
Abstract
Postpartum depression (PPD) is a common mental health complication of pregnancy and childbirth with long- and short-term consequences for the wellbeing and the functioning of parents. In particular, first-time parents seem to be at high risk for developing post-birth depressive symptoms as the transition to parenthood elevates stress and demands adjustment to significant changes. Prior research has mostly documented individual characteristics, such as prenatal depression and psychiatric history, as predictors of PPD, but much less is known about the potential contribution of interpersonal processes within relational contexts, such as the coparenting relationship, to PPD among first-time mothers and fathers. With evidence suggesting that coparenting dynamics start developing prior to the birth, it is imperative to consider characteristics of coparenting interaction behaviors as early as during pregnancy to identify such behaviors as risk or protective factors for PPD. In the current study, we explored one’s own (actor) and partner’s observed prenatal coparenting behaviors as predictors of mothers' and fathers' PPD. A mixed-method longitudinal study with 107 expectant couples provided both partners' self-report measures and observational data from interaction tasks prenatally, and at 3 and 6 months post-birth. APIM multilevel model analyses revealed that both negative (i.e., withdrawal and conflict) and positive (i.e., communication skills, support, and problem solving attempts) prenatal coparenting behaviors were uniquely predictive of PPD among first-time parents above and beyond other potential predictors of PPD, although several similarities and dissimilarities among fathers and mothers were detected.
Introduction
Postpartum depression (PPD) is considered one of the most common complications of pregnancy and childbirth, and can have adverse implications for the functioning of the parent, the couple relationship, the nature of the parent-infant bonding, and the development of the infant (Allen et al., 2023; Letourneau et al., 2017; Werner et al., 2015). With its obvious risk for all family members, researchers have been motivated to identify risk factors that can contribute to the development of PPD. Much of that work has highlighted individual characteristics, including personality traits and personal history, as central factors contributing to this mental health condition (Guintivano et al., 2018; Hahn-Holbrook et al., 2018).
Among these factors, parents' prenatal depression has been consistently identified as strongly associated with PPD (Ghaedrahmati et al., 2017; Liu et al., 2022). It has been suggested that, especially among first-time parents, depressive symptoms identified prior to the birth can increase with the new demands and elevated stress post birth (Burke et al., 2022; Scheyer & Urizar, 2016). One’s psychiatric history has also been identified as a risk factor for PPD, with prepartum anxiety, mood disorders, obsessive-compulsive disorder, and personality disorders were all associated with PPD (Puyané et al., 2022; Viguera et al., 2011). Other risk factors include one’s genetic background, traumatic and adverse life events, and physiological changes from pre-to post-birth (e.g., hormones) (Ertel et al., 2011; Batt et al., 2020). Existing research, then, has mainly considered PPD as a mental health condition rooted in the individual’s characteristics and history. Family systems theory (Kerr & Bowen, 1988), however, posits that the functioning of one partner relates not only to their own individual characteristics but rather, to the influences others have on them in their relational environments. In this sense, much less is known about how interpersonal and social contexts may contribute to increased or decreased depressive symptoms post-birth. Because most often than not, children are born into a couple or family system (Segrin & Flora, 2018), relational contexts are important to consider as a possible factor linked to depressive symptoms post-birth.
One such central context is the coparenting relationship of the couple. From a family systems perspective, the couple consists of two interdependent individuals that are best understood within the context of their relational unit. From this theoretical viewpoint, the mutual influences partners have on each other, and that are reflected and constructed in their interactions (Holmes et al., 2013), contribute to the shaping of each and both couple members' emotional experiences. Particularly in the early stages of the transition to parenthood, when partners become parents, the coparenting aspects are especially prominent in the couple relationship, as partners try to co-construct their emerging family functioning in their new parental roles. In this sense, while preparing for the birth of their first child during pregnancy, the amount and centrality of interactions about the nature of parenting and coparenting probably increase (Van Egeren, 2004). As such, coparenting – which refers to the aspects of the couple relationship that are concerned with parenting (Feinberg, 2003; 2012) – is essential to the daily experience of mothers and fathers, and can potentially contribute to either advancing or buffering against postnatal depressive symptoms.
Indeed, there is some evidence that point to associations between the perinatal coparenting relationship and PPD (Solmeyer & Feinberg, 2011; Tissot et al., 2017). However, with accumulating work suggesting that the coparenting relationship starts developing prior to the birth of the child, it is possible that prenatal coparenting dynamics contribute to the emotional experience of first-time mothers and fathers during pregnancy and post-birth. Moreover, a developmental conceptualization of the transition to parenthood suggests that it unfolds over time (Cowan & Hetherington, 2013) and thus, changes occurring over the transition to parenthood are best predicted based on the couple’s behavioral manifestations, functioning, and structural organization during the time period just prior to the transition (Kuersten-Hogan & McHale, 2021; Lewis, 1989). In other words, it may be that already prenatal – and not only postnatal – coparenting relationship emerging during pregnancy associated with PPD.
The serious implications of PPD on all family members call for identifying factors that may contribute to its development as early as during pregnancy. Given the critical role intimate partners play in providing a sense of emotional security and support during the stressful time of a birth of an infant – particularly for the first time (i.e., during the transition to parenthood) – it is imperative to consider the dynamics of prenatal coparenting as a predictor of depressive symptoms postpartum. In this paper, we report the findings of a study which aimed to assess the contribution of prenatal coparenting behaviors to PPD in first-time mothers and fathers. As an interpersonal exchange process involving two individuals, we specifically explored the effects of each partner’s prenatal coparenting behaviors on their own and their partner’s depression postnatally. In light of existing research on PPD, we tested our hypotheses controlling for both individual characteristics, such as pre-birth levels of depression, and coparenting dynamics, such as participants' prenatal coparenting expectations and their perceived postnatal coparenting quality.
