
Abstract
The aim of this study was to examine the gender differences in postural balance, physical activity (PA), and body mass index (BMI) and body composition in visually impaired (VI) athletes. A total of 66 athletes took part in this study. After anthropometric measurements, the PA level was assessed by the International Physical Activity Questionnaire-Short Form. The modified Clinical Test of Sensory Integration and Balance tool was used to assess postural balance in four standing conditions: (1) eyes-open on a firm surface, (2) eyes-closed on a firm surface, (3) eyes-open on a compliant surface, and (4) eyes closed on a compliant surface. Findings revealed gender differences in anthropometric measurements (p < .05). No statistically significant differences were found in fat mass and fat free mass between sighted male and VI male athletes and between sighted female and VI female athletes (p > .05). Weekly, high and moderate PA levels as well as walking were found to be different across the four groups (p < .05). Assessment of postural balance in four standing conditions revealed no gender differences in sighted athletes (p > .05). Postural balance scores in conditions 1 and 3 showed significant gender differences (p < .05), whereas conditions 2 and 4 showed no gender differences in athletes with VI (p > .05). Gender-matched differences were also apparent in conditions 1 and 3, revealing that VI male and female athletes scored worse in these conditions than their sighted male and female counterparts (p < .05). There is a delay in balance parameter in VI athletes even if their fitness levels are similar with their sighted counterparts. The present findings could also be useful for gender-specific training session preparations in VI sports.
Introduction
Humans predominantly use visual sensory systems to interact with the environment, and it plays many roles during locomotion and provides information for upright stability. Eighty percent of sensory perception is gathered by the visual system; movements are dominantly controlled by the eyes; henceforth, it is not only responsible for cognition of objects, but it is also used to give information to the brain about position of the body (Friedrich et al., 2008). Vision is a multifaceted sensory function that requires the hierarchical interaction of receptors, transmission, and processing structures to transform captured visual information into meaningful senses (Martin et al., 2016). However, damage to photoreceptors, optic nerves and optic radiations, and visual cortex of the eye results in some degree of vision loss or blindness. The leading causes are genetic factors, situations during prenatal and postnatal periods, illnesses, and traumatic injury. Global estimation of the prevalence of visual impairment (VI) and blindness is 2.2 billion, and it is reported that growth and ageing will increase the risk that more people acquire VI (Bourne et al., 2017). Vision is significant in terms of motor learning and development and unfortunately vision loss disturbs these skills, as well as static and dynamic activities (Hallemans et al., 2010). Individuals with VI interact with their environment through clues gathered by vestibular and proprioceptive systems, but ageing is a major problem which disturbs balance parameter and as a result, falls increases, independent living decreases, and movement skills are restricted among this population (Chen et al., 2012b; Enkelaar et al., 2019; Ray et al., 2008). In addition, it can negatively affect bipedal upright stability during quiet standing and locomotion and gait cycle modulation, navigation, and obstacle avoidance (Logan et al., 2010). The aim of the postural control is to support balance orientation and stability and it requires the harmonious interaction of three sensory systems, somatosensory, vestibular, and visual, for a good maintenance of the balance (Ivanenko & Gurfinkel, 2018; Parreira et al., 2017), and unfortunately, the absence of visual sensory system disturbs the postural control. Therefore, individuals with VI rely on vestibular and somatosensory systems to maintain postural stability (Melzer et al., 2011; Ray et al., 2008). Especially, they highly dependent on somatic sensations during activity of daily living such as walking with a cane, the discrimination of objects by touch, or reading Braille (Parreira et al., 2017).
Physical activity (PA) levels of individuals with VI are lower and their body mass index (BMI) is higher compared to their peers without disabilities (Furtado et al., 2015; Haegele et al., 2019a, 2019b, 2020; Haegele & Zhu, 2019; Kirk et al., 2020). In addition, PA levels differ between males and females with VI (Augestad & Jiang, 2015; Holbrook et al., 2009). In detail, studies found that males with VI accumulated more moderate and moderate-to-vigorous PA than females with VI (Starkoff et al., 2017; Wrzesinska et al., 2018). Another study reported that males with VI had higher passing rates in cardiorespiratory capacity test than females with VI (Furtado et al., 2016). Low levels of PA in VI population may lead to delay in motor development, balance impairments, and problems related to gait. Besides, significant BMI and balance correlation was reported (Greve et al., 2007). In other words, high BMI demands more displacements to maintain balance. Static and dynamic balance ability of individuals with VI are lower compared to peers without VI, and they also differ among individuals with various VI levels (Chen et al., 2012a; Giagazoglou et al., 2009; Müürsepp et al., 2018; Parreira et al., 2017). On the contrary, literature is scarce related to gender comparison in postural balance in individuals with VI. When compared with sighted controls, blind athletes’ dynamic postural stability scores were worse (E. Aydog et al., 2006). Nevertheless, studies carried out with non-VI population showed that gender affect was low for postural balance (Anderson et al., 2019; Sabin et al., 2010), whereas some studies found that women were better than men in dynamic postural control (Andreeva et al., 2020; Gribble et al., 2009; Whyte et al., 2015). As there are neuromuscular and biomechanical differences between gender during functional tasks (Gribble et al., 2009), it is not known whether there are gender similarities or differences during postural balance control in athletes with VI. In goalball, defensive balance, throw reading, and blocking are considered three defensive principles, whereas ball control, attack preparation, and throwing are considered three offensive principles (Morato et al., 2017). Gender might be an important aspect in development of each offensive and defensive principles. Therefore, investigating gender differences in postural balance might be relatively important in terms of developing gender-specific training skills in goalball.
