
Abstract
The purpose of this study was to investigate accuracy and bias effects in partners' reports and perceptions of diet- and exercise-related social control in conjunction with their relationship satisfaction. Actor–partner interdependence mediation models (APIMeM) were used to examine the reports of diet- and exercise-related social control in 192 couples. In line with the accuracy and bias framework, we found that couples are accurate and biased with regard to their social control attempts and that accuracy and bias were associated with relationship satisfaction for positive social control. Individuals also reported greater relationship satisfaction when they reported using less negative social control and when they perceived more positive social control from their partners. These findings provide corroboration for self-reports of social influence in close relationships while simultaneously demonstrating bias in perceptions of partners’ social control and highlighting concurrent associations with people’s relationship satisfaction.
Close relationships are integral to people’s health. Beyond the beneficial effects of relational involvement (House, Landis, & Umberson, 1988), couples’ interactions and relationship quality have been linked to their health and well-being (Kiecolt-Glaser & Newton, 2001; Robles & Kiecolt-Glaser, 2003). Mutual influence is prevalent in most relationships (Thibaut & Kelley, 1959) and is exhibited, for example, through couples’ use of health-related social control (Lewis, Butterfield, Darbes, & Johnson-Brooks, 2004). This study focuses on diet- and exercise-related social control specifically, as diet and exercise are adaptable lifestyle factors that are strongly related to being overweight or obese (Miller, Koceja, & Hamilton, 1997), the incidence of which has reached a staggering proportion of 69% of U.S. adults (Centers for Disease Control and Prevention, 2013; www.cdc.gov).
Social control is an ongoing health communication process (Lewis & Butterfield, 2007) that is often conceptualized as positive (e.g., praise and encouragement) or negative (e.g., guilt and withdrawal). Although researchers typically examine partners’ health-related social control in conjunction with their health behaviors (e.g., Butterfield & Lewis, 2002), partners’ perceptions of positive or negative social control can be highly consequential to their relationship quality as well. This investigation employs the social control framework in conjunction with the accuracy and bias framework (Kenny & Acitelli, 2001) to examine couples’ perceptual accuracy with regard to diet- and exercise-related social control in their relationships. Couples’ social control will also be examined in association with their relationship satisfaction.
Diet- and exercise-related influence in relationships
Interdependence and mutual influence are fundamental characteristics of relationships (Thibaut & Kelley, 1959). Indeed, couples’ relational experiences and outcomes are often intertwined such that one partner’s positive experience might become rewarding for the other partner (Rusbult & Buunk, 1993). For example, one partner’s healthy diet and exercise behaviors might be a positive force for the other partner. Conversely, one partner’s weight struggles might be challenging for the other partner. In this study, we draw upon the social control framework to examine how couples communicate health-enhancing influence messages to each other.
Research indicates that people consider their partners to positively influence their diet and exercise habits (Markey, Markey, & Gray, 2007). Further, when couples communicate health-enhancing social control, it likely reinforces their desire to maintain each other’s health and, consequently, their relationship. Individuals who wish to sustain their relationships often behave in ways that reflect broader interaction goals and promote their relationship satisfaction (Rusbult & Buunk, 1993). In other words, individuals who want their partners to adopt healthier behaviors typically engage in positive social control rather than negative social control (Butterfield & Lewis, 2002; Lewis & Butterfield, 2007; Markey et al., 2007), which serves to protect their relationship quality.
According to Butterfield and Lewis (2002), communication of positive social control includes partners’ expression of positive emotions, suggestions, and praise, whereas partners’ communication of negative social control involves guilt, withdrawal, and negative emotions. For instance, people might enact positive social control by expressing pride in their partners’ exercise accomplishments, thereby reflecting their encouragement and relational regard. These positive social control strategies reflect interpersonal influence that is aimed at generating the desired partner behavior through positive affect and constructive recommendations. Such positive (Gottman, 1982, 1994) and confirming communication (Liang, Phillipson, & Lee, 1966) should benefit the relationship. Alternatively, people might enact negative social control by communicating their disappointment in their partners’ lack of diet-related efforts, which signals frustration and relational distress. These negative social control strategies reflect interpersonal influence that is aimed at generating the desired partner behavior through negative affect and disengagement, and such negative (Gottman, 1982, 1994) and disconfirming communication (Weger, 2005) might be harmful to the relationship. Much of the research on social control suggests that positive social control should be more effective in influencing partners to be healthier (Lewis & Butterfield, 2007) and that negative social control is less effective, or potentially ineffective, when it comes to partners’ healthy behavior adoption (Tucker & Anders, 2001). The research on social control perceptions, particularly with regard to relationship quality is limited, however.
Health influence perceptions and relationship quality
Within the context of weight management conversations in close relationships, partners’ perceptions of message effectiveness are informed by their interpretations of distinct message characteristics. Indeed, Dailey, Romo, and Thompson (2011) found that people’s satisfaction with weight management conversations is positively related to their perception of acceptance messages (e.g., warmth, care, and positivity) from the partner. When both partners perceived low-challenge messages (e.g., push to be healthier) from each other, they were the most satisfied with the weight management conversation (and vice versa). Although these findings are only indicative of satisfaction with the conversation, and not satisfaction with the relationship, they reinforce the importance of partner perceptions and also highlight the potential differences among message types within weight management conversations.
With regard to weight-related communication and relationship quality specifically, people who perceive more positive health influence from their partners also report being in more loving, understanding, and harmonious relationships (Markey et al., 2007). In contrast, research indicates that women whose partners told them to lose weight and men whose partners told them to gain weight report significantly lower relationship satisfaction compared to those whose partners did not send such messages (Sheets & Ajmere, 2005). Further evidence indicates that individuals perceive their relationships to be less equitable as their partners' use of unilateral social control increases in frequency (Butterfield & Lewis, 2002). Together, these findings highlight the importance of understanding couples’ perceptions of weight management communication in relationships and their corresponding relationship quality.
