
Abstract
Emotional intelligence, as a mental ability, consists of attention, clarity, and repair abilities, contributing to emotion management. Emotional intelligence is subject to changes induced by external environmental factors. However, little is known about changes in emotional intelligence among people with visual disabilities. This study aims to advance knowledge of the degree to which people with visual disabilities change emotional intelligence between “before” and “amid” the COVID-19 pandemic. A total of 81 participants with visual disabilities completed a Trait Meta-Mood Scale to assess emotional intelligence in Fall 2019 (n = 20), Summer 2020 (n = 31), and Fall 2020 (n = 30). While the attention and clarity abilities did not significantly change in Summer 2020, the repair ability significantly increased in Summer 2020. However, all three abilities significantly decreased in Fall 2020. People with visual disabilities were able to manage their negative emotions just a few months after the pandemic was declared. Yet, 1 year after the pandemic was declared, their emotional intelligence was significantly weakened. As a long-term effect, emotional challenges caused by the COVID-19 pandemic might have become strong enough to lead to decreased emotional intelligence abilities.
Introduction
Emotional intelligence
Emotional intelligence is viewed as a mental ability as it is influenced by both intelligence and emotion (Mayer et al., 2000). Emotional intelligence involves one’s ability to concentrate on emotional stimuli from environments, perceive emotions, understand emotional meanings, and regulate emotions, ultimately leading to promoting better emotional experience (Salovey et al., 1995). Emotional intelligence is widely beneficial in a range of contexts (e.g., school, workplace, and everyday behavior). For example, there is cumulative evidence that emotional intelligence is related to academic performance and professional success (Chew et al., 2013; Codier et al., 2008; MacCann et al., 2020; Romanelli et al., 2006). Johnson (2015) conducted a literature review study, suggesting that a significant correlation exists between academic achievement and emotional intelligence of students. Ferrando et al. (2011) conducted an empirical study with 290 young students (11.53 years of age on average) and observed a positive correlation between academic performance and emotional intelligence. A meta-analysis conducted by MacCann et al. (2020) concluded that self-rated emotional intelligence could be considered a stronger predictor of students’ achievement, as compared with standardized test scores. They also argued that being smart and working hard would not be sufficient for students to earn good grades, but additional determination emotional intelligence should be included, such that students could be competent in understanding and managing various emotions they encounter while studying.
Professionals with greater emotional intelligence were found to be better evaluated as compared with their peers with lower emotional intelligence. For example, Lopes et al. (2006) found that emotional intelligence was closely related to interpersonal sensitivity, sociability, and a positive work environment. Employees with higher emotional intelligence were less likely to engage in a lower degree of work–family conflict, goal conflict, and frustration at the workplace (Suliman & Al-Shaikh, 2007). Executive employees with higher emotional intelligence outperformed their peers with lower emotional intelligence in terms of quality of work performance, amount of effort expended on the job, speed on the job, quantification of work, capacity of work, care in handling company, ability to work without supervision, ability to handle different jobs, ability to get along with others, attendance and punctuality, initiative on the job, and overall work performance (Khokhar & Kush, 2009). Failed and derailed managers at work are often found to be equipped with poor social skills, resulting in being incompetent and incapable of building strong working relationships (Furnham, 2009).
Emotional intelligence is widely used as an indicator of successful social relationships with others leading to mental and physical health (Ciarrochi et al., 2001; Ruiz-Aranda et al., 2012). For instance, greater abilities to clarify emotions and repair negative emotions were correlated with a lower level of alcohol consumption (González Yubero et al., 2019). Male college students who have a lower level of emotional intelligence tended to be more engaged in illegal drug and alcohol use, deviant behaviors, and poor relationships with friends (Brackett et al., 2004). Brackett et al. (2005) also investigated emotional intelligence of couples in college and their relationships. They found that couples with a lower level of emotional intelligence showed the lowest scores on the quality of depth, support, and positive relationship but the highest scores on the quality of conflict and negative relationship.