It is reported that VI reduces quality of life (Jones et al., 2019; Siira et al., 2019), whereas PA participation promotes quality of life (Esatbeyoglu & Kin İsler, 2018; Gill et al., 2013) and provides health-related benefits for individuals with VI (Furtado et al., 2016; Giese et al., 2017). It can be suggested that PA manages body composition, promotes postural balance ability, and reduces BMI in individuals with VI. Therefore, it is significant to increase the quality of life and independent living of individuals with VI through tailored rehabilitation programmes. Moreover, taking the gender-specific properties, neuromuscular and biomechanical, into consideration in athletes with VI during training sessions may help to reduce the risk of sport injuries, assess the physical conditions properly, and enhance the athletic performance. To our knowledge, no study investigated the gender differences in PA levels, body composition, BMI, and postural balance ability in VI athletes and compared them with sighted athletes. We hypothesized that there would be gender differences among these parameters in VI athletes. The aim of this study, then, was to examine the gender differences in postural balance, PA level, BMI, and body composition in athletes with VI and compare them with athletes without VI.
Method
Participants
Sixty-six athletes aged ⩾18 years old, healthy, free of injury, and chronic illnesses participated in this study voluntarily. VI athletes were national and international goalball players (14 females and 7 males) and B1 football players (12 males). Sighted athletes were regional and national athletes (15 females and 18 males) practicing football, handball, volleyball, and basketball. Causes of vision impairments of athletes with VI included congenital (14), glaucoma (5), retinis pigmentosa (4), fever (3), trauma (2), retinis detachment (1), amblyopia (1), cataract (19), optic atrophy (1), and doctor fault (1). The International Blind Sports Association (IBSA) sport classes (International Blind Sports Federation, 2018) were adopted for athletes with a VI (21 = B1: Athletes in sport class B1 had blindness presenting visual acuity in the better eye >3/60, 8 = B2: Athletes in sport class B2 had severe VI presenting visual acuity in the better eye <6/18 but 3/60 or better, and 4 = B3: Athletes in sport class B3 had mild and moderate VI presenting visual acuity in the better eye <6/12 but 6/18 or better; Bourne et al., 2017). All the athletes with VI were active as defined by being independent and proficient in their ability to move within their environment. Consent forms were read twice and immediately signed by the athletes. Ethical approval was obtained by the Non-Interventional Clinical Research Ethics Board (Decision no: 2019/08-35) and current study was conducted in accordance with the 2013 Helsinki Declaration.
Data collection procedures, instruments, and measures
Data collection was done in the afternoon between 3 p.m. and 6 p.m. Before the study, all the athletes were familiarized with the tests. Procedures for athletes with VI were done with sound and tactile stimuli. In particular, athletes with VI touched and felt the body composition analyser and wall-mounted stadiometer prior to measurements. After the measurements, questionnaire for PA level determination was read twice and explained elaborately to them, and then it was filled. Finally, they touched and moved their hands around the balance platform and foam pad (dimensions: 53.98 cm width × 48.26 length × 6.50 cm height) before postural balance evaluation commenced. This tactile sensing procedure was carried out to make sure that they were familiar with the balance equipment and felt safe while stepping on and maintaining balance in a quiet standing position. In addition, ‘3-2-1 go!’ count-down prior to each balance trial was verbally executed by the researcher as well as audible rest duration sound at intervals were present for athletes with VI. These auditive references enabled them to be aware of when to start and rest properly before and after each trial.
Athletes visited the laboratory at least ±2 hr post-prandial. They were instructed to report to each test session in well-hydrated state, not to exercise the day before the test trials and to abstain from the caffeine intake for 3 hr prior to each test (Glaister et al., 2015, 2019; Greer et al., 1998; Grgic, 2018). Muscle fatigue and vigorous PA may affect balance control; therefore, balance test did not take place after training and athletes who were engaged in vigorous PA excluded from the study (Barbieri et al., 2013). After anthropometric and body composition measurements, PA levels of athletes were determined followed by postural balance assessment.