Accuracy and bias perceptions
Accuracy and bias effects in close relationships are examined using a conceptual model developed by Kenny and Acitelli (2001). In the context of the current study, examining accuracy and bias effects involves assessing both partners’ self-appraisals for their use of positive and negative social control and each individual’s appraisals of their partners’ use of positive and negative social control. This model has identified accuracy and bias effects for closeness, caring, equity, and sex in married relationships (Kenny & Acitelli, 2001); feedback from romantic partners (Lackenbauer, Campbell, Rubin, Fletcher, & Troister, 2010); conflict styles in newlywed relationships (Segrin, Hanzal, & Domschke, 2009); and spouses’ preferences for lifesaving medical treatments (Lemay, Pruchno, & Field, 2006). Whereas social control research has examined individuals’ use of and partners’ perceptions of social control in the context of health (Butterfield & Lewis, 2002), it does not specifically identify the potential correspondence between partners’ use of and perceptions of social control. We extend the existing research by examining this potential correspondence in conjunction with partners’ relationship quality.
Accuracy effects are evident when one partner’s self-perceptions are predictive of the other partner’s partner perception. In this study, accuracy effects are illustrated by actors’ self-reported social control enactment predicting partners’ reported perceptions of the actors’ social control enactment (and vice versa; see the dashed lines in Figure 1). Accuracy effects reflect relational understanding (e.g., actors’ perceptions of partners’ behavior match partners’ accounts of their own behavior). In contrast, bias effects occur when people’s self-perceptions are predictive of their partner perceptions. In this study, bias effects are illustrated by actors’ self-reported social control enactment predicting their reported perceptions of their partners’ social control enactment (and vice versa; see the double lines in Figure 1). Bias effects signal assimilation in perceptions of relational partners (e.g., actors’ perceptions of their own behavior correspond with their perceptions of their partner’s behavior). It should be noted that we operationalize the concepts of “accuracy” and “bias” as others have in the research literature, by collecting self- and partner reports from both members of the dyad (e.g., Lackenbauer et al., 2010; Reysen, Hall, & Puryear, 2014). However, the use of these terms is largely relative (i.e., accuracy implies that one person’s partner report matches the other’s self-report, not necessarily that the partner report matches some objective and observable behavioral reality).
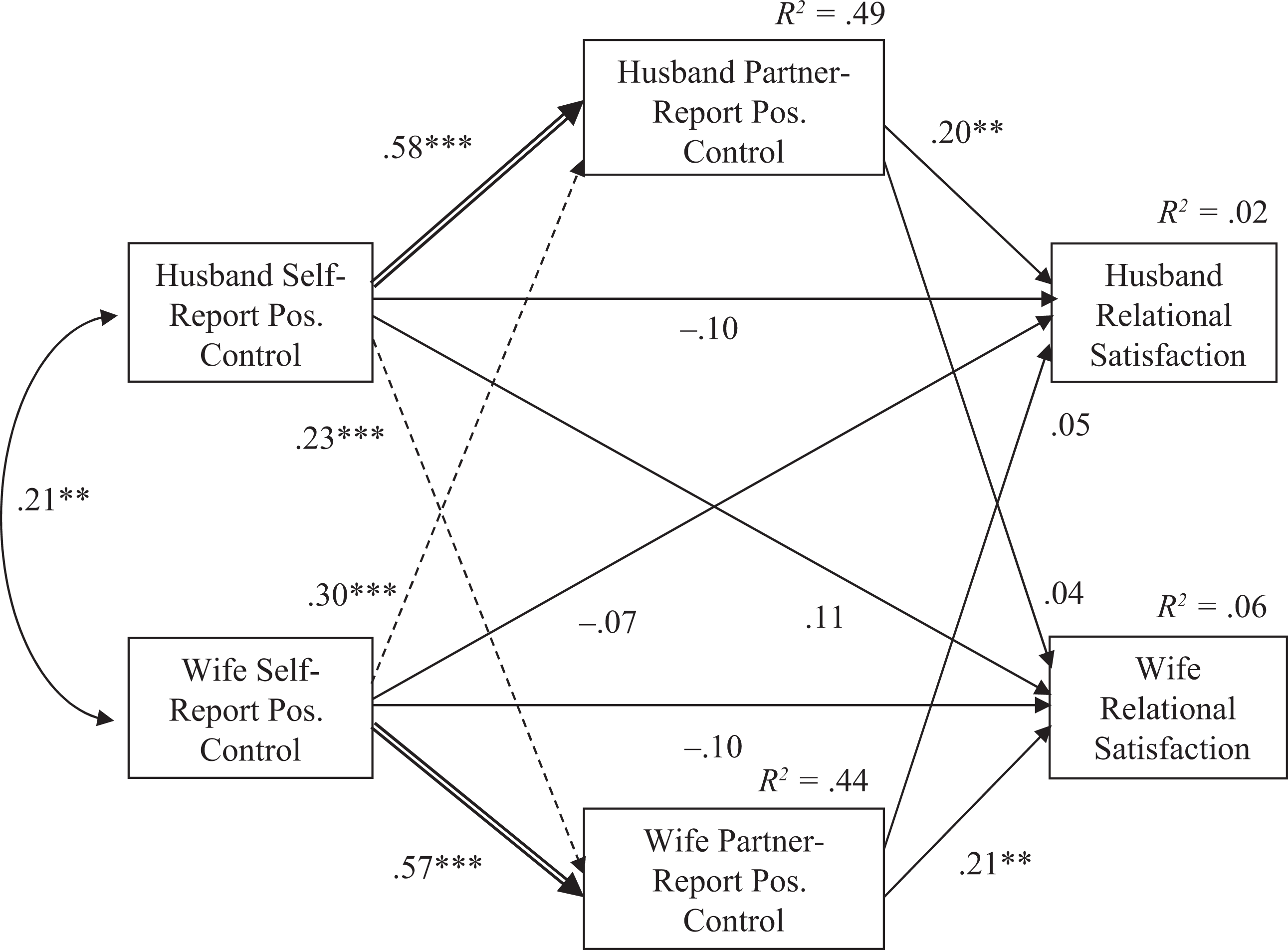
Actor–partner mediation model with self-reported positive control as the exogenous variable. Note. Figure values are standardized regression coefficients unless otherwise indicated. Dashed lines represent accuracy effects. Double lines represent bias effects. **p < .01; ***p < .001.
