
Abstract
Hope and happiness are positive emotions that affect an individual’s thoughts, feelings, and behavior. These two variables also affect different aspects of an individual’s life such as physical health, lifespan, academic performance, socialization process, creative thinking, problem-solving ability, and mental health. This study seeks to examine the effectiveness of mindfulness-based stress reduction (MBSR) in improving hope and happiness in visually impaired people. Employing a quasi-experimental pre-test–post-test design with a control group, this study sought to examine the degree of the effectiveness of MBSR therapy in improving hope and happiness in visually impaired people. The participants were selected from all visually impaired men aged 20 and 40 living in Tehran in 2023, who were supported by the State Welfare Organization of Iran and were members of the White Cane Society. A total of 40 visually impaired people were selected as the participants and randomly assigned to intervention and control groups (each with 20 members). The data were collected using Snyder’s Adult Hope Scale (1991) and Oxford Happiness Questionnaire (OHQ; 1990). The participants in the intervention group attended eight 90-min MBSR intervention sessions once a week. One-way analysis of covariance (ANCOVA) was used to analyze the data. The mean hope scores in the pre-intervention and post-intervention stages were 20 ± 3.28 and 25.53 ± 3.138, respectively. The mean happiness scores in the pre-intervention and post-intervention stages were 66.86 ± 5.91 and 75.93 ± 4.47, respectively (mean difference = 75.93 – 66.86). The findings showed that MBSR was effective in improving hope (F = 32.7; p = .01) and happiness (F = 45.86; p < .001) in men with visual impairment. As a result, MBSR can be considered an effective intervention to enhance happiness and hope while reducing the psychological complications associated with visual impairment in affected individuals.
Introduction
Visual impairment (VI) and blindness lead to increased mortality, reduced quality of life, and significant economic losses. The number of visually impaired and blind people is estimated to increase by approximately 90% and 50% from 2020 to 2050 (Taryam et al., 2022). Blindness and VI are challenges that make affected people face psychological and social problems (Bhagchandani, 2014). Mood changes and psychological challenges often manifest in VI people from childhood. For instance, a study found that the prevalence of anxiety and depression among American children with vision problems (3–17) was more than twice that of their peers (Zhu & Haegele, 2024). Visually impaired people face psychological and social problems, poor participation in social activities, and the lack of independent life (Aslan et al., 2012). Moreover, exposure to negative family and public attitudes can lead to the internalization of negative self-esteem in people with VI and limit their participation in social activities, the workforce, and the family itself (Chilwarwar and Sriram, 2018). Blindness or VI is associated with feelings of helplessness, low self-esteem, stress and anxiety caused by mobility problems, and depression (Onuigbo et al., 2019). In a comparative study of pupils who were blind from birth and pupils who had no VI, lower emotional intelligence, poorer performance, and reduced self-efficacy were associated with individuals born with VI (Raimule & Bhawalkar, 2015).
Studies have shown that around the world there are about 36 million people who are completely blind, 217 million people with moderate to severe VI, and 253 million people with (mild) VI (Ezinne et al., 2022). In Iran, according to statistics, the available data up to 2023 indicate that 865,127 people with mild to severe VI, which constitutes 13.5% of the country’s disabled people. Besides, 722,212 of VI people are female and 142,915 are male (Malekitabar et al., 2024). VI negatively affects quality of life and is associated with depression (Zhang et al., 2013). VI restricts the ability to move and control oneself and the surrounding environment. People with VI reported experiencing anxiety, depression, sleep problems, and fatigue (Choi & Harrison, 2023).
Hope is a feeling of ecstasy experienced when a person expects a better future ahead of his or her eyes. Snyder, the founder of the theory of hope and hope therapy, defines hope as a tool consisting of two concepts – the ability to design passages toward desirable goals despite the existing obstacles or a motivating factor necessary to use the agent of hope. According to Snyder, these passages include a set of requirements such as having valuable personal goals and realizing the ability to develop strategies in pursuit of goals. He considered hope to consist of the power of will, the power to find a way, having a goal, and recognizing obstacles. Hope is an active characteristic that involves having a goal, the power of planning and the will to achieve the goal, paying attention to obstacles to achieving the goal, and being able to overcome them (Feldman & Snyder, 2005). There is a significant relationship between hope and well-being as well as various positive life-related outcomes including sports performance, academic performance, physical health, and psychological adjustment, which is related to coping skills among people with illnesses and health-related outcomes (Singh, 2015). Hope is considered a psychological strength that can greatly help foster mental health. Hope facilitates crossing important obstacles and deep chasms on the way. Hope gives people the courage to face their circumstances and find the capacity to overcome them (Feldman & Snyder, 2005). One of the most important sources of psychological problems is the loss of hope in life (Banson, 2006).
