
Abstract
In the Netherlands, access to deafblind-specific rehabilitation and education is often based on medical definitions for vision impairment and for hearing loss. However, not everyone with deafblindness (DB) meets these definitions because DB is not solely a result of limitations in bodily functions and structures, but also of limitations in daily functioning. Therefore, using a functional definition that describes a disability in terms of its impact on daily functioning, alongside the medical definitions, would be better suited for determining who needs access to deafblind-specific support. However, such a definition did not yet exist in the Netherlands. To develop a functional definition of DB, consensus among experts (experts-with-lived-experience and experts-with-working-experience) on how to define DB was needed. To investigate the consensus of experts, a Delphi study was conducted, in which 45 Dutch experts participated. The study consisted of a questionnaire with 30 multiple-choice statements on eight topics related to defining DB. After three rounds, consensus was reached on 24 of the 30 multiple-choice statements. These results were used in a follow-up process in which the Dutch functional definition of DB was developed.
Keywords
Introduction
Within the field of deafblindness (DB) research and daily professional practice, there is no consensus on how to define the population of people with DB (Larsen & Damen, 2014), and the terminology used to describe this population varies (e.g., DB, dual sensory loss, combined vision and hearing loss; Minhas et al., 2022; Wittich et al., 2013). This variation could possibly be explained by the large heterogeneity within the population (Larsen & Dammeyer, 2021; Nelson & Bruce, 2016). Despite the European Parliament (2004) recognising DB as a distinct disability, it is often not defined as such and is instead described as a combination of two disabilities (Simcock & Wittich, 2019). However, people with DB face unique challenges because with both vision and hearing loss, one cannot compensate for the loss of one sense with the other (Dammeyer, 2015; Wittich et al., 2016). Therefore, DB should be recognised and defined as a distinct disability (Meekins-Doherty et al., 2025).
The existing definitions of DB are often medical definitions (Bright et al., 2023; Hoevenaars-van den Boom et al., 2009; Larsen & Damen, 2014; Minhas et al., 2022). These definitions usually include a combination of medical criteria for vision impairment (visual acuity and/or visual field) and hearing loss (loss of decibels in both ears and/or best ear). These criteria describe DB solely in terms of limitations in bodily functions and structures and are commonly used in the Netherlands by institutions such as healthcare organisations, rehabilitation centres, insurance companies, and educational organisations to assess eligibility for DB-specific support. The International Classification of Functioning, Disability, and Health (ICF) model, however, emphasises that the experience of a disability is not solely based on the physical aspect but on the interaction between impairments in bodily functions and structures, personal characteristics, environmental factors, and additional problems (World Health Organization [WHO], 2001). Therefore, defining DB only by medical criteria for vision impairment and hearing loss is not in line with the ICF model and may not be appropriate for determining eligibility for support.
Another approach to defining DB is through a functional definition (Larsen & Damen, 2014; Minhas et al., 2022). A functional definition describes a disability in terms of its impact on daily functioning and participation in society (Dammeyer, 2014). The term ‘functional’ in this context does not refer to the medical meaning (e.g., body functioning), but rather to the individual’s ability to perform activities and to participate in society, aligning with the domains of activities and participation in the ICF model (WHO, 2001). Describing a disability functionally underscores that similar impairments in bodily functions and structures do not necessarily lead to comparable challenges in daily functioning.
Using both a functional and a medical definition to define a population aligns with the ICF model (WHO, 2001). However, there is limited literature on functional definitions of populations with disabilities, apart from the Nordic Definition of DB, which is referred to as a functional definition (Dammeyer, 2010; Danermark & Möller, 2008; Larsen & Damen, 2014). Developed by experts from the Nordic countries (Centre for Welfare and Social Issues, 2016; Deafblind International, n.d.), this Nordic definition was considered not fully applicable to the Dutch context, according to Dutch experts, as it did not address the specific challenges and key issues present in the field of DB in the Netherlands. These key issues include the existence of various subgroups within the DB population, the characteristics (e.g., age of onset or syndrome) that should define these subgroups, and whether people with vision impairment and hearing loss due to ageing (age-related DB) are considered part of the DB population. The Nordic definition does not explicitly describe functional definitions for subgroups, such as congenital, acquired, and age-related DB. Consequently, it remains unclear what specific characteristics define these subgroups and what distinct challenges are faced by each subgroup. To achieve uniformity in defining the DB (sub)population(s) in the Netherlands, it was considered crucial that experts – specifically people with DB (experts-by-lived-experience) and those who support them (experts-by-working-experience) – reached consensus on these key issues.
This study
The primary aim of the study was to investigate the consensus of experts-by-lived-experience and experts-by-working-experience on how to functionally define DB in the Netherlands. This study is part of a larger project structured into three phases. Initially, a literature search was conducted to gather insights into how DB is defined in scientific literature. Following this, the study proceeded with a Delphi study, as detailed in this paper. Subsequently, the final phase focused on developing the Dutch functional definition of DB (Heppe et al., 2021) based on consensus meetings, the findings from the previous phases, and the expertise of an additional group of Dutch experts. The outcomes of this study (second phase of the project) are expected to contribute to the international scientific understanding of DB, inform professionals engaged in defining populations, and provide practical insights for daily practice involving people with DB.
Methods
Study design
In this study, the Delphi methodology was used to investigate the consensus among experts-by-lived-experience and experts-by-working-experience on how to define DB in the Netherlands. The Delphi methodology is a widely used method to research consensus (Hasson et al., 2000; Nasa et al., 2021), also in the process of developing definitions (Metzelthin et al., 2022; Swedo et al., 2022). In a Delphi study, opinions of a panel of experts on a specific topic are anonymously aggregated by the use of questionnaires. The expert opinions are assessed in an iterative process over a series of rounds. After each round, the panel of experts receives controlled feedback of the group responses (Linstone & Turoff, 1975; Nasa et al., 2021). Based on this feedback, experts can revise their opinion in each round until consensus on a question is reached. Each opinion is weighted equally in this process (Nasa et al., 2021). Although there are no set standards for conducting a Delphi study, most studies include an expert panel of 30 to 50 experts, define consensus on a question when there is between 50% and 97% agreement, and consist of two to three rounds until consensus is reached on most or all questions (Nasa et al., 2021). Since a Delphi study can include participants from different geographical locations, this method is particularly well suited to research consensus of experts living throughout the country. Furthermore, the online aspect of the method is also an advantage, especially for people with DB, as online documents are often particularly accessible to them through the use of assistive tools (Bell et al., 2023).
Procedure
Experts for the panel were recruited between March and May 2021. Two groups of experts were recruited: experts-by-lived-experience and experts-by-working-experience. Although the number of participants varies widely within Delphi studies (Niederberger & Spranger, 2020), larger samples (e.g., more than 60 people) can be difficult to manage, and smaller samples (e.g., less than 15 people) can result in too few participants because of the high probability of dropout in Delphi studies (Avella, 2016; Hsu & Sandford, 2007). In our study, we aimed for a minimum of 40 participants (15 experts-by-lived-experience: five with congenital DB, five with acquired DB, and five with age-related DB, 25 experts-by-working-experience: five per care organisation providing DB-specific support in the Netherlands) and a maximum of 50 participants. Because of the heterogeneity of the population, a smaller sample could have resulted in underrepresentation of one of the subgroups or organisations, but a larger sample may not have been feasible because of the low prevalence of both populations of experts. Approval to conduct the study was provided by the Ethical Review Committee (ETC-SACB) of Deelkracht (https://www.deelkracht.nl/en/). All potential experts in the panel received an information letter and signed a consent form before the start of the study.