Whereas accuracy effects are more intuitive—that is, people accurately perceive their partner’s behaviors—bias effects could be driven by a variety of mechanisms. People could be biased as a function of an egocentric assumption that their partners’ enactment of social control is similar to their own enactment of social control. Alternatively, people’s biased perceptions might stem from their tendency toward biased relational enhancement (Neff & Karney, 2005). For instance, people who express concern for their partners’ health by enacting social control might be motivated to perceive that their partners care about their health (and enact social control) as well. These scenarios illustrate mechanisms through which individuals might perceive their partners’ social control to parallel their own (i.e., bias).
Whereas some research suggests that people’s marital quality is associated with idealized, or biased, perceptions of their partners (Murray et al., 2011), other research indicates that marital quality depends on the correspondence between individuals’ behaviors and their partners’ perceptions of those behaviors (Swann, de la Ronde, & Hixon, 1994). Additionally, research on social support among couples suggests that partners’ relationship quality is predicted by their accurate and biased perceptions of supportive behavior (Lemay & Neal, 2014). Perceptions are crucial to interpersonal communication, and they may be of greater importance than the content of messages (Gregory & Levy, 2015) and may contribute to a version of reality that sustains partners’ happiness (Finkenauer, Wijngaards-de Meij, Reis, & Rusbult, 2010). Thus, in addition to identifying potential accuracy and bias effects of couples’ diet- and exercise-related social control, couples’ accurate and biased perceptions of diet- and exercise-related social control will be examined in association with their relationship quality.
The current study
Research indicates that partners can be both accurate and biased in their evaluations of each other (Kenny & Acitelli, 2001; Lemay, 2014). However, these perceptual phenomena have never been examined within the context of social control in relationships. Thus, the purpose of the current study was to understand partners’ accuracy and bias with regard to their perceptions of diet- and exercise-related social control in their relationships:
In addition to elucidating these accuracy and bias effects, it is important to understand how couples’ relationship quality is associated with accurate perceptions (e.g., matching actor self-report of social control use and partner-reported perception of actor social control use) and biased perceptions (e.g., matching actor self-report of social control and actor reported perception of the partner’s social control use) of social control communication in relationships. People’s relationship quality is associated with their partners’ accuracy (Swann et al., 1994), biases (Murray et al., 2011), and accuracy and biases (Lemay & Neal, 2014); however, this phenomenon has not been investigated in the context of social control. In line with research by Lemay and Neal (2014) that examined the potential mediational effect of perceptions on relationship quality, our second research question asked:
Finally, given that relational partners inherently influence each other (Thibaut & Kelley, 1959), couples who wish to sustain their relationships might promote their relationship satisfaction (Rusbult & Buunk, 1993) through their communication of social control. Research indicates that people in harmonious relationships perceive more positive influence (Markey et al., 2007), yet other research indicates that social control is unrelated to relationship satisfaction (Butterfield & Lewis, 2002). Given the contrasting findings in the literature, the third research question is posed in an effort to understand the dyadic association between diet- and exercise-related social control and relationship quality:
Method
Participants
This study included 384 individuals (192 heterosexual couples) with a mean age of 48 years (SD = 11.26, range = 22–86). The mean relationship length was 21.33 years (SD = 10.77, range 1–44 years), and 91% of the couples were married and 9% were cohabiting. A majority of the sample reported that they had children (85%). The sample was primarily White (85%), followed by 9% Latino/a, 2% African American, 3% Asian/Pacific Islander, and 1% other. Participants were fairly well educated, with 25% reporting that they had a graduate/professional degree, 46% reported having a bachelor’s degree, 25% reported having some college/associate’s degree, and 4% reported having only completed high school.
Procedures
Couples were recruited through student referrals at a large Southwestern university. Students in communication courses at the university were asked to refer a couple in which both members were over 18 years old and in a married or cohabiting relationship to complete an online questionnaire. Students e-mailed the first author two separate e-mail addresses for the participants. Each participant was sent a separate e-mail message containing a link to the online questionnaire and a unique code number to enter at the end of the questionnaire. The code numbers matched the couples’ responses without the provision of identifying information. After completing the questionnaire, participants were directed to a separate website where they entered their mailing address in order to receive a US$10 gift card to a major retail store. Students received course credit in exchange for the referral.
The response rate was 90% among the 466 participants who were recruited (418 individuals responded). Twenty participants were removed from the analyses because their partners failed to complete the questionnaire. Additionally, the questionnaire administration software recorded the start and finish times of the questionnaire responses, and the data from seven couples were dropped because at least one partner completed the survey in less than 10 min. Because this survey was part of a larger study, we considered 10 min to be an insufficient amount of time for participants to thoughtfully respond to the questionnaire items. Therefore, after dropping these seven couples, the final sample size was 192 couples.