Postpartum Depression
PPD is a common complication of pregnancy and childbirth with long- and short-term consequences for the mental experience and the functioning of all family members (Johnson et al., 2020; Patel et al., 2012). PPD can start at any time within the first year after the birth (O'Hara & Wisner, 2014), and although it usually lasts for several weeks or months and up to 1 year, for some parents PPD can last for several years (Goodman, 2004; Wang et al., 2021). The rates of PPD among first-time parents is higher than among parents who already have children (Räisänen et al., 2013), and both mothers and fathers report having depressive symptoms after the birth of their first child (Gross & Marcussen, 2017). In Western countries, whereas 10% to 30% of new mothers are reported to have persistent depressive symptoms postpartum (Simhi et al., 2019; Zaidi et al., 2017), 10% to 20% of new fathers are identified with such symptoms (Ansari et al., 2021; Eddy et al., 2019). It has been suggested, however, that the actual rates of paternal PPD may be higher, as lack of awareness of both professionals and fathers themselves keep paternal PPD invisible or, at least, less recognized than maternal PPD (Swami et al., 2020).
Whereas a large body of research has focused on maternal PPD, research on paternal PPD is still relatively scarce (Mueller et al., 2019). Accumulating evidence suggest that there are both similarities and differences among mothers and fathers in terms of PPD predictors and effects. According to Mickelson et al. (2017), PPD in fathers is better predicted by intrapersonal factors, whereas interpersonal factors better predict PPD in mothers. According to this perspective, fathers, who tend to be more self-focused than mothers, usually rely on their own internal resources when feeling distressed, whereas mothers, who tend to be more relationship-oriented than fathers, seek help and support from others (Galdas et al., 2005; Kwon et al., 2013). Some findings support this assertion, indicating that low social support and negative maternal relationship with extended family members strongly predict PPD among mothers, but not fathers, and that paternal self-efficacy and perceived stress are strong predictors of PPD among fathers, but not mothers (Kamalifard et al., 2014; Klainin & Arthur, 2009; Zheng et al., 2022).
On the other hand, other studies identified similar predictors of PPD among fathers and mothers, including low household income, number of stressful life events, and low prenatal social support (Leung et al., 2017). Yet other studies have suggested that men do seek emotional support, but they tend to be more dependent on their spouse for seeking and receiving such support, whereas women seem to rely on friends and other members of their social networks for sharing intimate information and requesting for advice (Escribà-Agüir & Artazcoz, 2011). One recurring finding points to partner’s PPD as a strong predictor of PPD in the other partner, among both mothers and fathers (Don & Mickelson, 2012; Altenau, 2020). In this sense, maternal and paternal PPD are often correlated (Gao et al., 2009; Paulson & Bazemore, 2010). This consistent finding suggests that PPD is potentially influenced by interpersonal processes within the couple with partners' emotional processes show interdependence (Estlein & Theiss, 2022). Considering that during the transition to parenthood, starting already during pregnancy, partners concentrate much of their efforts and time together to adjust to their emerging coparenting tasks (Van Egeren, 2004), it is imperative to explore prenatal coparenting dynamics as a predictor of postpartum emotional experiences, such as PPD.
Coparenting
Coparenting focuses on the partners in their parental roles (Feinberg, 2003). More specifically, the concept refers to the ways caregivers of a child share and divide tasks and activities under their responsibility, and to their dynamics of support and conflict management in this role (Feinberg, 2003; McHale, 1995). The coparenting relationship is critical to the family functioning due to its significant effects on the couple relationship, the parent-child relationship, and child development (Sahi, 2019; Eira Nunes et al., 2021; Pedro et al., 2012). Whereas some parent partners find effective ways to work together, others are struggling in their coparenting. The quality of the coparenting relationship depends on the degree of the partners' collaboration, affirmation, and support (McHale et al., 2004). Indeed, coparenting is conceptually considered to comprise a number of related aspects, including positive constructive elements, such as coparental cooperation, validation, childrearing agreement, as well as negative maladaptive communication patterns of coparental destructive conflict, and undermining (Feinberg, 2003; McHale et al., 2004). Although each aspect reflects a somewhat different area of coparenting, they all form a global concept of the coparenting relationship, which can be more, or less, positive (Feinberg et al., 2012), depending on the degree to which partners balance, communicate, and employ the different aspects in their interaction.
The coparenting relationship is first emerging and developing during the transition to parenthood, where first-time parents have to adjust to many changes and new demands. Increased time demands of infant care, and increased pressure that stems from creating a new routine with new responsibilities, can all lead to a significant decline in the amount of shared time spent by the partners for romantic joint activities, and fewer in opportunities for discussions related to relational issues compared to pre-birth (Theiss et al., 2013; Cowan & Cowan, 2000). Such decline in relationship maintenance is associated with decreased relationship satisfaction (Halford & Petch, 2010) that, due to the interdependence that exists across family subsystems, can also “spill over” onto the coparenting relationship (Estlein & Theiss, 2022). Particularly, first-time partners need to reestablish roles, reassign responsibilities, reorganize and renegotiate the division of housework, childcare tasks, and scheduling time at work (Theiss et al., 2013; Rauch-Anderegg et al., 2020). In order to effectively co-construct their new routines, partners are required to communicate and to interact cooperatively, which, during such a stressful time, can be significantly challenging for many couples. For such couples, coparenting can be a distressing context that can enhance negative emotion and cognition, reflected in increased depressive symptoms.
Indeed, studies have found associations between parents' depression and post-birth coparenting dynamics (e.g., Elliston et al., 2008; Solmeyer & Feinberg, 2011; Tissot et al., 2017). Specifically, prior research has indicated that negative elements in the coparenting relationship – undermining coparenting in particular – predict depressive symptoms among mothers and fathers (Volling et al., 2021). Along these lines, Takeishi et al. (2021) have highlighted coparenting as one central source of support for mothers who are coping with mental disorders in general and particularly depression, suggesting that a positive coparenting relationship can serve as a protective factor against PPD.
