
Abstract
Despite the incredible challenges of caring for a family member with Alzheimer’s disease or a related dementia, many dementia family caregivers exhibit resilience. Framed by the communication theory of resilience, this study examines how resilience processes unfold within dementia caregivers’ relationships with their family member, and dementia caregivers’ experiences of resilience. Analysis of 27 interviews with adult children and spousal caregivers revealed acknowledging dementia as an actor in the relationship as a central facilitating mechanism that enabled caregivers to enact other communicative resilience processes within their relationship. Resilience processes were enacted through shifting blame to dementia, accommodating dementia, and relying on memories. Caregivers experienced resilience through personal growth, enhanced relational closeness, and ambivalent resilience. We discuss implications for dementia caregiver resilience and forward facilitating mechanisms as an extension of communication resilience theorizing.
Keywords
Introduction
Dementia family caregivers experience incredible strain and change as the symptoms of dementia gradually alter the relationship with their family member with dementia (referred to hereafter as the family member). In this study, the term dementia caregivers refers to adult children or spousal caregivers to a person with dementia. Symptoms such as impaired logical processing, behavior changes, diminished communication ability, and memory loss create frustration and guilt, altered relational roles, and a sense of loss for family caregivers (Adams, 2006; Walters et al., 2010). Despite experiencing incredible challenges, some dementia caregivers exhibit remarkable resilience, experiencing personal growth and enhanced relational closeness with their family member through providing care (Netto et al., 2009; Yu et al., 2018). Resilience refers to the ability to positively adapt to endure or even thrive in the face of challenges (Windle, 2011). Dementia caregivers who exhibit resilience experience lower burden and depression, and greater quality of life despite their family member’s behavioral symptoms (Kalaitzaki et al., 2022; McKenna et al., 2022). Resilient caregivers are able to adapt to the challenges of dementia to maintain their personal wellbeing and preserve a sense of closeness in their relationship.
In this study, we draw upon communication theorizing to examine how caregiver resilience unfolds in relationships impacted by dementia. Across disciplines, resilience has been studied as a personal trait, a process, and an outcome (Masten, 2001; Windle, 2011) that functions on an individual level, between relational partners, or in a broader community (Jordan, 2004; Kimhi, 2016). Buzzanell’s (2010) communication theory of resilience (CTR) proposes that resilience is “constituted in and through communicative processes that enhance people’s abilities to create new normalcies” (p. 9). This theory takes a process-focused approach to resilience, suggesting that resilience is not a trait that individuals posess but a process that unfolds through communicative behavior in the face of distruption. The CTR “situates resilience in interactions and relationships” (Buzzanell, 2018, p. 99), providing a framework for examining the communication enacted by individuals or between relational partners that promote resilience. Taking this lens, we seek to understand how dementia caregiver resilience unfolds within the relationship with their family member and dementia caregivers’ experiences of resilience within these relationships.
Because the relationship with the family member with dementia is often the central site of change and stress for dementia caregivers, we position caregiver resilience as springing from their communication within these relationships. Qualities of the caregiver-care recipient relationship have been identified as a key factor influencing caregiver resilience (Cherry et al., 2013). For example, reciprocity and retaining a sense of togetherness promote resilience for couples impacted by dementia (Conway et al., 2020), and positive communication patterns, family connectedness, and social support promote resilence for adult child caregivers (Deist & Greeff, 2017). Yet less is known about the process through which family caregivers enact these beneficial behaviors within their relationships. Understanding how communicative resilience unfolds within dementia caregiving relationships will provide greater insight into the relational adjustments that promote positive interactions and the continuance of relationships despite the incredible changes and losses of dementia. This study will also shed light on the interconnected nature of communcation, relationsihps, and resilience in end of life care contexts.
Dementia family relationships as a site for stress and resilience
The relationship between a caregiver and their family member with dementia is often the source of incredible stress and thus might be an important site in which to consider the construction of resilience. Progressive symptoms of cognitive decline transform the relationship between the caregiver and their family member (Adams, 2006; Walters et al., 2010). Although the relational experiences of adult children and spousal caregivers are considerably different prior to dementia, the relational changes experienced in dementia are consistent across both groups of caregivers. Spousal relationships are marked by interdependence, sexual intimacy, co-residence, sharing of household tasks, and reliance on one another for support. In contrast, adult children generally share a more independent connection with their parents and are more likely to have other family and work responsibilities outside of caregiving (Wang et al., 2011). Adult children might also anticipate the decline and eventual death of their aging parent, whereas spousal caregivers might more keenly feel the loss of a relational future interrupted by dementia. Despite these relational differences, adult children and spousal caregivers both experience the same relational changes as the disease progresses: altered relational roles and a sense of relational loss.
The increasing dependence of the family member with dementia shifts the established roles within the relationship. Research with adult children has referred to this change as a “role reversal” because the responsibilities of caregiving are sometimes similar to those of parenting (Dempsey et al., 2020). For example, adult children caring for a parent with dementia report changes such as having to correct or reprimand their parent, making decisions for them, and controlling their private information (Adams, 2006; Miller-Ott, 2020). These interactions vary greatly from the child-parent relationship established prior to dementia and shift the nature of the relationship. Spousal caregivers describe this relational role change as a shift from spouse to caregiver which unfolds through monitoring/removing their partner’s driving privileges, changing household responsibilities, a decline in romance in the relationship, and increasingly severe symptoms (Cooper et al., 2022). For both adult children and spousal caregivers, shifting relational roles alter the nature of their relationship.