Experts-by-lived-experience were recruited by sending out information sheets and advertisements to potential eligible members of the Eye Foundation, a Dutch self-advocate organisation for people with vision impairment or DB (following Paramasivam et al., 2021 and Wittich et al., 2023). A list of potential eligible members of the Eye Foundation was prepared in advance, and these experts were subsequently invited to participate. During the recruitment and selection process, extra attention was paid to the aetiologies, biological sex, and age of the experts to ensure that the sample represented the highly heterogeneous population of people with DB. Eligibility of experts-by-lived-experience was based on: (1) having lived experience with DB or being a parent of a child with DB; (2) having gathered experiences of other people with lived experiences with DB; (3) being able to represent one subpopulation of DB (congenital DB, acquired DB, or age-related DB); (4) being able to understand Dutch or sign language of the Netherlands; (5) being able to use a computer or telephone; (6) being able to critically reflect on their own opinion and adjust it, if necessary. Our aim was to include the perspectives of experts-by-lived-experience themselves as much as possible, and to include family members only as experts in cases where the experts-by-lived-experience themselves are not able to participate, such as individuals with congenital DB.
Experts-by-working-experience were recruited by sending out an invitation letter directly to potential experts. To ensure national coverage, recruitment was conducted through five different care organisations providing DB-specific support in the Netherlands: Royal Kentalis, Royal Visio, Bartiméus, Kalorama, and GGMD. A list of potential eligible experts from these five organisations was prepared in advance based on the following criteria: (1) having extensive experience with working with people with DB; (2) being recognised as the go-to person for DB knowledge within their care organisation; (3) being able to understand Dutch or sign language of the Netherlands; (4) being able to use a computer or telephone; (5) being able to critically reflect on their own opinion and adjust it, if necessary. All listed potential experts-by-working-experience who were invited accepted the invitation to participate.
Participants (the panel)
A total of 20 experts-by-lived-experience and 26 experts-by-working-experience (e.g., care professional, educator, communication expert) provided informed written consent. One expert-by-lived-experience dropped out of the study prior to the start of the study (prior to receiving the questionnaire). This means that a total of 45 experts participated in the Delphi study. The experts-by-lived-experience were either family members of an individual with congenital DB (n = 7), had acquired DB (n = 8), or had age-related DB (n = 4). Fifty-three percent of the experts-by-lived-experience were female. The experts-by-working-experience all worked at one of the five care organisations in the Netherlands providing DB-specific care: Royal Kentalis (n = 6), Royal Visio (n = 6), Bartiméus (n = 5), Kalorama (n = 5), GGMD (n = 4). Sixty-two percent of the experts-by-working-experience had experience with supporting people with congenital DB, 88% of them with supporting people with acquired DB, and 54% of them with supporting people who have age-related DB. Ninety-two percent of the experts-by-working-experience were female. Of the total panel of 45 experts, all experts filled in the questionnaire in the first round and 44 experts in the second and third round.
Data collection
Prior to this study, in June 2020, a literature search was conducted to gather insights into how DB is defined in the scientific literature. This search resulted in several useful articles (Dammeyer, 2010; Larsen & Damen, 2014; Nelson & Bruce, 2016; Ravenscroft & Damen, 2019; Wittich et al., 2013). After thoroughly reading these articles, three researchers compiled a draft list of topics related to defining DB by highlighting relevant text and discussing it collaboratively. This draft list underwent three rounds of discussion involving the three Dutch researchers, two Dutch experts-by-working-experience, and one Dutch expert-by-lived-experience. The aim was to refine and finalise the list of topics to ensure its relevance and applicability to the Dutch context, as well as to reach consensus on the final list. The experts who participated in these discussions rounds, did not participate in the Delphi study. The final list of topics was used to develop the statements for the questionnaires of the Delphi study. These statements were formulated in Dutch, with translations into Sign Language of the Netherlands available upon request. For this article, all statements have been translated into English.
One questionnaire was developed, containing 30 multiple-choice statements. For each statement, participants were obligated to provide a written motivation for their chosen answer. Participants could not suggest new statements. Seventeen of the multiple-choice statements could be answered on a 5-point Likert-type scale of agreement (totally disagree, disagree, neutral, agree, totally agree). For the remaining 13 multiple-choice statements, participants were presented several answer options and instructed to select one or more. The questionnaire was available in two versions: one easy-read (B1 level [Common European Framework of Reference for Languages (CEFR), 2020]) and one with specialist jargon. Both versions were pilot-tested by two experts-by-lived-experience and one expert-by-working-experience. These experts did not participate in the Delphi study. This pilot testing provided an estimate of the time required to complete the questionnaire and offered feedback on whether any adjustments to the content, readability, or format were needed. No changes to the content, readability, or format of the questionnaire were necessary after the pilot. The final questionnaire was then distributed digitally to all 45 experts. The experts could choose which version to complete and were given 2 weeks to fill out the questionnaire in each round.
After each round, the experts received an anonymised summary of all participants’ answers and motivations. The summary consisted of the percentages of all answer options of the multiple-choice statements. This allowed participants to see which answer options were chosen most and less often. In addition, an anonymised summary of about three lines was provided for each answer option with the most frequently given motivations for each answer option. This allowed participants to read why participants had chosen a particular answer. Anonymity of participants was planned in the study design. Participants did not know who the other participants were and were explicitly asked not to talk with others, such as colleagues, about their participation in the study. All participants were assigned an anonymous number on registration. While analysing the results, only the anonymous number was visible to the researchers. Thus, during the study, researchers did not know who had given which answer.
Consensus on a statement was defined prior to the start of the study. If 80% or more of the experts agreed on a statement, consensus had been reached. Because of the large heterogeneity of the population, consensus on a statement was defined with a relatively high percentage, because it is important that a great majority of experts agrees on a topic. If consensus was reached on a statement, that statement was no longer included in the questionnaire in the next round. The questionnaire consisted of 30 statements in the first round, 16 statements in the second round, and 8 statements in the third round (see Tables 2 to 9 for an overview of the statements).
Data analysis
First, all 30 statements were analysed by IBM SPSS Statistics (Version 26), using descriptive statistics. For the 17 multiple-choice statements on a 5-point Likert-type scale of agreement, motivations for response options ‘(dis)agree’ and ‘totally (dis)agree’ were aggregated, resulting in three categories: (totally) agree, neutral, and (totally) disagree. Due to the small sample size, the Fisher’s Exact Test (Field, 2013; Kim, 2017) was used to identify potential differences between the experts-by-lived-experience and the experts-by-working-experience on the categories ‘(totally) agree’ and ‘(totally) disagree’. For these analyses, responses to the answer option ‘neutral’ were not taken into consideration, as only very few participants selected this response option. A difference was considered significant at p ⩽ .05.
Second, the motivations provided by the experts for each answer option of the statements were analysed using Microsoft Excel (Version 2302) by two researchers. Open coding (Glaser et al., 1968) was used, with each motivation systematically coded one-by-one by the researchers. To ensure consistency, motivations for several statements were independently analysed by both researchers to verify code alignment. Regular meetings were held between researchers to resolve discrepancies in coding. Subsequently, all codes were thoroughly reviewed and categorised by the same researchers based on mutual agreement. Final categorisations were validated by a third independent researcher. The categorisations of each motivation were summarised. Only motivations from the final round for each statement were analysed. Motivations from experts-by-lived-experience and the experts-by-working-experience were separately coded, categorised, and summarised when a significant difference was found between the two groups.
Results
Overall, consensus was reached on 24 of the 30 multiple-choice statements in the Delphi study. As can be seen in Table 1, consensus was reached on all statements from Topics 1, 3, 5, 7, and 8. On Topic 2, ‘functioning of people with DB’, consensus was reached on two out of four statements; on Topic 4, ‘functional definition of DB and terminology’, consensus was reached on two out of three statements; and on Topic 6, ‘Sub-target group demarcation’, consensus was reached on one out of four statements. For only one statement of the 17 Likert-type scale statements, a significant difference was found between the answers of experts-by-lived-experience and experts-by-working-experience (see Topic 2 below).
Overview of the topics in the questionnaire.
