
Abstract
Research into intervention strategies for developmental verbal dyspraxia (DVD) clearly demonstrates the need to identify effective interventions. The goals of this study were to examine changes in articulation skills following the use of phonetic, multimodal intervention and to consider the relationship between these improved articulation skills and perceptions of resilience behaviors. These changes were related to components of the World Health Organization (WHO) International Classification of Functioning, Disability, and Health, Children and Youth version (ICF-CY). The intervention was implemented daily for 12 children diagnosed with DVD, ages 3 to 10 years, enrolled in a school for children with speech, language, and hearing impairments on a university campus in the southeast of the USA. Eleven children presented with significant comorbid conditions. Changes in articulation, along with changes in parents’ and speech-language therapists’ (SLTs’) perceptions of resilience behaviors were measured. At the end of a 2-year period, statistically significant gains in articulation and parents’ and SLTs’ perceptions of resilience behaviors were noted. The relationship between improved articulation skills and increased resilience behaviors is discussed.
I Introduction
The relationship between improvement in articulation skills and how parents and teachers perceive changes in children’s resilience behaviors has little documented research in the literature. Also, there has been little research into the use of multimodal therapies for children with developmental verbal dyspraxia (DVD). Historically, however, intervention that made use of more than one modality has been noted by researchers such as Darley et al. (1975) and Dworkin (1991) for use with adults who have acquired apraxia through stroke or other brain insult.
This study sought to examine changes in articulation skills and in resilience behaviors and to consider the relationship between these changes following intensive intervention for children diagnosed with DVD. Intervention consisted of a phonetic, multimodal, structured teaching strategy delivered on an intensive basis where children were exposed to intervention across all curricula during the entire school day. Results may be considered in the context of the World Health Organization’s ICF-CY (WHO, 2007). McLeod and McCormack (2007) discussed the Activities and Participation component of the ICF-CY as being relevant to children with speech impairment. This component includes learning and applying knowledge; communication; domestic life; interpersonal interactions and relationships; major life areas (including education); and community, social, and civic life. In a systematic review conducted by McCormack et al. (2009), it was stated that the presence of a severe articulation disorder such as DVD may be associated with decreased Activities and Participation. The ultimate goal of this study is for children with DVD to realize both increased articulation skills and, because of better communication skills, increased behaviors that reflect resilience.
1 Resilience
Resilience can be defined as one’s ability to successfully adapt to, and overcome, a challenging situation (Benard, 1991; Card and Barnett, 2015; Howard et al., 1999; Linquanti, 1992; Masten et al., 1990; Tian and Hong, 2014). When assessing resilience, one typically considers the bidirectional relationship between the child and the environment, meaning the child influences the environment and the environment influences the child; keeping in mind resilience changes over time, as it depends on individual, social, psychological, and biological factors (Greeff and Nolting, 2013; Masten et al., 1990; Shannon et al., 2007). To determine resilience, two major judgments must be made: (1) a child has to be ‘doing okay’ in terms of what behaviors are expected, and (2) the child must have significant exposure to risk or adversity that poses a serious threat to positive outcomes (Masten et al., 2009). In studies of resilience, diverse criteria have been used to judge ‘good’ adaptation, including social and academic achievements; happiness or life satisfaction; normative mental health and conduct; and the overall absence of undesirable behavior (Card and Barnett, 2015; Masten, 2009).
Children are more likely to display resilience if protective factors are present (Shannon et al., 2007). According to Masten (2009), protective factors include positive attachments and relationships with caregivers/other adults; intellectual skills; self-regulation; a positive perception of self and self-efficacy; faith, hope, and a sense of meaning in life; supportive and prosocial friends; bonds to effective schools and other prosocial organizations; communities with positive services for families and children; and cultures that provide positive standards, rituals, relationships, and supports. Behavior problems, on the other hand, often increase the risk of poor family outcomes (McConnell et al., 2014).
The concept of resilience has been studied since the 1980s and has been applied to a variety of fields. Few studies have examined resilience in children with communication disorders, and no literature was found on resilience behaviors in children with DVD; rather, much of the resilience literature focuses on children with autism or attention deficit hyperactivity disorder (ADHD). Masten and Wright (2009) acknowledge that resilience is dynamic and can vary based on different stressors throughout a person’s lifespan. A review of the literature found no evidence to support a correlation between resilience and maturation.
2 Developmental Verbal Dyspraxia
Developmental verbal dyspraxia (DVD), or childhood apraxia of speech (CAS) as it is more commonly known in the USA, is discussed by the Royal College of Speech and Language Therapists (RCSLT) in the Policy Statement on DVD (RCSLT, 2011). In this document, DVD is described as a subset of speech impairment (SI) that is represented by a rare set of symptoms and often over-identified. According to the American Speech-Language-Hearing Association (ASHA), the national professional certification organization in the USA, CAS is defined as a neurological speech sound disorder (ASHA, 2007a, 2007b).
The RCSLT Policy Statement on DVD (RCSLT, 2011) and the ASHA CAS Technical Report (ASHA, 2007b) state that there is little research regarding the prevalence of this disorder. Prevalence rates for DVD vary and may reflect differences in the manner in which the condition is identified. In the United Kingdom (UK), for example, prevalence is estimated at 0.2% of the population (RCSLT, 2011), whereas in the USA, a range of prevalence has been noted from 0.1% to 4.3% (ASHA, 2007b).
DVD causes impaired precision of speech and inconsistent muscular movements during speech production in the absence of neuromuscular deficiencies. Impaired motor planning results in a severe speech disorder with significant errors in articulation and prosody of speech. Lewis et al. (2004) reported comorbidity with language disorders, both oral and written, and ASHA (2007b) referenced autism, epilepsy, fragile X syndrome, galactosemia, Rett syndrome, and chromosomal disorders as comorbidities.
3 Intervention for DVD
The primary goal of the intervention used as treatment for DVD is to improve speech intelligibility through the use of multimodal avenues of learning (i.e. visual, auditory, motor-kinesthetic, and tactile, or VAKT) by improving the accuracy of the articulation of phonemes. This is based on the motor theory of speech perception (Liberman and Mattingly, 1985), in that motor activity builds memory (Lane, 1965). Sloan (1980) recognized the need for motor-kinesthetic feedback of speech sounds to reinforce perception of these sounds. The premise is that precise articulation of each phoneme and systematic, incremental practice will increase a child’s memory for that phoneme while improving motor programming.
Intervention begins with the teaching of individual phonemes (Martin, 2012). Articulation as precise as possible for each child is required from the beginning and continues throughout the course of instruction. Martin (2012: 61) stated: for children with severe speech-language disorders … teaching-learning is more effective and efficient when skills of precise articulation are required, established, and maintained at each level of instruction … Thus, the child will not be producing and practicing poor speech which will need to be corrected.
Shaping of correct articulation is a continuous process as the child moves from the phoneme level through increasingly complex utterances. One goal of this phonetic, multimodal intervention for the remediation of DVD is to build competence and fluency of spontaneous speech.
4 Therapy model
Intervention consisted of the use of the DuBard Association Method®, a phonetic, multimodal speech-language therapy at a special school for children with severe communication disorders in a university setting, the DuBard School for Language Disorders at The University of Southern Mississippi, USA. The multidimensional aspects of this approach include concepts, language structure, sequential language, and skills for learning. The procedures are systematically organized so instruction consists of incremental units of language/speech with which a child can experience more success than failure. It requires that the child begins to acquire precise articulation of phonemes, using VAKT sensory modalities. As specific skills are mastered with phonemes, the small units are organized into larger and, gradually, more complex units related to communication until the child no longer experiences multiple uncertainties about language and speech (DuBard and Martin, 2000; Martin, 2012).