In addition to shifting relational roles, both adult children and spousal caregivers experience a sense of relational loss. Symptoms of dementia such as memory loss and personality change leave many family caregivers with the sense that the person they knew prior to dementia is gone. Spousal caregivers describe tension between who their spouse was prior to dementia and who they are in the present creating a loss of both their partner and their marriage (Baxter et al., 2002; Evans & Lee, 2014). For adult children, decline in competencies, changes in personality, and lack of recognition lead to this sense of loss (Aslett et al., 2019). Boss (2009) has categorized this type of relational loss as ambiguous loss because the person is mentally absent but physically present. Dementia caregivers must live in this ambiguous loss even while continuing to interact with their family member on a regular basis. Thus, we center the construction of resilience as driving from caregivers’ ongoing communication amidst the change and loss within their relationship with their family member. To this end, we turn to the CTR to guide our inquiry into dementia caregivers’ communicative resilience within the relationship with their family member.
Communication theory of resilience
The communication theory of resilience (CTR) suggests that resilience is constructed through language and communication that enables individuals to “constitute the new normal of their lives after disruption, loss, trauma, and disaster” (Buzzanell, 2018, p. 100). The CTR proposes that resilience is initiated by a trigger event that disrupts the established norms and routines of an individual, family, organization, or community. Trigger events can be singular or accumulated over time (Buzzanell, 2018), and individuals can experience multiple triggers simultaneously (Geary et al., 2023). Trigger events differ across contexts. For example, parents of children with hearing loss experience medical screening, diagnosis, decision making, and costs, as well as confrontations about their choices, as triggers (Scharp et al., 2023). US migrants experience bureaucratic complexities, cultural differences, and distance from loved ones as triggers (Scharp et al., 2021). In the context of dementia, the diagnosis might be considered a trigger event. However, the ongoing progressive nature of dementia means that dementia caregivers often experience multiple compounding stressors over time (i.e., primary and secondary stressors, Pearlin et al., 1990) and several relational turning points as the disease progresses (Cooper et al., 2022). Considering the progressively changing nature of dementia caregiving relationships, dementia caregivers might experience multiple, compounding triggers as the disease progresses.
Following a trigger event, the CTR asserts that resilience unfolds through five communicative processes: (1) crafting normalcy, drawing on language and routines to create a sense of normal despite disruption; (2) affirming identity anchors, communicating in ways that support central aspects of one’s own or others’ identities; (3) maintaining and using communication networks, seeking support from one’s established social network; (4) putting alternative logics to work, reframing a situation to gain new perspectives on contradictory, ambiguous, or paradoxical circumstances; and (5) foregrounding productive action while backgrounding negative feelings, acknowledging the legitimacy of negative emotions while taking action to manage challenging circumstances (Buzzanell, 2010, 2018). These communicative processes are interwoven, meaning that they operate simultaneously and sometimes interdependently in response to trigger events (Scharp et al., 2021; Tian & Bush, 2020), and they can be enacted individually, dyadically, or on behalf of others (Lillie et al., 2018; Scharp et al., 2023). Enacting these resilience processes is associated with improved health management, better mental health, and positive evaluations of dyadic coping (Kuang et al., 2023; Lillie et al., 2021; Venetis et al., 2020). These communication processes enable individuals to “talk normalcy into being” (Buzzanell, 2010, p. 4) in the face of challenge and disruption. We build from this theorizing to investigate dementia caregiver resilience.
The current study
Buzzanell (2010) describes resilience as “unfolding over time and through events, evolving into patterns, and dependent on contingencies” (p. 2). The main contingency in dementia care is the impact of the disease on the family member. We sought to examine the patterned way in which dementia caregiver resilience unfolds within the relationship with the family member, and the ways in which caregivers experience resilience. The CTR establishes a pattern of resilience that entails the occurrence of some trigger event and the enactment of resilience processes in response (Buzzanell, 2018). The prolonged and increasingly severe nature of dementia might alter this pattern. For example, caregivers experience multiple relational turning points as the disease progresses (Cooper et al., 2022) which might serve as a series of trigger events each requiring the enactment of different resilience processes. Boylstein and Hayes (2012) characterized the relational experience of dementia as a repeated pattern of disruption and reconstruction of relational closeness. This pattern suggests that trigger events and caregivers’ enactment of communicative resilience processes might ebb and flow as they seek to construct relational closeness. Further, as a terminal illness, dementia brings with it the certainty that the relationship will end with the death of the family member who has dementia (Cooper & Pitts, 2022). Anticipating the death of their family member might impact which communicative resilience processes caregivers use and how these processes unfold. Thus, to better understand the patterned nature of the dementia caregiver resilience, we pose the first research question:
How do trigger events and resilience processes unfold to promote dementia caregiver resilience within the relationship with their family member? In addition to examining the patterned nature of resilience, we also sought to examine caregivers’ experiences of resilience in dementia. Resilience can be observed when caregivers maintain physical and/or psychological health despite the challenges of caregiving (Harmell et al., 2011), however, the experience of dementia likely extends beyond physical and mental health. Some caregivers report feelings of accomplishment, personal growth, gains within the caregiver-care recipient relationship, broader family cohesion, and spiritual development as positive aspects of care which might reflect an experience of resilience (Netto et al., 2009; Yu et al., 2018). For couples impacted by dementia, creating a sense of normalcy and maintaining togetherness was perceived as resilience (Conway et al., 2020). These studies suggest that experiences of resilience forwarded by the CTR (i.e., constructing normalcy) might be central to dementia caregivers’ resilience. To better understand caregivers’ experiences of resilience, we pose the second research questions:
In what ways do dementia family caregivers experience resilience?