Variations in emotional intelligence
Such mental ability as emotional intelligence is prone to changes. Such fluctuations in emotional intelligence were often observed among students (Esnaola et al., 2017; Khan et al., 2021; Stratton et al., 2008). For example, Gribble et al. (2017) conducted an observational study to assess the degree to which emotional intelligence changes among college students (650 undergraduate students enrolled in occupational therapy, physiotherapy, and speech pathology programs) during clinical placements (7 or 8 months). They found that emotional intelligence fluctuated while students undertook full-time, extended clinical placements. They argued that students with low-performance outcomes were likely to panic and withdraw in stressful contexts and could not work independently, all of which were associated with students’ emotional intelligence. Yadav et al. (2020) uncovered a negative correlation between emotional intelligence and perceived stress among dental undergraduate students.
Emotional intelligence and COVID-19 pandemic
Since the COVID-19 pandemic was declared, people have been practicing public safety measures such as social distancing, quarantine, and isolation. There have been growing concerns about the general population, health professionals, and people with underlying conditions experiencing mental health issues such as anxiety, fear, acute/posttraumatic stress disorder, and depression during the COVID-19 pandemic (Pfefferbaum & North, 2020; Talevi et al., 2020). It is reported that 5% of people affected by a crisis are likely to be left with a long-term problem, 20%–40% are likely to suffer from a psychological disorder in the medium term, and the remaining people (up to 80%) are likely to experience short-term mild distress (Hunt & Greaves, 2017).
Yet, people with high emotional intelligence are expected to successfully cope with emotional challenges via self-awareness, emotional control, and effective communication during the COVID-19 pandemic (Baba, 2020). In particular, the ability of emotional repair, one of the emotional intelligence constructs, could significantly contribute to amending the feeling of emotional struggle caused by stressful situations (Salovey et al., 1995). Given the logic, it is not uncommon to anticipate that the psychological effects of the COVID-19 pandemic on people today would be various by depending on one’s emotional intelligence level (Alonazi, 2020; Moroń & Biolik-Moroń, 2021; Soto-Rubio et al., 2020; Sun et al., 2021). Zysberg and Zisberg (2022), for instance, stated that emotional intelligence is likely to cause individual differences in managing emotions and securing social support contributing to reducing concerns about COVID-19.
Emotional intelligence also affects people with visual disabilities, leading to better emotional management (Parween, 2015). For example, Eniola (2007) empirically observed that Nigerian people with visual impairments who were trained to enhance emotional intelligence resulted in better controlling aggressive behavior, as compared with their peers with no training. Al-Tal et al. (2017) also found that the level of emotional intelligence in students with visual impairments was higher than that in peers with hearing impairment. They argued that those with visual impairments could speak and hear without restriction in contrast to their peers with hearing impairments; thus, the opportunity (or lack of opportunity) to communicate with others was believed to be a significant determination, facilitating (or weakening) one’s emotional intelligence ability. During the COVID-19 pandemic, many people (including those with visual impairments and blindness) had a lack of opportunity to interact with people due to public safety measures (e.g., social distancing and stay-at-home orders) (Senjam, 2020). It is expected that emotional intelligence in people with visual disabilities may be affected during the COVID-19 pandemic. However, little is known about the degree to which people with visual impairments and blindness increase, decrease, or fluctuate their emotional intelligence abilities as they live with the COVID-19 pandemic today. Thus, this study aimed to investigate the degree to which the emotional intelligence of people with visual disabilities changed before and during the pandemic.