Intervention was provided by SLTs who serve as the classroom teachers at the school. Children were placed in classrooms with a maximum enrollment of 10 children with the SLT as teacher and a full-time paraprofessional also trained in the multimodal method. The intervention was delivered in small-group settings daily in the classroom during an 11-month school program. The phonetic, multimodal principles of this method also were incorporated into reading, math, science, and social studies units.
All professional staff met the requirements for being Highly Qualified for K-4 as outlined by the No Child Left Behind (NCLB) Act of 2001 (NCLB, 2001). In addition, all staff members were extensively trained in the use of the teaching method. The DuBard Association Method® training course is accredited by the International Multisensory Structured Language Education Council (IMSLEC); therefore, the training meets national standards for content and principles of instruction for multisensory structured language education (MSLE) (IMSLEC, 1997). Training consists of a minimum of an advanced university course or its equivalent, a 40 clock-hour noncredit course. In addition to training, the professional staff completed a minimum of 60 clock hours of practicum in this approach with a trained professional who was proficient in the method. Fidelity to the tenets of the multimodal intervention is assured through intensive training and extensive supervision prior to independent implementation.
II Methodology
1 Design
A repeated measures design was used to assess articulation and resilience behaviors in a pre- and post-test model. Because the same children were tested at pre- and post-intervention with zero attrition, potential error was reduced. To control for maturation, which is a threat to validity in a study of children over time, the Intervention Efficiency Index (IEI) (Bagnato and Neisworth, 1980) and the Proportional Change Index (PCI) (Bain and Dollaghan, 1991; Wolery, 1983) were used. The IEI, developed as a way to document progress in preschool programs, compares the developmental gain during treatment to the time spent in intervention, thus relating changes in a child’s performance to the amount of time in therapy. Wolery (1983) presented the PCI, which uses the IEI, but also adds a measure to control for children’s developmental status at the beginning of intervention. It compares the child’s rate of development prior to therapy to the rate of development during therapy. Therefore, a PCI of 1.0 indicates that changes made in articulation would be expected due to maturation. A PCI of greater than 1.0 indicates an impact attributed to the intervention beyond what is expected from maturation alone (Bain and Dollaghan, 1991; Salisbury and Copeland, 2013). The authors acknowledge that few clinical settings are able to provide speech-language therapy throughout each day of a school year. With no comparison group available, the PCI was used as a way to compare children’s progress during therapy to the amount of progress they made prior to this intervention.
2 Admission to the school and diagnosis of DVD
As part of the school’s admission process, each child is given a battery of standardized diagnostic tests. This battery includes hearing and vision screenings, orofacial examinations, measures for nonverbal ability, receptive and expressive oral language, written language, articulation, auditory processing, visual perception, visual-motor integration, word recognition, reading comprehension, word analysis, phonological coding, and spelling. Once testing is complete, the prospective enrollee undergoes diagnostic teaching, which is a ‘method of determining abilities and limitations of a child by careful observation of the response to specific instructional intervention’ (Martin, 2012: 29). Each prospective enrollee spends a minimum of three hours in the classroom during diagnostic instruction.
Once the diagnostic process is completed, a multidisciplinary team of SLTs, educators of the deaf, psychometrists, and/or general and special educators reviews previous records, current testing and diagnostic teaching notes. If it is determined that the child’s primary disability is in the area of oral and/or written language, speech and/or hearing, that child is eligible for placement in the school’s enrollment program.
As part of the diagnostic process, it is important to differentiate DVD from ‘inconsistent phonological disorder’ as described by Dodd et al. (2005). In research by Ozanne (2005), it was found that underlying motor programming deficits differentiate students with DVD from those with inconsistent phonological disorder. The RCSLT (RCSLT, 2011) referenced ASHA (2007b) when saying that three major features were identified as essential in the diagnosis of DVD. These features are inconsistent errors on consonants and vowels in repeated productions of syllables or words, lengthened and disrupted coarticulatory transitions between sounds and syllables, and inappropriate prosody, especially in lexical or phrasal stress. The Apraxia Characteristics Checklist (Figure 1) developed internally based on prior research (Crary, 1984; Haynes, 1985; Jaffe, 1984) was completed by a team of SLTs on staff and used to confirm the diagnosis of DVD.
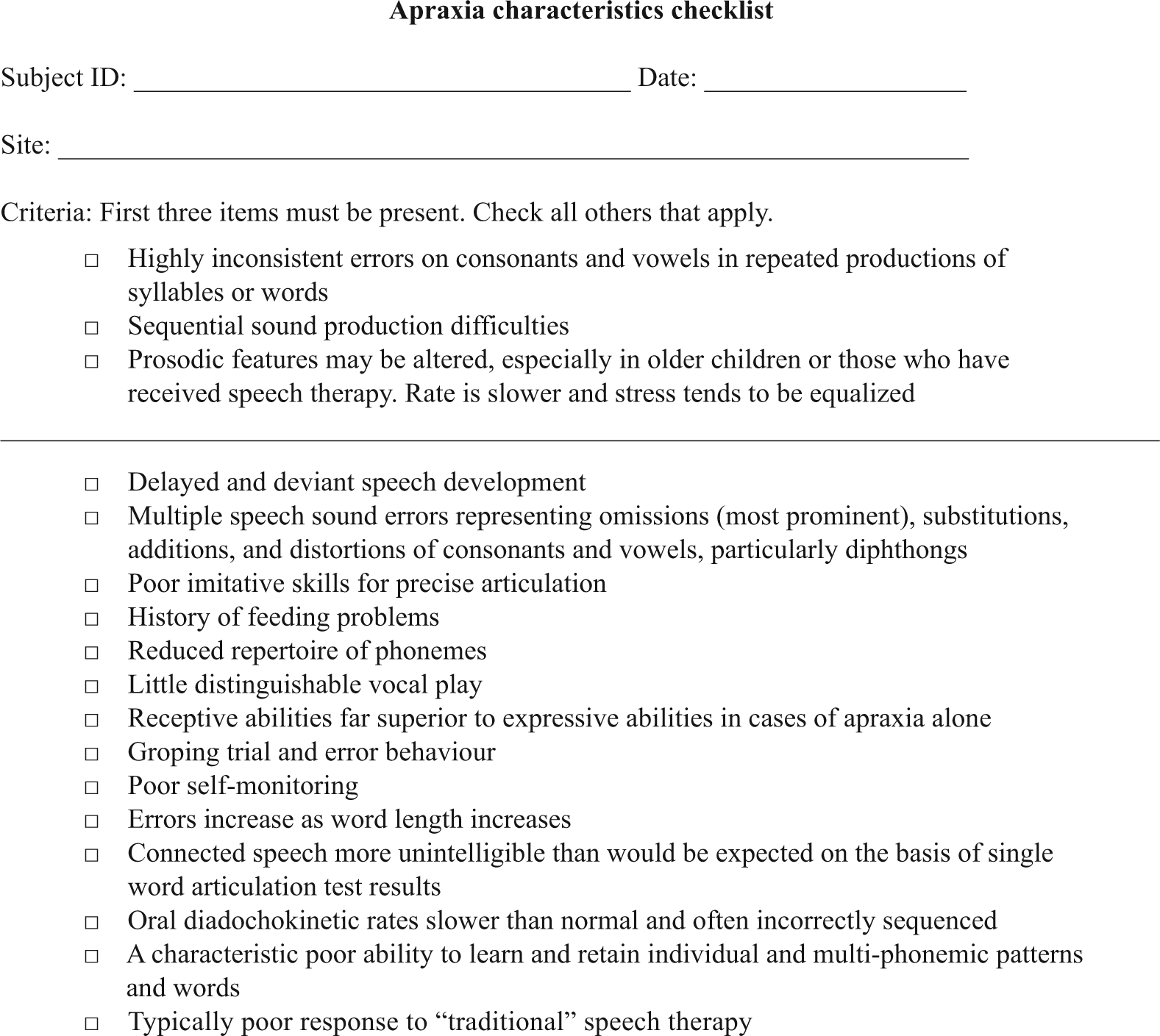
Apraxia characteristics checklist.