Method
Participants and procedure
Data for this study consisted of in-depth interviews with 26 dementia family caregivers who were recruited as part of a larger project focused on dementia caregiver resilience and wellbeing. To participate, individuals had to be (1) over age 18, (2) living in the US, (3) fluent in English, and (4) the primary caregiver of a family member who had been living with symptoms of dementia for at least three years. After receiving IRB approval, recruitment for this project occurred through online caregiving research boards hosted by the Family Caregiver Alliance 1 and by the Alzheimer’s Prevention Registry, 2 and through local organizations in the Southwest region of the US focused on supporting individuals with dementia and their caregivers. All participants completed a short consent and demographic survey before participating in the interview. Interviews were conducted over the phone (n = 13), via Zoom (n = 12), and in-person (n = 1) and lasted 51–116 minutes (M = 74.69, SD = 16.20). During the interview, participants were asked to describe their relationships and communication patterns prior to dementia onset, shortly following the recognition of symptoms, and over the last three months. Participants received a $10 Amazon gift card for participating. Interviews were transcribed using transcription software (https://otter.ai) and participant names were replaced with pseudonyms during transcription.
Demographics.
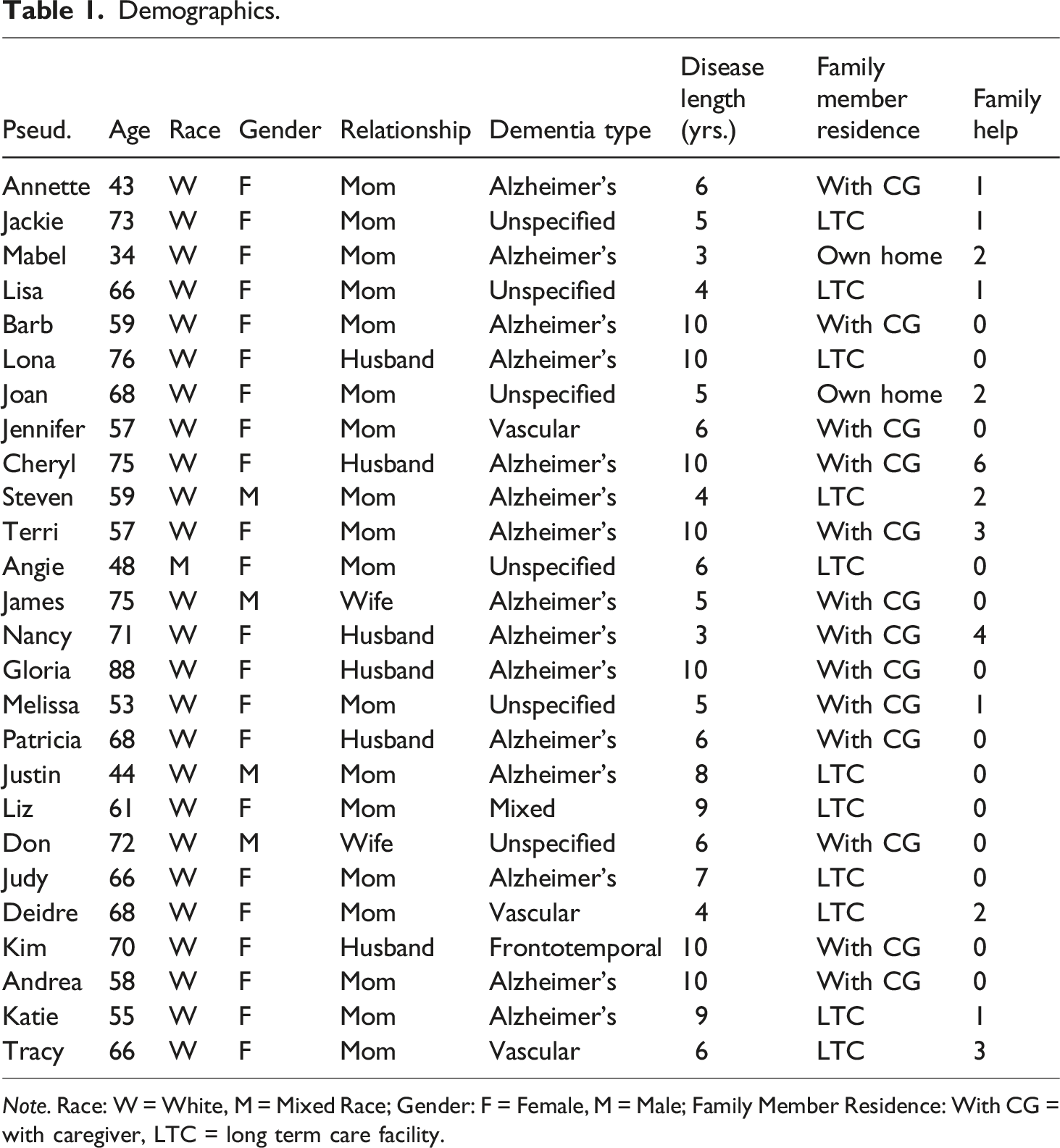
Note. Race: W = White, M = Mixed Race; Gender: F = Female, M = Male; Family Member Residence: With CG = with caregiver, LTC = long term care facility.
Data analysis
The first author conducted the analysis supported by regular peer debriefing with the second author to discuss emerging patterns in the data, refine categories, and ensure rigorous analysis (Lincoln & Guba, 1985). Assisted by NVivo software, the data were analyzed using constructivist grounded theory (Charmaz, 2014). Constructivist grounded theory was used because it provides a means for examining patterns and processes by identifying links between categories/themes with the goal of developing an emergent theory. This approach allowed us to examine the pattern through which resilience processes unfold (RQ1). The analysis began with becoming familiar with the data through reading and rereading the interviews. The next step was open coding, which breaks the data into manageable pieces (i.e., codes) that can be compared and categorized. Open coding involves identifying relevant pieces of data and labeling them to identify the meaning of the code (Strauss & Corbin, 1990). Whenever possible we used in vivo coding, labeling codes with participants’ own language, to keep the coding grounded in the participants’ experiences (Creswell, 2013). Open coding was guided by the goal of identifying dementia-related disruption and the communicative behaviors enacted in response (RQ1), as well as caregivers’ experiences of resilience (RQ2). This process yielded 1084 codes.