Anthropometric variables and body composition procedures, instruments, and measures
Weight was measured in light indoor clothing to the nearest 0.1 kg using a digital scale (Tanita TBF401A, Tanita Corporation, Tokyo, Japan). Height was measured by a wall-mounted stadiometer with an accuracy of ±0.1 cm (Holtain, England). Measurements of body composition components (fat%, fat mass [kg], fat free mass [kg], body mass [kg]) were performed with a foot-to-foot bioelectrical impedance analysis (BIA) to the nearest 0.1 kg using a digital scale (Tanita TBF401A, Tanita Corporation, Tokyo, Japan).
PA levels
Self-reported PA levels of participants were evaluated through the short form of the International Physical Activity Questionnaire (IPAQ-S) (da Silva et al., 2018; Demirturk & Kaya, 2015; Haegele et al., 2017; Saglam et al., 2010; Starkoff et al., 2017) and PA scoring was performed as described elsewhere (Craig et al., 2003).
Postural balance evaluation
Athletes balance and sensory integration scores were measured by the Biodex-BioSwayTM device (Biodex Medical Systems, Shirley, NY) (E. Aydog et al., 2006; S. T. Aydog et al., 2004; Palm et al., 2009). The modified Clinical Test for Sensory Interaction and Balance (m-CTSIB) is an accepted test protocol to assess how well a person can integrate various senses (somatosensory, visual, and vestibular) with respect to balance and compensate when one or more of those senses are compromised on a static surface. The m-CTSIB consists of four different testing conditions: eyes open-firm surface (EO-FIS), eyes closed-firm surface (EC-FIS), eyes open-foam surface (EO-FOS), and eyes closed-foam surface (EC-FOS). The device tracks the subjects’ sway angle and direction from centre. This measure is called the Stability Index (SI). It is the average position from centre and we used SI and composite (avg.) sway for statistical analysis (Boulgarides et al., 2003). Athletes were tested bare foot for four conditions and they were assessed for 30 s. One familiarization trial was completed prior to the four conditions.
Statistical analysis
Data are presented as means and standard deviations (SD) with confidence intervals (CIs %). Normal distribution was checked with Shapiro–Wilk test and variables included in the study revealed a normal distribution. Differences between genders within the same groups for sport experience, training duration, age, and height and body weight were determined using the Student’s unpaired t-tests. The magnitude of the difference of sport experience, training duration, age, and height and body weight was calculated by determining the Cohen’s d effect size (ES) which represents the mean difference over the standard deviation of the difference. The difference was considered trivial effect when d was <0.2, small effect when d was 0.2 to <0.5, medium effect when d was 0.5 to <0.8, and large effect when d was ⩾0.8 (Cohen, 2013). To examine the gender (female athletes without VI = Group 1; male athletes without VI = Group 2; VI female athletes = Group 3; and VI male athletes = Group 4) effect on postural balance, BMI, body composition, and PAL, a one-way analysis of variance (ANOVA) was performed. If overall statistical difference was observed for the dependent variable (p < .05), the Bonferroni post hoc test was used to identify the location of pairwise differences. Differences between groups were considered significant at p < .05. SPSS statistical software version 22.0 (Chicago, IL) was used to perform the analyses.
Results
Sport experience, training frequency, and physical characteristics of athletes are presented in Table 1. Findings showed that female athletes with and without VI were shorter and lighter than male athletes with and without VI, t(30) = −7.474, ES = 2.546; t(31) = −4.706, ES = 1.718; t(30) = −5.767, ES = 2.04; t(31) = −4.122, ES = 1.441; p = .00, respectively. In addition, female athletes with VI were found to be younger than male athletes with VI, t(30) = −6.222, ES = 2.218; p = .00, whereas age for athletes without VI did not differ between genders, t(31) = −1.397, ES = 0.046; p = .17, and sport experience, weekly and daily training durations did not differ across the four groups (p > .05), although medium effect for sport experience, weekly training duration, and small effect for daily training duration in athletes with VI was observed (ES = 0.565, ES = 0.577, and ES = 0.294, respectively). The effect was trivial for sport experience and daily training duration, whereas the effect was small for weekly training duration in athletes without VI (ES = 0.068, ES = 0.122, and ES = 0.321, respectively).
Sport experience, training frequency, and physical characteristics of athletes (M ± SD with 95% CI).