3 Participants
In August 2006, 27 children from eight school districts in the area near the university-based school, who had completed the diagnostic process and had met the criteria of a primary disability in the area of oral and/or written language, speech and/or hearing, were enrolled in the full-time program. Of these 27 children, 12 were diagnosed with DVD as described above.
The 12 children ranged in age from 3 years, 8 months to 10 years, 3 months at the beginning of the study. All children had received prior speech therapy which ranged from twice-weekly therapy in a school setting to therapy three times weekly at a half-day speech-language preschool (Table 1).
Prior therapy and comorbidities.
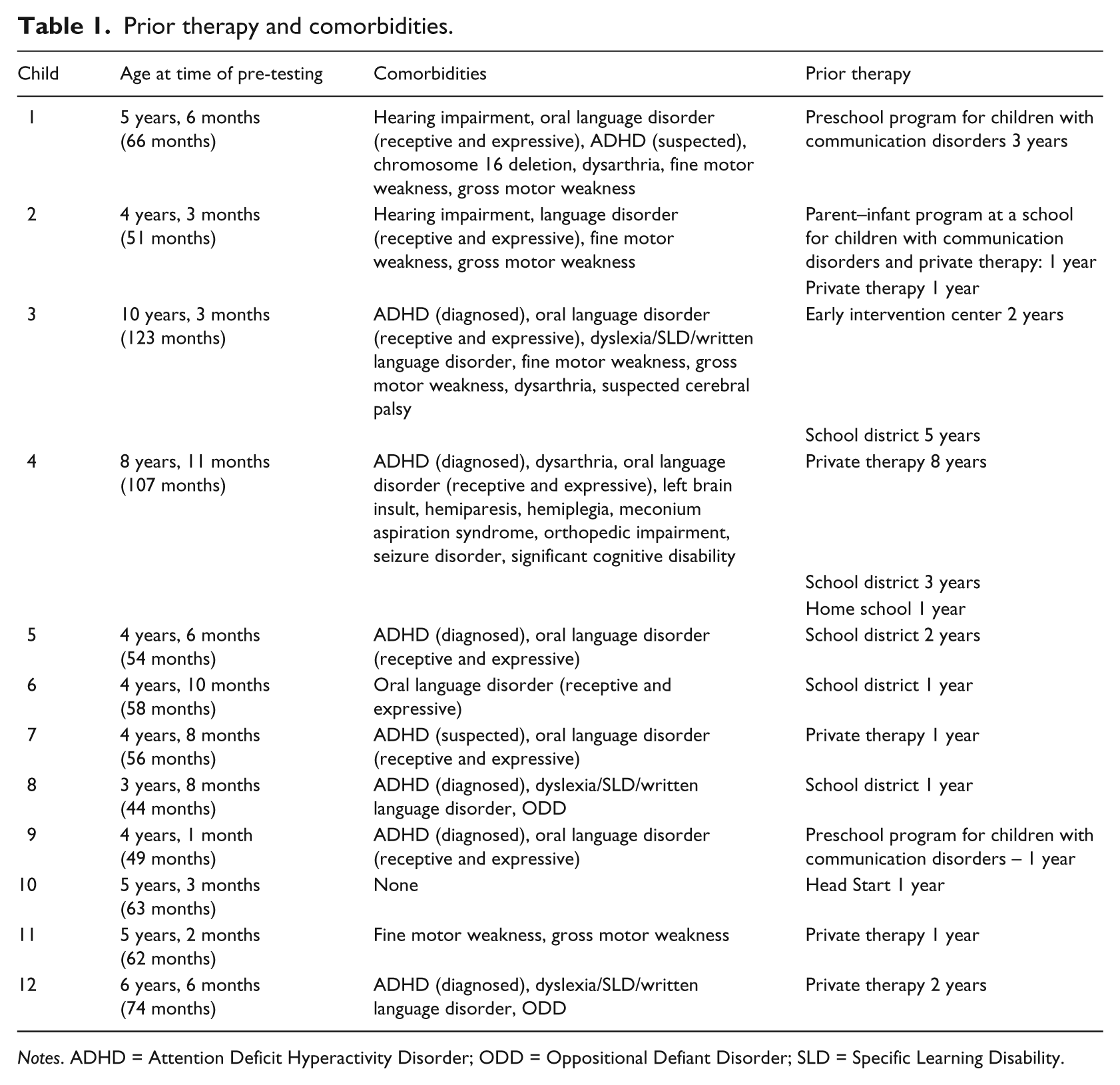
Notes. ADHD = Attention Deficit Hyperactivity Disorder; ODD = Oppositional Defiant Disorder; SLD = Specific Learning Disability.
In addition to DVD, 11 of the 12 children described in this article presented with 2–11 comorbid conditions, contributing to the heterogeneity of the sample (Table 1). However, no children were excluded from this study based on the number or severity of the comorbid conditions present. When discussing possible classifications of children with speech sound disorders, Lewis et al. (2006) affirmed the likelihood of a group of children with speech disorders being heterogeneous in terms of number and types of co-occurring conditions. The authors acknowledge that the heterogeneity of the current sample made statistical analysis of results more difficult and agree with the ASHA technical report Childhood apraxia of speech (ASHA, 2007), which stated that a ‘significant research constraint is the heterogeneity of children with CAS due to the co-occurrence of other disorders with CAS, as well as individual differences in compensatory behaviors that may be secondary to the primary deficits’ (ASHA, 2007b: 14).
4 Data collection: Articulation
Prior to enrollment in the study, the children were administered the Arizona Articulation Proficiency Scale-Third Revision (AAPS-3) (Fudala, 2000). The AAPS-3 also was used to measure articulation skills at the end of the intervention period. Standard scores, total scores, and mean length of utterance (MLU) were analysed. Calculations for MLU were done according to guidelines published by Brown (1973). Total scores were used to determine changes in intelligibility ratings. AAPS-3 total scores reflect weighted values assigned to each sound tested, based on the frequency of occurrence in American speech. Because of these weighted values, total scores are able to express intelligibility since an increase in the proportion of sounds made incorrectly will be reflected in the level of difficulty in understanding speech experienced by a listener (Fudala, 2000). The PCI (Bain and Dollaghan, 1991; Wolery, 1983), calculated using AAPS-3 total scores to determine the ratio of clinical significance attributable to the intervention, was used to determine the amount of progress made by the children during the intervention.
5 Data collection: Resilience
After children were enrolled in the school, parents and SLTs were asked to complete the Resilience Assessment of Exceptional Children (RAES) (Perry and Bard, 2001). The RAES was repeated at the end of the study, after two school years of intervention, with approximately 20 months elapsing between pre- and post-testing. The Parent Rating Form and Teacher Rating Form, completed by the SLTs, were used. Three domains measured by the RAES were Exceptionality Problem-Solving, Resilience Behaviors, and Social Support. Table 2 presents factors included in the resilience domain and behaviors that comprise each factor.
Resilience factors and behaviors measured by the Resilience Assessment of Exceptional Children (RAES).