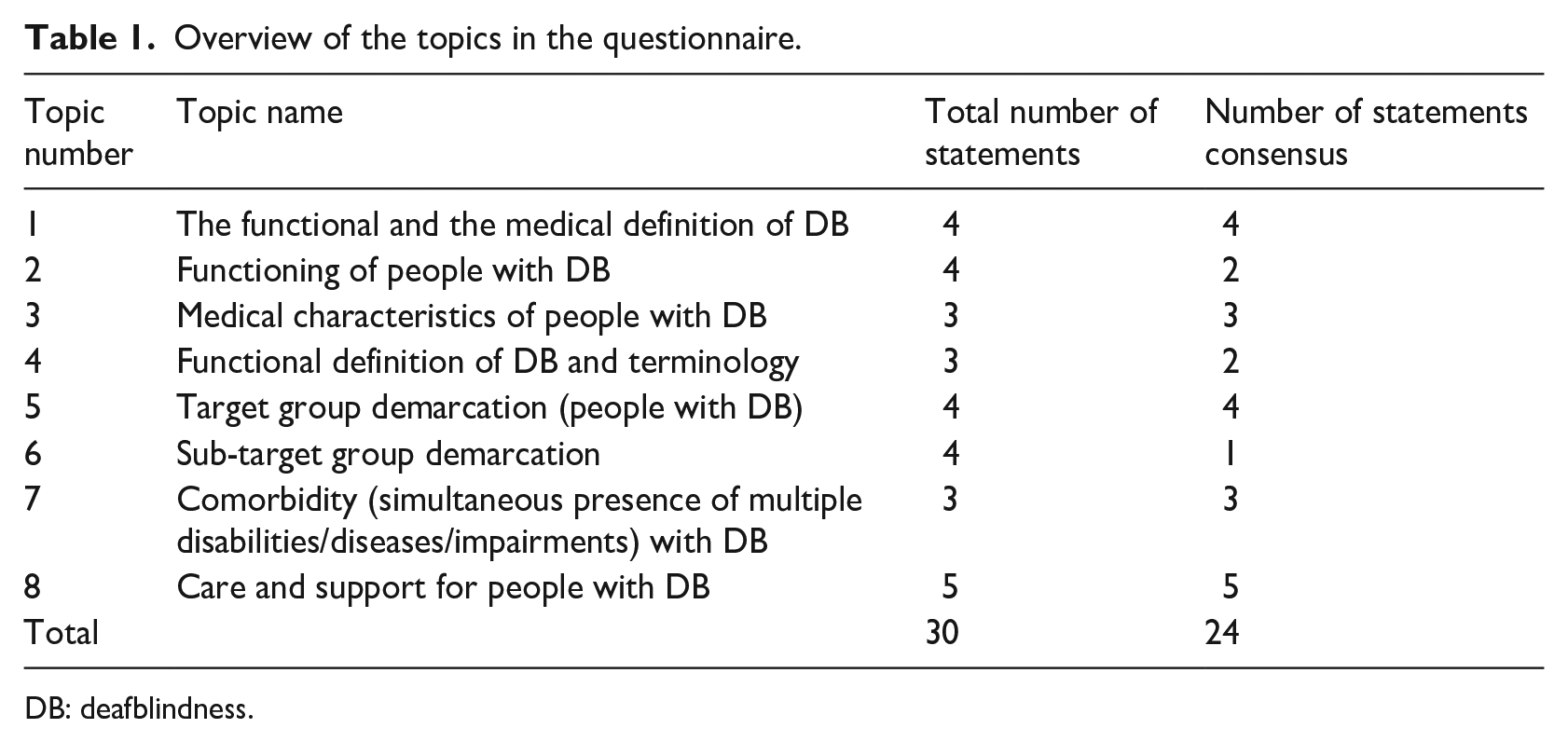
DB: deafblindness.
Topic 1 – the functional and the medical definition of DB
As shown in Table 2, the experts reached consensus on the statement that a new medical definition of DB is needed (91%). The most frequently mentioned reason for this was that this new medical definition should take into account that visual and auditory impairments affect each other in people with DB and that the boundaries of the criteria should, therefore, be expanded. The experts also reached consensus on that both the medical and functional definition should be used when determining DB (87%). The most frequently mentioned reason for this was that using both definitions provides a better description of DB than using only one. Consensus was also reached on that a functional definition would help with ‘providing the right kind of support to people with DB’ (96%) and ‘identifying DB’ (80%), and that a medical definition would help with ‘determining DB’ (87%).
Results of Topic 1: the functional and the medical definition of DB.
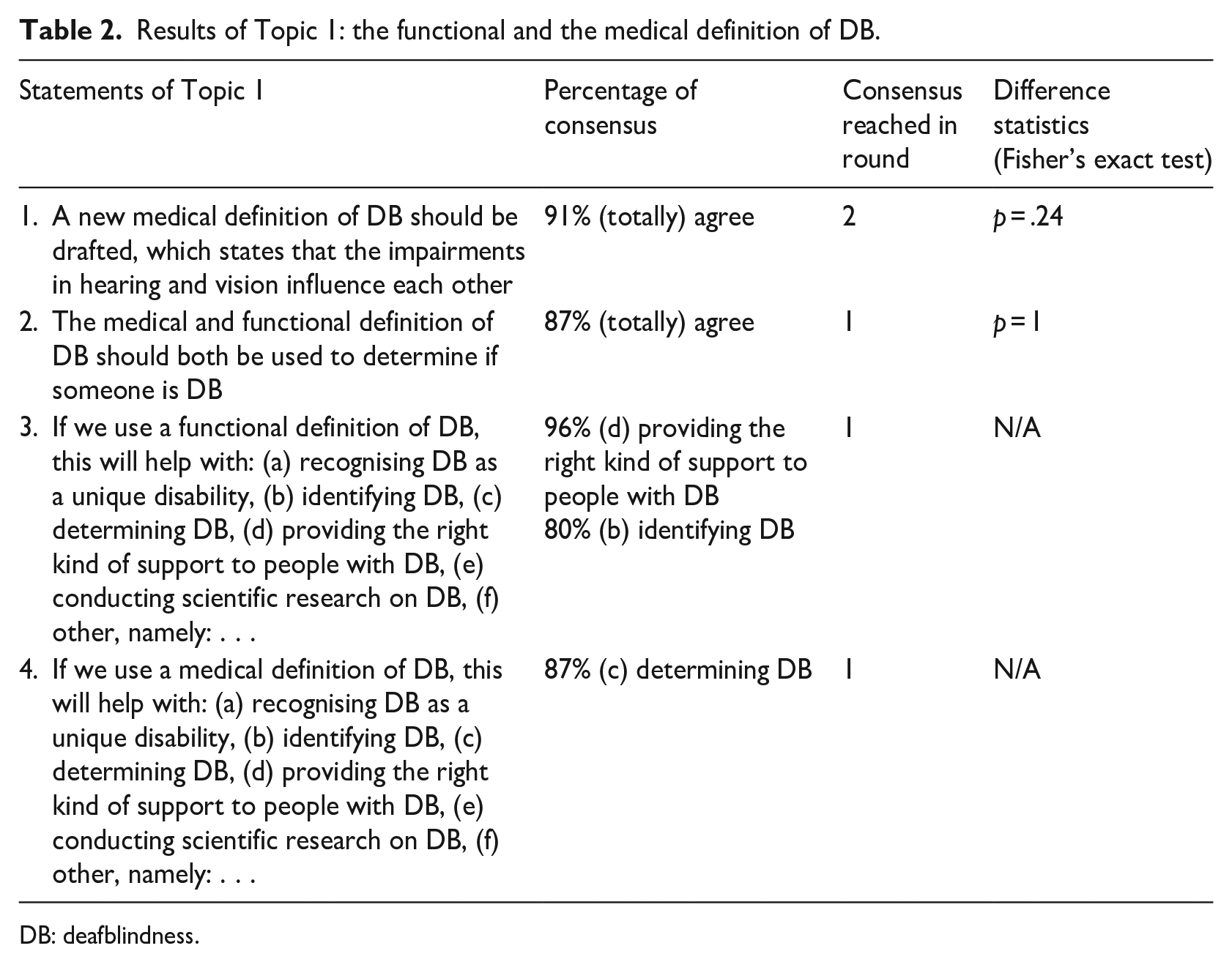
DB: deafblindness.