The second stage of analysis involved constant comparison between codes to identify conceptual patterns across the dataset (Charmaz, 2014). This was an iterative process that began with grouping conceptually similar codes into categories, then comparing categories and grouping conceptually similar categories into broader themes. Themes were deemed complete when they met the following criteria: (1) reoccurrence, the theme appeared across multiple interviews in the dataset; (2) repetition, the theme appeared multiple times within an interview; and (3) forcefulness, the theme appeared in participants’ talk through vivid, dramatic, and evocative language (Owen, 1984). Because both adult children and spousal caregivers were included in this study, we carefully examined the codes contributing to each theme looking for patterns of difference between participants caring for a parent versus those caring for a spouse. All themes were represented with equal repetition, reoccurrence, and forcefulness by adult children and spousal caregivers, so data from all caregivers were kept together. After identifying initial categories/themes we engaged in an additional step of comparison, theoretical coding, to better understand the process through which dementia caregiver resilience unfolds. This process involves comparing emergent categories/themes to identify the relationships between them (Charmaz, 2014). Theoretical coding revealed a distinctive pattern through which caregivers’ communicative resilience unfolds.
We took several measures to ensure the trustworthiness, or quality, of the analysis (Lincoln & Guba, 1985). The first author kept an audit trail, or detailed notes, to document analytic decisions and theme development (Rodgers & Cowles, 1993) this facilitated regular peer debriefing to ensure rigorous analysis (Lincoln & Guba, 1985). We used negative case analysis by seeking codes that did not align with the emerging categories/themes and using them to revise and refine the themes (Lincoln & Guba, 1985). This process added greater nuance to the themes and allowed us to honor the varied experiences of dementia caregivers. In reporting the findings, we used thick description and evocative exemplars to richly capture participants’ experiences and increase the transferability of the findings (Geertz, 1973; Tracy & Hinrichs, 2017). Finally, we engaged in member checking to ensure that the findings aligned with participants’ lived experiences (Lincoln & Guba, 1985). Member checking involves sharing findings with participants and inviting them to share their reactions to the findings. We shared the findings with all participants, 11 of which responded. These participants affirmed that the findings aligned well with their experiences. A few participants also shared additional insights which have been incorporated into the reporting of the findings.
Findings
Our analysis revealed the patterned way in which dementia caregiver resilience unfolds within the relationship with their family member (RQ1), and the ways in which caregivers experience resilience (RQ2). The pattern of caregiver resilience will be presented first, followed by caregivers’ experiences of resilience. Throughout the findings, caregivers’ relationships with the family member are indicated parenthetically. Figure 1 provides a visual summary of the findings. Summary of Findings. Note. Theme names are bolded, CTR trigger and process labels appear in italics.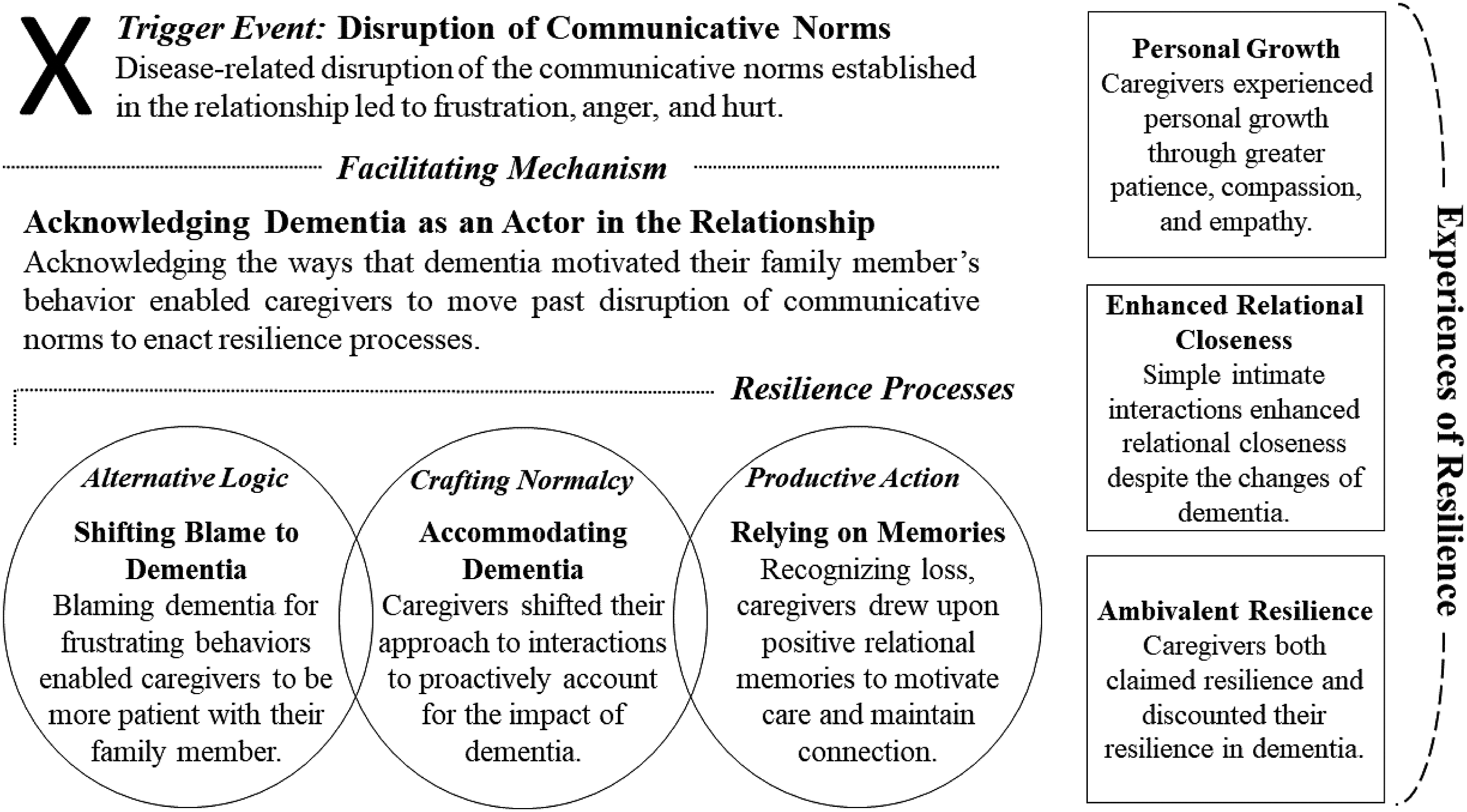
The patterned nature of dementia caregiver resilience
As proposed in the CTR (Buzzanell, 2010, 2018), dementia caregiver resilience was initiated by a trigger event (disruption of communicative norms) and enacted through three communicative behaviors that map onto CTR processes: shifting blame to dementia, accommodating dementia, and relying on memory. Extending the CTR, the analysis revealed an essential facilitating mechanism, acknowledging dementia as an actor in the relationship, which enabled caregivers to move beyond disruption to enact communicative resilience processes. This facilitating mechanism was central to the construction of caregiver resilience within their relationships (see Figure 1).