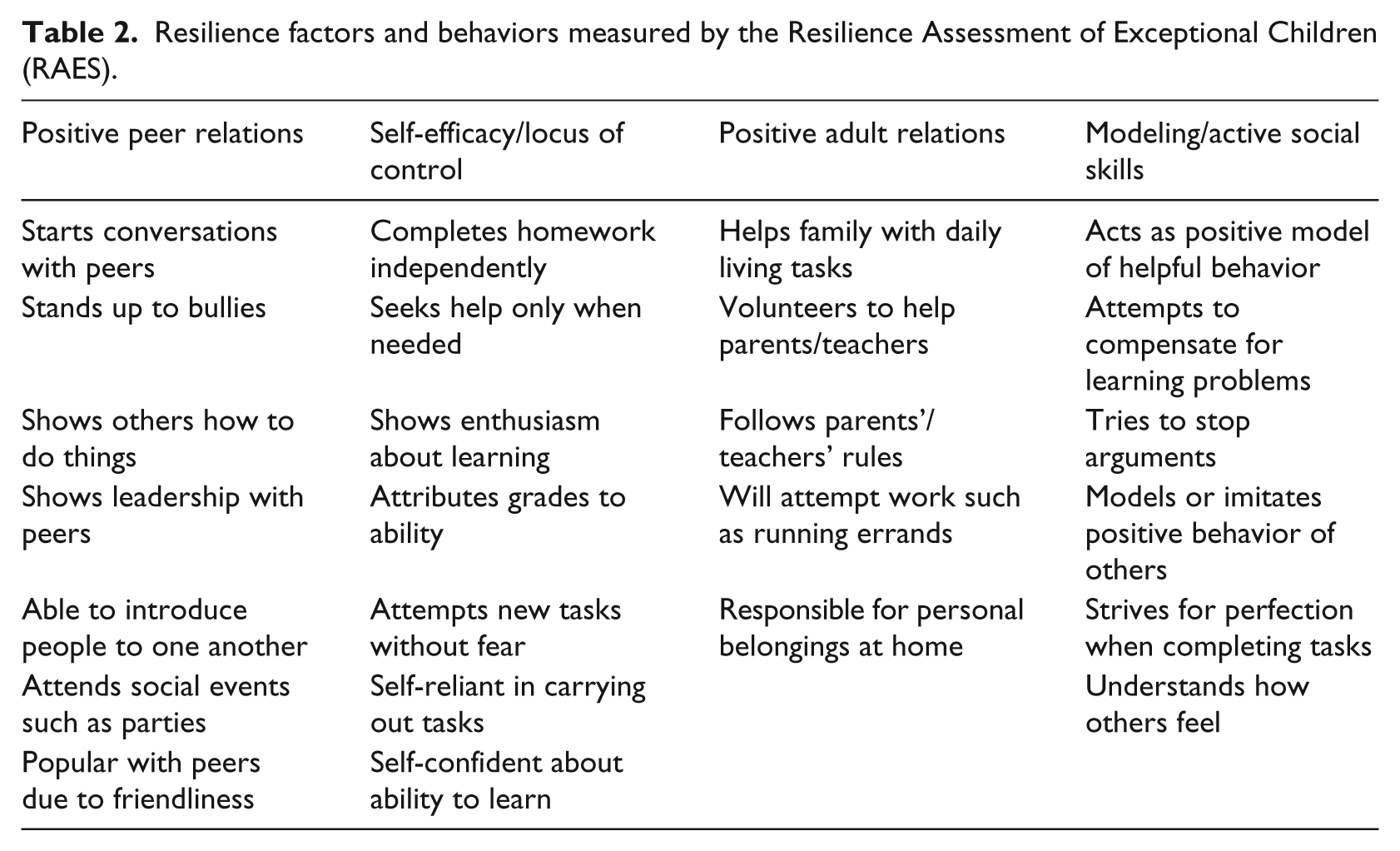
Both the parent and teacher forms of the measure include items rated for frequency of occurrence and need to improve. Frequency of occurrence items are rated on a four-point scale, with the following answer choices: 0 = never, 1 = sometimes, 2 = often, 3 = very often. Need to improve items are rated as follows: SA = strongly agree, A = agree, D = disagree, SD = strongly disagree. For analysis, a numerical scale was assigned to the need to improve items as follows: 0 = strongly agree, 1 = agree, 2 = disagree, 3 = strongly disagree. Therefore, a higher rating for need to improve items indicated the attitude that there was less need to improve a particular behavior.
III Results
1 Changes in articulation skills
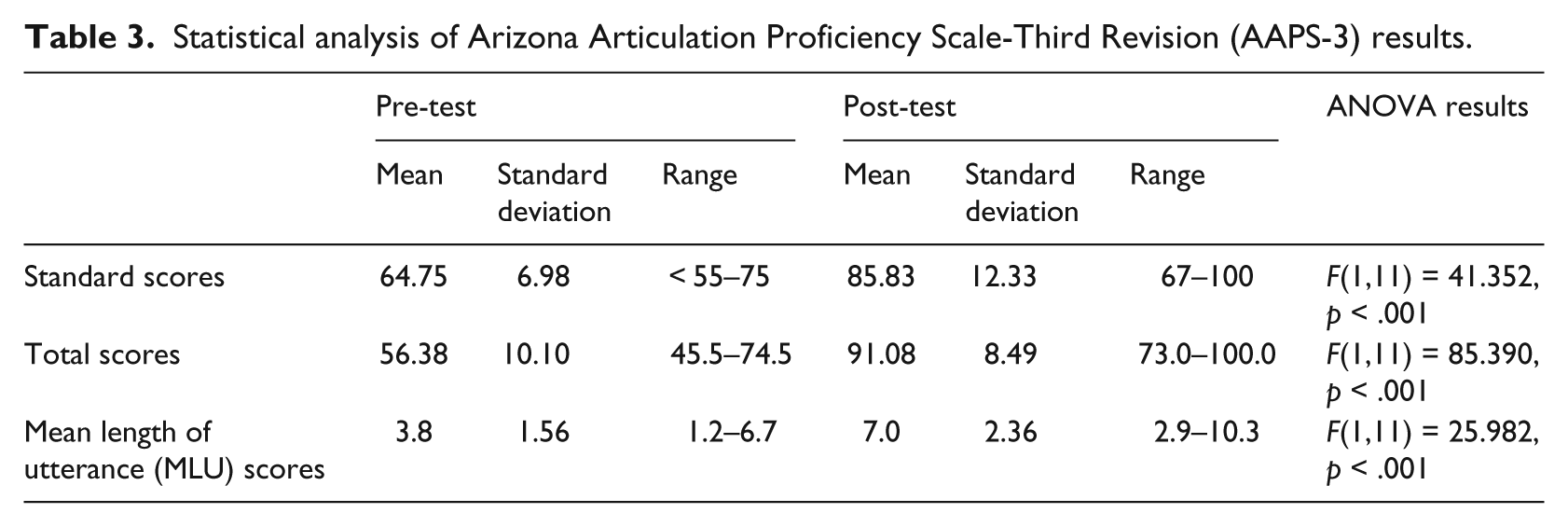
One goal of the study was to examine changes in articulation following intensive multimodal intervention for children diagnosed with DVD. Results of analyses of pre- and post-test measures of articulation revealed significant improvement in AAPS-3 standard scores, total scores, and MLU. Results of repeated measures ANOVA analyses are reported in Table 3. The changes in standard scores, total scores, and MLU scores are presented graphically in Figures 2, 3 and 4, respectively. At pre- and post-testing, the speech of all students was rated using the Speech Intelligibility Interpretation Values from the AAPS-3 illustrated in Figure 5. Based on analysis of percentage of Total Score improvement on the AAPS-3, ([Total Score Retest – Total Score Initial / Total Score Initial] × 100 = % improvement), percentage of improvement ranged from 17.81% to 116.30% with an average improvement of 66.02%.