Measures
Social control
To measure (a) individuals’ use of social control and (b) individuals’ perceived social control from their partners, we adapted Butterfield and Lewis’ (2002) Health-Related Social Control Scale. The original scale was used to measure health-related social control strategies in general, but in this study, it was adapted to include a diet- and exercise-related focus. The adapted measure included 16 social control strategies: asked, bargained, guilt, expressed negative emotions, persistence, persuasion, expressed positive emotions, reasoned, stated importance, made suggestions, invoked obligation, told, used withdrawal, change, model/hint, and praise. Consistent with Tucker and Anders (2001), participants indicated how often in the last 6 months (a) they used each strategy to influence their partner to engage in healthier dieting behaviors (e.g., choose foods low in salt, fat, and calories) or exercise activities (e.g., walking, jogging, swimming, and bike riding) and (b) they perceived that their partners used each strategy to influence them to engage in healthier dieting and exercise activities. Participants indicated their own use of and perceived partner use of social control on a 1 (never) to 7 (daily) scale.
A principal components analysis was conducted to examine how people’s use of each of the 16 social control strategies loaded onto factors. Direct oblimin rotation was used to identify factor loadings. Two components emerged: positive social control and negative social control. Both factors had an eigenvalue greater than 1 and were above the elbow of the scree plot. Together the factors accounted for 70% of the variance. The positive social control factor included the following items: asked, expressed positive emotion, stated importance, made suggestions, change, model/hint, and praise. The negative social control variable included the following items: bargained, guilt, expressed negative emotions, invoked obligation, told, and used withdrawal. The factor loadings for positive social control ranged from .58 to .89, and the factor loadings for negative social control ranged from .67 to .84. The following items did not load on to either factor: persistence, persuasion, and reasoned. 1 The results were identical for people’s perceived social control from their partners, except that the two factors accounted for 61% of the variance.
The internal consistencies for individuals’ use of positive social control were α = .88 and α = .84 for women and men, respectively, and the internal consistencies for individuals’ perceived positive social control from the partner were α = .87 and α = .83 for women and men, respectively. The internal consistencies for individuals’ use of negative social control strategies were α = .87 and α = .88 for women and men, respectively, and the internal consistencies for individuals’ perceived negative social control from the partner was α = .89 for women and men. The negative social control composite variables were positively skewed (i.e., low scores reported for negative social control), so they were log transformed to obtain variables with a more normal distribution. All subsequent analyses were conducted with the transformed variables.
Relationship satisfaction
Hendrick’s (1988) Relationship Assessment Scale was used to assess relationship satisfaction. This 7-item scale included items such as, “How well does your partner meet your needs?” and “How often do you wish you hadn’t gotten into this relationship? (reverse scored). These items were measured on a 1 (negatively valenced) to 7 (positively valenced) scale. The internal consistencies for relationship satisfaction were α = .90 and α = .88 for women and men, respectively.
Demographic items
Demographic items included participants’ sex, age, race, education level, relationship type, and relationship length.
Results
Model fit
Tests of the hypothesized associations between self- and partner-reported social control and relational satisfaction were conducted with structural equation modeling following the actor–partner interdependence mediation model (APIMeM; Ledermann, Macho, & Kenny, 2011) using AMOS 20.0 with maximum likelihood estimation. Before testing individual paths and effects in the model that represents specific predictions from this study, it is first necessary to determine the overall fit of the model (Kline, 2010). Tests of global model fit can also be compared to a model in which partners’ paths are constrained equal versus one in which they are free to vary. The χ2 difference test for the global fit of two such models effectively indicates whether there are statistically significant sex differences in the effects specified in the models. The first model was estimated with self-reported positive social control as the exogenous variable and the second was estimated with self-reported negative social control as the exogenous variable. In both cases, the corresponding partner report of positive or negative social control was specified as the mediating variable and relationship satisfaction was the dependent variable. Most of the couples in the study were in married relationships (91%); therefore, for ease of interpretation, we henceforth refer to the partners as husbands and wives.
Following procedures recommended by Kenny and Ledermann (2010), we first fit an unconstrained version of the APIMeM, which is a saturated model, and compared that model to the fit of one that had all of the direct effects from husbands’ exogenous and mediating variables constrained equal to the corresponding direct effects from wives’ exogenous and mediating variables. This was followed by estimation of the indirect effects in each model and their 95% confidence intervals. For both models, a bias-corrected bootstrapping procedure based on 5,000 bootstrap samples was used to estimate the confidence intervals around the indirect effects.
Results from the first model, with self-reported positive social control as the exogenous variable, appear in Figure 1. The constrained model exhibited a close fit to the sample data, χ2 = 8.54, degrees of freedom (df) = 5, p = .13, χ2/df = 1.71, comparative fit index (CFI) = 0.99, root mean square error of approximation (RMSEA) = .06 (90% confidence interval (CI) = .00, .13). The χ2 from the constrained model was not significantly different from 0, which is the theoretical χ2 value of the unconstrained saturated model. Therefore, the more parsimonious constrained model in which husbands’ effects were constrained equal to the corresponding effects for wives was used to generate estimates of the hypothesized effects.
Results from the second model, with self-reported negative social control as the exogenous variable, appear in Figure 2. The constrained model exhibited a close fit to the sample data, χ2 = 7.47, df = 5, p = .19, χ2/df = 1.497, CFI = 0.99, RMSEA = .05 (90% CI = .00, .12). The χ2 from the constrained model was not significantly different from 0, which is the theoretical χ2 value of the unconstrained saturated model. Therefore, the more parsimonious constrained model was used to generate estimates of the hypothesized effects.