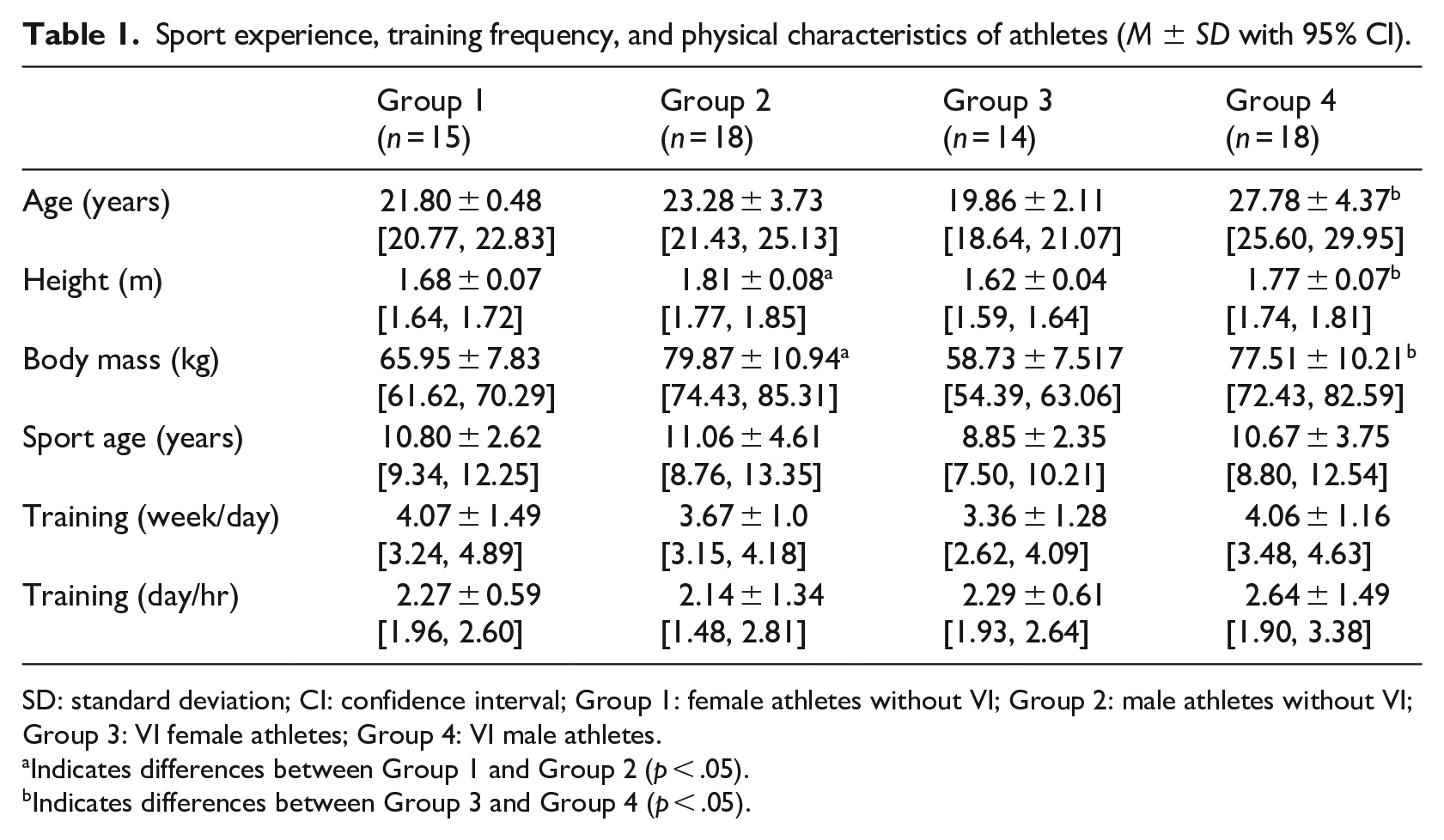
SD: standard deviation; CI: confidence interval; Group 1: female athletes without VI; Group 2: male athletes without VI; Group 3: VI female athletes; Group 4: VI male athletes.
Indicates differences between Group 1 and Group 2 (p < .05).
Indicates differences between Group 3 and Group 4 (p < .05).
Table 2 shows that the main effect was significant in BMI, F (3, 61) = 3.47, p = .02, fat%, F (3, 61) = 40.56, p = .00, fat mass, F (3, 61) = 12.84, p = .00, and fat free mass, F (3, 61) = 46.17, p = .00. The difference was significant only between female and male VI athletes in BMI stating that male VI athletes had higher BMIs than female VI athletes (p = .04). When VI was taken into consideration, no significant difference was observed between female athletes with and without VI and between male athletes with and without VI (p = 1.00). Fat% results revealed gender differences that female athletes without VI and with VI had higher percentage of body fat than male athletes with and without VI (p = .00). Within group comparison between male athletes with versus without VI and female athletes without VI versus VI female athletes showed no significant differences in fat% (p = 1.00). Gender interaction was found in fat mass and female athletes without VI and with VI had higher fat mass than male athletes with and without VI (p = .00). Fat mass and fat free mass between male athletes with versus without VI and female athletes without VI versus VI female athletes were similar (p = 1.00). On the contrary, there was a gender interaction on fat free mass, indicating that male athletes with and without VI had higher fat free mass than female athletes with and without VI (p = .00).
Gender comparisons for body composition, BMI, postural balance, and physical activity level.