Disruption of communicative norms
Dementia caregiver resilience was triggered by disease-related disruption of the communicative norms established in the relationship prior to dementia onset. This trigger event became increasingly salient over time as dementia impacted the family member. Cheryl (spouse) described this disruption of communicative norms, “They don’t always respond to what you’ve explained to them and they take everything in a different light than what’s normal.” Cheryl’s use of the word “normal” illustrates the extent to which dementia-related communication changes violated communication norms in her relationship. Caregivers attempting to relate as they had prior to dementia experienced confusion and frustration when their family member did not respond as expected. Gloria (spouse) explained, “Well, of course, the first thing you do is you try to reason, but then, you can’t reason with someone with dementia.” Similarly, Judy (daughter) explained, “The first thing you want to do is correct them, and it just gets frustrating when you try and do that.” Without understanding the extent to which dementia alters behavior, many caregivers responded to these changes with anger. Andrea (daughter) recalled, “At first it was just utter frustration where I’d yell, and the only thing that was accomplishing was getting my blood pressure to go through the roof. I wasn’t getting anywhere. Then I had to learn to adapt.” As Andrea suggests, the futility of these interactions helped caregivers recognize the impact of dementia and prompted them to adopt an alternative view of their relationship.
Acknowledging dementia as an actor in the relationship
Acknowledging dementia as an actor in the relationship was an essential change in perspective that occurred as caregivers recognized that their family member’s uncharacteristic behavior was being driven by the disease. Acknowledging dementia as an actor in the relationship aligns with the CTR process putting alternative logics to work; however, we position this process as a facilitating mechanism because it was essential in enabling caregivers to move from the frustration of disrupted norms to the enactment of communicative resilience processes (see Figure 1). Acknowledging dementia as an actor in the relationship occurred gradually as caregivers came to fully recognize the degree to which dementia influenced their family member’s behavior. We refer to this recognition as acknowledging dementia as an actor in the relationship because many caregivers described dementia as if it was a third party in the relationship influencing interactions with their family member. For example, statements like “this is the disease talking” (Mabel, daughter), or “he wouldn’t hit me, but his disease might hit me” (Kim, spouse) give agency to dementia as an actor in the relationship. Acknowledging dementia and giving it agency allowed caregivers to separate their family member’s current behavior from their past self and enabled caregivers to adjust their expectations for interactions with their family member. Nancy (spouse) described this recognition: As I more and more fundamentally get that [his behavior] is not volitional. I’m much more forgiving. It’s like asking a person who has no legs stand up straight. When you think they have two legs, it’s different. As I see there’s only one leg, I have different expectations.
This recognition of the extent to which dementia influenced their family member’s behavior was an essential facilitating mechanism that enabled caregivers to adapt their relational communication to enact communicative resilience processes.
Communicative resilience processes
Acknowledging dementia as an actor in the relationship enabled caregivers to enact three communicative behaviors that map onto CTR processes: shifting blame to dementia, accommodating dementia, and relying on memory (see Figure 1). These communicative behaviors represent new ways of interacting and relating within the disruption of dementia.
Shifting blame to dementia
Acknowledging dementia as an actor in the relationship enabled caregivers to shift the blame for frustrating behaviors from the family member to dementia. Shifting blame to dementia reflects the CTR process putting alternative logics to work. Andrea (daughter) explained how she adopted this alternative logic, “I was raging at the person for something that wasn’t their fault. And the light bulb went off. I was blaming them for their disease… I realized there was nothing they could do and I stopped yelling.” Shifting the blame to dementia enabled caregivers to respond with greater patience and compassion for their family member. Joan (daughter) explained, “I’m really not upset with her. I’m upset with the dementia… I try to remember that this is not her fault, there’s no control over it, so I need to be as kind and patient as I can.” As this quote suggests, shifting blame to dementia did not prevent caregivers from experiencing frustration or getting upset, rather it enabled them to direct their frustration to a source other than their family member and respond in a more compassionate way. This alternative logic, shifting blame to dementia, enabled caregivers to change the way they communicated with their family member and preserve a sense of compassion and goodwill toward their family member.
One caveat to consider is that although most caregivers could shift the blame for hurtful or frustrating behaviors, this was more difficult if the family member had been hurtful or frustrating to deal with prior to dementia. Terri (daughter) explained, “I have a very hard time going, it’s not my mom who’s saying these things, it’s Alzheimer’s. No, it’s very much her. She knows exactly how she’s treating me. She just doesn’t care because she never did.” Thus, blaming dementia was only possible for caregivers who saw a change in their family member’s behavior and were able to attribute that change to dementia.