Happiness is also known as one of the most important psychological needs of human beings, which has a major impact on personality development and mental health. Indeed, happiness is one of the basic human emotions that everyone has experienced based on their world and almost everyone wants it for their loved ones (Bayani, 2008). Feeling happy is a good psychological or emotional state defined by positive or pleasant feelings that range from contentment to extreme happiness, the absence of negative affect, and a combination of positive affect and life satisfaction, and the way a person evaluates their life and plans where he or she is going (Fitzgerald & Danner, 2012). Happiness and health have a significant relationship with each other (Diener, 2008).
Mindfulness is defined as the distance between a certain type of awareness and a state of attention and awareness of what is happening, which was introduced by Kabat-Zinn in 1985 (Brown & Ryan, 2003). Mindfulness-based interventions are efficient interventions that provide potential assurance as an effective method for medical care. Mindfulness is an ancient Buddhist practice that is deeply relevant to our lives today. This connection has nothing to do with Buddhism or becoming a Buddhist per se, but everything to do with awakening and living in harmony with oneself and the world. It has to do with examining who we are, by questioning our view of the world and our place in it, and by cultivating some appreciation for the completeness of each moment we live. The most important thing is to be yourself and not try to become something you are not already (Kabat-Zinn, 2001). Mindfulness has a negative correlation with negative and incompatible thoughts and has a significant positive relationship with mental and physical health (Baer et al., 2019). Physical activity-based interventions such as tai chi, yoga, and dance can have positive outcomes for people with VI (Sweeting et al., 2020).
People might have misperceptions about their abilities and strengths. Sometimes these perceptions are caused by countless stresses that they experience in their daily lives. Mindfulness-based stress reduction (MBSR) is now considered a non-pharmacological option for treating many diseases (Lyngroth & Gammelsæter, 2023; Niazi and Niazi, 2011). MBSR, as an intervention rooted in Eastern cultures and with special emphasis on moments of awareness and relaxation, can be effective for visually impaired people who live in Eastern cultures and are somewhat familiar with other mindfulness techniques. As such, this study seeks to examine the effectiveness of MBSR in improving hope and happiness in visually impaired men.
Method
Research design and participants
This study adopted a quasi-experimental pre-test–post-test design with a control group. The participants were selected from all visually impaired men aged 20 and 40 living in Tehran in 2023, who were supported by the Satet Welfare Organization of Iran and were members of the White Cane Society. All participants had been blind or visually impaired since birth. A total of 40 visually impaired men were selected as the participants and randomly assigned to intervention and control groups (each with 20 members). The sample size was estimated using the Fleiss sample size estimation equation (Fleiss et al., 1980), where β = 0.90, p0 = .80, p1 = .7, r = .7, and α = .05. Accordingly, the sample size for each group was estimated at 20 participants. The effect size for this sample can detect medium effect.
The inclusion criteria were: (1) not having severe psychological disorders, confirmed through medical record evaluations of welfare organization and structured clinical interviews based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) implemented by psychiatrist, (2) not suffering from other sensory–motor disabilities, (3) willingness to participate in the study and the intervention sessions, (4) obtaining a score one standard deviation below the mean on the Adult Hope Scale and OHQ, and (5) the ability to read the items in the questionnaire in braille and answer them independently. The exclusion criteria were: (1) simultaneous participation in other psychological or support programs and (2) the absence in more than two intervention sessions.
Instruments
Adult Hope Scale: This self-report instrument was developed in 1991 to measure Hope using 12 items that take 2 to 5 min to complete (Snyder et al., 1991). The scale measures operative thinking (four items) and strategic thinking (four items), and the remaining four items are distractors. The total score on the scale ranges from 0 to 48, with higher scores indicating more hope. Many studies have supported its reliability and validity as a measure of hope. The internal consistency of the whole scale was estimated at 0.74. The average validity and reliability coefficients for the scale were reported as 91%. The internal consistency of the whole scale ranged from 0.74 to 84%, and its test–retest reliability was 0.80 and higher within an 8- to 10-week interval (Snyder & Lopez, 2007). In this study, the reliability of the scale was confirmed with Cronbach’s alpha of .90 for people with VI.