According to prior research, thus, the postnatal coparenting relationship is associated with PPD. Conceptual and empirical evidence, however, suggest that coparenting starts developing even prior to the arrival of the infant (e.g., Ammaniti et al., 2006; Darwiche et al., 2016). Some studies, for example, have documented associations between prenatal coparenting expectations and postnatal cohesion and solidarity (McHale et al., 2004; McHale & Rotman, 2007), where others showed associations between prenatal and postnatal coparenting characteristics (Altenburger et al., 2014; Kuersten-Hogan, 2017). Such evidence points to the nature of the coparenting relationship as an ongoing developing process, and highlights the need to consider prenatal coparenting dynamics as predictors of postnatal characteristics of the family and the parents. In the current study, we highlight the possibility that specific aspects of prenatal coparenting dynamics predict PPD among first-time mothers and fathers; specifically, we suggest that emerging coparenting dynamics pre-birth can contribute to more turbulence or alternatively stability in the couple developing parent partners' relationship, which can constitutes an important relational context for the emotional experience, such as depression, of both partners. Because the coparenting relationship is interpersonal, and because prior research suggests that an individual’s PPD is associated with both their own prenatal depression and their partner’s postnatal depression, in the current study we look at both one’s own (actor) and partner’s prenatal coparenting behavior as potential predictors of mothers' and fathers' PPD. We, thus, hypothesize that a first-time mother’s and father’s own (actor) and partner’s prenatal coparenting behaviors will predict own and partner postnatal depressive symptoms, such that:
Own and partner’s prenatal negative coparenting behavior predicts first-time mothers' and fathers' PPD.
Own and partner’s prenatal positive coparenting behavior predicts first-time mothers' and fathers' PPD. To probe the possibility that actor’s and partner’s prenatal coparenting behaviors predict PPD among first-time mothers and fathers above and beyond other potential factors, we test our hypotheses controlling for previously documented predictors of PPD, such as prenatal depression levels, partner’s PPD, prenatal coparenting expectations and perceived postnatal coparenting, as well as demographic variables, including parents' age, sex of the child, education, and family income (see prior research on the associations between these demographic characteristics and PPD, for example, Muraca & Joseph, 2014; Segre et al., 2007; Watkins et al., 2011).
Method
Participants
One hundred and seven Israeli families participated in the current longitudinal study on the transition to parenthood. Families included co-habiting heterosexual Jewish couples who were expecting their first child (M = 29.7 weeks pregnant, SD = 2.55 weeks). The study was approved by the local Institutional Review Board. Participants were recruited through Internet advertisement, flyers, and medical centers. For each completed phase in the study, families received 250 NIS (approximately $72 at the time of data collection). Mothers' mean age was 30.82 (SD = 3.63, range = 23–42) and fathers' mean age was 32.41 (SD = 4.01, range = 23–42). All pregnancies were reported non-at-risk and parents reported no neurological or psychological disorders. Participates were mostly middle-to upper-class and college-educated (years of education: M = 16.30, SD = 2.10 for women; M = 15.36, SD = 2.41 for men). Family income referred to the average gross income for a household with children in Israel at the time of the study, and ranged from below-average (25.5%) to average (15.3%), or above-average (59.2%). Mothers' education level was 16.3 years (SD = 2.10), and fathers' education level was 15.36 years (SD = 2.41). Fifty-seven of the infants were boys (53.27%) and 50 were girls (46.72%).
Procedure
The data for the current study were taken from three sampling times: prenatally (T1; during the third trimester of pregnancy), 3 months (T2), and 6 months postpartum (T3). At T1, the couple was invited to the laboratory where each partner completed a questionnaire assessing their perceptions of their post-birth coparenting relationship, depressive symptoms, and sociodemographic variables. After the partners completed the survey, the couple was video recorded during the Inconsolable Doll Task (IDT) procedure (Shai, 2019) to be coded later for manifestations of coparenting behaviors. In this procedure, a doll resembling a real infant in physical appearance, size, and weight (2.95 kg) is used to simulate a real infant. The doll (RealCare Baby II-Plus; Realityworks, Eau Claire, WI, USA) is programmed with various realistic crying sounds and physical features modeled in a way that should prompt real caring and nurturing. In the IDT, the participating expectant parents received instructions on how to take care of the baby, and were asked to try and soothe it when it cries. A research assistant introduced the doll to the couple and demonstrated how to comfort and take care of it (for a full description, see Shai, 2019).
After this introduction, the research assistant asked one of the parents to stay with the doll (counterbalanced), while the other waited in the waiting room. Upon leaving the room, the research assistant discretely programmed the doll’s status to “non-responsive” to parental care. Following this, the parent who stayed in the room with the distressed “infant” had to respond to its intermittent crying for 5 minutes. After 5 minutes, the research assistant asked the other parent to join the first parent in the mission of soothing the “infant” for 5 additional minutes. The doll was programmed in the same manner as with the one parent so it did not respond to any of the partners' attempts to calm it down. This procedure was designated to invoke some stress in the participating partners to which they could have responded with collaborative coparenting behaviors or, alternatively, more conflictual coparenting dynamics.
In addition to the prenatal IDT procedure at T1, in all three time points, participants completed questionnaires about their coparenting relationship (in T1, participants were asked about their expected coparenting relationship and in T2 and T3 they were asked about their present coparenting relationship), and their emotional state (in T1, they were asked about current depressive symptoms, and in T2 and T3, participants were asked to report depressive symptoms directly related to their postpartum experience).
Measures
Prenatal Coparenting Behavior
To assess coparenting behavior in the IDT, we employed the Interactional Dimensions Coding System (IDCS; Julien et al., 1989). This coding system examines various communication behaviors that express emotional content and interpersonal exchanges to tap both individual and interactional (i.e., dyadic) dimensions. Because we wanted to examine how each partner’s PPD is potentially affected by their own and/or their partner’s prenatal coparenting behavior (i.e., actor and partner effects), we only considered the individual variables in this study. These included individual behavioral attempts of each partner to generate positive communication (e.g., support, expressing ideas and suggestions in a constructive manner) or negative communication (e.g., relying on conflictual behaviors such as arguing, and attempts to avoid the interaction) (Kline et al., 2004), as well as their regulation strategies in the stressful context of the IDT. To ensure the specific assessment of coparenting dynamics rather than marital or spousal ones, we coded only the communications and exchanges in the interaction pertaining to the care of the doll (e.g., an expectant father says to his partner, “Your child eats a lot!”, then she replies, “My baby?! And what, when he is calm, he is your baby?”; see further elaboration and additional examples in Shai, 2019).