Accommodating dementia
As caregivers acknowledged dementia as an actor in the relationship they were better able to anticipate how dementia might influence their family member’s behavior and communicate to craft normalcy around the symptoms of dementia. For example, knowing that dementia caused her mother to sometimes forget who family members were, Tracy (daughter) made a point to introduce herself every time she visited. She explained, “I’m not here to test her memory and make her guess who I am. I’m here to support her.” This simple behavior crafted normalcy around her mother’s memory loss, helping her mother feel more comfortable and allowing Tracy to avoid the pain of her mother not recognizing her. Accommodating dementia meant changing the approach to managing frustrating interactions. James (spouse) experienced frustration when his wife thought she needed to leave the house to attend work meetings, but acknowledging dementia helped James recognize that dementia had altered his wife’s perception of reality. Rather than arguing with his wife, he began taking her for a drive when she tried to leave the house. This approach enabled James to keep his wife safe and avoid unnecessary conflict. James referred to this as “learning to be in her reality.” Crafting normalcy around the family member’s new reality by accommodating dementia helped caregivers avoid frustrating, conflict-ridden situations and keep their family member safe.
Relying on memories
Acknowledging dementia as an actor in the relationship required caregivers to acknowledge the loss they experienced as dementia changed their family member. In the face of this loss, caregivers drew upon memories of their relationship prior to dementia to sustain them. Deidre (daughter) said, “I have good memories. You don’t have to think about the last eight years or so being the only time that you had a relationship.” Relying on memories was a means of foregrounding productive action while backgrounding negative feelings because it motivated caregivers to continue providing care as their family member changed. Barb (daughter) used a physical reminder of her relationship with her mother to motivate her ongoing caregiving. She said, “I put my favorite photograph of us together next to my bed so in theory, it’s one of the first things I see in a day. It helps me set for the day.” Relying on memories also helped caregivers maintain a sense of continued relational connection with their family member. Kim (spouse) explained, “Just reminding myself that no matter who he becomes, I’ll always know who he was, and I will be connected that way.” Similarly, Nancy (spouse) described how relying on memories of the past relationship helped sustain her in the face of the relational loss of dementia. She said: We have a huge backlog of happiness and happy memories and we can fall back on those in a good way. So if we were starting from today, I would say [our relationship is] not so happy. But since we’re not starting from today, I would still say we’re mainly pretty good.
As described above, relying on the backlog of happy memories from the past enabled caregivers take action to provide care and to find the positive in their relationship despite ongoing loss.
The experience of resilience
To yield further insight into dementia caregiver resilience, RQ2 focused on caregivers’ experiences of resilience. Caregivers described three forms of resilience in dementia: personal growth, enhanced relational closeness, and ambivalent resilience (see Figure 1).
Personal growth
Many caregivers experienced personal growth through providing care as a form of resilience. Caregivers’ personal growth centered on the development of valued characteristics such as greater patience, compassion, and empathy. Talking of her experience caring for her mom, Katie (daughter) said, “The overall experience of going through it with her definitely changed me, I think I’m a lot more empathetic.” Reflecting on his growth through dementia, James (spouse) said, “I am amazed at how gentle and how patient I’ve become… I’ve become shockingly patient and shockingly gentle.” Most commonly, caregivers discussed the development of greater patience through providing care, “I’ve grown to be more patient through this process” (Jennifer, daughter). Andrea (daughter) summed up this personal growth aspect of resilience when she said “I’m a hell of a lot more resilient than I ever was… I don’t snap under stress like I would have years ago. I’m flexible.” Caregivers exhibited resilience in their personal development through the challenges of providing care.
Enhanced relational closeness
Caregivers also experience resilience through enhanced closeness and love in their relationships with their family members. Gloria (spouse) said, “Our love continues to grow… [our relationship] is closer than ever.” Caregivers exhibited resilience in their ability to experience enhanced relational closeness, even as the symptoms of the disease altered their relationships. Describing her interactions with her husband, Cheryl (spouse) said, “There’s nothing but just eye contact and smiles and that kind of thing. It’s all there is, but right now that’s enough.” Similarly, Lisa (daughter) explained, “Our relationship we have now is probably deeper than it ever has been, and I would say it’s very loving, and two-sided if I could use that as a description.” Lisa continued by clarifying that she used the words “two-sided” to describe the way dementia had stripped away the “external forces on [the relationship].” She said, “Now it’s just person to person.” Like Lisa, many caregivers experienced relational resilience by finding sustained, and sometimes deepened, relationships despite the relational changes of dementia.
Ambivalent resilience
Some caregivers expressed ambivalence about their resilience. These caregivers both claimed some aspect of resilience and discounted their resilience, often in the same sentence. Mabel (daughter) said, “I want to say I have better patience, but I also personally feel like some days I don’t have better patience… I’m only human, so I have patience some of the time, I don’t have it all the time.” Mabel exhibits ambivalence about her resilience by claiming an aspect of personal growth (better patience) but expressing doubt about the extent to which she has actually grown. Similarly, Nancy (spouse) entertained the possibility that she could have grown or regressed through her experience with dementia, “Maybe I’m more compassionate to other people who suffer. I don’t know. Maybe I’m more self-centered than I ever was because I feel I have so much to contend with.” Nancy’s statement suggests that the sheer weight of dementia caregiving made it difficult for caregivers to perceive resilience in themselves. Caregivers also expressed ambivalence about resilience by expressing that experiencing personal growth and enhanced relational quality are not worth the difficulty they experienced in dementia. Annette (daughter) explained, “My relationship with mom is better than it was, but I still wish it wasn’t happening… I guess I’m growing, and there’s some beautiful moments, but it’s not worth it… the beautiful moments and the strength are not worth it.” This experience of ambivalent resilience illustrates the complicated nature of resilience in dementia.