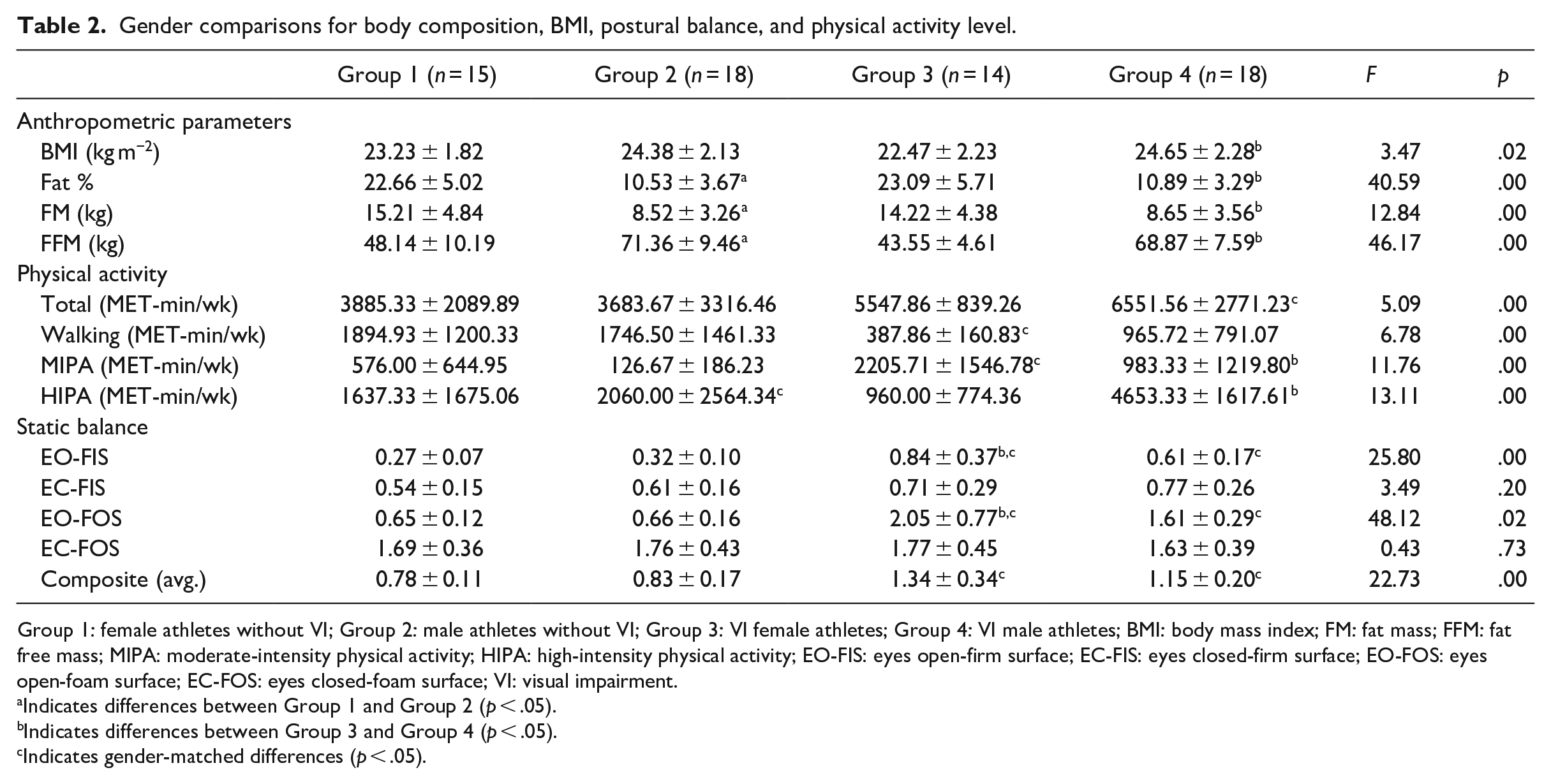
Group 1: female athletes without VI; Group 2: male athletes without VI; Group 3: VI female athletes; Group 4: VI male athletes; BMI: body mass index; FM: fat mass; FFM: fat free mass; MIPA: moderate-intensity physical activity; HIPA: high-intensity physical activity; EO-FIS: eyes open-firm surface; EC-FIS: eyes closed-firm surface; EO-FOS: eyes open-foam surface; EC-FOS: eyes closed-foam surface; VI: visual impairment.
Indicates differences between Group 1 and Group 2 (p < .05).
Indicates differences between Group 3 and Group 4 (p < .05).
Indicates gender-matched differences (p < .05).