Topic 2 – functioning of people with DB
The experts reached consensus on that what a person with DB can and cannot do in daily life depends on the following aspects: personal characteristics (96%), help from the social environment (87%), adaptations in the environment (82%), and acceptance in society (80%). As shown in Table 3, the experts also reached consensus on that DB affects multiple life domains and limits one’s abilities in the areas of: communication (98%), mobility (96%), orientation (93%), access to information (91%), and social life (91%). The experts did not reach consensus on the statement that for a person with DB, touch, smell and taste, among others (other senses) are the most important sources of sensory information, even if a person still has residual hearing or vision (55%). For this statement, the responses of experts-by-lived-experience and experts-by-working-experience were significantly different (Fisher’s exact test, p = .02). Most experts-by-lived-experience agreed with this statement (82%), compared to less than half of the experts-by-working-experience (44%). The most frequently given motivation by experts-by-working-experience was that it is impossible to determine which senses are the ‘most important’ because of the individual differences between people with DB. The experts also did not reach consensus on the statement that a person with congenital DB always falls behind in all areas. Nevertheless, a majority of the experts disagreed with this statement (70%). This was most frequently explained by the motivation that there are many differences between people with congenital DB.
Results of Topic 2: functioning of people with DB.
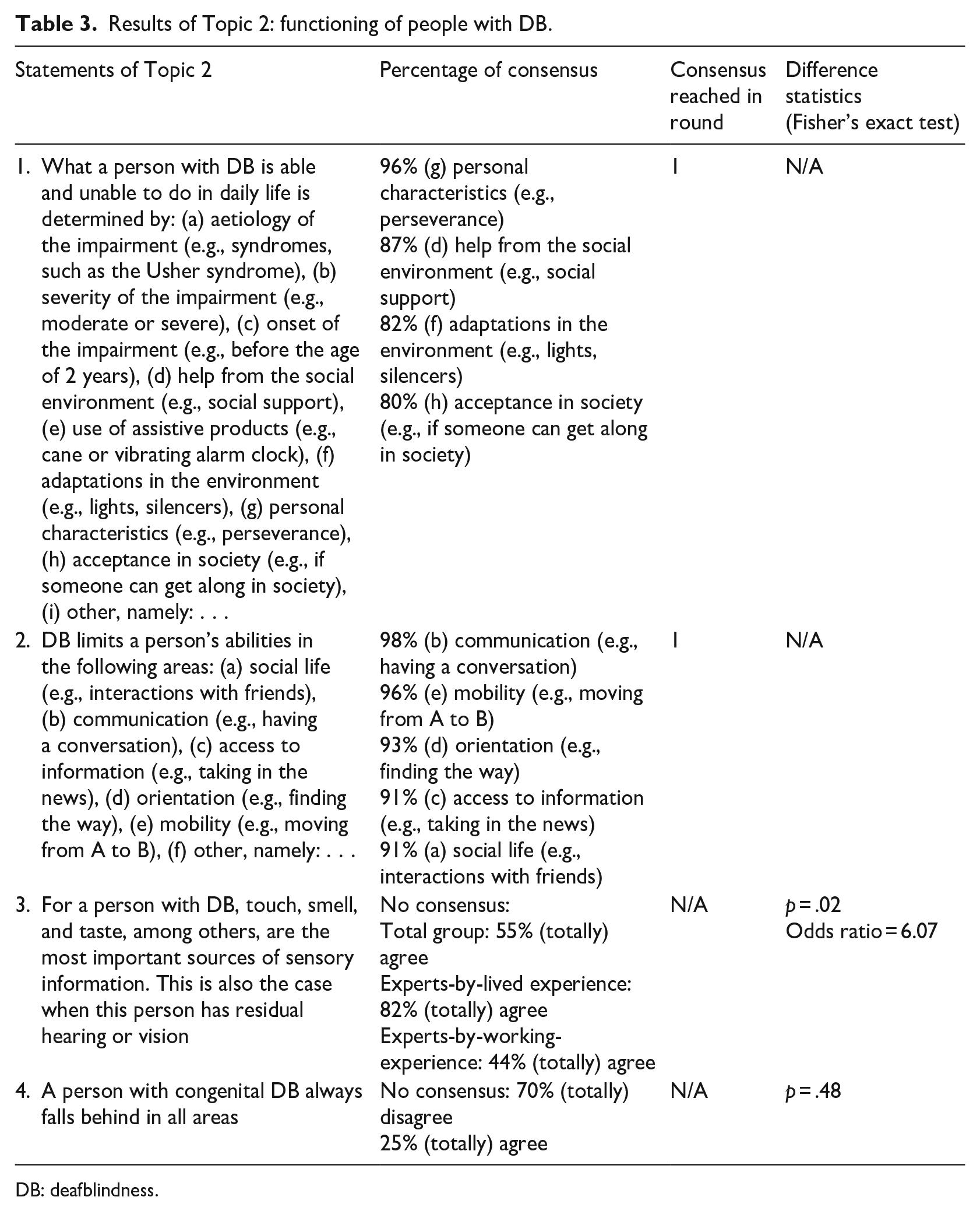
DB: deafblindness.
Topic 3 – medical characteristics of people with DB
As shown in Table 4, consensus was reached by the experts on the statement that DB cannot be described solely on the basis of how much a person still hears and sees (based on the results of medical tests; 82%). The most frequently given motivation was that it is important to also include the impact that DB has on daily functioning when describing DB. The experts also reached consensus on that one of the characteristics of DB is that the impairments in vision and hearing are not 100% solvable (84%). Moreover, the experts reached consensus on that it is impossible to determine exactly how much a person with DB still hears or sees (based on the results of medical tests; 80%). They mentioned that medical tests are not 100% reliable in people with DB, that scores can change from day to day, and additional factors such as fatigue, stress, and background noises affect the results on these tests.
Results of Topic 3: medical characteristics of people with DB.
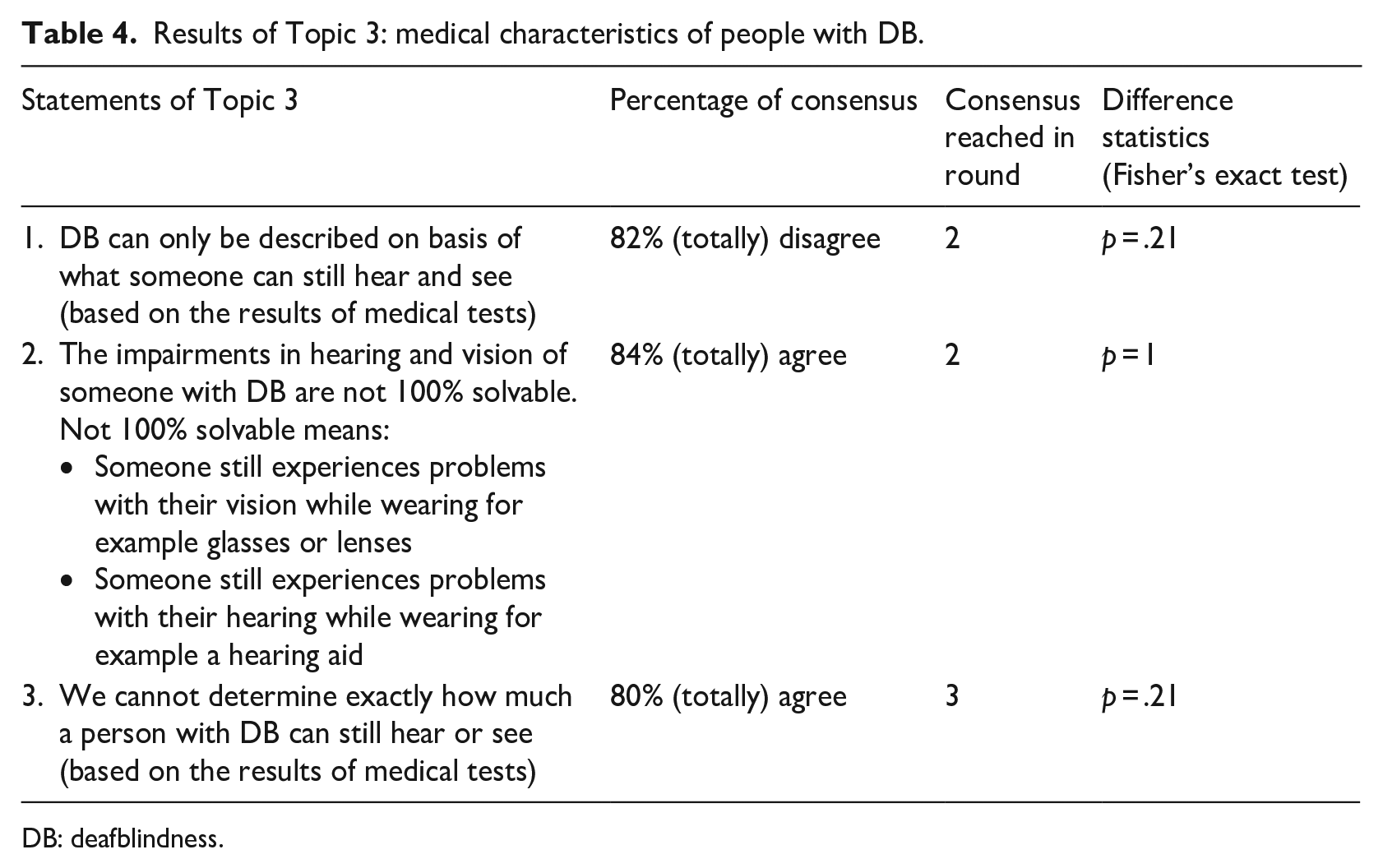
DB: deafblindness.