The individual dimension included five scales, with three positive behaviors (i.e., support and validation, problem solving, and communication skills) and two negative behaviors (i.e., conflict and withdrawal): (1) communication skills reflect the extent to which an individual is clear and constructive in conveying their emotions and thoughts; (2) support and validation refers to the extent to which an individual is being responsive to their partner, employs active listening, and expresses understanding and acceptance toward their partner; (3) problem solving assesses one’s attempts to find positive mutually satisfactory solutions in the stressful situation; (4) conflict refers to the level of hostility, oppositionality, and negative affect displayed by an individual toward their partner during the interaction; and (5) withdrawal reflects the verbal and nonverbal avoidance of a partner from taking an active part in the interaction.
Three coders (graduate students), who were blind to all other aspects of the study, coded the interactions. Prior to starting coding the data, and as part of their training, the coders were given the conceptual definitions of each of the five scales. They then watched examples of behaviors demonstrating each scale and coded them as a whole group before being allowed to code independently. These examples were taken from data collected by the first author for another study. Ratings for each of the five scales were made on a 9-point Likert-type scale ranging from very low (1) to very high (9). Coders were instructed to rate each couple interaction on the nine-point scale for each one-minute interval of the conversation. The final score given to each partner was the mean score of the rates given to all segments on each dimension. Interactions were coded directly from the video recording, and coders coded all videotaped interactions. Coders attended weekly meetings with the first author to discuss disagreements and questions, whenever they came up, until agreement was reached. Using intraclass correlation (ICC), an acceptable reliability was set at ICC = 0.70 (Wahlund et al., 1998). Coders were reliable across all dimensions: ICC was 0.82 for support and validation, 0.74 for problem solving, 0.83 for communication skills; 0.80 for conflict, and 0.93 for withdrawal.
Perceptions of the Coparenting Relationship Pre- and Post-Birth
To assess both prenatal representations of coparenting and postnatal perceptions of the coparenting relationship we used the Coparenting Relationship Scale (CRS; Feinberg et al., 2012), which is a multi-domain self-report questionnaire used to evaluate parental perceptions regarding coparenting relationships. The prenatal version was modified to ask the parents about their ideas and perceptions regarding their future coparenting relationship, once the baby was born. Therefore, the statements in this version were in the future tense.
In both the prenatal and postnatal versions, six sub-scales were assessed: (1) coparenting agreement, which refers to whether parents’ views of how to rear a child are similar; (2) coparenting closeness, which assesses the extent to which partners work together as a team and encourage each other’s development as a parent; (3) coparenting support, which refers to the affirmation of the other partner’s competency as a parent, acknowledging the other’s contributions, and backing up the other’s parenting decisions and authority; (4) coparenting undermining, which pertain to undermining the other parent with criticism, disparagement, and blame; (5) endorse partner parenting, referring to ratifying and approving one’s partner’s parenting; and (6) division of labor, referring to the way partners divide childrearing labor responsibilities. Ratings were made on 7-point Likert-type scales ranging from 1 (not true at all about us) to 7 (very true of us). High scores on the agreement, closeness, support, endorse, and division scales reflected a more positive coparenting relationship. In contrast, a high score on the undermining scale reflected a more negative coparenting relationship. We used the global CRS score, which is the mean of all the items (the undermining scale items were reverse-coded prior to combining the scales on the global score; prenatal: M = 4.78; SD = 0.65; α = 0.91 for fathers; M = 4.89; SD = 0.62; α = 0.92 for mothers; postnatal: M = 4.98; SD = 0.62 for fathers; M = 5.01; SD = 0.64 for mothers).
Depressive Symptoms
To assess PPD, we employed Cox et al.'s (1987) Edinburgh Postnatal Depression Scale (EPDS). Consists of 10 statements on a scale ranging from 0 to 3, the EPDS asks parents to indicate to what extent each statement corresponds with how they have been feeling during the past week (e.g., I have been able to laugh and see the funny side of things, with 0 = as much as I ever could to 3 = not at all). Summing scores could range from 0 to 30 with higher scores indicating a higher intensity of depressive symptoms (M = 5.19; SD = 3.33; α = .85 for fathers; M = 5.95; SD = 4.07; α = .89 for mothers). To assess a baseline of the participants' depressive symptoms pre-birth, we used the depression sub-scale from Derogatis and Spencer’s (1982) Brief Symptom Inventory (BSI) on T1. This 6-item sub-scale ranges from 0 (not at all) to 4 (all the time) to capture participants' depressive symptoms over the preceding seven days (e.g., feeling no interest in things). Each participant’s final score is the sum of their responses, that can range from 0 to 24 (M = 3.69; SD = 3.32; α = .79 for fathers; M = 4.45; SD = 3.47; α = .82 for mothers).
Results
Following previous studies (e.g., Takeishi et al., 2021), and because the literature on PPD points to variability in the onset, intensity, and course of development of PPD among individuals (Goodman, 2004; Kettunen et al., 2014), we have explored our research hypotheses at each of the study time point (i.e., 3 and 6 months postpartum) separately. This way we were able to identify the unique relations between the study variables at 3 and 6 months after the birth independently. With much research points to 3 months postpartum as a timeframe within which more than 50% of affected women and men begin to develop depressive symptoms, and many experience decrease in symptoms by the time the baby is 6 months of age (Vismara et al., 2016), we wanted to make sure we document the associations between the study variables in each of the two different time points individually.
Descriptive Statistics
Mean Scores of First-Time Mothers’ and Fathers' PPD at 3 and 6 months postnatally, prenatal coparenting communication skills, support and validation, withdrawal, conflict behaviors, and problem solving attempts.
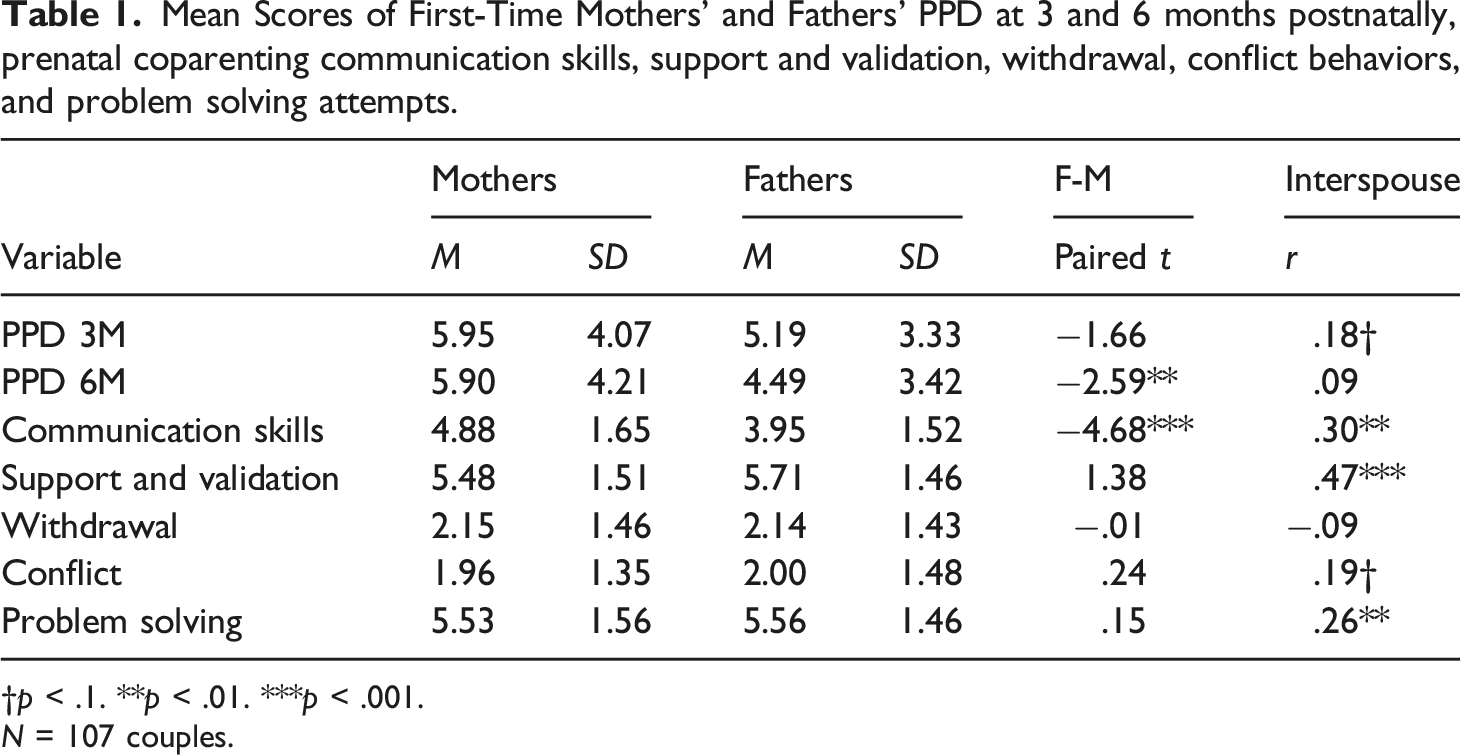
†p < .1. **p < .01. ***p < .001.
N = 107 couples.
Substantive Analyses
We used multilevel regression models to probe actor and partner effects (see Boman et al., 2012; Hong & Kim, 2019). Multilevel modelling (MLM) is also useful in accommodating missing data (Knobloch & Theiss, 2010), especially in longitudinal designs (Estlein et al., 2022).We used the Hierarchical Linear Model (HLM8.2) software, which is designed to accommodate nonindependent or nested data (Bryk & Raudenbush, 1992), for analyzing actor and partner effects in couples during the transition to parenthood. Missing data were handled using Full Information Maximum Likelihood (FIML) estimation. We evaluated our hypotheses using a two-level model, with participants' individual variables (i.e., PPD, actor’s and partner’s prenatal coparenting behaviors, prenatal depression, prenatal coparenting expectations, and postnatal perceived coparenting quality) at Level 1 and stable individual variables and dyadic characteristics (i.e., age, education, sex of the child, and family income) at Level 2. To assess the effects of actor’s and partner’s prenatal coparenting behaviors on PPD among first-time mothers and fathers above and beyond all other variables, we constructed four sets of models where the outcome variable in each model was either father’s or mother’s PPD at 3 or 6 months post-birth. In each of the models, the predictors were one behavioral aspect in the actor’s and partner’s prenatal coparenting (e.g., actor’s and partner’s communication skills, actor’s and partner’s withdrawal), entered as group mean-centered, controlling for all other variables, including prenatal depression levels, prenatal coparenting expectations, postnatal coparenting quality, and individual and family characteristics.
Multilevel Analysis Regressing PPD at 3 months post-birth on Five Domains of Prenatal Coparenting Behavior.
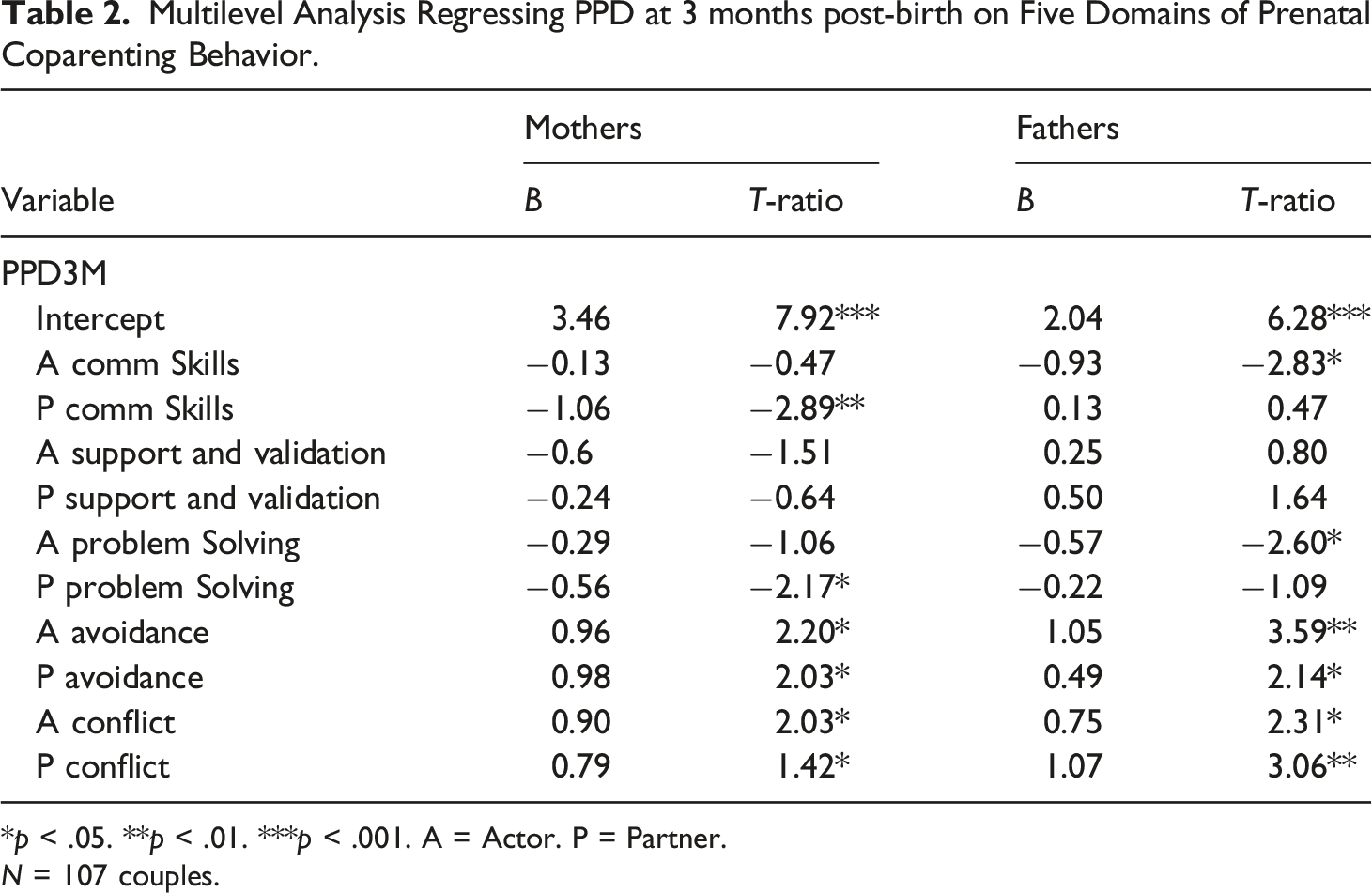
*p < .05. **p < .01. ***p < .001. A = Actor. P = Partner.
N = 107 couples.
Multilevel analysis Regressing PPD at 6 months post-birth on Five Domains of Prenatal Coparenting Behavior.
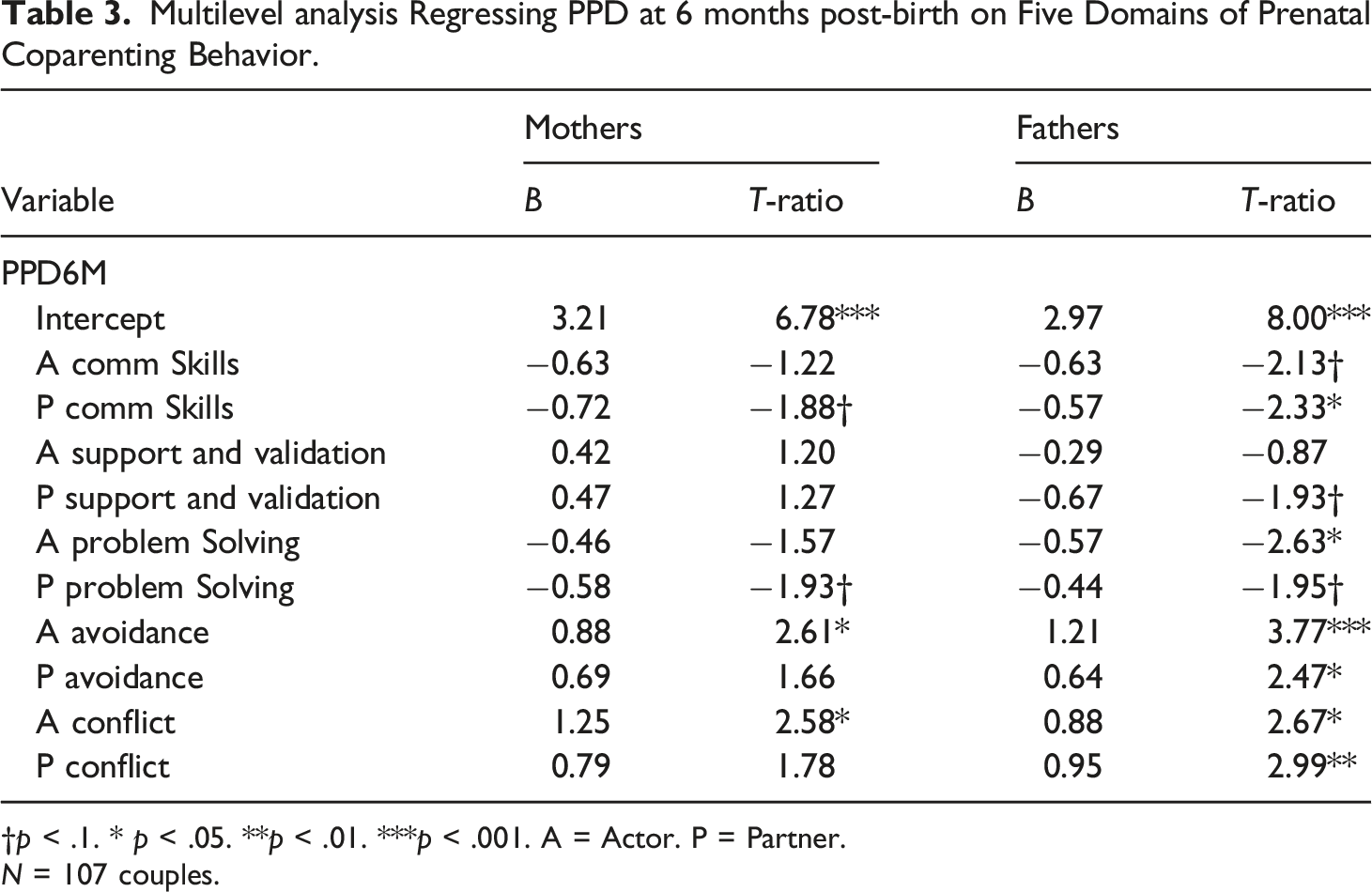
†p < .1. * p < .05. **p < .01. ***p < .001. A = Actor. P = Partner.
N = 107 couples.
In terms of the association between prenatal positive coparenting behaviors and PPD among first-time parents (H2), results showed that, above and beyond prenatal depressive levels, partner’s PPD, perceived prenatal and postnatal coparenting, and parents' age, education, and family income, father’s prenatal communication skills were associated with low levels of PPD at 3 months post-birth among both fathers and mothers (see Table 2). None of the covariates altered the value of the intercept for mothers or fathers. Father’s prenatal communication skills were associated with low levels of PPD among both fathers and mothers also at 6 months post-birth, and mother’s prenatal communication skills were negatively associated with her partner’s PPD at that time point, but not with her own (see Table 3). Also at 6 months post-birth, mother’s support and validation during the prenatal coparenting interaction was negatively associated with her partner’s PPD, father’s prenatal problem solving was negatively associated with both his own and his partner’s PPD, and mother’s prenatal problem solving attempts were negatively associated with her partner’s PPD (Table 3). None of the covariates altered the value of the intercept for mothers or fathers.
Discussion
The main goal of this study was to explore associations between behavioral aspects of prenatal coparenting among expectant first-time mothers and fathers and PPD. Prior research has documented prenatal individual predictors of PPD, such as the parent’s depression before the birth and their psychiatric history, and couple-level predictors, such as one’s partner’s PPD and postnatal coparenting dynamics; however, little is known about prenatal couple-level predictors of PPD, such as prenatal coparenting. Family systems theory and developmental frameworks suggest that the transition to parenthood unfolds over time. Indeed, evidence suggests that the coparenting relationship starts developing as early as during pregnancy (e.g., Kuersten-Hogan, 2017) thus, our goal in the current study was to explore potential associations between specific behavioral aspects of the coparenting relationship in its early stages (i.e., prenatally) and PPD among first-time mothers and fathers.
Our findings showed that both negative and positive prenatal coparenting behaviors were uniquely predictive of PPD among first-time parents. Specifically, both fathers' and mothers' negative prenatal coparenting behaviors (i.e., withdrawal and conflict) predicted their own and their partner’s PPD. Positive prenatal coparenting behaviors (i.e., communication skills, support and validation, and problem solving attempts), however, were mostly predictive of father’s, but not mother’s low PPD. Specifically, mothers' positive behaviors predicted only her partner’s – but not her own – PPD, and only at 6 (but not at 3) months post-birth, whereas fathers' support and validation as well as problem solving attempts predicted, in addition to his own PPD, also his partner’s PPD, at 3 and 6 months post-birth. These findings, which were evident even when controlling for one’s prenatal depression levels, partner’s PPD, expectations of prenatal and appraisals of postnatal coparenting, and parents' sociodemographic characteristics, add to the existing literature by highlighting first, associations between prenatal coparenting behaviors and postnatal mental outcomes across the transition to parenthood, second, how both positive and negative aspects of coparenting are significant in predicting PPD, and finally, how both one’s own (actor) and their partner’s behaviors are associated with PPD.
Prenatal Coparenting Behaviors and PPD
First, we found associations between prenatal coparenting behaviors and postnatal depression among first-time mothers and fathers. The associations between postnatal coparenting dynamics and PPD in the existing literature (e.g., Takeishi et al., 2021) call for further understanding of the significance of coparenting for parents' postpartum mental functioning as early as possible, even prenatally. With studies documenting associations between prenatal coparenting behaviors and various postpartum couple and family features (Kuersten-Hogan & McHale, 2021), identifying prenatal coparenting behaviors that may contribute to or buffer against PPD is a path worth taking that can inform early interventions and prevention programs to improve mental health among parents by helping them pay attention to such behaviors. In this sense, our findings provide an initial contribution to consider such programs, suggesting that the ways expectant parents manage their coparenting interaction at the early stages of this relationship have consequences for their emotional experience after the child is born.
Importantly, whereas previous studies have pointed to associations between prenatal and postnatal coparenting dynamics (e.g., Albenburger et al., 2014; Kuersten-Hogan, 2017), the current findings extend the literature on prenatal coparenting and postnatal implications in the form of mental and health conditions, namely, PPD. Reflecting family systems thinking, the findings also highlight the significance of prenatal interpersonal relational processes for PPD, as research has mostly illuminated individual characteristics, such as genetics, psychiatric history, and biological predisposition, as predictors of PPD (Osborne et al., 2016; Viktorin et al., 2016).
Prenatal Negative and Positive Behaviors Predicting PPD
Second, our findings highlight the role of both negative and positive aspects of prenatal coparenting behaviors in first-time parents' mental health by potentially contributing to or counteracting PPD. When parents and their partner presented more withdrawing and conflictual (i.e., negative) behaviors before the birth, they reported higher levels of depressive symptoms after the birth, and lower levels of PPD when they exhibited more constructive communication and positive problem solving attempts (i.e., positive) prenatally. For fathers only, partner’s prenatal support and validation predicted lower PPD as well. These results support prior research that found associations between positive prenatal characteristics of coparenting, such as alliance and coparental warmth, and postnatal family dynamics (Favez et al., 2012; 2013), but further emphasize the importance of considering negative aspects of prenatal coparenting dynamics as well. These findings also support family systems theory’s conceptualization of feedback loops, suggesting that couples who rely on more open and constructive communication are able to more effectively and flexibly adapt to the transition to parenthood than those who communicate more rigidly during this transition (Fiese et al., 2019).