Statistical analysis of Arizona Articulation Proficiency Scale-Third Revision (AAPS-3) results.
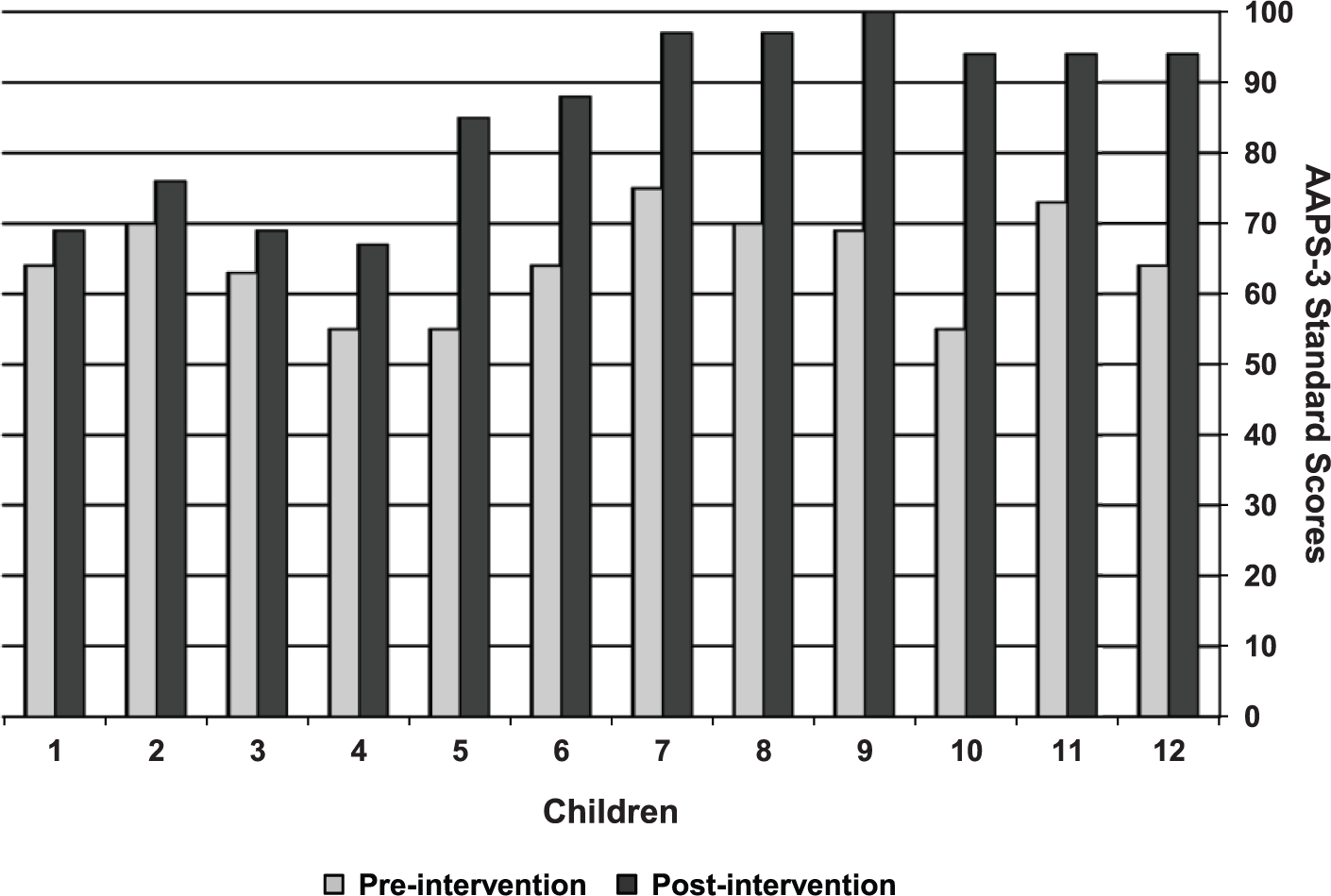
Arizona Articulation Proficiency Scale-Third Revision (AAPS-3) pre- and post-intervention standard scores graph.
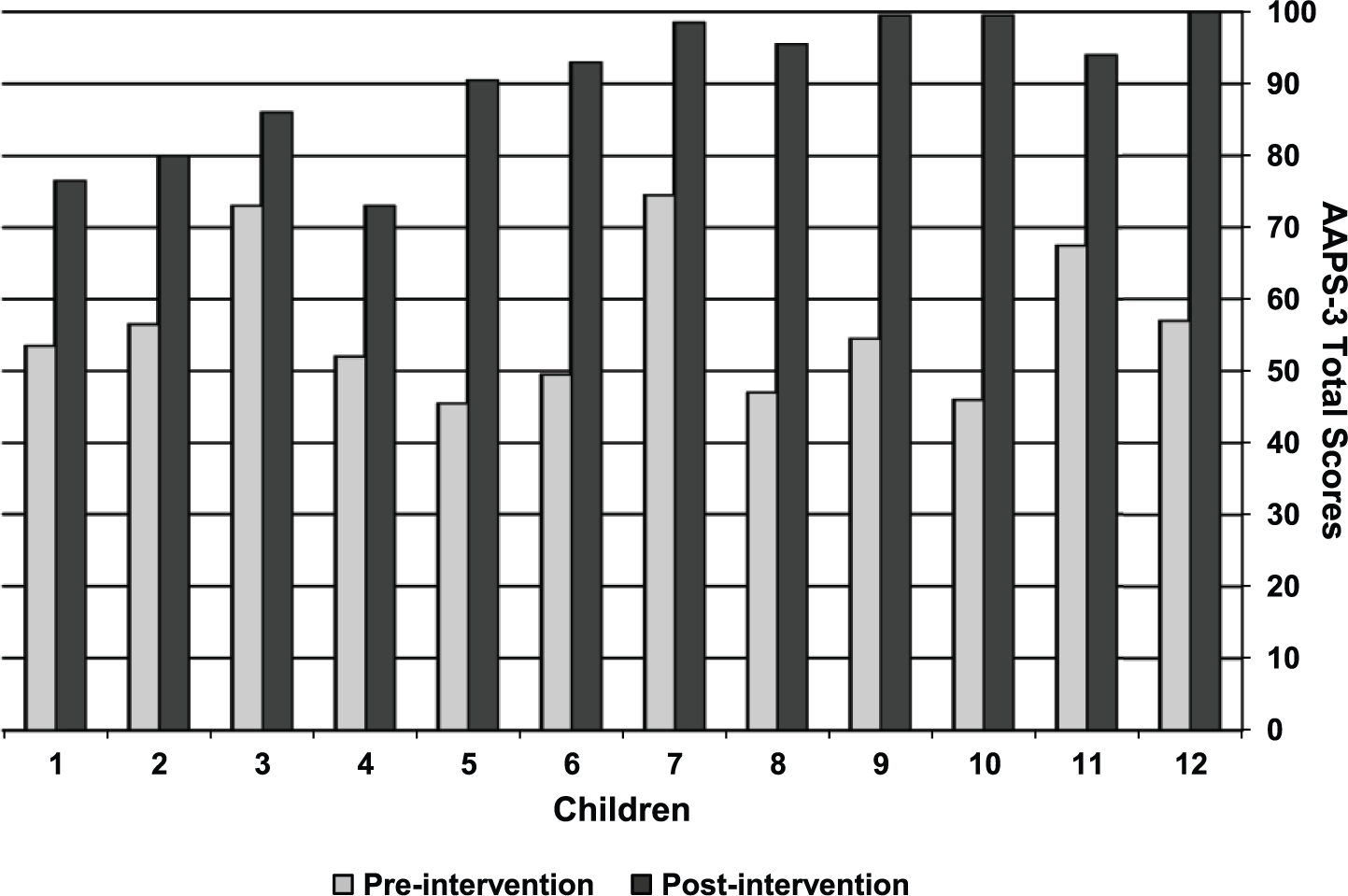
Arizona Articulation Proficiency Scale-Third Revision (AAPS-3) pre- and post-intervention total scores graph.
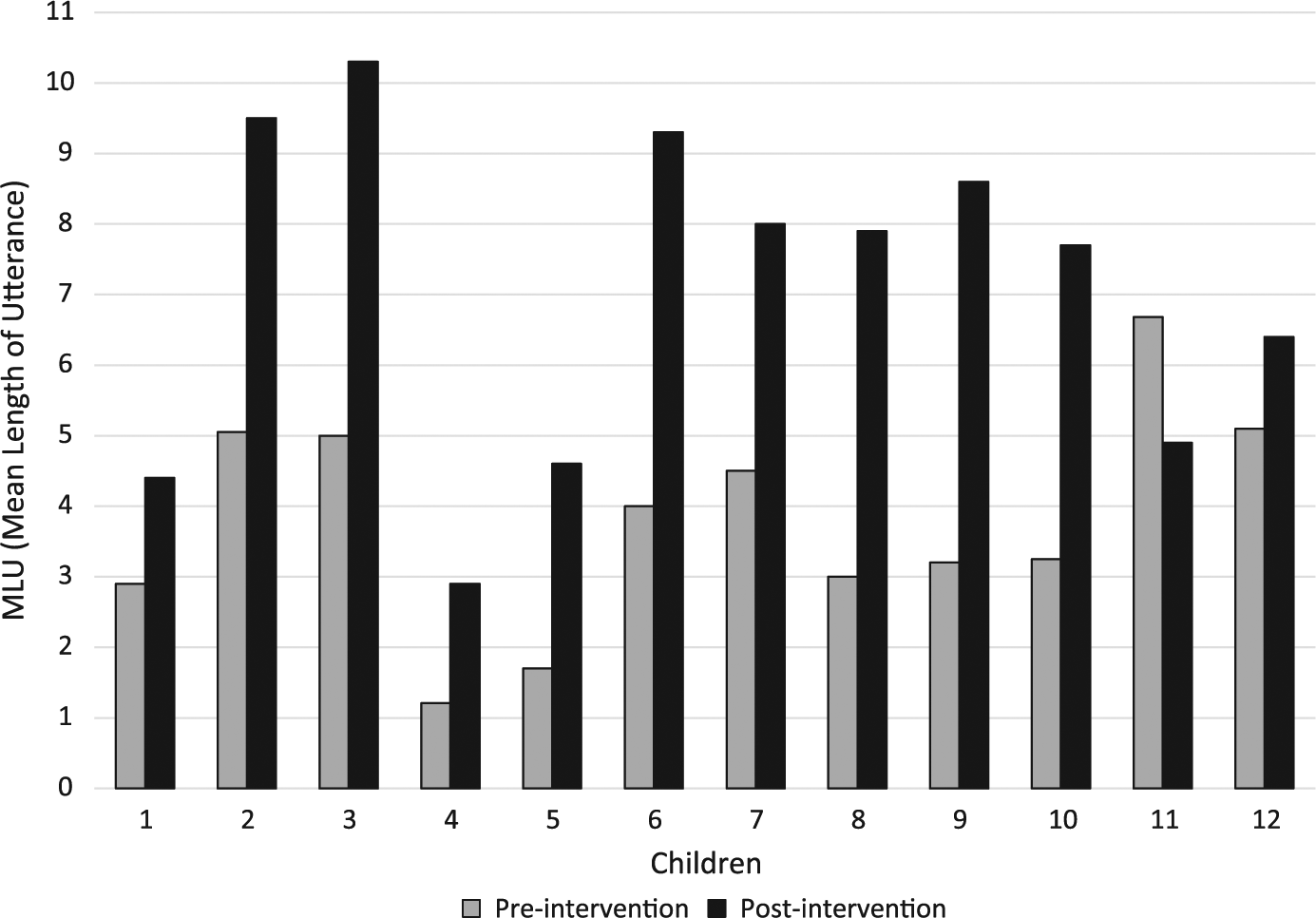
Arizona Articulation Proficiency Scale-Third Revision (AAPS-3) pre- and post-intervention mean length of utterance (MLU) ratings.
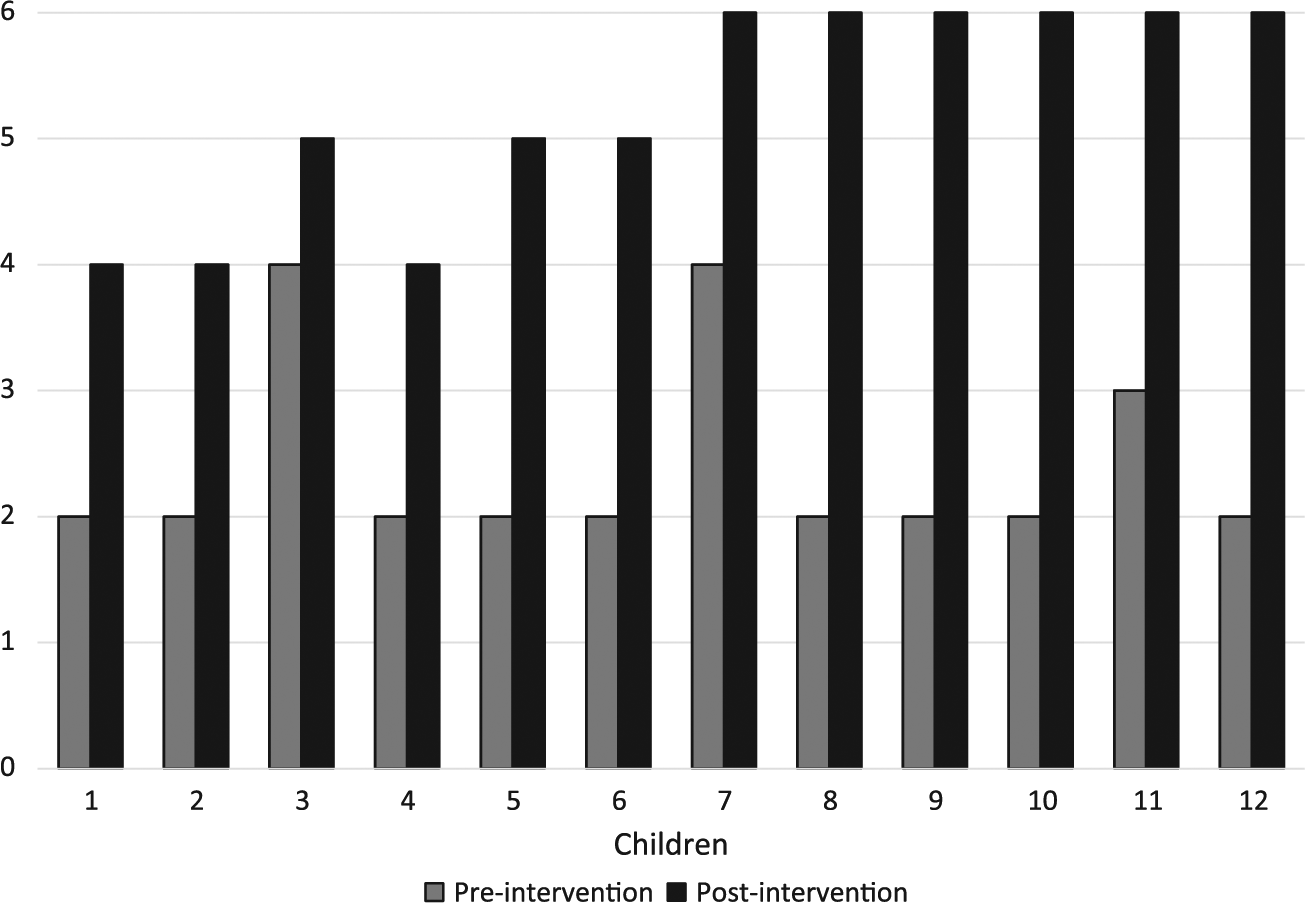
Arizona Articulation Proficiency Scale-Third Revision (AAPS-3) pre-and post-intervention intelligibility ratings.
Bain and Dollaghan (1991) and Salisbury and Copeland (2013) stated that a PCI of 1.0 indicates that a participant progressed at the same rate before intervention as during intervention. A PCI of 2.0 indicates that a participant made twice as much progress during intervention than prior to intervention. The children had a mean PCI (Bain and Dollaghan, 1991; Wolery, 1983) of 6.62 (range: 1.16–18.00), and 10 of the 12 children had a PCI greater than or equal to 2.0 (Figure 6).
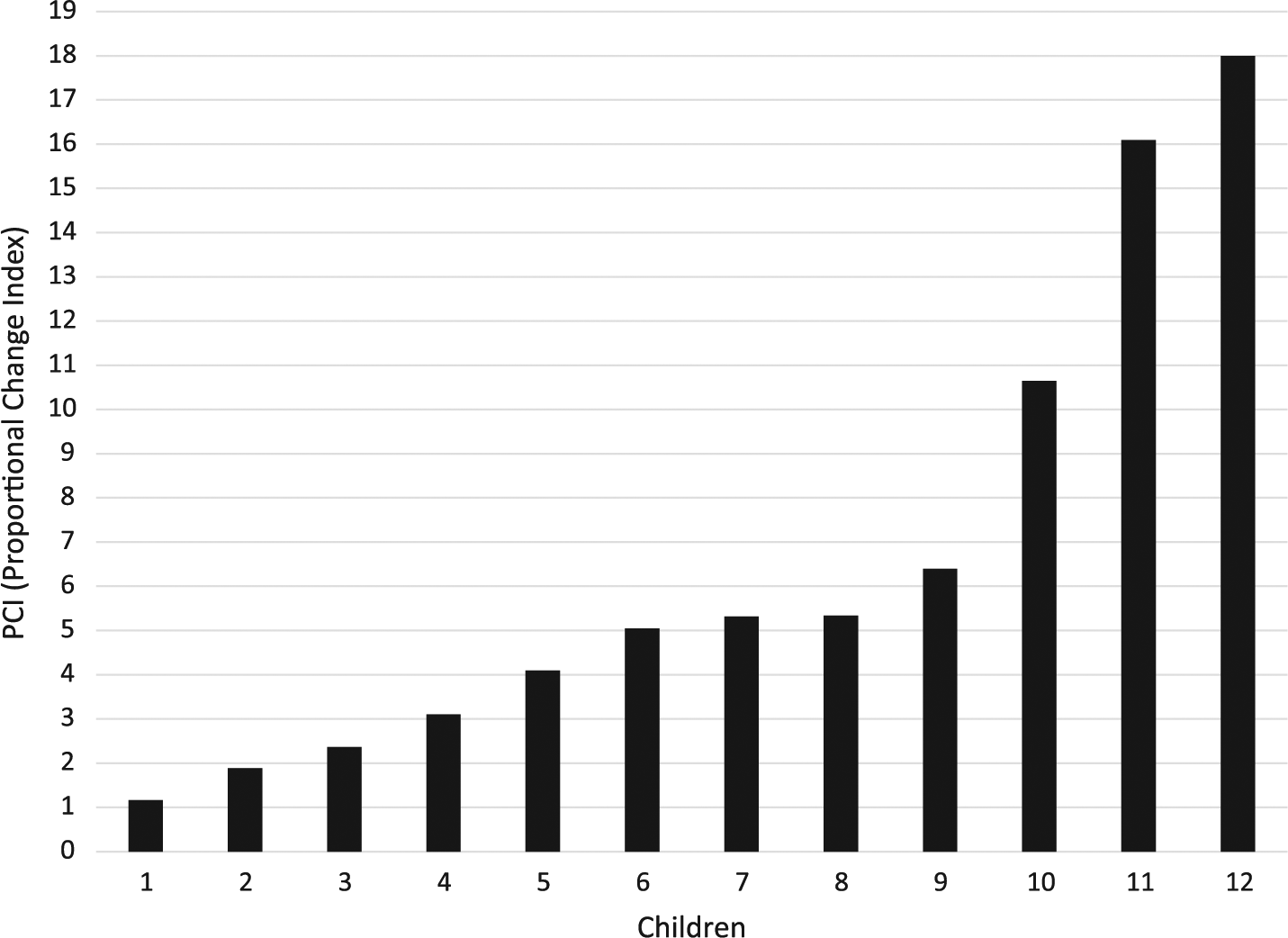
Proportional Change Index (PCI) scores.
2 Changes in parents’ and teachers’ perceptions of resilience behaviors
Another goal of the project was to examine whether or not parents’ and SLTs’ perceptions of the children’s resilience behaviors changed from the time the project started until the time the project ended. A repeated measures ANOVA was conducted that considered parents’ and SLTs’ perceptions of resilience behaviors at pre-test and after two school years of intervention for the remediation of DVD. Four factors were rated on the Resilience Behavior domain on the RAES: Positive Peer Relations, Self-Efficacy/Locus of Control, Positive Adult Relations, and Modeling/Active Social Skills. Two dimensions were considered within each factor: frequency of behaviors and the need to improve behaviors. Ratings values ranged from zero to three for each dimension.
Significant findings regarding changes in parents’ and SLTs’ perceptions of resilience behaviors are presented in Table 4. Parents’ ratings were higher than SLTs’ ratings for frequency of Positive Peer Relations, frequency of Self-Efficacy/Locus of Control, and frequency of Modeling/Active Social Skills. This may be indicative of differences in behaviors seen by parents outside of the school setting as compared to those observed by SLTs during school time.
Statistical analyses of Resilience Assessment of Exceptional Children (RAES) results.
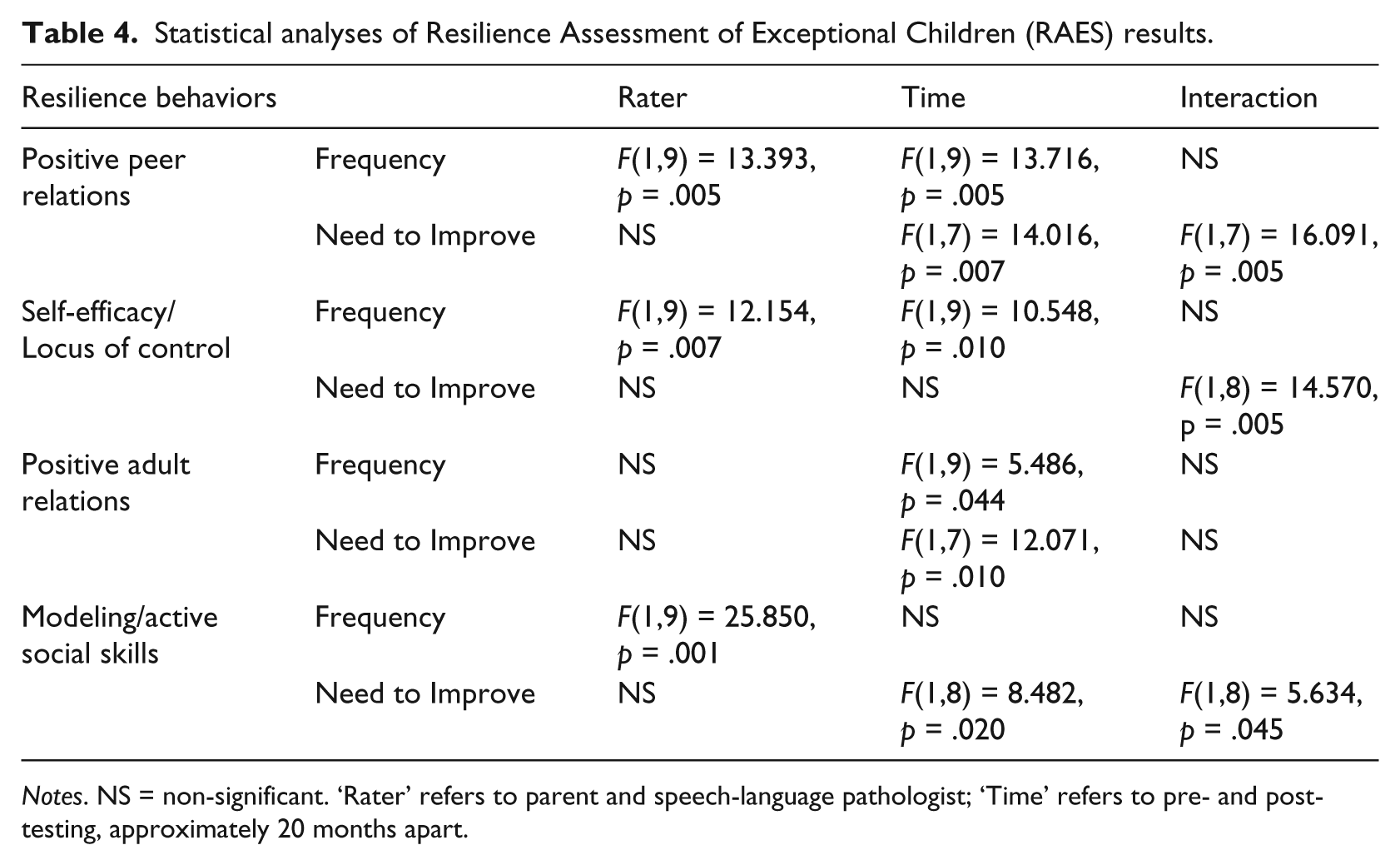
Notes. NS = non-significant. ‘Rater’ refers to parent and speech-language pathologist; ‘Time’ refers to pre- and post-testing, approximately 20 months apart.
Ratings increased from pre-test to post-test for frequency and need to improve Positive Peer Relations, frequency of Self-Efficacy/Locus of Control, frequency and need to improve positive adult relations, and need to improve Modeling/Active Social Skills. Increases in frequency ratings showed that parents and SLTs observed an increase in these behaviors related to resilience. Increases in need to improve ratings indicated less need to improve these behaviors over time, as a higher rating indicated that parents and SLTs showed higher disagreement that a particular behavior needed improvement.
Significant interactions were found for need to improve Positive Peer Relations, need to improve Self-Efficacy/Locus of Control, and need to improve Modeling/Active Social Skills. For each of these three factors, the mean rating for parents increased from pre- to post-test and the mean rating for SLTs decreased slightly. This may have been indicative of increased expectations by parents for improvement of resilience behaviors due to differences in behaviors observed outside of the school setting as compared to those observed by SLTs during school.
IV Discussion
DVD is a neurological speech sound disorder that often results in significant reduction in communication ability. Under the WHO ICF-CY (WHO, 2007), as outlined by McLeod and McCormack (2007) and further reviewed by McCormack et al. (2009), and McCormack et al. (2010), significant articulatory impairments may result in a decrease in Activities and Participation, which encompasses areas including communication, interpersonal relationships, and education.
The goals of this study were two fold. The researchers sought to increase articulation skills in children diagnosed with DVD through the use of use of a phonetic, multimodal, structured teaching strategy on an intensive basis where children were exposed to intervention across all curricula during the entire school day. As a result of increased speech competence and fluency, the researchers sought to examine changes in parents’ and teachers’ perceptions of children’s behaviors that reflected resilience.
Significant changes in articulation scores and intelligibility ratings were noted at the conclusion of this study. Keeping in mind the subjectivity of the assessment of resilience behaviors, significant changes in parents’ and SLTs’ perceptions of changes in resilience behaviors also were found. It appeared that parents’ and SLTs’ impressions of these behaviors differed somewhat. This was attributed to the two different settings in which behaviors were observed: home and school.
Both parents and SLTs noted increased peer relations, self-efficacy, adult relations, and modeling behaviors following intervention. There was a decrease in the need to improve resilience behaviors by the end of the intervention. For these results to show significant findings from both parents and SLTs is promising and speaks to the need for the use of a more holistic framework for treating children with severe speech impairments (McCormack et al., 2009, 2010; McLeod and McCormack, 2007).
Although the speech of some children may always contain errors, the change in quality of life because of ability to better communicate with family, friends, and potential employers cannot be underestimated. Studies have shown that impairment in communication ability impacts areas other than communication (McCormack et al., 2009, 2010). Individuals with good communication skills are more likely to arrive at school ready to learn and have higher achievement success (Frank Porter Graham Child Development Institute, 2014). At the end of this study, all children’ speech intelligibility ratings were at the ‘speech is intelligible with careful listening’ level or better, according to the AAPS-3.
V Study limitations, conclusions, and future research
Limitations to the study included small sample size, heterogeneity of the sample due to the number and type of comorbid conditions, and the lack of a comparison group. Because this study took place in a special school, intervention was provided on a more intensive basis than traditional, twice-weekly therapy; therefore, results found here may not be typical. However, therapy techniques using the DuBard Association Method® may be implemented in a more traditional therapy setting.
Despite limitations listed above, along with the subjective nature of resilience measurement, there were significant findings when considering parents’ and SLTs’ perceptions of changes in resilience behaviors. The continued use of the phonetic, multimodal, structured intervention approach for the remediation of DVD in an intensive therapy setting may result in improvement in articulation skills and in behaviors related to the ability to successfully adapt to, and overcome, a challenging situation. An increase in resilience behaviors may decrease social challenges in children with communication disorders, therefore increasing the likelihood of full involvement in the components of Activities and Participation as defined by the ICF-CY (WHO, 2007).
The results of this study supported the need for further research into the use of a phonetic, multimodal, intensive intervention with children diagnosed with DVD with comorbid conditions. The addition of the resilience component and the positive changes in resilience behaviors reflected in this study reinforce the need to consider the whole child, not just communication skills, when providing remediation for children with DVD. The use of the ICF-CY framework (WHO, 2007) would enable practitioners to consider a more holistic view to include factors that contribute to increased resilience as communication abilities improve.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.