Topic 4 – functional definition of DB and terminology
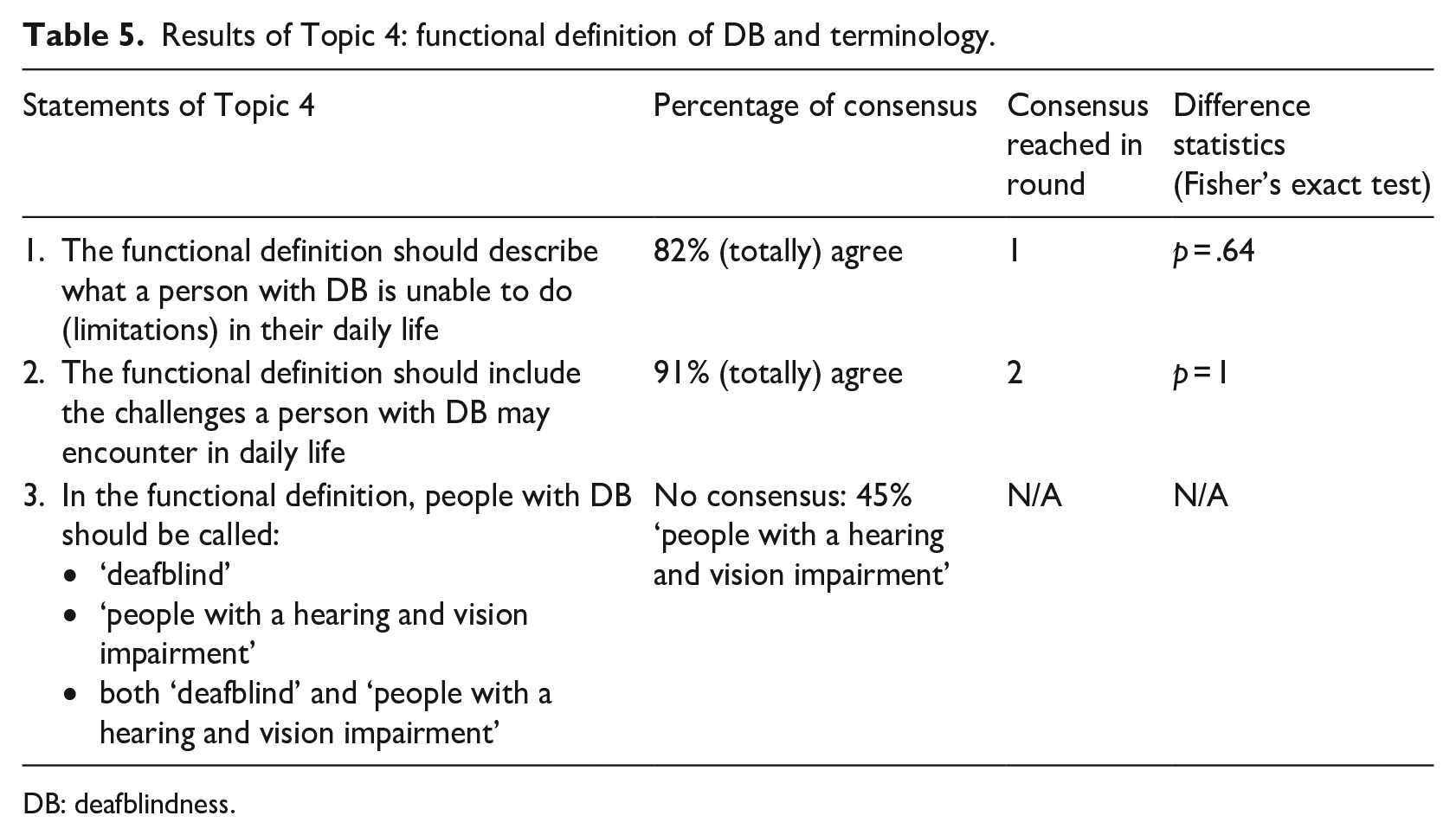
As shown in Table 5, the experts reached consensus on that the functional definition should describe the limitations (82%) and challenges (91%) that people with DB experience in everyday life. The most frequently given motivation was that such descriptions will help people apply for support and thus ensure better care. The experts did not reach consensus on what terminology should be used to describe people with DB in the functional definition. Less than half of the experts agreed on using the term ‘people with a hearing and vision impairment’ (45%).
Results of Topic 4: functional definition of DB and terminology.
DB: deafblindness.