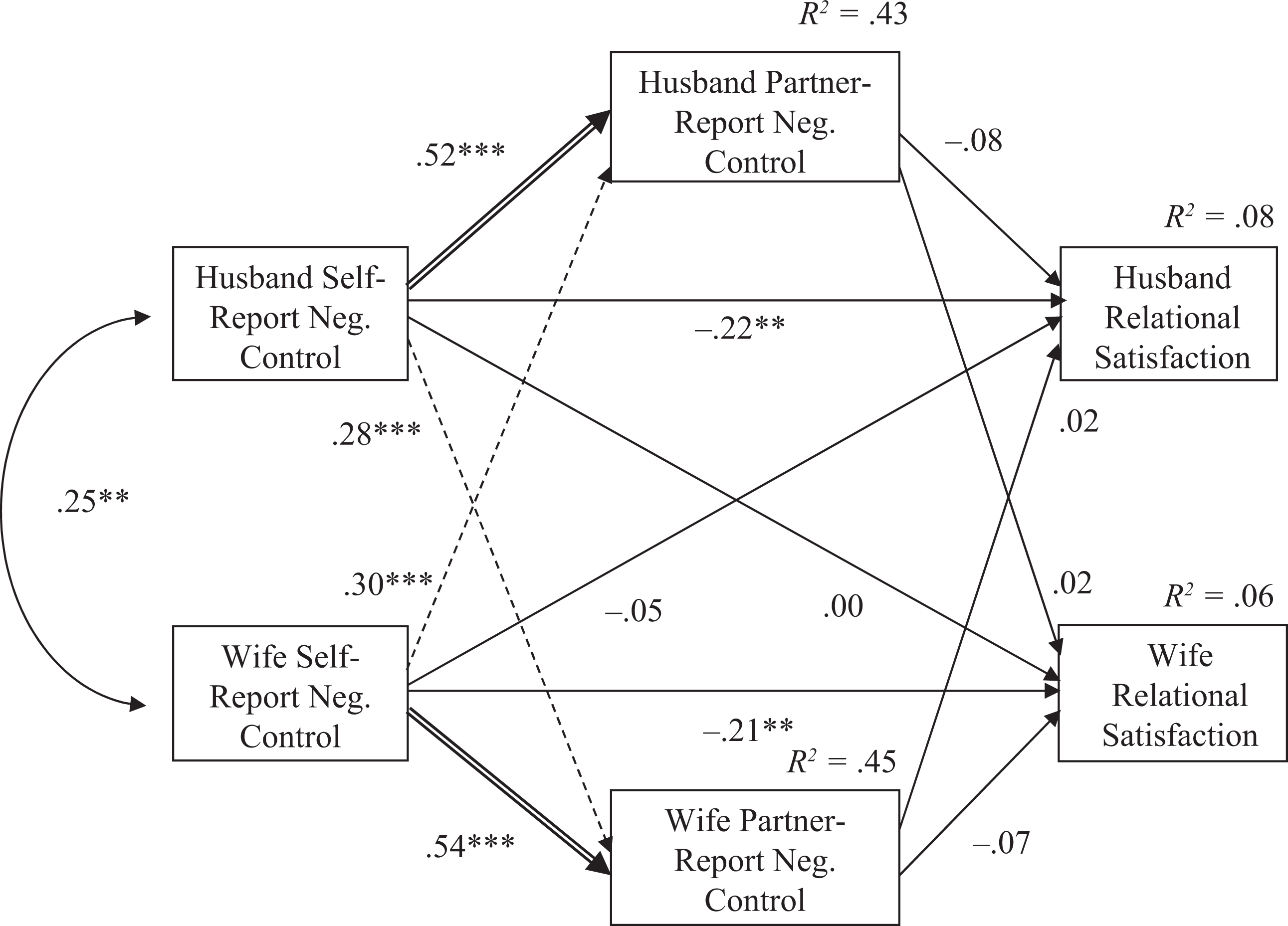
Actor–partner mediation model with self-reported negative control as the exogenous variable. Note. Figure values are standardized regression coefficients unless otherwise indicated. Dashed lines represent accuracy effects. Double lines represent bias effects. **p < .01; ***p < .001.
For the sake of thoroughness, we report separate effects for husbands and wives from the constrained models in the following report. However, both of the constrained models fit as well as the unconstrained models, which indicates that there is no evidence of meaningful differences in the magnitude of effects that are presented for husbands versus wives.
Research questions
Research question 1 asked whether partners are accurate, biased, or both in their perceptions of each other’s use of diet- and exercise-related social control. See Table 1 for means and standard deviations for study variables. In the APIMeM, accuracy effects are evident in significant paths from one person’s self-reported social control strategy use to the partner’s partner-reported perception of social control strategy use. There were four such potential effects, two for positive (Figure 1) and two for negative (Figure 2) social control strategies. For positive social control, wives’ self-reports were predictive of husbands’ partner reports (β = .30, p < .001) and husbands’ self-reports were predictive of wives’ partner reports (β = .23, p < .001). For negative social control, wives’ self-reports were predictive of husbands’ partner reports (β = .30, p < .001) and husbands’ self-reports were predictive of wives’ partner reports (β = .28, p < .001). Collectively, these findings provide evidence of accuracy in people’s perceptions of their partner’s social control strategy use, relative to their partner’s self-reports.