Methods
Participants
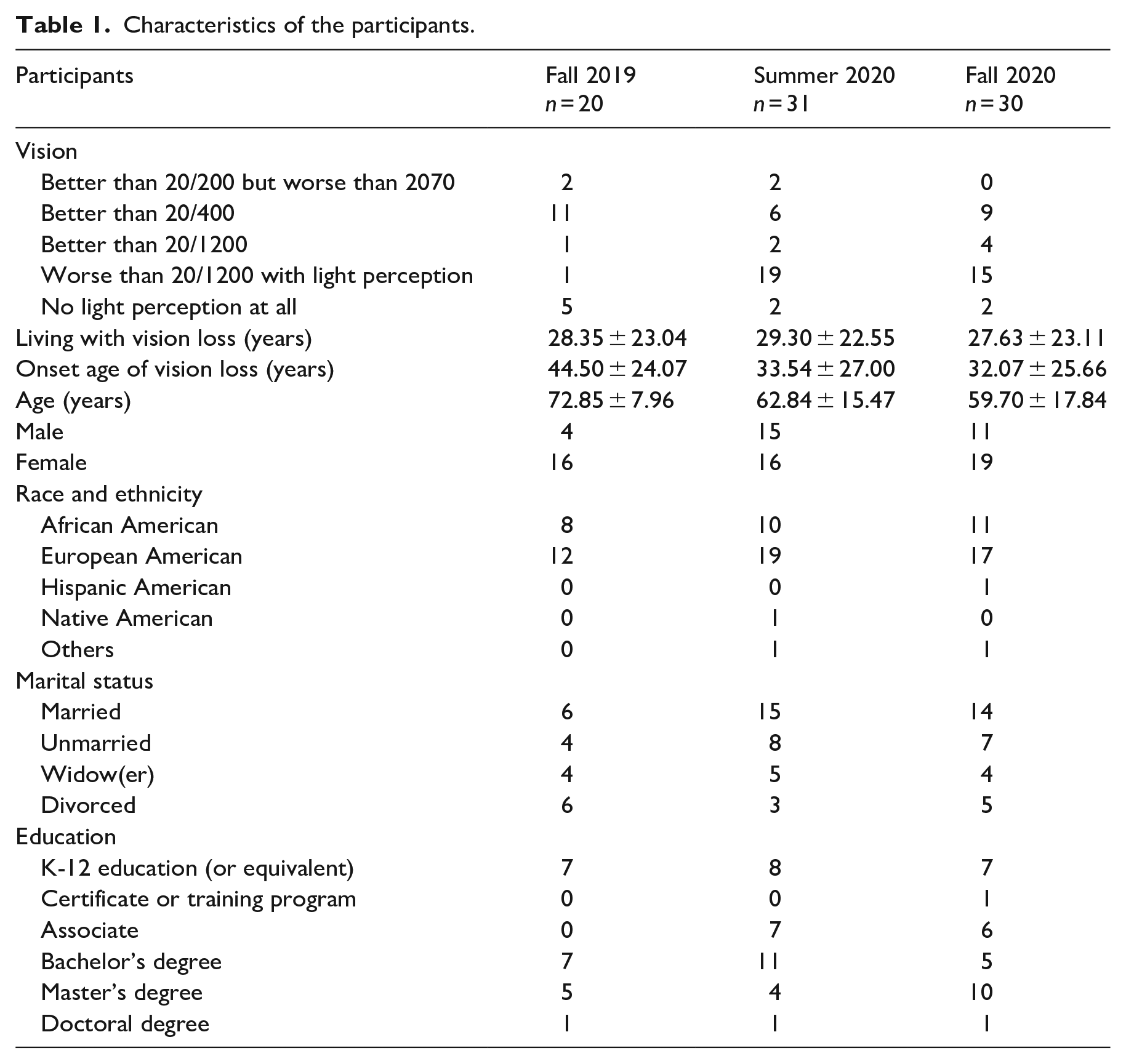
This study included 81 participants who met the following inclusion criteria: 18 years of age and older and visual acuity equal to or worse than 20/70 (see Table 1) (World Health Organization, 2008). This study referred to two previous studies completed in Fall 2019 (Kim, 2022) and Summer 2020 (Kim & Sutharson, 2023) to examine the trajectories of changes in emotional intelligence as compared with a set of newly collected data in Fall 2020. The data in Fall 2019 included 20 participants, the data in Summer 2020 included 31 participants, and the data in Fall 2020 included 30 participants. The same research participants were not invited. Recruiting different participants in each phase can help to ensure that the study sample is diverse and also reduce bias in the study, which will make research results more generalizable to the target population (Kukull & Ganguli, 2012; Lesko et al., 2017).
Characteristics of the participants.
Materials
This study used the Trait Meta-Mood Scale (TMMS) to assess participants’ emotional intelligence (Fitness & Curtis, 2005). Salovey et al. (1995) shortened the original TMMS-48 version by selecting 30 items as the 30 items had the highest factor loadings (⩾0.40) on the three meta-mood constructs (attention, clarity, and repair). Hence, this study used the TMMS-30 version with three constructs: attention to feelings (13 items, e.g., “I pay a lot of attention to how I feel,” Cronbach’s α = .86), clarity of emotional experience (11 items, e.g., “I usually know my feelings about a matter,” Cronbach’s α = .88), and repair of negative emotion (6 items, e.g., “No matter how badly I feel, I try to think about pleasant things,” Cronbach’s α = .82) (Salovey et al., 1995). Participants should complete the TMMS by using a 5-point Likert-type scale from 1 (“strongly disagree”) to 5 (“strongly agree”). The TMMS has often been used for the measurement of self-perceived emotional intelligence in people with visual disabilities (Kim, 2022; Kim & Sutharson, 2023). There is evidence that the TMMS can also be used for aging populations (Condon et al., 2021; Delhom et al., 2017, 2020, 2022; Galdona et al., 2018) including those with visual disabilities (Kim, 2022).