Topic 5 – target group demarcation (people with DB)
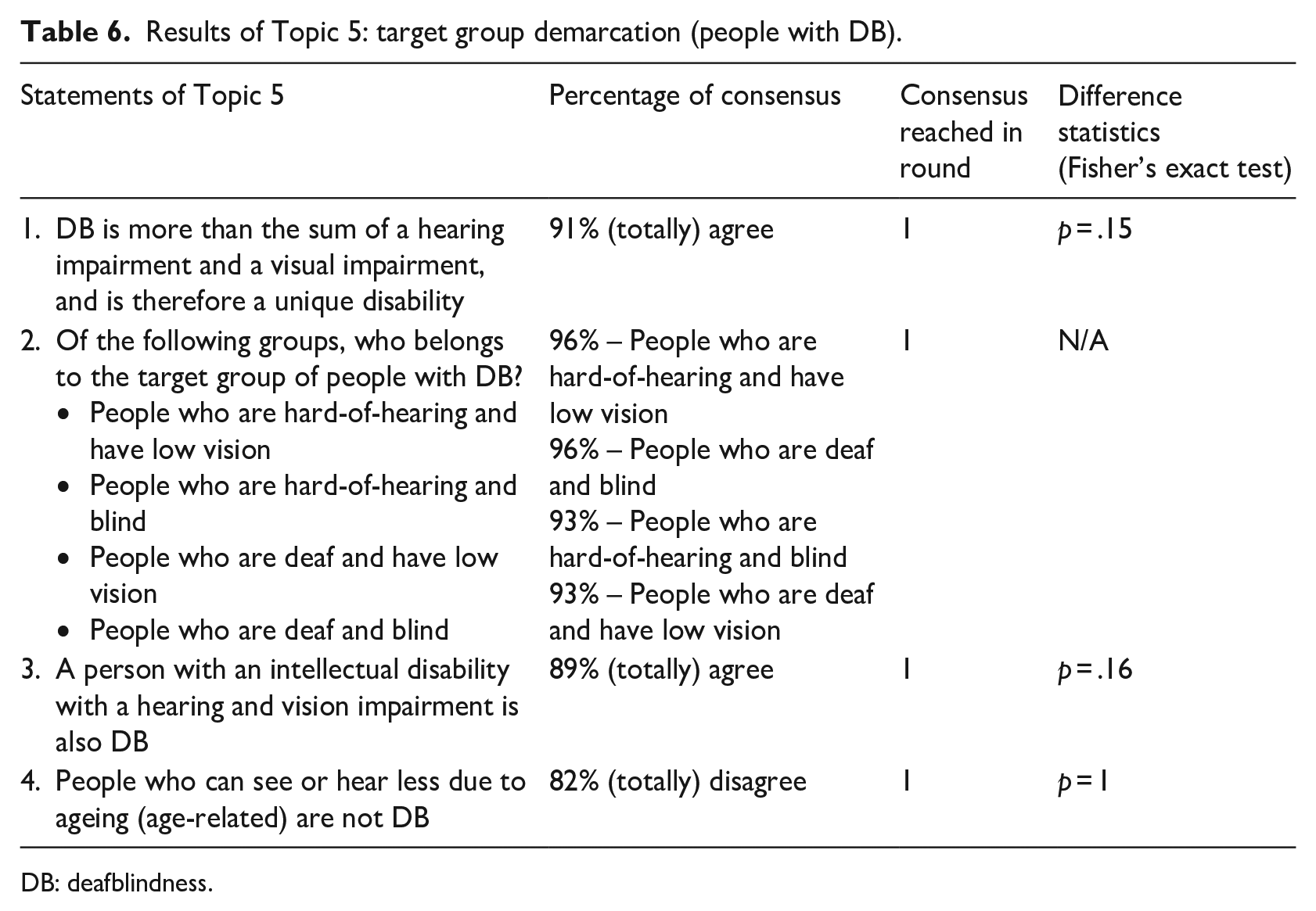
The experts reached consensus on the statement that DB is a unique disability (91%). The most frequently given motivation was that with DB, the vision and hearing impairment are less able to compensate for each other and, therefore, it is a unique disability. Experts also reached consensus on that all combinations of being deaf or hard-of-hearing and being blind or having low vision belong to the population of DB (range 93%–96%). Experts also reached consensus on that people with an intellectual disability with a vision and hearing impairment and people who can see or hear less due to ageing (age-related DB) belong to the DB population (89% and 82%, respectively; see Table 6). The most provided motivation for including these subgroups is that people in all these groups face similar challenges in daily functioning due to DB. It was also stated that an intellectual disability and DB are two distinct disabilities, meaning that people with an intellectual disability may or may not have DB, and vice versa (see also Topic 7 below).
Results of Topic 5: target group demarcation (people with DB).
DB: deafblindness.
Topic 6 – sub-target group demarcation
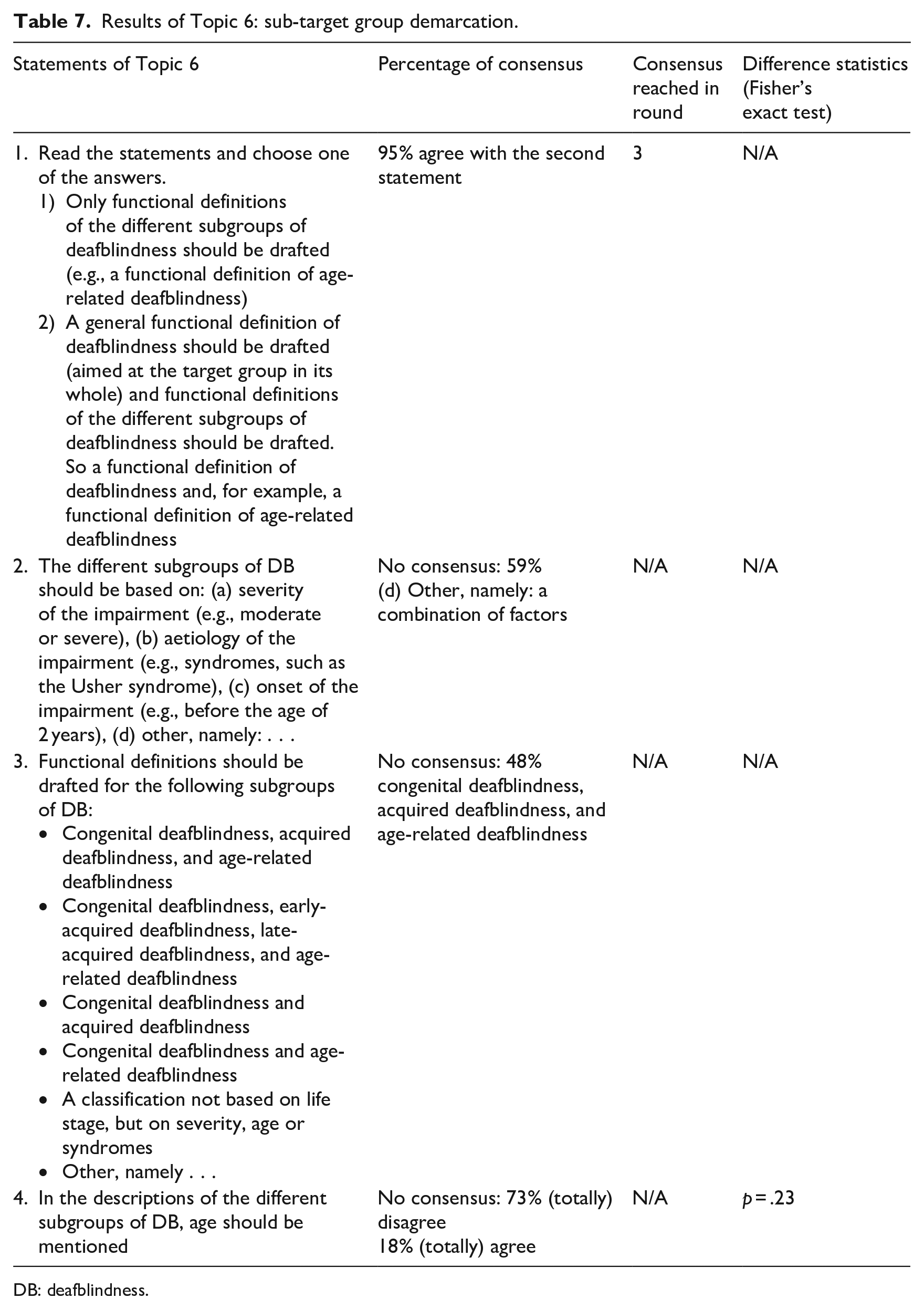
The experts reached consensus on that there should be one general functional definition of DB and functional definitions of the subgroups of DB (95%). The most frequently given motivation was that this best reflects the diversity of the target population. The experts did not reach consensus on what characteristics (e.g., severity, aetiology, onset of the impairment) should distinguish the subgroups of DB. The experts also did not reach consensus on for which subgroups of DB (e.g., congenital, acquired, age-related DB) functional definitions should be established. Also, no consensus was reached on whether the functional definitions of the subgroups should include a specific age. However, most experts did not want to include age in the functional definitions of the subgroups of DB (73%; see Table 7).
Results of Topic 6: sub-target group demarcation.
DB: deafblindness.