Oxford Happiness Questionnaire: The OHQ was developed by Hills and Argyle (2002). This questionnaire has 29 items that are scored on a four-point scale ranging from 0 to 3. The highest score in this questionnaire is 87, which indicates the highest level of happiness and the lowest score is 0. The lower the respondents’ scores are; the less happy they are. The reliability of the questionnaire using Cronbach’s alpha coefficient was reported as 0.9 and its retest reliability within 7 weeks was estimated at 0.78. The concurrent validity of this instrument was calculated using peer evaluation and was reported as 0.43 (Hills & Argyle, 2002). In this study, the validity of the questionnaire was recalculated for people with VI and was reported to be 0.82.
Procedure
After the approval of the research proposal, the participants were selected based on the questionnaire scores and inclusion criteria and were then randomly divided into two intervention and control groups (see the flow diagram in Figure 1). Then, in the pre-test phase, the questionnaires were written in braille and administered to the participants in both groups. The participants in the intervention group attended the MBSR intervention for eight 90-min sessions held once a week. During the intervention, the participants in the control group did their routine work and received their routine care needs and brochures about diet compliance and proper use of urban space and urban furniture. The content of the intervention was developed by the researchers based on the educational materials written by Kabat-Zinn (2003) and de Vibe et al. (2017), as detailed in Table 1. The intervention days and places were specified upon the agreement of the participants in the intervention group. The questionnaires were re-administered to the participants in both groups as the post-test one week after the completion of the intervention sessions.
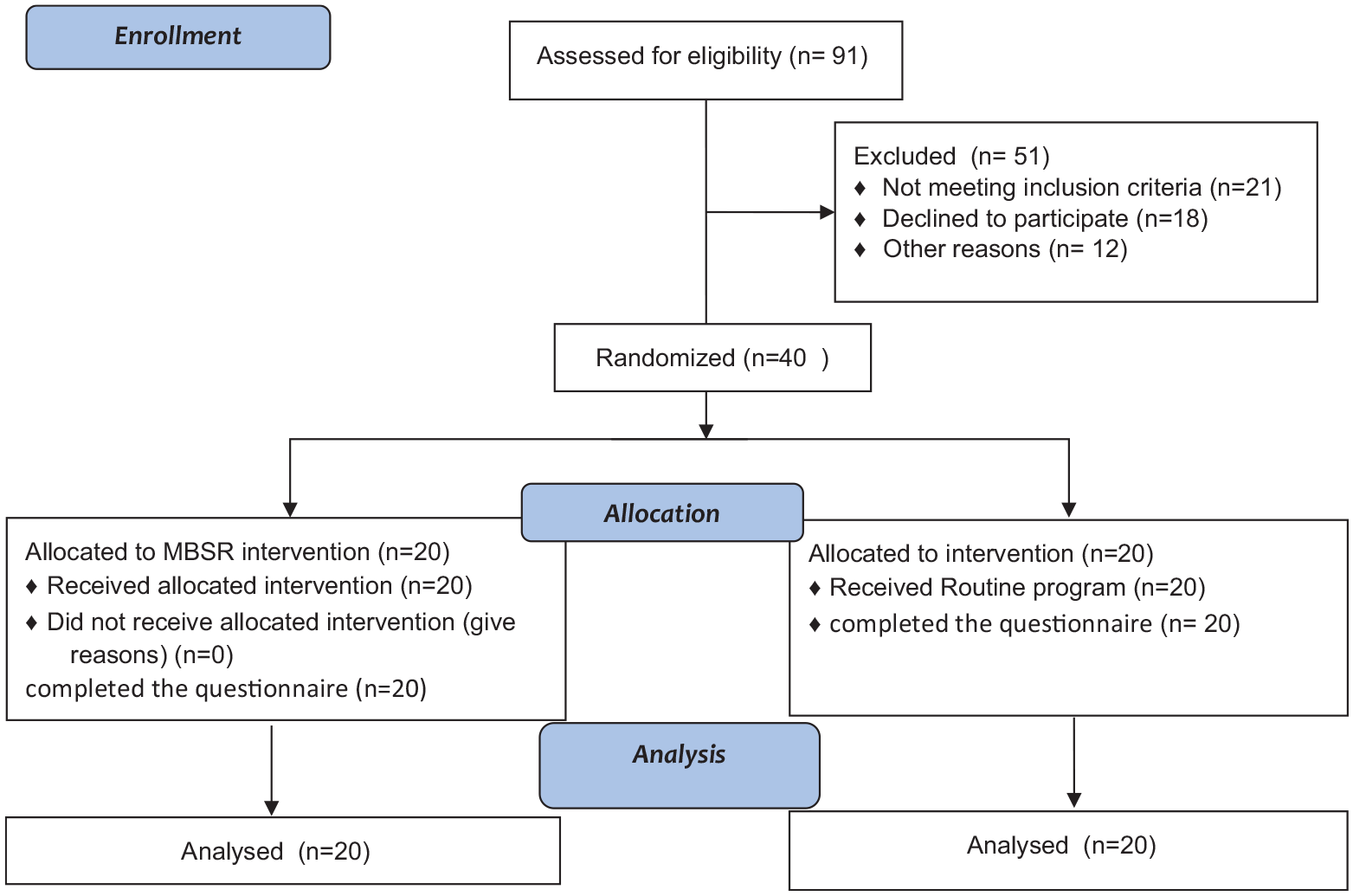
CONSORT flow diagram of reporting enrolment, allocation, and analysis of participants.
The content of the MBSR sessions (de Vibe et al., 2017; Kabat-Zinn, 2003).
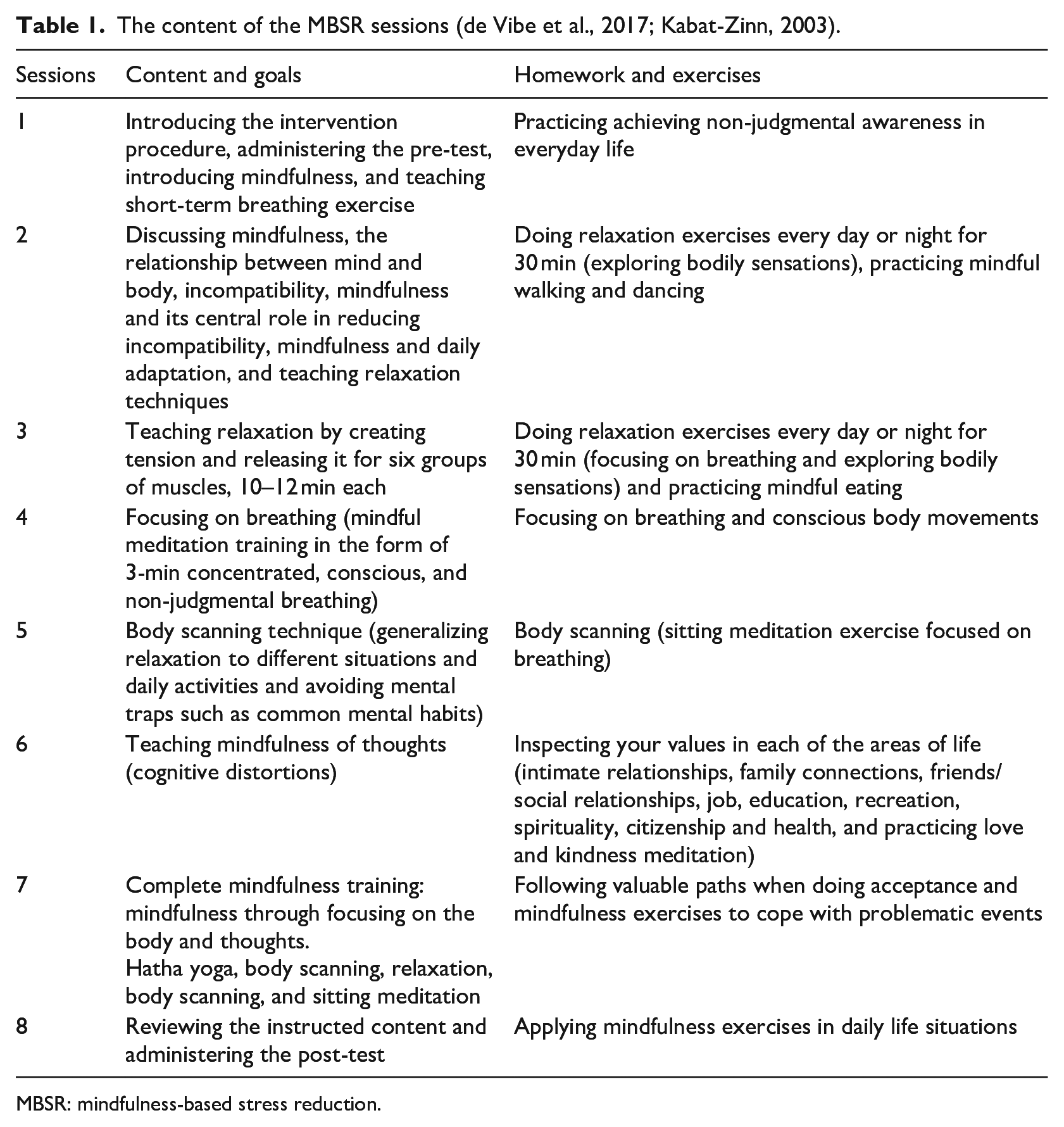
MBSR: mindfulness-based stress reduction.
Data analysis
Descriptive statistics were used to manage the data and calculate measures of central tendency and dispersion. The data analysis was performed using the analysis of covariance (ANCOVA). Moreover, the dependent sample t-test was run to compare the participants’ scores in the pre-intervention and post-intervention phases. Data analysis was performed using SPSS-28 software.
Ethical considerations
The participants’ data were kept anonymously and confidentially and were used only in line with the research objectives. Participation in the study was voluntary and both verbal and written consent was obtained from all participants. The intervention sessions were held free of charge. After the completion of the study, the intervention sessions were also held for the patients in the control group.
Results
The mean age of the participants in this study was 33 ± 3.21 years. Table 2 shows the descriptive statistics for the hope and happiness scores in the two intervention and control groups in the pre-intervention and post-intervention stages.
The descriptive statistics for hope and happiness in the two groups.
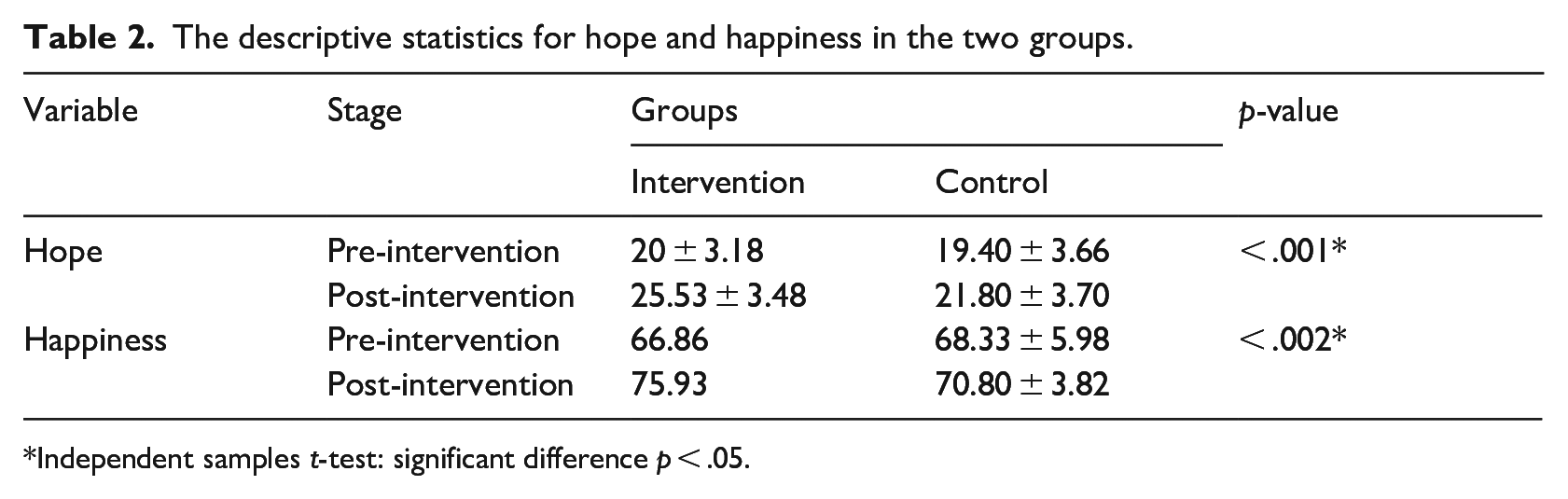
Independent samples t-test: significant difference p < .05.
As shown in Table 2, the scores of both variables in the post-intervention stage show some changes compared to the pre-test stage. However, to check if there were any significant differences between the pre-intervention and post-intervention scores, ANCOVA was used. Before running ANCOVA, its assumptions including the normal distribution of the variables, homogeneity of variances, and homogeneity of the regression slope were tested using the Kolmogorov–Smirnov and Levene’s tests (see Table 3).
Testing ANCOVA assumptions.
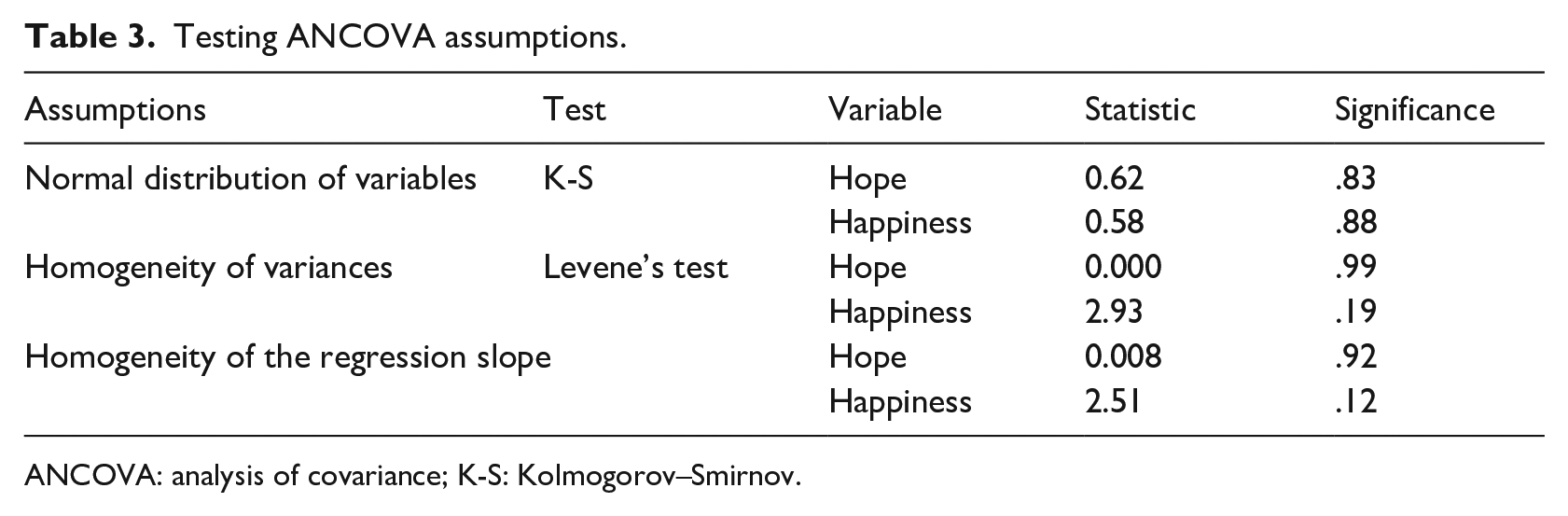
ANCOVA: analysis of covariance; K-S: Kolmogorov–Smirnov.
The ANCOVA results to compare the hope and happiness scores in the intervention and control groups in the post-intervention stage confirmed a significant difference in the hope scores between the intervention and control groups at a 99% confidence level (F = 7.32; p = .01; see Table 4). Thus, the MBSR intervention was effective in improving the hope of visually impaired people, and a 29% increase in the hope of visually impaired men can be attributed to the effectiveness of the MBSR intervention. Moreover, a significant difference was observed in the happiness scores between the intervention and control groups at a 99% confidence level (F = 45.86; p = .001). Thus, the MBSR intervention was effective in improving the happiness of visually impaired people, and a 62% increase in the happiness scores of the visually impaired men can be attributed to the effectiveness of the MBSR intervention.
ANCOVA results for the research variables in the two groups of visual impairments participants.
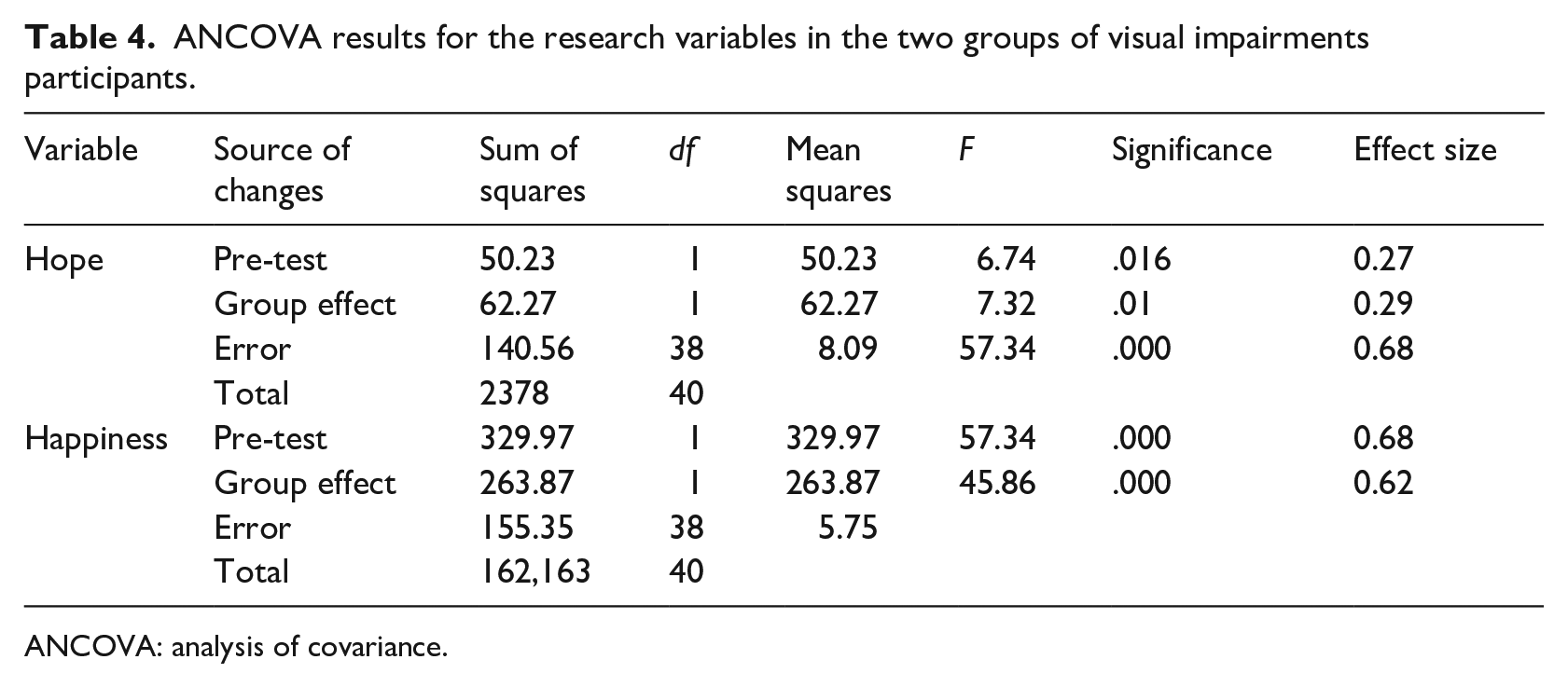
ANCOVA: analysis of covariance.
Discussion
This study examined the effectiveness of the MBSR intervention on the hope and happiness of 40 visually impaired people in 2023 in Tehran. The findings indicated that the MBSR intervention effectively improved hope and happiness in visually impaired people. Moreover, after the intervention, the experimental group scored higher on the hope questionnaire. Participants believed that the MBSR intervention helped them focus on the present moment and appreciate what they have in their lives. Hope is a construct that provides a sense of ability to cope with negative life events and has a positive effect on emotional health (Tumkaya, 2005).
In addition, participants reported increased happiness scores following the intervention compared to before the intervention. They acknowledged that engaging in group exercises and activities, including walking and eating mindfully with other people, listening to music, and performing rhythmic movements provided them with valuable opportunities to enjoy the moments of being together. Besides, MBSR enabled them to experience something different in their lives.
Happiness is one of the most influential variables in a person’s life, which makes people evaluate positive events more than negative events. Happiness brings peace and security and is a factor for better decision-making in life plans (Taylor & Adams, 2019). This is to argue that being in the present involves developing new attitudes, non-judgmental acceptance, and getting closer to understanding of feelings, thoughts, and bodily sensations to get rid of negative moods. In addition, MBSR therapy changes thoughts, feelings, and emotions and replaces maladaptive coping skills with adaptive ones. As a result, MBSR exercises teach a person how to see the events around and inside them exactly as they are, accept themselves and their experiences as they are, and accept and logically respond to negative thoughts and unpleasant feelings such as feeling burdened, inability to do daily and personal affairs, concerns about becoming a burden on the family, and the loss of emotional and social support. Effective MBSR exercises and solutions can reduce stress and improve the quality of life of visually impaired people.
Likewise, Mohanty et al. (2019) showed that yoga exercises as an alternative to physical fitness for visually impaired children can improve a wide range of physical variables, including muscle strength, endurance, coordination, flexibility, and respiratory health in these children. Marques (2014) found that mindfulness improves spiritual health by increasing the sense of intrapersonal, interpersonal, and transpersonal connection, which is associated with an increase in self-perceived emotional, social, and physical health. Stone (2022) implemented a yoga and mindfulness program for visually impaired students and showed that performing yoga and mindfulness exercises improves students’ mobility, class participation, and self-regulation. The use of mindfulness-based interventions in other age groups of people with VIs, such as the older adults, can be useful. For example, in a research, mindfulness-based music therapy helped reduce depression in blind older women. Also, this treatment helped in emotional regulation of the research participants (Chan et al., 2023). In this study, the intervention was implemented in the form of group therapy on men with VI. Participation in the group allowed these men to learn from and interact with one another, gaining insights into other’s experiences. Participation in group therapy forms could have positive effects of interventions on all groups, including people with VI (Naylor & Labbé, 2017).
Furthermore, research shows that MBSR can even be used as a complementary treatment to help people with VIs. For example, MBSR has been employed to reduce intraocular pressure in people with ocular hypertension (Dada et al., 2022). In addition, MBSR has been shown to alleviate acute central serous chorioretinopathy in patients (Özcan & Karapapak, 2024). Tran et al. (2024) conducted a systematic review and meta-analysis on the integration of meditation and breathing exercises as a potential management method in people with VI. The findings showed improvement in physical fitness for people with VI after meditation and breathing exercises. Moreover, Rondhianto et al. (2023) showed that mind–body therapy effectively reduces intraocular pressure in patients with glaucoma by 16%, so mind–body therapy, especially mindfulness meditation and yoga (ocular yoga, pranayama, and hatha yoga) can be complementary treatment options in glaucoma patients to reduce intraocular pressure without a head-down position. This study has some limitations, most notably that participants were selected only from visually impaired men living in Tehran. Besides, the study was exclusively conducted on male participants.
Conclusion
The findings from this study showed that MBSR improves the hope and happiness of visually impaired people. One of the most important problems of people with VI is adapting to the limitations and disabilities caused by VI, which can lead to maladaptive behaviors and psychological problems such as depression, anxiety, and stress. Thus, MBSR can be applied as an effective intervention to improve the happiness and hope of visually impaired people, help them adapt to their living conditions, and reduce psychological complications.
Footnotes
Acknowledgements
The authors would like to appreciate the officials in the State Welfare Organization in Tehran, and the participants who cooperated closely with them.
Author contributions
A.K.-K., S.G., and A.M. contributed toward conducting research, data gathering, and analysis. A.K.-K. was involved in the conceptualization, study design, and drafting of the initial version, data gathering, and analysis. Final approval was done by all the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
To comply with the ethical principles of voluntary participation, verbal and written informed consent was obtained from the participants for conducting the research. The participants were also reassured of the confidentiality of their information. This research was approved by Khatam University research administration.