Discussion
This project revealed the patterned way in which caregiver resilience unfolds in the context of dementia and caregivers’ experiences of resilience. The findings extend the CTR (Buzzanell, 2010, 2018) by identifying a facilitating mechanism necessary for enacting the communicative resilience processes identified by the CTR. In the following sections, we discuss these findings within the context of CTR theorizing and present practical recommendations for dementia family caregivers.
Implications for CTR theorizing
The findings of this study support and extend CTR theorizing. Supporting CTR theorizing, the analysis revealed that dementia caregiver resilience was initiated by a trigger event and enacted through communicative processes (Buzzanell, 2010). Interestingly, the disruption of communicative norms, rather than the diagnosis, triggered resilience for dementia caregivers. This suggests that it is not the singular moment of a diagnosis that triggers resilience but the “recognition of accumulated challenges” (Buzzanell, 2018, p. 100) through daily living with illness that triggers resilience. This mirrors Geary and colleagues (2023) finding that the ongoing daily challenges of living with HIV served as trigger events rather than the HIV diagnosis. This finding supports CTR theorizing about the sometimes ongoing and accumulated nature of trigger events.
Caregivers’ use of three CTR resilience processes also supports CTR theorizing. Examining these processes provides insight into how individuals construct a sense of normalcy within challenging end-of-life relational contexts. First, caregivers put alternative logics to work to shift blame for frustrating behaviors from their family member to dementia. This alternative logic enabled caregivers to shift attributions (Weiner, 1986) about the family member’s behavior from internal/controllable (assuming the family member had purposeful control over their behaviors) to external/uncontrollable (assigning blame to an external force – dementia). Making this shift in attributions was essential for facilitating ongoing relating in dementia because making internal/controllable attributions motivates ineffective conflict behaviors and diminishes relational satisfaction (Madden & Janoff-Bulman, 1981; Sillars, 1980). Applying this alternative logic helped caregivers preserve good will toward their family member despite frustrating communication changes. Second, accommodating dementia enabled caregivers to craft normalcy around the symptoms of dementia. Accommodating dementia required caregivers to recognize the reality their family member was living in and create new ways of interacting within that reality. Creating new routines has been shown to increase perceptions of dyadic coping through reduced uncertainty and anger (Lillie et al., 2021). Mirroring this finding, accommodating dementia enabled caregivers to avoid frustration, anger, and hurt, and maintain peaceful interactions in their relationships. Accommodating dementia enabled caregivers to cultivate more positive interactions with their family member and likely aided them in sustaining or even enhancing a sense of relational closeness (see Cooper et al., 2022; Netto, 2009). Third, caregivers foregrounded productive action while backgrounding negative feelings by relying on memories. Relying on memories motivated caregivers’ continued efforts to provide care and helped them move past the relational loss they experienced in dementia. Reminiscing has been described as a means of self-care for dementia caregivers (Anderson et al., 2019), and has been shown to promote wellbeing for both dementia caregivers and their family member (Fletcher & Eckberg, 2014; Haight et al., 2003). As suggested by the CTR (Buzzanell, 2010), enacting these resilience processes enabled caregivers to cultivate resilience in the face of relational disruption.
There were two CTR resilience processes that were not revealed through our analysis, affirming identity anchors and maintaining and using communication networks. We are not suggesting that these processes are not enacted by dementia caregivers, rather we suggest that these processes might be less prevalent in their interactions with their family member. Affirming identity anchors might be particularly challenging in dementia caregiving relationships because of the significant disruption to caregivers’ established relational identities and the complete transformation of the family member’s personality/identity (Hayes et al., 2009). In this transformed and ever shifting relational context, it might be difficult for caregivers to know which aspects of their own or their family member’s identity to hold on to. Similarly, caregivers might struggle to know how to maintain and use the communication network established with their family member as the relationship shifts. Although they continue to interact and seek to maintain connection with their family member, caregivers likely turn to other members of their social networks for support while providing care. An examination of dementia caregiver resilience beyond their interactions with their family member might reveal ways in which caregivers enact these two additional resilience processes.
Introducing facilitating mechanisms
Extending the CTR, this study revealed the patterned way in which resilience unfolds. Whereas the CTR conceptualizes the five communicative resilience processes as unfolding concurrently (Buzzanell, 2018), this study revealed that in some contexts one resilience process might serve as a facilitating mechanism requisite for the enactment of other resilience processes. The alternative logic, acknowledging dementia as an actor in the relationship, was a prerequisite process that enabled caregivers to enact other CTR resilience processes. Tian and Bush (2020) identified a “deep connection and simultaneity among these processes” which they referred to as “interwovenness,” suggesting that CTR processes unfold in concert to construct resilience. Our findings build upon this insight, suggesting that the CTR processes are not only interconnected, but that one process might serve as an essential facilitator of other resilience processes. In contexts of disruption and difficulty, identifying the processes that facilitate the enactment of other resilience processes (i.e., facilitating mechanisms) might provide productive points of intervention to promote the enactment of resilience. Work examining the associations of CTR resilience process with health-related outcomes has thus far treated resilience processes as occurring concurrently (see Kuang et al., 2023; Lillie et al., 2021), but future work might be benefitted by examining the ways that certain resilience processes (e.g., alternative logics) might promote the enactment of others. The identification of acknowledging dementia as an actor in the relationship as a facilitating mechanism enabling caregivers to enact other resilience processes provides greater insight into the way in which resilience processes operate together in the construction of resilience.