Topic 7 – comorbidity
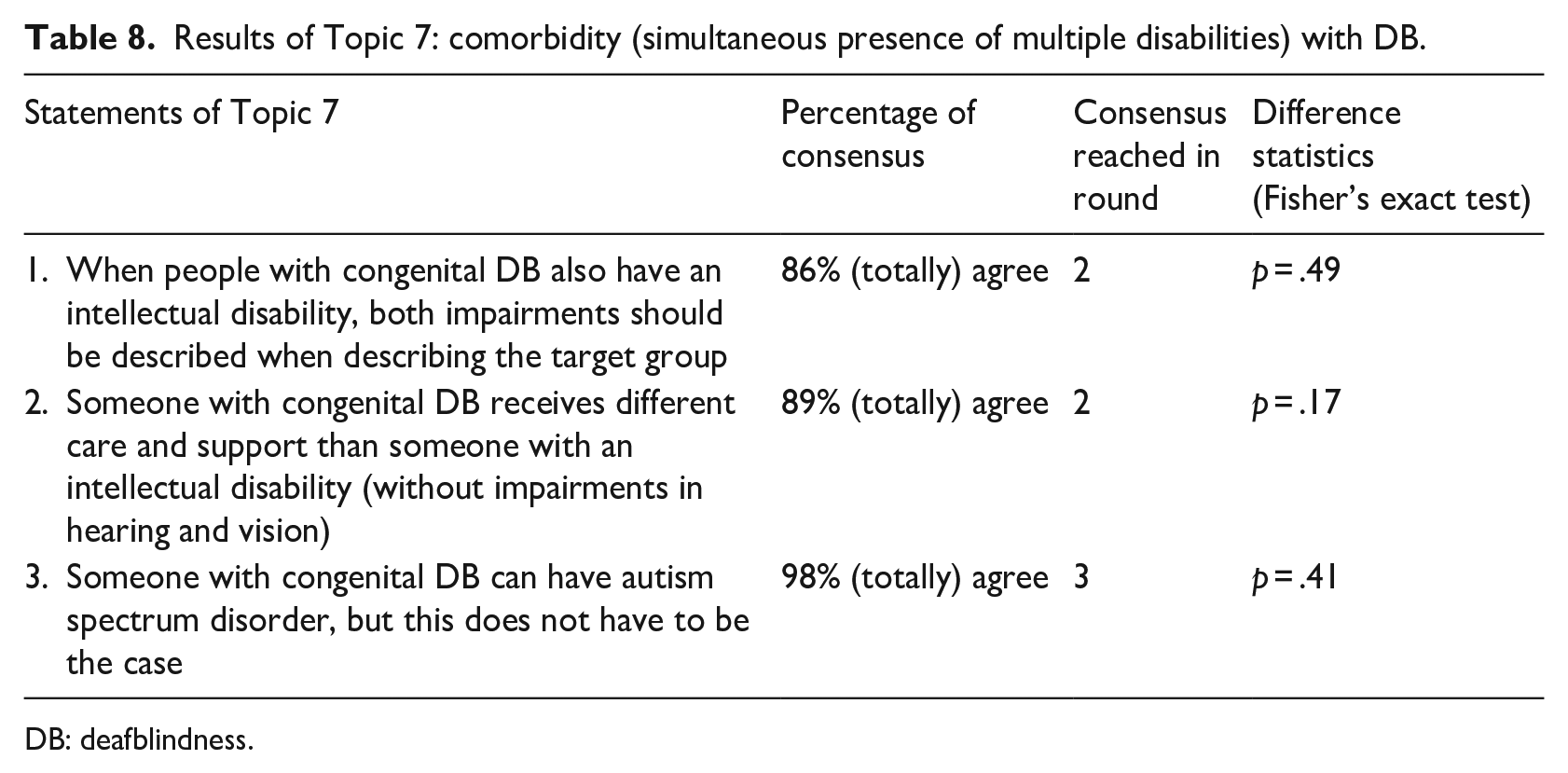
As shown in Table 8, the experts reached consensus on the statement that people with congenital DB can also have an intellectual disability and, therefore, both disabilities should be described separately when describing this subgroup (86%). The most commonly given motivation was that DB and an intellectual disability are two distinct disabilities. In addition, the experts reached consensus on that people with congenital DB and an intellectual disability and those with an intellectual disability and no vision impairment and/or hearing loss, require different types of support (89%). The most commonly given motivation was that DB and an intellectual disability are two distinct disabilities. The experts also reached consensus on that people with congenital DB can have autism spectrum disorder, but that is not always the case (98%). Also with this statement, experts indicated that these are two distinct conditions.
Results of Topic 7: comorbidity (simultaneous presence of multiple disabilities) with DB.
DB: deafblindness.
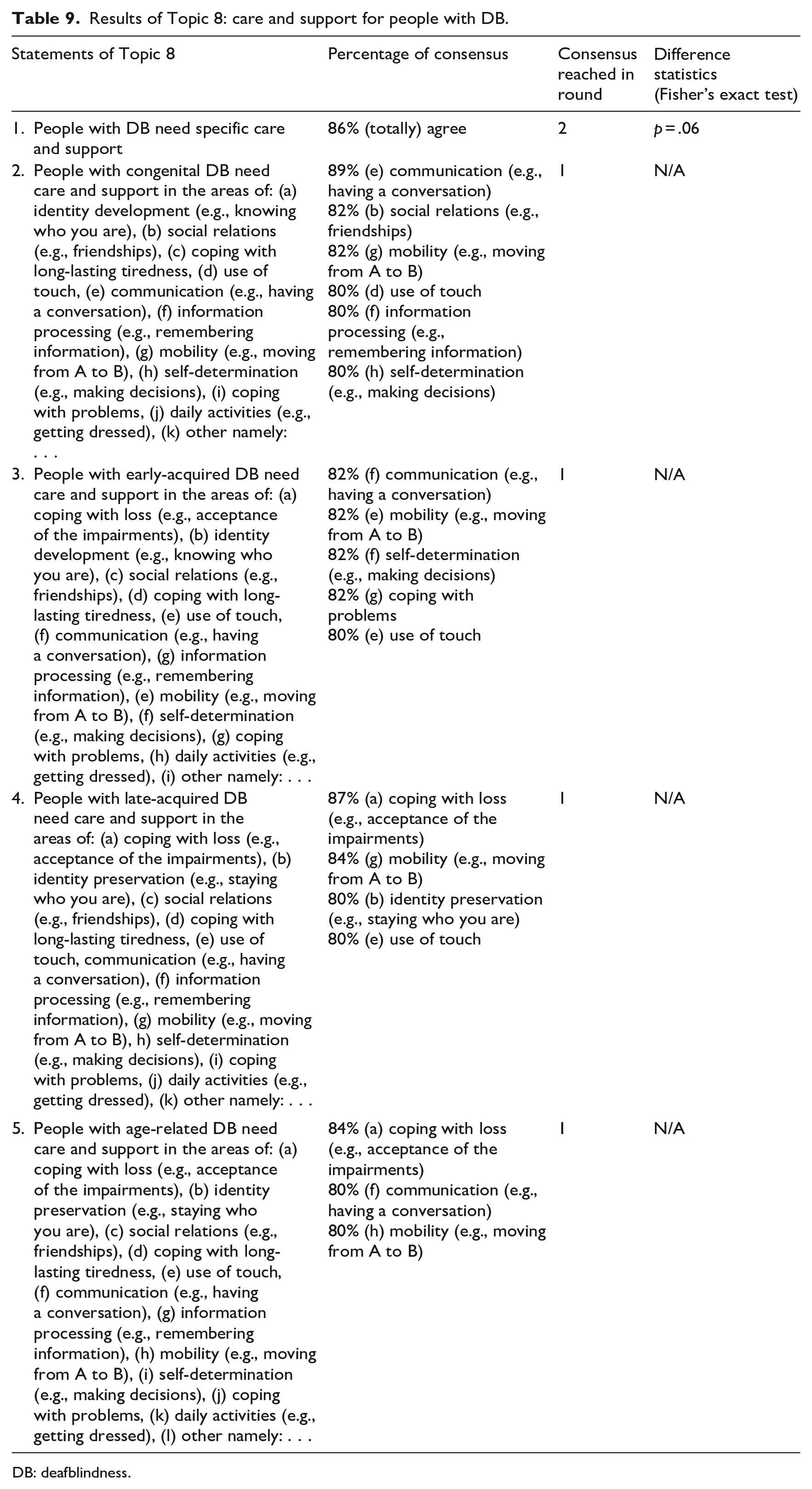
Topic 8 – care and support for people with DB
The experts reached consensus on that people with DB need specific care and support (DB-specific support; 86%). The most frequently given motivation was that care and support for people with DB should always be adapted to DB. The experts also reached consensus on that people with congenital DB need support in the following areas: communication (89%), social relations (82%), mobility (82%), use of touch (80%), information processing (80%), and self-determination (80%). For people with early-acquired DB, there was consensus for the following areas: communication (82%), mobility (82%), self-determination (82%), coping (82%), and use of touch (80%). For people with late-acquired DB, consensus was reached on the following areas: coping with loss (87%), mobility (84%), identity preservation (80%), and use of touch (80%). For people with age-related DB, there was consensus for the following areas: coping with loss (84%), communication (80%), and mobility (80%; see Table 9).