In this sense, our results also extend findings from previous studies, that showed how both positive (Takeishi et al., 2021) and negative (e.g., Elliston et al., 2008; Volling et al., 2021) aspects of postnatal coparenting dynamics are associated with PPD, by highlighting their significance already during pregnancy. Identifying both negative and positive components of coparenting behavior in the prenatal stage can help expectant parents and professionals who work with them to fine tune their coparenting cooperation as early as possible, to promote better adjustment to the transition to parenthood.
Actor and Partner Effects on Fathers' and Mothers' PPD
Finally, our results pointed to both similarities and dissimilarities in the associations between specific prenatal coparenting behaviors and fathers' and mothers' own and partner effects on PPD. Specifically, postpartum depressive symptoms were higher among both fathers and mothers who presented, as well as their partner, avoidant and conflictual (i.e., negative) behaviors prenatally. Fathers and mothers were also similar in terms of the associations between paternal prenatal constructive communication and problem solving (i.e., positive) behaviors and PPD. First-time fathers and mothers were different, however, in terms of the effect maternal positive coparenting behaviors had on their PPD, with fathers showing lower PPD at 6 months after the birth but not mothers. In other words, whereas for fathers, all negative and positive prenatal coparenting behaviors were associated with postpartum depressive symptoms, post-birth levels of depression among mothers were associated with actor and partner negative prenatal coparenting patterns and only partner positive behaviors.
These results may suggest that one’s partner’s behavior in the prenatal coparenting dynamics is particularly important in contributing to their emotional experience, as both first-time fathers' and mothers' PPD was associated with negative and positive partner behavior. This finding reflects the nature of the coparenting dynamics as an interpersonal exchange, where individuals are emotionally reactive to their partner’s behavior. Within this relational context, parent partners are required to interact, which can be experienced as either supportive or interfering (Tissot et al., 2017). Although one’s own (actor) behavior in the prenatal coparenting interaction is also important, it seems that among first-time mothers it is their partner’s behavior that plays a significant role in explaining their postpartum depressive experience, as their own positive behavior in the prenatal coparenting interaction was not predictive of their PPD.
In this sense, it is interesting to note that whereas expectant mothers' own positive behavior in the prenatal coparenting interaction was not associated with their PPD, their own negative behavior was. Prior research showed that first-time mothers are more reactive than fathers to conflictual perinatal coparenting, and maternal adjustment, relationship satisfaction, and PPD were all found to be negatively associated with postnatal couple conflict (Feeney et al., 2001; Halford et al., 2010; Solmeyer & Feinberg, 2011). Our findings reflect, as well as extend previous findings by suggesting that first-time mothers may be reactive to couple conflict in the context of coparenting, and to their own contribution to such episodes, even prenatally. The longitudinal nature of the transition to parenthood is reflected in the potential effect of prenatal coparenting conflictual behaviors, presented by both actor and partner, on postpartum difficulties, such as PPD, among first-time mothers. Whereas our interpretations are speculative and encourage yet further research, professionals are encouraged to pay attention to expectant mothers' negative coparenting behaviors during pregnancy, as they may be a predictor of maternal PPD.
Strengths, Limitations, and Future Research
The current study has considerable strengths, including its longitudinal mixed-method design and its inclusion of both partners, which yielded dyadic data that allowed us to probe into complex systems-oriented research inquiries and discover associations between prenatal and postnatal experiences among first-time parents. Importantly, our study adds to the limited number of observational studies that explored prenatal observed coparenting interaction predictors of postpartum functioning (Kuersten-Hogan & McHale, 2021).
Despite its strengths, this study has some limitations that need to be acknowledged. First, the generalizability of the findings is somewhat limited as our sample included only low-risk community-based heterosexual couples. It may be that higher-risk couples, who may show higher prevalence rates of PPD (Horowitz et al., 2011), demonstrate different patterns of prenatal and postnatal coparenting dynamics that may associate differently with PPD. Similarly, same-sex couples may or may not employ similar coparenting dynamics or have similar or dissimilar prenatal coparenting expectations as different-sex first-time parent couples, which may result in different patterns of associations between the studied mechanisms. Second, the participants in our sample had relatively low levels of PPD, which might have deprived us from identifying some effects of prenatal coparenting dynamics on postpartum depressive symptoms. Although collecting data from parents who present more severe depressive symptoms is extremely complex (Tissot et al., 2017), such task should be considered in future research. Related, we did not use the same measure to assess depressive symptoms pre- and post-birth. Future research may benefit from employing the EPDS in the prenatal assessment as well, as it is valid to detect prenatal depressive symptoms as well (Cox et al., 1996). Finally, although we employed a longitudinal design, that provided rich information about the experiences and behavior of the participants in this study, we could have benefited from assessing the studied variables within less-spaced time points (e.g., at 12 or 18 months postpartum). Such examination could have yielded more nuanced information on how PPD among first-time parents unfolds over the transition to parenthood and on the extent to which prenatal coparenting dynamics predict depressive symptoms at different stages during that intense time.
In light of this study’s findings, strengths, and limitations, future research should explore questions on the associations between the different components of prenatal coparenting dynamics and PPD among first-time parents in more diverse family settings, such as same-sex couples, adoptive parents, and clinical samples. Additionally, future studies could benefit from following parents across the transition to parenthood at closer time points to identify unique effects of prenatal coparenting dynamics on PPD over time. Finally, due to its multifaceted nature, future researchers should look further to examine the associations between different coparenting domains and postpartum psychological and health outcomes. Advancing our understanding of the ways that the emerging coparenting relationship is associated with the wellbeing of first-time parents will both extend theory and promote the development of prevention and intervention programs for families across this life-changing transition. Specifically, professionals who work with expectant parents are encouraged to highlight both the supportive and conflictual aspects of coparenting as early as during pregnancy, and consider the divergent effects they have on first-time fathers and mothers. Such work can have significant implications for first-time parents, their relationship, and their developing bonding with their infant.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Israel Science Foundation (No. 1888/14)
Data availability
The data used in the research cannot be publicly shared but are available upon request. The data can be obtained by emailing to the corresponding author at