In these APIMeMs, biased perceptions are evident in significant paths from a person’s self-reported strategy use to his or her partner-reported strategy use. For positive social control, wives’ self-reports were predictive of their partner reports (β = .57, p < .001) and husbands’ self-reports were predictive of their partner reports (β = .58, p < .001). For negative social control, wives’ self-reports were predictive of their partner reports (β = .54, p < .001) and husbands’ self-reports were predictive of their partner reports (β = .52, p < .001). Collectively, these four significant effects provide strong evidence of biased perceptions such that people tend to see social control strategy use in their partners similarly to how they see these strategies used by the self.
Research question 2 asked whether individuals’ accurate or biased perceptions of diet- and exercise-related social control are associated with their relationship satisfaction. In the APIMeM, the effect of accuracy on satisfaction was examined by testing the indirect effect from one spouse’s self-reported social control to the other spouse’s relationship satisfaction, through the other spouse’s partner-reported social control. There are two such indirect effects in each model. For positive social control use (Figure 1), the wife self-report → husband partner report → husband relationship satisfaction indirect effect was statistically significant (B = .05, p < .05), as was the husband self-report → wife partner report → wife relationship satisfaction indirect effect (B = .05, p < .05). For negative social control (Figure 2), neither the wife self-report → husband partner report → husband relationship satisfaction indirect effect (B = −.19, ns) nor the husband self-report → wife partner report → wife relationship satisfaction indirect effect (B = −.03, ns) was statistically significant. These results therefore provide no evidence that accurate perceptions of a partner’s negative social strategy use contribute to that partner’s relationship satisfaction. However, the results indicate that accurate perceptions of a partner’s positive strategy use are significantly associated with relationship satisfaction.
In the APIMeM, the effect of biased perception on satisfaction was examined by testing the indirect effect from one spouse’s self-reported social control to that same spouse’s relationship satisfaction through that same spouse’s partner-reported social control. In other words, these indirect effects are the product of two actor effects, all within the same individual. For positive social control use, the wife self-report → wife partner report → wife relationship satisfaction indirect effect was statistically significant (B = .07, p < .05) and the husband self-report → husband partner report → husband relationship satisfaction indirect effect was just outside the range of statistical significance (B = .13, p = .06). For negative social control use, the wife self-report → wife partner report → wife relationship satisfaction indirect effect (B = −.06, ns) and the husband self-report → husband partner report → husband relationship satisfaction indirect effect (B = −.36, ns) were both nonsignificant. These results indicate that biased perception is predictive of relationship satisfaction, but only for positive social control strategy use.
Research question 3a asked how self-reported use of diet- and exercise-related social control is associated with self (actor effect) and partner (partner effect) relationship satisfaction. Tests of these effects are evident in the path from both of the actor-reported social control use variables to both of the relationship satisfaction variables. For positive social control strategies (Figure 1), both actor effects (self positive social control use → self relationship satisfaction) and both partner effects (self positive social control use → partner relationship satisfaction) were nonsignificant. For negative social control strategies (Figure 2), the actor effects for husbands (β = −.22, p < .01) and wives (β = −.21, p < .01) were statistically significant, but the partner effects were nonsignificant. Individuals who reported using more negative social control reported lower relationship satisfaction.
Means and standard deviations for study variables.
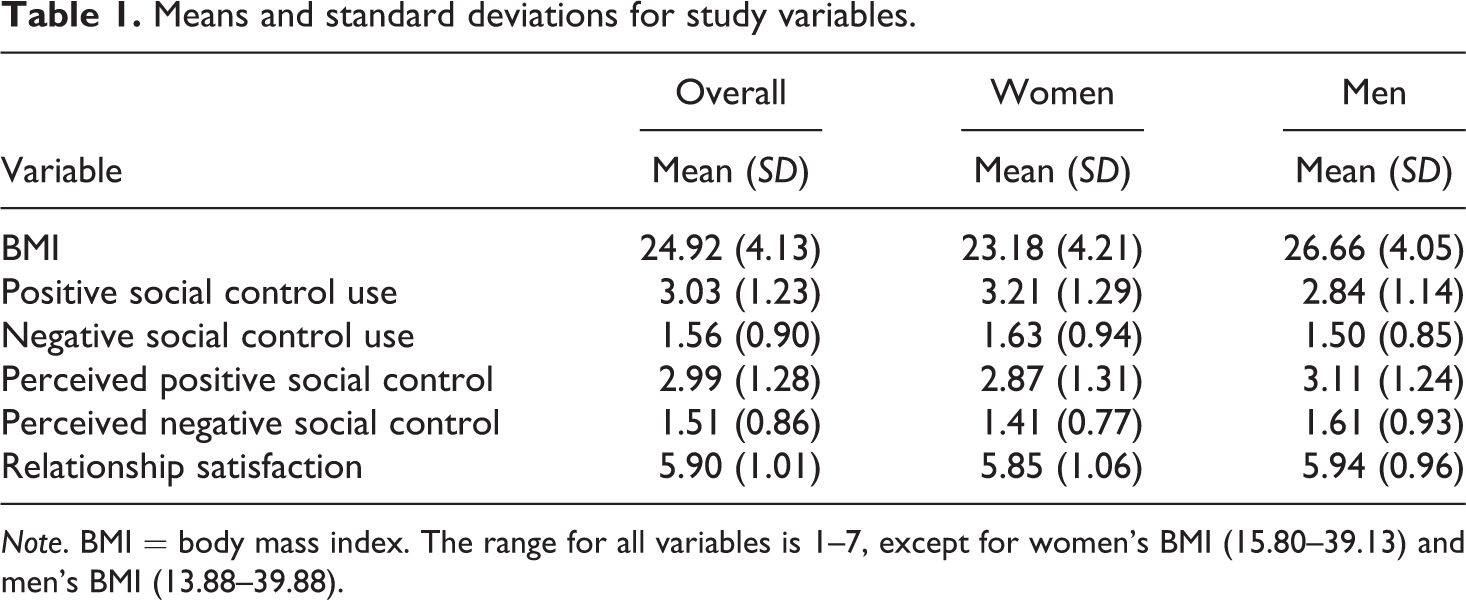
Note. BMI = body mass index. The range for all variables is 1–7, except for women’s BMI (15.80–39.13) and men’s BMI (13.88–39.88).
Research question 3b asked how perceived diet- and exercise-related social control is associated with self (actor effect) and partner (partner effect) relationship satisfaction. Tests of these effects are evident in the path from both partner-reported social control variables to both of the relationship satisfaction variables. For positive social control (Figure 1), the actor effect (self positive social control perception → self relationship satisfaction) for husbands (β = .20, p < .01) and for wives (β = .21, p < .01) were both statistically significant. However, both of the partner effects (self positive social control perception → partner satisfaction) were nonsignificant. For negative social control (Figure 2), both actor effects and partner effects were nonsignificant. Individuals who perceived greater positive social control from their partners reported greater relationship satisfaction.
Discussion
The purpose of this study was to investigate potential accuracy and bias effects in couples’ health-related social control and the concurrent associations with relationship satisfaction. We found that people were both accurate and biased with regard to their positive and negative social control communication. That is, individuals’ reported use of social control corresponded with their partners’ perceptions of these individuals’ social control use (accuracy), and individuals perceived their partners’ social control use to be similar to their own (bias). Accurate perceptions were related to people’s relationship satisfaction when considering positive, but not negative, social control. Biased perceptions also predicted relationship satisfaction only in the context of positive social control perceptions. Finally, people reported greater relationship satisfaction as their own use of negative social control decreased and as their perceptions of positive social control from their partners increased.
Accuracy and bias
The results for the accuracy and bias effects in this study are consistent with the idea that relational partners mutually influence each other (Thibaut & Kelley, 1959), which is demonstrated through their use of diet- and exercise-related social control. Further, partners can be simultaneously accurate and biased in their perceptions (Boyes & Fletcher, 2007; Kenny & Acitelli, 2001) of the diet- and exercise-related social control communication in their relationships. Accuracy effects indicate that actors perceive greater positive social control from their partners as their partners report using greater positive social control, thereby highlighting couples’ correspondence with regard to social control in their relationships. The bias effects demonstrated perceived similarity between the partners illustrated through actors’ increased perception of positive social control from their partners as their own reports of positive social control use increased. Parallel patterns emerged for negative social control.
Simultaneously, accurate and biased perceptions of social control can be illustrated in the following hypothetical example. Assume that a wife’s mean score for her own use of positive social control was 7, her husband’s mean score for his own use of positive social control was 2, and the wife’s mean score for her perception of positive social control from her husband was 5. This example illustrates that there is agreement between the husband and wife in terms of the husband’s relatively low enactment of positive social control (accuracy), while at the same time illustrating how the wife might assimilate the mean score for her husband’s use of positive social control in the direction of her own self-reported use of positive social control (bias).
Given the preponderance of relational literature suggesting that partners are similar in terms of their attitudes (Gaunt, 2006), personality (Luo & Klohnen, 2005), communication (Burleson & Denton, 1992), and emotional experiences (Gonzaga, Campos, & Bradbury, 2007), it makes sense that partners would enact similar social control behaviors. If partners are similar in terms of their enactment of social control, then it stands to reason that their bias might enhance their accuracy with regard to social control. Another explanation for the concurrent accuracy and bias effects in these couples lies within the notion that people have two distinct motivations driving their relationship evaluations. People have objectivity needs (i.e., accuracy), as well as self-esteem needs (i.e., benevolence; Gagné & Lydon, 2004), and they are motivated to attend to partner behaviors when they want to be accurate. For example, people who detect guilt from their partners might gather evidence of this guilt induction. At the same time, people might feel compelled to enhance their relational perceptions. For instance, people who use positive social control might also attribute greater positive communication to their partners. This is consistent with the idea that satisfied couples tend to see their interactions in a positive light (Fincham & Bradbury, 1991). Similarly, people who use negative social control might attribute greater negative communication to their partners, which could reflect their negative sentiment override (Fincham, Bradbury, & Scott, 1990). Although they seem inextricable, these two motivational states are independent and can operate concurrently in relationships.
The correspondence between social control use and perceptions in these couples reflects a reciprocal, health-oriented relational environment for those couples who are actively communicating health-enhancing influence messages. For instance, it could be that people enact social control to encourage their partners to adopt healthier behaviors and are also the target of their partners’ health-enhancing social control. This pattern confirms the idea that partners influence each other’s health (Lewis et al., 2004) as well as each other’s relational experiences and outcomes (Rusbult & Buunk, 1993). Thus, partners’ diet- and exercise-related social control transactions likely demonstrate their desire to maintain each other’s health and, ultimately, their relationships. This is not the case for all relationships, however, as some partners engage in limited health-related social control, thereby allowing for a more health-neglectful or permissive environment.
Whereas people appear to engage in healthier behaviors in association with positive social control from their partners (Lewis & Butterfield, 2007), they might have more maladaptive health responses to negative social control from their partners (Tucker & Anders, 2001). Understanding the benefits and barriers of health-related social control is becoming increasingly important, given that health conditions including diabetes, hypertension, cardiovascular diseases, and certain cancers are associated with obesity (Poirier et al., 2006) and corresponding lifestyle factors such as diet and exercise. The results from this study reinforce the significance of perceptions in relationships (Finkenauer et al., 2010) and highlight the correspondence between individuals’ use of diet- and exercise-related social control and their partners’ perceptions of these individuals’ social control use. These findings provide crucial information regarding health-related social control transactions in couples. Whereas people who perceive positive social control from their partners might evaluate this communication as relationship maintenance, people who perceive negative social control from their partners might feel ridiculed; therefore, it is important to understand how these accuracy and bias effects are associated with relationship quality.
Social control and relationship quality
Extant research indicates that marital quality depends on couples accurately identifying each other’s perspectives and behaviors (Swann et al., 1994) and that accuracy and bias with regard to partners’ support is predictive of their relationship satisfaction (Lemay & Neal, 2014). In the present study, accurate perceptions of social control were associated with people’s relationship satisfaction, but only for positive social control. Moreover, the results were consistent with the notion that individuals’ relationship quality is associated with their biased relational enhancement (Neff & Karney, 2005), as biased perceptions of positive social control were also significantly associated with people’s relationship satisfaction. These findings were also aligned with research suggesting that people’s biased perceptions of partner responsiveness promote relationship satisfaction (Lemay, Clark, & Feeney, 2007) and that people report positive outcomes when they perceive their own and their friend’s communal responsiveness to be similar (Lemay & Clark, 2008). While accurate and biased perceptions of positive social control appear to be indicative of positive relationship quality, no significant indirect effects emerged for negative social control. Although people are both accurate and biased with regard to negative social control in their relationships, their accuracy and bias is not associated with their relationship satisfaction for negative social control.
As mentioned previously, people generally prefer to enact positive social control in their relationships (Lewis & Butterfield, 2007; Markey et al., 2007). This tendency is illustrated among the couples in the current study and also makes sense in the context of health communication wherein people enact social control because they want their partners to be healthier (Butterfield & Lewis, 2002). These individuals appear to consider their partners’ feelings in enacting positive social control and also detect their partners’ concern for their welfare in their perceived social control from their partners. Together, this positive communication is associated with greater relationship satisfaction. Given that this study is cross-sectional, however, we cannot determine whether people in high-quality relationships are more likely to enact and perceive positive social control or whether people feel more satisfied because they enact and perceive positive social control.
When we examined the direct effects of individuals’ use of and perceptions of social control on their relationship satisfaction (RQ3), we found that people reported greater relationship satisfaction as they perceived greater positive social control from their partners. This finding is consistent with the indirect effects models and with the literature indicating that people in harmonious relationships perceive greater positive social influence from the partner (Markey et al., 2007). Together these findings reinforce that people’s perception of their partners’ health communication is important to consider in conjunction with their relationship satisfaction (Markey et al., 2007) and their health communication (Dailey, Romo, & Thompson, 2011). However, this study builds upon the previous research by identifying how positive and negative social control are distinctly associated with their relationship satisfaction.
Specifically, people’s relationship satisfaction increased as their own use of negative social control decreased. Analyzing people’s use of and perceptions of social control separate from the accuracy and bias indirect effects allowed us to detect this significant actor effect for negative social control. This finding is intuitive within the context of diet- and exercise-related communication. People generally employ positive social control rather than negative social control (Butterfield & Lewis, 2002; Lewis & Butterfield, 2007) and negative weight-related communication is associated with decreased relationship satisfaction (Sheets & Ajmere, 2005). Therefore, individuals likely feel more satisfied in relationships where they do not feel compelled to exercise negative social control. These results provide a more complete picture of how positive and negative social control operate in romantic relationships.
Limitations and future directions
The primary limitation with this study is the cross-sectional design, which limits any potential conclusions about the directionality of the significant effects. In order to better understand the direction of the associations between the variables in this study, it would be useful to examine them longitudinally or experimentally in future research. Similarly, given that the measures were not randomized, it is possible that people’s reports of social control use could have influenced their reports of perceived social control from their partners. The actor effects in the models were generally stronger than the partner effects, which might have been due in part to common method variance. Although we did make an effort to separate these variables in the questionnaire, it may be useful in future research to randomize the order of presentation to mitigate potential carry over effects in the measurement of social influence strategies. This study is also limited by the use of self-report measures to assess the variables. Participants could have altered their responses to be more socially desirable, particularly with regard to weight status and social control (Burleson et al., 1988), as people tend to underreport less socially desirable types of influence. Alternatively, it is possible that the large proportion of relatively satisfied intact couples in this study do not engage in negative social control strategies frequently in their relationships. Finally, as mentioned previously, the terms accuracy and bias are best understood as relative, and not absolute processes. Thus, future research might incorporate a laboratory element wherein people’s interactions could be observed and coded in order to counteract biases in either self- or partner reports that may cause some derivations from observable levels of social control behaviors.
Conclusion
The current study builds upon the extant research on health-related social control by identifying couples’ accurate and biased evaluations of positive and negative social control in their relationships. Individuals clearly demonstrate relative agreement with their partners concerning the use of positive and negative social control in the context of weight-related communication. At the same time, people’s perceptions of their partner’s social control communication also tend to align with perceptions of their own social control communication. Moreover, people’s relationship satisfaction is associated with their accurate and biased perceptions of positive social control, with their own use of negative social control and with their views of their partners’ positive social control communication. Together these findings show that partners can and will agree on how they influence each other in the context of diet- and exercise-related discussions as well as how their perceived control tactics may have implications for their relationship satisfaction.
Footnotes
Authors’ note
An article featuring data from this dissertation research was published in Health Communication.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a dissertation research award from the Department of Communication at the University of Arizona.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.