Results of Topic 8: care and support for people with DB.
DB: deafblindness.
Discussion
Main findings
This study investigated the consensus among experts on topics related to defining the functional definition of DB in the Netherlands. The variability in definitions and terminology surrounding DB has been a long-standing issue, as indicated by previous research (Larsen & Damen, 2014; Minhas et al., 2022; Wittich et al., 2013). A Delphi study was conducted with a panel of 45 Dutch experts, consisting of experts-with-lived-experience and experts-with-working-experience.
One key issue addressed in this study is the distinction between medical and functional definitions of DB. The consensus among experts in this study regarding the factors that influence the daily functioning of people with DB, highlights the limitations of relying solely on medical definitions for defining DB. Recognising that a functional definition complements the medical perspective aligns with the principles of the ICF model, which emphasises the importance of considering daily functioning and participation in society in understanding a disability (WHO, 2001). Various studies have shown the effective application of the ICF model to DB (Cantin et al., 2022; Jaiswal et al., 2019, 2024; Wittich, Dumassais, Jaiswal, et al., 2024; Wittich, Dumassais, Prain, et al., 2024). Therefore, adopting an ICF-based approach that integrates a functional definition alongside a medical definition is essential for accurately defining DB and determining who requires deafblind-specific support.
The study also explored the demarcation of the DB population and its subgroups. The results revealed a consensus on the need for both a general functional definition and specific functional definitions tailored to subgroups within DB. However, no consensus was reached on which specific subgroups should be included. Nearly half of the experts supported distinguishing three subgroups: congenital, acquired, and age-related. Different care and support needs were identified for these subgroups; for example, the importance of touch was particularly highlighted for people with congenital and acquired DB, while it was less emphasised for people with age-related DB. This finding indicates the necessity of distinguishing between specific subgroups within DB and underscores the need for a functional definition tailored to the Dutch context. For example, the Nordic definition primarily outlines areas of focus for the broader DB population without addressing subgroup-specific care and support needs. Furthermore, the results showed no consensus on whether age should be part of the functional definitions for subgroups, though most disagreed with its inclusion. In conclusion, while the need for subgroup functional definitions is acknowledged, further discussion was needed to refine them, which was addressed in the third phase of the project based on consensus meetings.
Another notable finding was the minimal divergence between the opinions of experts-with-lived-experience and experts-with-working-experience. Only on one statement did these groups differ significantly. The fact that both groups largely agreed suggests they can collaborate effectively in establishing a Dutch functional definition together.
Strengths and limitations
The Delphi methodology used in this study facilitated the aggregation of expert opinions and reaching consensus. The inclusion of a diverse panel of experts-by-lived-experience alongside experts-by-working-experience ensured a comprehensive understanding of the lived realities and professional perspectives surrounding DB. The fact that there was no consensus in the first round on more than half of the topics drawn from the literature showed the need to perform this study. Furthermore, the consensus among Dutch experts on the need to include specific functional definitions for subgroups in the Dutch functional definition of DB underscores the necessity for a definition tailored to the Dutch context.
However, several limitations to the study should be noted. First, individuals with DB who have limited communicative and cognitive abilities were not included in the panel, as participation in the Delphi process required proficiency in Dutch or sign language of the Netherlands and the capability to use a computer or telephone. However, family members of individuals with DB who have low communicative and cognitive abilities were included in the panel as representatives. In addition, the sample included a diverse range of aetiologies, biological sexes, and ages to represent the highly heterogeneous population of people with DB. Nevertheless, obtaining an ideal representation of the Dutch community of people with DB remains challenging, as precise data on the distribution of subgroups (congenital DB, acquired DB, age-related DB) is unavailable. This makes it difficult to define the optimal composition of an experts panel in terms of representativeness.
Furthermore, we did not balance positively and negatively formulated statements in the questionnaire, which may have unintentionally directed participants’ responses. However, the anonymity of the questionnaire likely encouraged participants to provide less socially desirable answers. At the same time, the anonymity of the questionnaire leads to the third limitation of our study: participants could not be contacted in case of uncertainties about the motivations they provided for their choices. This could have led to some misinterpretations by the researchers during the coding procedure. Moreover, coding reliability was not formally assessed, as the researchers divided the data for analysis. Nonetheless, alignment was ensured through joint analysis of several statements, ongoing discussions, and mutual agreement on final categories.
In addition, it was not feasible to check whether interpretations of the questionnaire version containing jargon and the easy-read version were exactly the same, because participants filled out one version. Although the phrasing was done very carefully, it is possible that the two versions yielded slightly different interpretations for some statements. Finally, the specific context of the Netherlands may limit the generalisability of the results to other countries, especially those with different healthcare systems and resources.
Implications for practice
The results from this study were used to develop a Dutch functional definition of DB (Heppe et al., 2021). The next step is to implement this functional definition in the eligibility criteria for healthcare, education, and support services in the Netherlands, so that professionals and service providers can use both the medical and functional definition when assessing eligibility for deafblind-specific support. Our research team is currently developing a tool to assess problems in functioning of people with DB and their support needs, which will aid in the implementation of the Dutch functional definition.
Furthermore, the results of this study demonstrate that tailored care and support (deafblind-specific support) should be provided to people with DB, taking into account their unique needs and challenges across various domains of functioning. This is in line with the importance of specialised early intervention described by Anthony (2016) for infants and toddlers with DB, as this prevents unnecessary developmental delays and social isolation. To ensure that people with DB in the Netherlands who meet the Dutch functional definition receive deafblind-specific support and get this support reimbursed, the Dutch functional definition should be integrated in policies and guidelines of institutions, insurance companies, and branch organisations. Integrating the Dutch functional definition of DB into policies, assessments, and interventions enables better recognition and identification of people with DB, ultimately leading to better care and support for this group. By not only focussing on limitations in bodily functions and structures but also on problems in daily functioning and participation in society, the person is considered as a whole beyond their impaired vision and hearing.
Future research
Future research should test the validity of the newly developed Dutch functional definition of DB and assess the effectiveness of its implementation in clinical practice. It could be examined whether people who meet the criteria of the functional definition actually benefit from deafblind-specific support and care. This would give us information about the predictive validity of using the Dutch functional definition in practice.
In addition, comparative studies across different countries could provide insight into cultural differences in defining and supporting people with DB, caused by differences in socioeconomic factors, healthcare systems, and policy frameworks. By examining how DB is understood and addressed in diverse cultural contexts, researchers can identify best practices and areas for improvement in the provision of care and support for people with DB worldwide.
Moreover, future research could compare the Dutch functional definition of DB with the recent efforts in developing ICF core sets for DB (Jaiswal et al., 2024; Wittich, Dumassais, Jaiswal, et al., 2024; Wittich, Dumassais, Prain, et al., 2024). Experts-with-lived-experience as well as experts-with-working-experience were involved in the development of the ICF core sets. A comparison could identify overlaps and gaps between the Dutch functional definition of DB and the ICF core sets for DB. This will allow enrichment of both the functional definition and the ICF core sets, leading to a more comprehensive understanding of DB.
Conclusion
This Delphi study has established consensus among the foremost experts on DB in the Netherlands regarding topics related to defining the functional definition of DB in the Netherlands. By incorporating insights from both experts-by-lived-experience and experts-by-working-experience, this study has achieved a uniquely comprehensive understanding of how to define DB and its profound impact on individuals’ lives. Future steps involve implementing the Dutch functional definition of DB to facilitate access to deafblind-specific support.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by ZonMw’s program, Expertisefunctie Zintuiglijk Gehandicapten, Deelkracht (Grant number 637003001).