PA levels of athletes differed significantly for all parameters. Weekly, F (3, 61) = 5.09, p = .00, high, F (3, 61) = 13.11, p = .00, and moderate, F (3, 61) = 11.76, p = .02, PA levels as well as walking, F (3, 61) = 6.78, p = .02, were found to be different across the groups. In detail, VI male athletes spent more time in total PA compared to male athletes without VI (p = .01). On the contrary, significant difference was not observed between VI male and female athletes (p = 1.00). In addition, there were no significant differences in total PA between male and female athletes without VI (p = 1.00). Total PA levels were not different between female athletes with and without VI (p = .49). Female athletes without VI spent more time on walking than VI female athletes (p = .00). Conversely, time spent on walking was not different between VI athletes (p = .77) and between sighted group (p = 1.00). Likewise result was found that time spent on walking in male athletes with VI was not significantly different from male athletes without VI (p = .18). Moderate PA levels of female athletes with VI were higher than female athletes without VI and male athletes with VI (p = .00). On the contrary, moderate PA levels of female athletes without VI did not differ from male athletes without VI (p = 1.00). Likewise, time spent on moderate levels of PA of VI male athletes were not statistically different from male athletes without VI (p = .08). When high-intensity PA levels of athletes were compared, VI male athletes had higher levels than male athletes without VI and female athletes with VI (p = .00). Female athletes with VI showed similar results and no significant difference was found when compared with female athletes without VI (p = 1.00). In addition, the difference between male and female athletes without VI was not significant for high-intensity PA parameter (p = 1.00).
Eyes open-firm surface, F (3, 61) = 25.80, p = .00, eyes open-foam surface, F (3, 61) = 48.12, p = .02, and composite, F (3, 61) = 22.73, p = .00, postural balance scores revealed significant differences whereas eyes closed-firm surface, F (3, 61) = 3.49, p = .20, and eyes closed-foam surface, F (3, 61) = 0.43, p = .73, showed no difference in athletes. VI female athletes scored worse on firm surface eyes open condition than VI male athletes and sighted female controls (p = .00 and p = .01). Eyes open-firm surface scores of VI male athletes were worse than sighted male controls (p = .00), whereas the difference between sighted athletes was not significant (p = 1.00). There were no significant differences between female athletes with and without VI (p = .27) and male athletes with and without VI (p = .20) in eyes closed-firm surface condition. Similar trends were observed and no statistically significant differences were found in sighted and VI group in eyes closed-firm surface condition (p = 1.00). In addition, Eyes open on unstable surface score was worse in VI female athletes than female athletes without VI and male athletes with VI (p = .00 and p = .02). VI male athletes scored worse than their sighted male controls in eyes open-foam surface (p = .00) and no significant difference was observed between male and female athletes without VI for this condition (p = 1.00). Eyes closed-foam surface results revealed no significant differences among four groups (p = 1.00). Average scores for m-CTSIB showed no significant difference in sighted group (p = 1.00) and in VI group (p = .12). On the contrary, findings revealed that male and female athletes without VI had better average m-CTSIB score than VI male and female athletes, respectively (p = .00).
Discussion
This study was undertaken to investigate the gender differences in postural balance, PA level, BMI, and body composition in athletes with VI and to compare them with gender-matched controls without VI.
Normal and healthy BMI range is 18.5–24.9 kg m−2 (Starkoff et al., 2017), and healthy BMI range is a main indicator of body composition (Holbrook et al., 2009). Being underweight (<18.5 kg m−2), overweight (25.0–29.9 kg m−2), or obese (⩾30 kg m−2) during youth is associated with adhere health conditions throughout the life span (Collaboration, 2017). Past research demonstrated that young and middle-aged men and women with VI were overweight and obese (29.5 ± 5.7 kg m−2 and 30.5 ± 5.8 kg m−2, respectively) (Holbrook et al., 2009). Furthermore, men and women with VI were also found to be overweight with BMIs ranging from 28 ± 5.4 and 28.1 ± 8.1 kg m−2, respectively (Starkoff et al., 2017). On the contrary, data from our study showed that female athletes and male athletes with VI were in healthy BMI range (24.65 ± 2.28 and 22.47 ± 2.23 kg m−2, respectively). In addition, we did not find any difference in this parameter between VI athletes and their sighted counterparts. Therefore, it can be said that being physically active may help to be in a healthy BMI range and having a VI would not be a barrier. Our data also confirmed our hypothesis and revealed gender differences in VI athletes stating that male VI athletes had higher BMIs than female VI athletes. In addition, body composition components showed that mean fat % and fat masses of male athletes with and without VI were lower and fat free masses were higher compared to female athletes with and without VI whereas within gender-matched comparisons showed no differences. These results are consistent with literature confirming gender differences in body composition that women with VI had higher fat percentages (%37) than men with VI (%26) (Holbrook et al., 2009). It was reported that sedentary individuals with VI had higher body mass, BMI, and body composition and their physical fitness levels were worse than male and female goalball players (Colak et al., 2004; Karakaya et al., 2009). Performance wise, fat free mass and fat% showed strong indicators for performance-related physical fitness parameters such as vertical jump and aerobic capacity in male and female goalball players and 7 months training significantly decreased fat mass and increased fat free mass in tandem cyclists with VI (Goulart-Siqueira et al., 2019; Malwina et al., 2015). Another study demonstrated that 16 weeks of training was enough to significantly improve aerobic and anaerobic parameters in six B1 football players (De Campos et al., 2013). Overall, it can be suggested that keeping body composition in healthy range is possible with PA participation as it promotes health and performance-related physical fitness parameters not only for general population but also for VI population.
Previous studies conducted with youth and adults with VI reported low levels of PA in comparison with peers without VI (Marmeleira et al., 2014; Sadowska & Krzepota, 2015). Conversely, in this study, VI male athletes spent more time in PA compared to male athletes without VI. It is important to note that PA participation behaviour differs by gender in non-VI population and males accumulate more time in PA than females (Ding et al., 2016; Kin-Isler et al., 2009). Likewise, male VI student reported greater total PA than female VI students (Aslan et al., 2012; Demirturk & Kaya, 2015; Wrzesinska et al., 2018). Our findings are not congruent with these studies that total PA levels did not significantly differ between male and female athletes with VI as well as between female athletes with and without VI. Since the current study participants are non-sedentary population and VI participants are national and international athletes, it is logical to expect them to be physically active. We found that female athletes without VI spent more time on walking than VI female athletes. It must be mentioned that data collection of VI female athletes was done during their national training camp where they were familiar with and all the facilities were in close proximate. What is more, the IPAQ-S is a self-reported PA questionnaire based on last 7 days recall. Therefore, one possible explanation could account for not to be obliged to walk long distances. Conversely, time spent on walking was not different between female and male athletes with VI. Likewise result was found that time spent on walking in male athletes with VI was not significantly different from male athletes without VI. It is worth to mention that walking is considered as one of the most achievable and convenient forms of PA (Starkoff et al., 2017) and having VI did not limit the amount of time spent in walking in the present study participants. In this study, moderate PA levels of female athletes with VI were higher than female athletes without VI and male athletes with VI. Times spent on moderate levels of PA in VI male athletes were not statistically different from male athletes without VI. Conversely, PA behaviours differed in adults with VI showing that males with VI spent more moderate PA compared to their female counterparts (Starkoff et al., 2017). When high-intensity PA levels of athletes were compared, VI male athletes had higher levels than male athletes without VI and female athletes with VI. This is parallel with the literature that males with VI spent more moderate to vigorous PA compared to females with VI (Starkoff et al., 2017). Female athletes with and without VI have similar high-intensity PA levels. This finding is significant because it is reported in the literature that youth with VI took part fewer days of moderate-to-vigorous PA per week than those without impairments (Haegele et al., 2019a). Various aspects of physical fitness parameters and PA levels of individuals with VI are well documented in the literature (Augestad & Jiang, 2015; E. Aydog et al., 2006; da Silva et al., 2018; Haegele et al., 2019a, 2019b; Marmeleira et al., 2014). Compared to their sighted peers, children with VI were found to be less active, have poorer physical fitness, and have higher prevalence of obesity and overweight (Augestad & Jiang, 2015). In addition, adults who have a vision loss found to be less active compared to general population (Marmeleira et al., 2014). Another study conducted with goalball players indicated that physical fitness levels of goalball players were better than their sedentary peers with VI (Karakaya et al., 2009). Low level of PA is a serious health issue in individuals with VI (Barbosa Porcellis da Silva et al., 2018). In brief, we can conclude that there is a trend of high PA participation in female and male athletes with VI and having a VI is not a restriction to be physically active in the current study participants.