Procedures
This study was in collaboration with local community organizations such as a public library for the blind. They informed their community members of the opportunity to participate in this study. Potential participants were given the research team’s contact information. The research team waited until potential participants reached out to the team. Potential participants were verbally informed of key elements of this study (e.g., objectives, procedures, and expected outcomes), and they decided to participate (or decline to participate) in this study. The informed consent form was offered in various formats (e.g., large print, Braille, and verbal) depending on participants’ preference. Participants could use assistive technologies (text-to-speech software, magnifiers, closed-circuit televisions, and so on) to read the informed consent form. Participants could obtain assistance from their family members by reading the informed consent form. The research team could also inform them verbally. During the COVID-19 pandemic, informed consent was verbally obtained from each participant as this research was conducted by phone. This study was approved by the Institutional Review Board (IRB). Each interview was administered for no longer than 60 min. The interviews were voice-recorded. The interviews in Fall 2019 were conducted by visiting each participant’s home, while the interviews in Summer and Fall 2020 were conducted by phone due to the COVID-19 pandemic. The TMMS questionnaire contains texts only without any visual components. Participants completed the TMMS questionnaire verbally as an interviewer read out loud each question. Participants opted to do so because it was a relatively short questionnaire, and an interviewer was available for them to clarify any questions while completing the questionnaire. Participants were allowed to ask for the interviewer to repeat reading out loud questions as many as they wanted but also allowed to pause while thinking.
Results
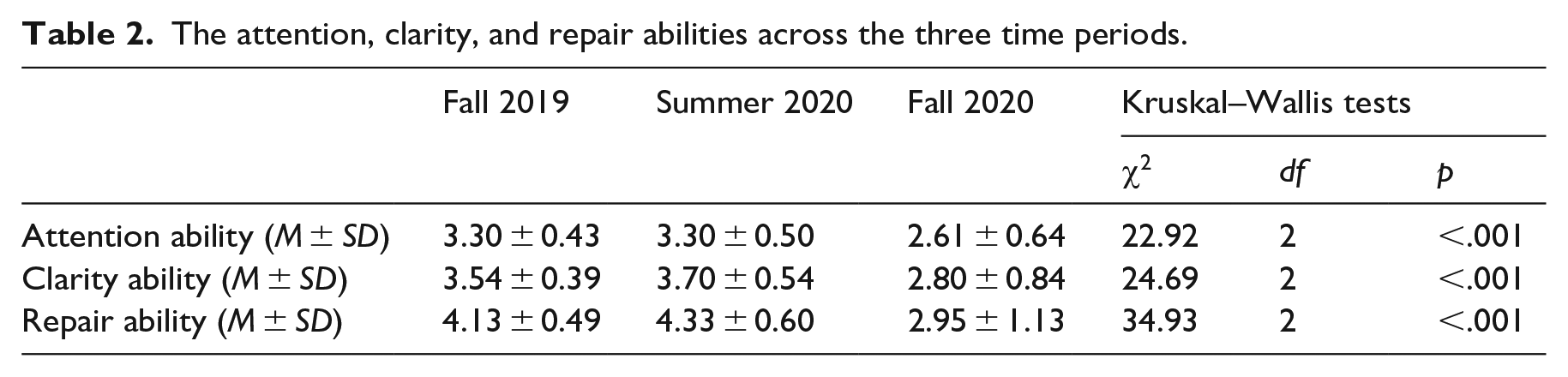
Cronbach’s alpha of the participants’ responses to the TMMS was .72, .72, and .9 for Fall 2019, Summer 2020, and Fall 2020, respectively. The TMMS assessed three constructs of emotional intelligence: attention, clarity, and repair abilities. As shown in Table 2, Kruskal–Wallis tests found that there were significant differences in each construct across the three time periods.
The attention, clarity, and repair abilities across the three time periods.
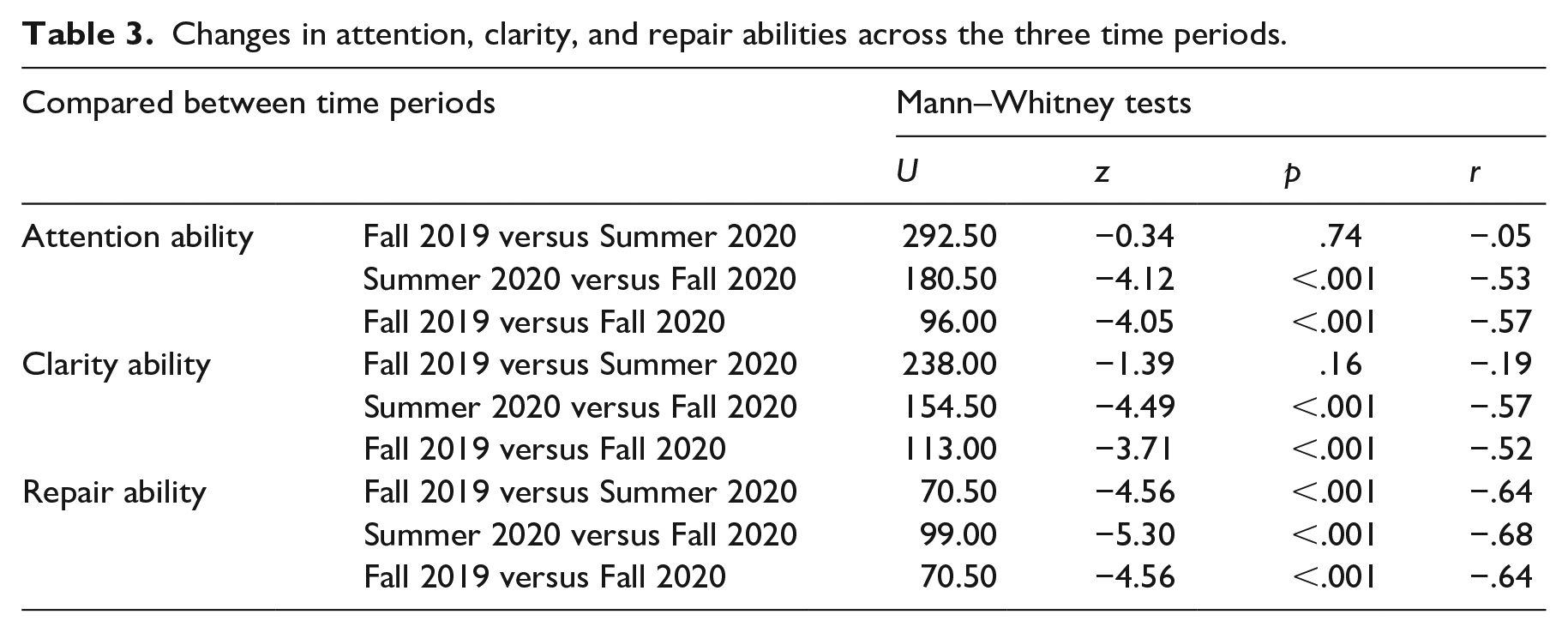
As shown in Table 3, a post hoc analysis with Mann–Whitney tests was followed to investigate the significant differences. The attention ability and the clarity ability did not significantly change in Summer 2020 compared with Fall 2019; however, both significantly decreased in Fall 2020 compared with Summer 2020. Furthermore, both significantly decreased in Fall 2020 compared with Fall 2019. As another construct of emotional intelligence, the repair ability showed fluctuation in that it significantly increased in Summer 2020 but significantly decreased in Fall 2020. The level of repair ability in Fall 2020 was significantly lower than that in Fall 2019.
Changes in attention, clarity, and repair abilities across the three time periods.
Such fluctuation in the repair ability might account for the changes in the other two abilities, attention and clarity. For example, as the repair ability increased, the participants’ emotions might be somehow well controlled and, in return, their attention and clarity abilities were not significantly impaired resulting in no significant changes between Fall 2019 and Summer 2020. On the contrary, after 1 year, in Fall 2020 significantly decreased repair ability might be unable to successfully manage the emotional stimuli from environments amid the pandemic; thus, the attention and clarity abilities might have also significantly decreased in Fall 2020.
Discussions
Emotional intelligence is viewed as a critical human mental ability as it can help people enhance interpersonal relationships via emotion management both personally and professionally. Although emotional intelligence is subject to changes due to external environmental factors such as the COVID-19 pandemic, little is known about the changes before and during the pandemic among people with visual disabilities. Thus, this study examined their emotional intelligence in terms of three constructs: attention, clarity, and repair abilities. It found changes in emotional intelligence abilities over the three seasons (Fall 2019, Summer 2020, and Fall 2020) before and amid the COVID-19 pandemic. Both attention ability and clarity ability of emotional intelligence remained constant between Fall 2019 and Summer 2020; however, they significantly decreased in Fall 2020, along with repair ability. One year of the pandemic duration (Fall 2019 to Fall 2020) might be sufficient time to negatively affect their emotional intelligence abilities.
Yet, time per se might not necessarily be considered as a sole determinant affecting their emotional intelligence but there might also be other factors. For instance, Esnaola et al. (2017) conducted a 1-year observation study with students (aged from 12 to 18 years) and found that the students experienced changes in emotional intelligence abilities, for example, a combination of increasing, decreasing, and remaining constant over 1 year. They hypothetically stated that individual backgrounds (e.g., age, education, and social interaction) could induce such fluctuations in emotional intelligence. Stratton et al. (2008) also observed that emotional intelligence of medical students was significantly decreased between the first year orientation and the third year clinical training, especially associated with two abilities of emotional intelligence, attention to feelings and mood repair. They claimed that the reduction of emotional intelligence was likely influenced by the nature and quality of personal and professional relationships while the students were in medical training. Hill et al. (2018) found that medical students were vulnerable to being exposed to stressors related to excessive workload, difficulties with studying, conflicts in work–life balance, medical school peer relations, and health concerns.
Given the logic, it could be argued that emotional challenges induced by the pandemic could cause emotional intelligence to weaken among the participants in this study. The argument is supported by the empirical research study of Yadav et al. (2020) who found a negative correlation between perceived stress and emotional intelligence among college students. They suggested that the inverse relationship occurred due to students’ stressful environments (e.g., time-bound work and personal pressure to do well). Gribble et al. (2017) also reported that emotional intelligence could fluctuate depending on stressful settings. Thus, we theoretically suggest that damaged emotional intelligence might be recovered if stressors were eliminated. Khan et al. (2021) contended that emotional intelligence was closely associated with well-being, self-control, emotionality, and sociability. Therefore, in-person relationships could serve as a facilitator for the building of emotional closeness and bonding, which was, however, difficult to accomplish via online communication only (Khan et al., 2021). Based on the literature, the results of this study could hypothetically be interpreted accordingly—that is, participants in this study might have struggled from being lonely away from in-personal relationships with family and friends since the COVID-19 pandemic was declared and have been under a lot of stress, so that their emotional intelligence was weakened.
Therefore, we conclude with the suggestion that emotional intelligence in people with visual disabilities is not static, but more likely to be dynamic, such that it could increase or decrease in response to various environmental factors. If there was, for example, a safe way for them to keep social relationships or to learn how to manage their emotional challenges, their emotional intelligence would have been protected. Further research is needed to address the knowledge gap.
Limitations of the study
Due to the COVID-19 pandemic, the data collection was accomplished using different methods (in-person in 2019 and phone calls in 2020). A consistent method might have led to different results. To protect the participant’s privacy, the research team requested that family members did not attend or stay nearby during the study. When conducting the study in person, the research team could manage family members’ access. Yet, when conducting the study by phone, the research team could not manage it directly but assumed that they complied with the research team’s request.
Future research
The World Health Organization has recently declared an end to COVID-19 as a public health emergency (United Nations, 2023). Another data collection will be performed to compare before, amid, and after the COVID-19 pandemic. The research findings will help many stakeholders to better prepare for similar pandemic situations in the future.
Conclusion
This study contributed to advancing knowledge of changes in emotional intelligence abilities among people with visual disabilities before and amid the COVID-19 pandemic. A short-term effect of the pandemic may not be significant, but a long-term effect could be significant leading to poor mental health and low quality of life. Adequate training to enhance emotional intelligence would be necessary to cope with emotional stress, yet it should be ensured to make the training accessible to people with visual disabilities. For example, visual training materials should be avoided and prepared in alternative formats such as large print and audio files. Future research will focus on developing an emotional intelligence training program suitable for those with visual disabilities at risk of emotional instability.