens, and where help is required to access such spaces, there will be reduced use of them: Rappe and Topo (2007H) suggest that easy access promotes daily use. Bossen (2010L) notes a number of potential barriers to the use of outdoor spaces by residents of care homes for people with dementia, including heavy or locked doors, entrance or exit designs which fail to facilitate disabled access, lack of cueing features or landmarks, and lack of weather protection. Kwack et al. (2005) mention the roles of raised door sills and poorly located exits to gardens in deterring the use of outdoor spaces.
By contrast, the literature on entrances and exits for people with sight loss emphasises their ability to use these independently. For example, Long (1995L) suggests that larger than normal landings at stairs makes their use easier for people with sight loss; it is desirable for people with sight loss not to have proud door thresholds, as these may be a tripping hazard; pocket or sliding doors and recessed door handles reduce the risk of walking into doors; well-lit exterior doors and lighted keyholes, as well as sound-activated light, can be beneficial to those with sight problems; alarm control panels should have tactile markings and audible confirmation when buttons are pressed; and intercoms should be positioned to allow doors to be entered from anywhere in the property. Unwin et al. (2009L) also suggest that people with sight loss might benefit from bright lights at external doors and lighted keyholes.
Best and Porteous 2 (2012L) assert that there should be straightforward access to buildings and that doorways should be built to wheelchair standards: this perspective emphasises access and independence for all. Goodman and Watson (2010L), similarly, suggest that entrances and exits should be easy to locate and use by all.
Gardens and outdoors
People with dementia living in care homes who use gardens on a regular basis may experience benefits: Bossen’s (2010L) review of literature on nature and nature-based stimuli for people with dementia indicates that among other benefits, there is evidence that more frequent ‘wander garden’ users have fewer falls and their dosage of anti-psychotic medications may reduce.
Recommendations for gardens appropriate for people with dementia suggest they should be designed for accessibility to help people find features and to prevent injury. This might include using easy entrances, incorporating raised flowerbeds or container gardening, or pulleys to raise/lower hanging baskets, and adapting tools to make them easier to use (Kwack et al., 2005L).
Recommendations are given for garden boundaries, generally for safety reasons (Kwack et al., 2008L; Rappe and Topo, 2007H; Unwin et al., 2009L). For further safety within the garden, Kwack et al. (2005L) suggest that contrasting colours to highlight features and hazards can help people with dementia and may reduce falls, hence preventing injury; Unwin et al. (2009L) recommend the removal of all poisonous plants.
To make the garden more pleasurable, Kwack et al. (2005L) recommend that attention is given to the colours, scents, and textures of plants to ensure olfactory, auditory, and tactile stimulation. They suggest that plants should be selected with reference to the experiences, memories, and preferences of residents. They recommend looped paths for people with dementia, to help guide their movement round a garden; however, Marquardt (2011M) suggests that continuous paths may interfere with way-finding.
External steps or stairs, often located in or leading to gardens and outdoor areas, were identified as one of a range of potential hazards as part of a home safety programme intervention trialled by La Grow et al. (2006L). Steps, stairs, and kerbs were most commonly highlighted, accounting for 30% of all hazard-related falls. A home safety programme addressing these issues was able to reduce falls.
Mitchell and Burton (2010M) argue that if local neighbourhoods are not dementia-friendly by design, people with dementia are likely to become increasingly isolated in their homes. Their work defines dementia-friendly neighbourhoods as welcoming, safe, easy, and enjoyable for people with dementia and others to access, visit, use, and find their way around. They identify six design principles: familiarity, legibility, distinctiveness, accessibility, comfort, and safety and provide detailed recommendations as to how these could be achieved.
Considering people with sight loss and dementia, Goodman and Watson (2010L) observe that there may be differences in preferences for people with dementia and people with sight loss with respect to path layout, whereby straight paths with right angle turns where necessary are easier for people with sight loss than the looped paths recommended by some authors (e.g. Kwack et al., 2005L).
Discussion and conclusion
The literature considers a wide range of design issues, with an emphasis on making recommendations either for people with dementia or for people with sight loss. While the quality of research is not high, some relatively consistent recommendations can be identified as we have noted. Our subsequent work with service providers and service users in developing our guidelines (Greasley-Adams et al., 2014) suggested that many of them made sense in the context of their experiences. However, it remains the case that the evidence base needs further research to build it more securely, as much of the literature is not research based, or has an unclear evidence base. There are widespread calls for further research, especially in terms of improved research design and scale of studies. Currently, research is often fragmented, focusing on small issues out of context and on single conditions, rather than on the whole person who is likely to experience several conditions, including dementia and sight loss. It is notable that we did not identify studies which had explicitly used research designs guided by the Medical Research Council (MRC) framework for evaluating complex interventions (Craig et al., 2008), recent developments in process evaluation (Moore et al., 2015), or by innovative evaluation designs and approaches such as realistic evaluation (Pawson and Tilley, 1997). Given that design issues are complex and do involve the whole person, exploring the use of such approaches appears merited.
There are some interesting contrasts in the literature relating to people with dementia and that relating to people with sight loss. For people with dementia, there is an emphasis on care settings, especially care homes. There are also a number of areas in which a key concern is control, such as the work on entrances and exits, and on altering behaviour, such as the recommendations about lighting to change people’s sleep patterns, or activities to improve well-being, such as the use of gardens. We would not suggest that the emphasis on control and behaviour change is necessarily detrimental, but would urge careful consideration of the ethical aspects of the recommendations (cf. Zwijsen, Niemeijer, & Hertogh, 2011M).
By contrast, the research relating to people with sight loss is focused on supporting independence and enabling people to do things for themselves: this is the ‘default’ for this research. We are aware that many of the design recommendations for people with dementia are derived from those for people with sight loss, and that many of them do indeed support independence (such as ease of eating at a table or using a bathroom). A consistent ‘default’ focus on independence for people with dementia would be welcome.
One stimulus for this research, including this literature review, was the existence of apparent contradictions between design guidelines for people with dementia and those for people with sight loss: examples included, as we noted, debates about curved or straight paths and about reducing clutter or introducing reminiscence objects. If a genuinely person-centred perspective is adopted by service providers, whereby the needs of the individual are prioritised, there is a sense in which these are not contradictions, but simply alerts to a service provider to consider what is appropriate for particular individuals. Thus, a core topic for future research must concern how to deliver person-centred design which has a clear evidence base.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the research from the Thomas Pocklington Trust.