Quality of posture and balance depends on the efficiency of receptors, good work of central nervous system integrating and coordinating the postural system, and effective musculoskeletal system (Bibrowicz et al., 2019). Visual information is important for motor activities and when it is restricted, it causes instability and disturbs the balance ability. In line with latter comment, sighted controls in the current study scored better on stable and unstable surfaces eyes-open conditions and their average m-CTSIB scores were superior than male and female athletes with VI. These findings are consistent with the literature that postural control characteristics in eyes-open condition of static and dynamic tests in children with VI were worse compared to sighted children (Müürsepp et al., 2018). It has also been found that limited vision has a negative impact on overall postural stability and VI individuals rely on greater use of hip strategy to maintain postural stability (Ray et al., 2008). Unfortunately, increase in the risk of falls (Pan et al., 2015) may be due to utilizing greater hip strategy in individuals with VI (Ray et al., 2008). In addition, it has also been shown that vision level affects the postural control and balance ability (Rutkowska et al., 2015). Sighted and low vision elderly achieved smaller average body sway angles during forward and backward platform translations compared to blind elderly (Chen et al., 2012a). Present study results showed that when visual input eliminated for sighted group, their postural balance responses on stable and unstable surfaces were not different than male and female athletes with VI. Studies also confirmed these findings and regardless of age, youth, and elderly without VI scored similar with their VI counterparts in eyes-closed conditions (Müürsepp et al., 2018; Ray et al., 2008). The automatic response depends on the prior experience of the individual and the task being performed (Enoka, 2015). VI athletes in this study rely on different combination of feedback from somatosensory and vestibular sensors in their day-to-day activities and sporting environment. Thus, athletes without VI are not accustomed to changing needs of the quick environmental responses due to their existing visual inputs. Likewise, the influence of vestibular and visual information is greater when standing on moving or unstable surfaces, whereas somatosensory feedback is more critical when standing on a firm, stable surface (Enoka, 2015). The nature and environment of the movements involved in the practice of different sports influence postural adaptation (Paillard, 2014). VI athletes in this study practice goalball and B1 football that require wearing eye-masks during the game. Considering the nature of both sport disciplines, we can presume that VI athletes already developed sport-specific balance adaptations (Hrysomallis, 2011; Zemkova, 2014). These adaptations might be the reason why we did not find any gender differences when they were performing the tasks while wearing eye-masks on stable and unstable platforms and likewise, this might affect their average scores for m-CTSIB. Supporting our findings, it was reported that male and female goalball players who participated in 2012 London Paralympic Games did not differ in static balance assessment (Bednarczuk et al., 2017). In addition, it was found that youth with VI participating in physical education classes 2–3 times a week exhibited no differences between genders in dynamic and static balance conditions (Rutkowska et al., 2015). Conversely, we found gender differences, and male athletes were better than female athletes with VI while performing the tasks without wearing eye-masks on stable and unstable platforms. In female athletes, the Star Excursion Balance Test (SEBT) scores were positively correlated with hip strength recommending that hip strength exercises could help to improve their postural balance (Ambegaonkar et al., 2014). Another study found that balance training performed three times a week for 7 weeks improved neuromuscular power and control in female athletes (Myer et al., 2006). In addition, significant associations between trunk muscle strength and balance performances of elderly were reported (Granacher et al., 2013). These findings suggest that VI female athletes could add strength and balance training programmes to improve their physical fitness levels.
Literature is scarce related to gender differences in postural balance in athletes with VI whereas studies conducted to investigate gender differences in individuals without VI revealed conflicting results. In detail, some studies showed that gender affect was low for postural balance (Anderson et al., 2019; Sabin et al., 2010); on the other hand, others found that women were better than men in dynamic postural control (Andreeva et al., 2020; Gribble et al., 2009; Whyte et al., 2015). Literature reports that girls perform better in balance tasks during childhood, in adolescence this difference disappears between boys and girls and a plateau in both sexes (Malina et al., 2004). Evidence also indicates less pivot displacement, both laterally and anteroposteriorly, in females than in males 9–14 years of age and 16–22 years of age (Malina et al., 2004). However, in the SEBT, male basketball players reached 5% farther than women in posterior reach direction, whereas average scores were not different across the genders (Sabin et al., 2010). To the best of our knowledge, postural balance has not been investigated adequately on samples of athletes with VI with taking the gender differences into consideration. Therefore, further research is needed for a better understanding of the gender differences in postural control of athletes with VI.
It is worth to discuss the limitations of this study. We utilized self-reported questionnaire to determine PA levels of athletes. In future, other PAL determination techniques such as accelerometers can be used (Starkoff et al., 2017). In total, 64% of participants in athletes with VI were blind athletes in B1 sport class, so number of athletes in B2 and B3 sport classes may be increased and then comparisons can be made according to sport classes. Finally, participants of this study were athletes so sedentary counterparts can be included and examinations can me made accordingly.
In conclusion, male athletes with VI had higher BMIs than female athletes with VI though their BMIs were found to be in a healthy range. In addition, VI group and their sighted controls had similar BMIs. Body composition parameters revealed gender differences, whereas VI athletes and sighted controls showed no differences. With respect to PA participation, we found that having a VI was not a barrier to have higher levels of PA stating that VI male athletes had higher levels of PA than their sighted male controls. Similar trends were observed between female athletes with and without VI as well as between male and female VI athletes. Only female athletes without VI spent more time on walking than their female VI counterparts. However, time spent on moderate levels of PA was higher in VI female athletes than their sighted female controls and male VI athletes. This was not different between male athletes with and without VI. High-intensity PA participation was higher in VI male athletes than male sighted controls and female athletes with VI. No difference was found between female athletes with and without VI in high-intensity PA participation. With respect to postural balance results, sighted athletes were better in conditions 1 and 3 and composite postural balance assessments. On the contrary, conditions 2 and 4 were not different between sighted and VI athletes. Only difference in VI athletes was observed in condition 2.
Footnotes
Acknowledgements
We thank the Turkish Blind Sports Federation for their full support. This research would not have been possible without B1 football and goalball athletes. We fully appreciate their willingness to be part of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.