Of the CTR processes, putting alternative logics to work might be particularly likely to serve as a facilitating mechanism because alternative logics involve reframing to construct a new reality within disruption (Buzzanell, 2010). In this study, through acknowledging dementia as an actor in the relationship, caregivers constructed a new reality in which they viewed dementia as an active third party in their relationships. Working within this new reality, caregivers were able to enact resilience processes in ways that were previously unavailable to them. Constructing new realities through applying alternative logics opens new possibilities for crafting normalcy, foregrounding productive action, affirming identity anchors, engaging with social networks, and putting additional alternative logics to work. Communication plays a central role in applying alternative logics to construct a new reality. Caregivers’ statements describing the ways that dementia was “acting” in their relationships became a constitutive rhetoric (Seitz & Tennant, 2017) that shaped this new reality in their relationships and enabled them to communicate in new, more effective ways. The communicative nature of alternative logics makes them available to individuals facing any form of disruption. This first line evidence demonstrating the usefulness of an alternative logic as a facilitating mechanism could be expanded by examining the extent to which other resilience processes might serve as facilitating mechanisms in other contexts of disruption.
Experiences of resilience in dementia caregiving
Although resilience is the focus of the CTR, CTR studies rarely examine individuals’ perceptions of their own resilience. This study extends this literature by examining caregivers’ experiences of resilience. The majority of participants reported experiencing resilience through personal growth and/or enhanced relational closeness with their family member who has dementia. This aligns quite well with research about the positive experiences of dementia family caregiving. Netto and colleagues (2009) found that personal growth and improved relationships with the family member were two of the “gains” reported by dementia family caregivers. These findings confirm the potential for resilience and positive experiences in dementia, despite the challenges associated with providing care (Yu et al., 2018). These positive aspects of care promote lower depressive symptoms and burden, and higher quality of life for dementia caregivers (Quinn & Toms, 2019). Despite these encouraging findings, some participants painted a more complicated picture of resilience.
The theme ambivalent resilience reflects the mixture of growth and struggle that coexist in dementia caregiving. Although these caregivers claimed an aspect of resilience, they were quick to discount their resilience. Research on ambivalence in dementia caregiving suggests that ambivalent caregivers express both the pain associated with the changes in their family member and satisfaction at being able to support them (Shim et al., 2012). Despite including some positive emotions about care, ambivalence in caregiving is positively associated with depressive symptoms for dementia caregivers (AboJabel & Werner, 2022; Losada et al., 2017). This raises the question of whether ambivalent resilience is truly an experience of resilience. There is a chance that caregivers feel some pressure to be resilient, even if they do not feel resilient at all. One participant, Nancy, alluded to this pressure, “They say to me ‘You’re handling this so well.’ It’s just like f** no, I’m not. But then you have to live up and pretend you are handling it well.” Social pressure to be resilient might be an additional source of stress for caregivers who are already facing considerable difficulty. This finding affirms Buzzanell’s (2018) assertion that scholars must recognize both the benefits and costs of the ways resilience is constituted within our society. Researchers and organizations should exercise caution not to put the burden of resilience on individuals who are already overburdened by the weight of difficult situations.
Practical implications
This work has practical implications for family caregivers, particularly those who are early in the disease trajectory, when confusion between symptoms and deliberate behavior is most common. The earlier caregivers can acknowledge dementia as motivating their family member’s behavior, the sooner they will be able to enact other resilience processes and experience more effective interactions with their family member. Knowledge of the early symptoms of dementia might help caregivers recognize and characterize the role of dementia in their relationships. Dementia first rears its head through symptoms such as repetitive questions, irritability, and confusion. Interventions aimed at empowering family caregivers could be designed to train them to recognize these behaviors as dementia acting (rather than the family member) in order to help them acknowledge dementia earlier. With that as a foundation, caregivers could be further trained to focus on techniques for relational maintenance (e.g., joint engagement in enjoyable activities), identification of personal growth through caregiving, reviewing positive memories, normalization of ambivalence throughout these processes, and recognizing that there will always be good days and bad days. Such training could be embedded into printed information provided by care providers, presented through YouTube videos or podcasts, 3 or given through direct interactions during support group meetings or care appointments.
Limitations and directions for future research
The limitations of this research should be considered when interpreting these findings. This homogeneous sample of predominantly White, female, heterosexual, well-educated, and financially comfortable caregivers likely represents a privileged experience with caregiving and misses the experiences of individuals who might face additional risk factors regarding their resilience. Future work should examine the experiences of caregivers from marginalized groups who might draw upon different communicative behaviors to construct resilience. The retrospective nature of these data should also be considered when interpreting these findings. Retrospective accounts provided a useful overview of caregivers’ experiences and the processes they enacted to cultivate resilience but are shaped by caregivers’ sense-making over time. Examining the resilience processes caregivers employ across time would yield additional insights about the role of facilitating mechanisms in the construction of resilience.
In conclusion, this study revealed the patterned nature of dementia caregiver resilience within the relationship with their family member, particularly the central role of acknowledging dementia as an actor in the relationship as a facilitating mechanism. This study also highlighted the nuanced ways in which caregivers experience resilience. These findings extend the communication theory of resilience by conceptualizing facilitating mechanisms as resilience processes that facilitate the enactment of other resilience processes. This work provides insight into the interconnected way in which resilience processes unfold and might aid practitioners in identifying points of intervention to promote resilience. In the context of dementia family relationships, acknowledging dementia as an actor in the relationship was central to caregivers’ ability to enact resilience. Although most caregivers described themselves as resilient, some caregivers expressed ambivalence about their resilience, reflecting the incredible challenge of dementia caregiving. Taken together, these findings provide insight into dementia caregiver resilience and extend communicative resilience theorizing.
Footnotes
Acknowledgements
We would like to thank Dr Maggie Pitts and Dr Jake Harwood for their thoughtful feedback on earlier versions of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional review board
This study was approved by the Institutional Review Board at the University of Arizona, approval number STUDY00002222.
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research cannot be publicly shared but are available upon request. The data can be obtained by emailing: