
Abstract
The aim of this study was to evaluate the effectiveness of a computer-based executive function (EF) training in children with specific language impairment (SLI). Ten children with SLI, ages 8 to 12 years, completed a 25-session training of visuospatial working memory, inhibition and cognitive flexibility over a 6-week period. Treatment outcome was examined directly after training and at 6 months follow-up by tasks of the three trained EF, tasks of untrained neurocognitive functions (verbal working memory, attention, planning and fluency), and ratings of EF and behavioral problems by parents and teachers. Directly after training, results showed significant improvement on cognitive flexibility and a positive trend for visuospatial storage and inhibition. At 6 months follow-up, the children performed significantly better on tasks of all three trained EFs. Furthermore, the results showed significant improvement on sustained attention, attention control, parent- and teacher-rated attention behavior and parent-rated EF and externalizing behavior with medium effect sizes. The results of this pilot study highlight the importance of a large-scale, randomized controlled trial examining the possible effects of EF training in children with SLI.
I Introduction
Growing evidence suggests that executive functions (EFs) are in some way involved in the problems associated with specific language impairment (SLI). Several studies reported limitations in EFs in children with SLI (Henry et al., 2011; Im-Bolter et al., 2006). This raises the question whether training of EF might be a meaningful intervention for these children. Especially since EF training has proven to be a promising intervention in other groups of children characterized by impairments in EF (Klingberg et al., 2002, 2005, Melby-Lervåg and Hulme, 2012). To date, however, research describing interventions directed at improving EF in children with SLI is very limited. The present study, therefore, explores the effect of EF training in children with SLI.
1 Executive functions in children with SLI
Executive function (EF) is a broad term that comprises cognitive processes responsible for purposeful, goal directed behavior and is typically considered a multifaceted concept with distinct subfunctions (Miyake and Shah, 1999; Miyake et al., 2000). These processes are inter-related and function together as an integrated, supervisory control system (Stuss and Alexander, 2000). The three most frequently postulated components of EF are working memory, inhibition and cognitive flexibility (Huizinga et al., 2006; Miyake et al., 2000). Working memory (WM) refers to the structures and processes used to temporarily store and manipulate information (Baddeley, 2003; Baddeley and Hitch, 1974). Inhibition is the ability to stop prepotent or ongoing responses (Miyake et al., 2000). Cognitive flexibility, also described as shifting, has been conceptualized as the ability to switch the focus of attention between activities (Miyake et al., 2000). However, some debate remains about the exact components of EF. Various additional components have been postulated, for instance planning, fluency, emotional control, initiation and monitoring (Gioia et al., 2000; Piatt et al., 1999). Another issue in the field of EF research is the question of ecological validity of the performance-based tasks used to measure EF. Some evidence exists that standardized tests may not be sufficiently sensitive to the multidimensional nature of EF in daily life (Chaytor et al., 2006). Based on these findings, it is suggested that behavioral ratings of EF should be used to collect information in different contexts and from different sources (Gioia et al., 2001).
Children with SLI show a selective failure to make normal progress in language acquisition without further evidence of underlying intellectual, neurological, social, or emotional impairments (Bishop, 2006). They form a heterogeneous group with different profiles of language deficits; the impairment can affect different linguistic domains including phonological, morphological, lexical, and grammatical domains. Moreover, the linguistic profile may change with age and development (Bishop, 2006; Leonard, 1998). Different theories and hypotheses have been proposed to explain the underlying causes of SLI. Some hypotheses presume that SLI originates from a deficit or delay specific to language, and particularly grammar (Rice and Wexler, 1996; Van der Lely, 2005). More recently, however, there is growing evidence that nonlinguistic factors are also involved in SLI (Bishop, 2006; Montgomery et al., 2010). One factor that has been implicated is EF (Henry et al., 2011; Im-Bolter et al., 2006). Several behavioral studies provided evidence of EF deficits in children with SLI (Archibald and Gathercole, 2006b; Im-Bolter et al., 2006; Lum et al., 2011; Marton et al., 2007). Findings from neuroimaging studies furthermore concluded that children with SLI show anomalies in frontal brain areas normally related to EF (Dibbets et al., 2006; Jernigan et al., 1991).
Significant group differences have been reported in children with SLI compared to typically developing (TD) children on several components of EF, including WM, inhibition, cognitive flexibility, planning and fluency. These impairments were not confined to verbal EF tasks, but occurred for some nonverbal EF tasks as well. However, not all components of EF have been equally extensively studied, and in some cases results are still somewhat contradictory. Strong links have especially been found between working memory limitations and SLI (Archibald and Gathercole, 2006a; Bishop, 2006; Montgomery et al., 2010). Significant group differences have been reported between children with SLI vs. TD children on tasks of non-word repetition, recall of words or digits, and complex verbal span tasks (Archibald and Gathercole, 2006b; Conti-Ramsden, 2003; Gray, 2003, 2006). Visuospatial WM has been less extensively investigated with somewhat contradictory results. Several studies showed children with SLI to perform similarly to TD peers on visuospatial WM tasks (Alloway and Archibald, 2008; Archibald and Gathercole, 2006a, 2006b; Lum et al., 2011; Williams et al., 2000). Other studies and a recent meta-analysis, however, have yielded evidence suggesting that the WM deficits of children with SLI may extend to the visuospatial domain (Vugs et al., 2013).
Significant group differences have been reported between children with SLI vs. TD children on several tasks of inhibition, such as go/no-go tasks and tasks requiring resistance of distractors (Bishop and Norbury, 2005; Finneran et al., 2009; Im-Bolter et al., 2006; Marton et al., 2007; Spaulding, 2010). With regard to cognitive flexibility, studies in preschool children with SLI (age 4 and 5 years) showed poorer performance in comparison with their TD peers (Roello et al., 2015; Farrant et al., 2012). In contrast, no group differences were found between school-aged children with SLI and their TD peers on several shifting tasks, including the Trail Making Test (TMT) and set-shifting tasks (Dibbets et al., 2006; Henry et al., 2011; Im-Bolter et al., 2006). Planning has received considerably less attention in research on children with SLI, although difficulties with planning abilities in children with SLI have been reported on the Tower test and a Sorting test (Henry et al., 2011; Marton, 2008). With regard to fluency, children with SLI obtained significantly lower scores on both verbal and non-verbal fluency tests compared to their TD peers (Henry et al., 2011). Deficits in non-verbal fluency have not been found in all studies, however. For instance, Bishop and Norbury (2005) showed the performance of children with SLI not to differ from that of TD children on two tasks of non-verbal fluency.
Regarding behavioral ratings of EF in daily life, Hughes and colleagues (2009) found more negative parental and self-ratings of EF behaviors for adolescents with SLI compared to a TD group, with half of the parents of adolescents with SLI rating their child’s EF abilities in the clinically impaired range. In recent studies, parents and teachers of preschool and school-aged children with SLI reported significantly more problems relative to TD children on everyday EF behaviors (Cuperus et al., 2014; Vugs et al., 2013; Wittke et al., 2013). These included difficulties with inhibition, WM, shifting, emotional control, initiation, and planning. In school-aged children with SLI most problems have been reported on behavioral ratings of WM and initiation in classroom settings, with one third of the children scoring in the clinically impaired range (Cuperus et al., 2014).
2 Training of executive functions
Increasing evidence suggests that it is possible to improve EF by cognitive training. The underlying assumption for such interventions is that the maturation and/or efficiency of the neural circuitries underlying the trained EFs can be improved by intensive practice and training. Several novel, computer-based training programs have demonstrated promise in children and adolescents. To date, most studies particularly focused on the training of WM. Convincing evidence has been found for the trainability of WM in children with ADHD (Beck et al., 2010; Green et al., 2012; Holmes et al., 2010; Klingberg et al., 2002, 2005). Klingberg and colleagues (2002, 2005) were among the first to show, in a randomized controlled study in children with ADHD, that a computer-based WM training improved the trained visuospatial WM of the children. Significant improvement on at least one trained WM task has also been reported in several other studies and meta-analytic reviews (Gray et al., 2012; Green et al., 2012; Holmes et al., 2010; Melby-Lervåg and Hulme, 2012; Rapport et al., 2013; Shipstead et al., 2012). Furthermore, some studies showed that in children with ADHD these positive effects tend to be stable after training (Holmes et al., 2010; Klingberg et al., 2005). In a recent meta-analytic review it was found that the training effects on visuospatial WM tasks are maintained at follow-up, on average 5 months after the training (Melby-Lervåg and Hulme, 2012). It is generally accepted that WM training leads to positive effects on tasks closely related to the trained tasks, so called near-transfer effects.
However, some controversy exists about the generalizability or far-transfer of the training effects on functions not closely related to trained tasks, such as other neurocognitive functions, ADHD behavior, and academic performance (Melby-Lervåg and Hulme, 2012; Shipstead et al., 2012). Based on results of reviews documenting limited or negligible far-transfer effects, increasing concerns are expressed about the generalization of the trained task effects in WM training (Chacko et al., 2013; Melby-Lervåg and Hulme, 2012; Rapport et al., 2013; Redick et al., 2015; Shipstead et al., 2012). In contrast, a recent systematic review and meta-analysis showed persistent training effects for inattention in daily life for children with ADHD (Spencer and Klingberg, 2015).
Fewer studies have examined the trainability of inhibition and cognitive flexibility. A study of cognitive training of inhibition in TD children showed significant improvement on most of the trained tasks, but no generalization of the effect to tasks measuring WM or attention (Thorell et al., 2009). A study on the trainability of cognitive flexibility in children, adolescents and adults, showed significant improvement on cognitive flexibility tasks, and also on other EFs, including WM and interference control. White and Shah (2006) reported that adults with ADHD showed significant improvement on both trained and non-trained tasks after task-switching training.
Van der Oord et al. (2014) examined the effect of a computerized EF training in which three EFs were trained (i.e. WM, inhibition and cognitive flexibility) in children with ADHD. Game elements were added in order to increase children’s motivation and potentially optimize their cognitive performance during training. Adding game elements has proven to enhance the cognitive performance of children on EF tasks (Dovis et al., 2012; Prins et al., 2011). There was significant improvement on parent-rated EF and ADHD behavior. Effects were maintained at 9 week follow-up. A positive effect of this EF training has also been found in obese children, showing significant improvement on a WM task and childcare workers’ reports of WM and metacognition. In addition, children were more capable of maintaining their weight at 8 weeks after the training (Verbeken et al., 2013).
3 Cognitive training in children with SLI
To date, studies examining the possible effects of EF training in children with SLI are scarce. Whether cognitive nonlinguistic training in general could have a positive effect on language abilities in children with primary (or specific) language impairment was investigated in two exploratory single-subject design studies. Ebert and Kohnert (2009) trained processing speed and auditory memory in two school-aged children with SLI. Results indicated that the participants made gains in processing speed and some language abilities, including sentence formulation and grammatical morpheme production. These results were replicated and extended to two bilingual children with SLI using a training of processing speed and sustained attention (Ebert et al., 2012). Both children made gains in nonlinguistic skills, as well as in Spanish and English. More recently, Ebert and colleagues (Ebert et al., 2014) compared the effects of three different treatment programs in 59 bilingual school-aged children with SLI. The participants received either nonlinguistic cognitive, English, bilingual (Spanish–English) or deferred treatment. All three active treatment groups outperformed the deferred treatment control group and showed gains in the skills directly trained in the treatment. Children in the nonlinguistic cognitive treatment group significantly improved on processing speed and improvements on sustained attention approached statistical significance. Furthermore, cross-domain effect occurred: children in the nonlinguistic cognitive treatment group made significant gains in some of the language tasks from pre-test to post-test.
Holmes and colleagues (2015) investigated whether WM training could be effective in enhancing verbal WM in a group of 12 children with low language abilities, aged 8–11 years, and 15 matched TD children using Cogmed WM training (Cogmed, 2005). Both groups showed significant post-training gains on visuospatial storage (or visuospatial short-term memory). Further exploratory analyses revealed some predictive links between pre-training scores and training outcomes. First, visuospatial WM improved to the greatest extend following training for children with higher verbal abilities. Furthermore, children with the lowest verbal IQs at baseline made the greatest gains in verbal short-term memory (STM) after training.
Taken together, these results indicate that cognitive training could have positive effects on both nonlinguistic and language outcomes in children with SLI. Although cumulating evidence shows limitations in EF in children with SLI, the possible effect of cognitive training directed at improving EF has not yet been examined in these children.
4 Aims of the study
The aim of the present pilot study was to explore the effects of EF training in children with SLI. We evaluated the effectiveness of a 6-weeks computerized EF training program suitable for children aged 8–12 years, in which visuospatial WM, inhibition and cognitive flexibility are trained. The performances of the children with SLI before and after training were compared on tasks measuring the three EFs trained in the program, tasks of other untrained neurocognitive functions and ratings of EF and behavioral problems by parents and teachers. Since it was the first study of the possible effects of EF training in children with SLI, the research questions were mainly exploratory as follows:
Does EF training produce significant improvement on tasks of trained EFs (visuospatial WM, inhibition, cognitive flexibility) in children with SLI?
Does EF training produce significant improvement on other untrained neurocognitive functions in children with SLI?
Does EF training produce significant improvement in parents and/or teachers’ ratings of EF and behavioral problems in children with SLI?
II Methods
1 Participants
Ten children with SLI participated in this study; participants were: 8 boys and 2 girls aged 8–12 years, mean age 9;05 (SD 15.61 months), range 8;05 to 12;05. They were recruited from a Speech and Language Centre for children with severe language problems in the Netherlands. Diagnosis was based on extensive clinical and psychometric assessment by speech and language therapists; all participants scored 1.25 SD or more below the mean on at least two language measures (following Tomblin, 1996). Any children with a diagnosis of hearing disorder, frank neurological disorders, or autism spectrum disorder were excluded. All children had average nonverbal intelligence (mean 101.78, SD 12.96) and were native speakers of Dutch. Prior to attending the treatment center the children had received daily support for their speech or language problems for at least one year, without substantial improvement of their persistent problems. Children who showed clear impairments in EF based on their personal files or clinical evaluation (e.g. −1 SD on at least one task of WM, inhibition or cognitive flexibility) were sent information about the research project and invited to participate. Those from whom we received informed consent participated in the study. During the training period children did not receive any other treatment directed at improving EF or other neurocognitive functions.
2 Procedure
The study design included a pretest one week before the start of the training, a post-test at the conclusion on the training period and a follow-up 6 months later. The children were assessed in the Speech and Language Centre on the three trained EFs (visuospatial WM, inhibition, cognitive flexibility) and tasks of other untrained neurocognitive functions. Additionally, parents and teachers completed questionnaires about the behavior of the child.
At an introduction session the child and his or her parents were given practical information about the training. It was ensured that the program worked on the child’s computer and that it was placed at a location with limited distraction and without possible contact with the internet or other software. Sessions 1, 2, 10 and 20 were led by a research assistant in the Speech and Language Centre, other sessions were completed at home. All children kept a diary of their experiences with the game, and time spent on the training, the number of sessions played in a week, and difficulties or problems were reported. Time spent on training and frequency of the sessions were evaluated in the meetings with the research assistant. After completion of the training participants no longer had access to the program.
One week after treatment, the post-test was conducted, in which the children completed the tasks of the trained EFs. Follow-up was conducted 6 months after treatment and included all tasks and questionnaires of the pre-test session. Tasks were administered by neuropsychologists with expertise in assessment of children with SLI. All participants completed the post-test. At the follow-up session, one of the participants did not complete three of the included tasks. In addition, all questionnaires were returned at post-test. For the follow-up, the teacher questionnaires of one participant were missing.
3 Treatment
The intervention is the EF training ‘Braingame Brian’, in which three EFs (visuospatial WM, inhibition and cognitive flexibility) are trained, embedded in a game-like environment (Prins et al., 2013; Ten Brink et al., 2013). In this game world the main character is Brian, a creative boy who likes to invent things. The training consists of 25 sessions of about 45 minutes, played by the child four times a week over a period of 6 weeks, with not more than one session in each day of training. All sessions contain two blocks (of about 15 minutes) of the three training tasks in a fixed order: first WM training, second inhibition training and third cognitive flexibility training. After each block of tasks, the difficulty level is automatically adjusted to the child’s level of performance. Before, after and between training tasks, the child can walk around in the game world. To enhance motivation, every completed block results in an elaboration of the game world and extra powers for Brian, with which he can create interventions to help people in his village, resulting in happier village people (the more Brian helps them, the more they smile).
a Working memory training
The WM training combines different types of WM (Dovis et al., 2008a). It consists of five levels, training of (1) short-term memory, (2) short-term memory, updating and keeping information online, (3) short-term memory and manipulation/updating, (4) short-term memory and keeping information online during a delay, and (5) short-term memory, keeping information online and manipulation of information/updating. Each level is trained for 5 of the 25 sessions. The training consists of a 4 × 4 grid of equally sized rectangles (Figure 1), which light up in a random sequence. The first rectangle lights up for 900 ms and, after 500 ms, the next one lights up. At the first level, the child reproduces each sequence by clicking the rectangles in the right order with the computer mouse. In the other levels, tasks are more complex. For instance, the child holds information online about the position of side bars that lit up before the rectangles appeared or has to remember the position of rectangles in different colors. The session finishes when he or she has reproduced the required number of sequences, and sequence length is adapted to the child’s individual level of performance.
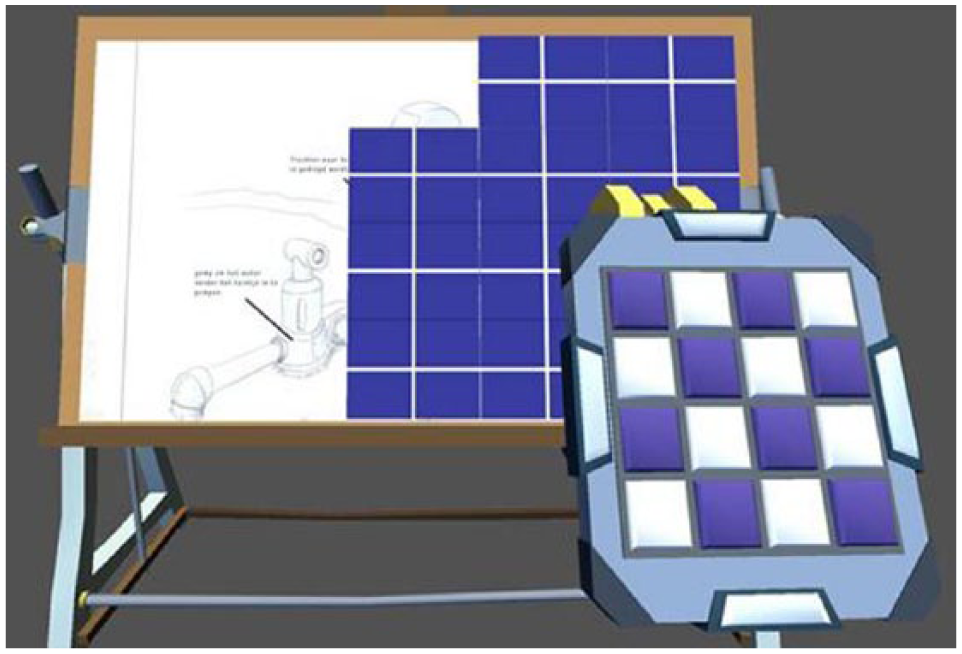
The working memory training.
b Inhibition training
This task trains prepotent response inhibition (Dovis et al., 2008b). It is visually designed as a factory, in which the child responds as quickly and accurately as possible to an arrow on a machine (Figure 2). In the first practice block of trials a stimulus lights up on the left or right side of the machine. These are the ‘go trials’. If the stimulus lights up on the left, the child presses the left button (Q key), and if the stimulus lights up on the right, the child presses the right button (P key). A stimulus at the top of the screen shows the range of time within which the child has to respond (a bar colored green between 700 and 1,000 ms and red before 700 ms and after 1,000 ms). In the next block ‘stop trials’ are introduced. After presentation of the stimulus, a stop signal is given (a tone, and the stimulus on the machine turns red), and the child has to inhibit his or her ongoing response. The time a child needs to stop his or her response is the Stop Signal Reaction Time. This reaction time is progressively shortened; the presentation of the stop-signal is automatically adjusted to the level of the child’s performance. Twenty-five percent of the trials are stop trials and 75% are go trials.
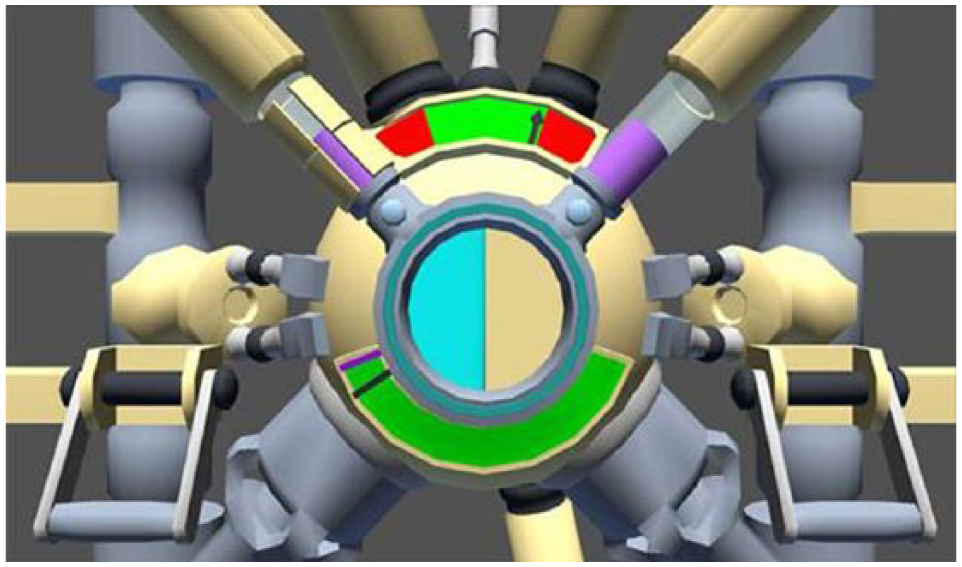
The inhibition training.
c Cognitive flexibility training
This task is based on training described by Karbach and Kray (2009), and designed to train cognitive flexibility (Dovis et al., 2008b). The child sorts various objects according to the instruction given, in a task which is also visually designed as a factory (Figure 3). In the two practice blocks the child is instructed first to sort objects according to color, and second according to shape. In the subsequent blocks switch trials are introduced, in which the child has to switch the rule of sorting the parts from color to shape, or from shape to color; 25% are switch trials and 75% are non-switch trials. The interval to respond is progressively shortened based on the child’s level of performance on the task. The switch cost is the time needed for switch trials subtracted from the time needed for non-switch trials, and the training is intended to reduce the switch cost.

The cognitive flexibility training.
d Training compliance
Nine of the 10 participants completed all 25 sessions of the training; one participant completed 24 sessions. Because a minimum of 20 training sessions was required to complete the training program, all children were considered to have finished the EF training. The duration of the training period varied from 39 to 50 days. On average participants spend 46.45 minutes on one training session (SD 9.12).
4 Outcome measures
a Trained executive functions
Visuospatial working memory: The Automated Working Memory Assessment (AWMA; Alloway, 2007) is a computerized assessment battery measuring different components of Baddeley’s WM model, including verbal and visuospatial storage tasks relying on the serial recall of information, and verbal and visuospatial central executive (CE) tasks in which the children simultaneously store and process information (Gathercole and Pickering, 2000). The subtest Dot Matrix is a task of visuospatial storage in which a sequence of red dots is presented on a 4 × 5 grid. All of the dots appear in the grid for 2 seconds, then disappear and the child points to the position of each dot in the same serial order as presented. Spatial Span is a task of visuospatial CE in which two identical shapes are presented with a red dot above the right shape. The child judges whether the two shapes are in normal or mirror image and remembers the location of the dot, which rotates to one of three positions of a triangle. After trials requiring the child to judge the similarity of the shapes, they disappear and a triangle of three dots reflecting the possible positions of the previous dots appears and the child points to the positions of the previous dots in the right order.
Inhibition: The subtest Walk Don’t Walk of the Test of Everyday Attention for Children (TEA-Ch; Manly et al., 2007) requires the periodic and unpredictable withholding of a routine response. Children are given a sheet showing ‘paths’, each made up of 14 squares. They are asked to listen to a tape that will play one sound (go tone) if they should move to the next square and another (no-go tone) if not. Moves are made by ‘dotting’ each square with a marker pen. The go and no-go tones are identical for the first millisecond, requiring the child to listen to the entire sound before making their response.
Cognitive flexibility: The Trail Making Test (TMT) is a test of task switching (Delis et al., 2001). It consists of five parts in which the child is instructed to connect dots with numbers or letters in the right order as fast as possible while still maintaining accuracy. It also includes a number–letter switching condition, in which the child has to switch between numbers and letters. For this study we used this switching condition.
b Untrained neurocognitive functions
Verbal working memory: The subtest Digit Recall of the AWMA is a task of verbal storage in which the child recalls a sequence of digits in the right order. The digits range from one to nine and are spoken at a rate of one digit per second. Sequences are randomly generated and no digits are repeated. The subtest Listening Span of the AWMA is a task of verbal CE in which the child is presented short sentences of subject–verb–object order and containing early developing vocabulary. She or he then judges whether the content of the sentence is correct (by saying ‘true’ or ‘false’) and must remember the first word of the sentence. After a series of sentences have been presented the child recalls the first words of the sentences in the correct serial order. The number of sentences in each set increases.
Attention: The subtest Sky Search of the TEA-Ch is a task of selective attention. Children are given a laminated A3 sheet depicting rows of paired spacecraft. There are four distinctive types of crafts, and most pairs are of mixed type. The children are instructed to find all the pairs of identical crafts as quickly as possible. Twenty targets are distributed among 108 distractors. Both accuracy and time taken to complete the task are recorded. The Score! subtest from the TEA-Ch is a task of sustained attention in which the child counts identical tones which are separated by silent interstimulus intervals of variable duration. Children are asked to silently count the tones (without assistance from fingers) and to give the total at the end. The subtest Creature Counting of the TEA-Ch is a measure of attention control. Children have to repeatedly switch between two relatively simple activities of counting upwards and counting downwards. They are asked to count aliens in their burrow, with occasional arrows telling them to change the direction of counting. Time taken and accuracy are scored.
Planning: The subtest Six Elements of the Behavioural Assessment of the Dysexecutive Syndrome for Children (BADS-C) is a test of planning, task scheduling and performance monitoring (Emslie et al., 2003). The children are instructed to do three tasks each of which is divided into two parts. They have to schedule their time on these six subtasks over a five minute period. They are not allowed to do two parts of the same task consecutively. Scoring is based on the number of tasks attempted, and penalties are given for rule infractions or not spending an equal amount of time on each task.
Fluency: The subtest Verbal Fluency of the Developmental Neuropsychological Assessment Battery (NEPSY; Korkman et al., 1998) is designed to assess verbal productivity through the ability to generate words within specific semantic and initial letter categories. The child is given a semantic or initial letter category and asked to produce as many words as possible in 60 seconds.
c Behavioral ratings
EF behaviors: The Behavior Rating Inventory of Executive Function (BRIEF) is a standardized rating scale for parents and teachers of children aged 5–18 years old (Gioia et al., 2000). We used the Dutch version, which contains 75 items (Huizinga and Smidts, 2011). Each item pertains to specific everyday behavior, relevant to EF. Items are categorized in eight non-overlapping theoretically and empirically derived clinical scales that measure different aspects of EF: Inhibit, Shifting, Emotional control, Initiate, Working memory, Plan/organize, Organization of materials, and Monitor. These eight clinical scales form two broader indexes: Behaviour Regulation Index (BRI) and the Metacognition Index (MI). Based on these two composite scores an overall global EF score (i.e. Global Executive Composite, GEC) is calculated. For this study we used the subscales Inhibit, Shift, Working memory, the Metacognition index, and the Total scale as dependent variables. The normative mean is 50 (SD 10), with higher scores indicating more problems.
Behavioral problems: The Child Behavior Checklist (CBCL) is a standardized rating scale for parents to detect emotional and behavioral problems in children and adolescents aged 6 to 18 years (Achenbach and Rescorla, 2001). The questionnaire is made up of eight syndrome scales, including Anxious/depressed, Depressed, Somatic complaints, Thought problems, Attention problems, Rule-breaking behavior and Aggressive behavior. These group into three higher order factors: Internalizing, Externalizing and Total Problems. We used the scales Thought problems, Attention problems, Internalizing, Externalizing and Total Problems. The versions for parents (CBCL) and for teachers (Teacher Report Form; TRF) were used. The normative mean is 50 (SD 10), with higher scores indicating more problems.
5 Statistical analyses
Data were analysed using SPSS Version 21.0. All data were complete for 80% of the children at pre-test, post-test and follow-up. Missing data were imputed using multiple imputation (Rubin, 1987). Because of the small number of participants the data cannot be assumed to be normally distributed and the nonparametric Wilcoxon signed-rank test was used to examine changes between scores at the post-test and follow-up and pre-test scores. Additionally, effect-sizes were calculated using the following equation: r = z / √N, in which N is the total number of observations on which z is based. The effect size is a measure of the magnitude of the mean difference and is considered small for r = .20, medium for r = .50 and large for r = .80 (Cohen, 1988).
III Results
1 Pre-Test Results
Descriptive statistics for the pre-test are shown in Table 1. Performances of the participants were compared to the normative mean scores in one-sample t-tests. The number of children scoring −1 standard deviation (SD) or more below the normative mean was also calculated.
Mean and standard deviations of pre-test standard scores (SS), T test statistics and p values of comparison between study participants and normative data.
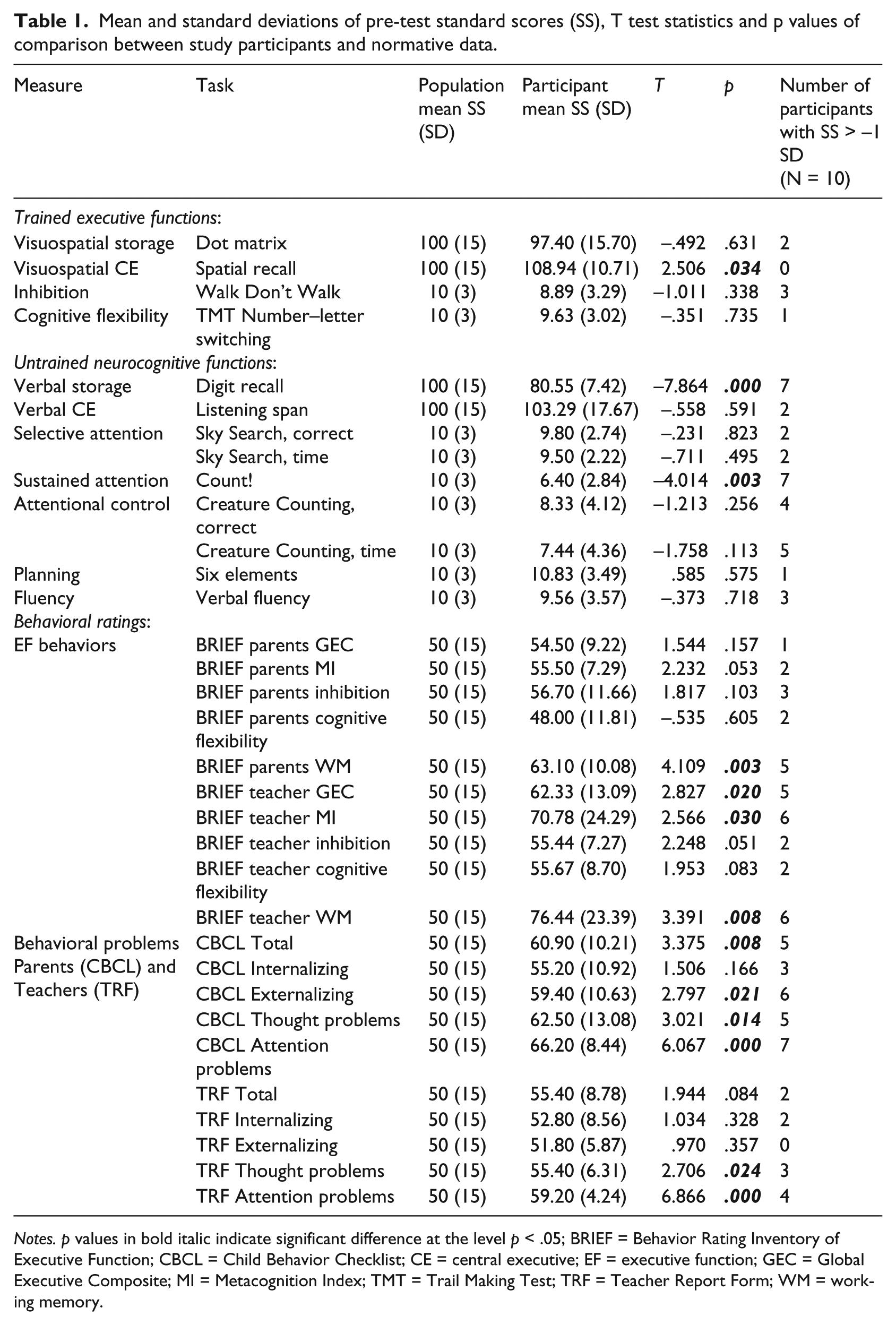
Notes. p values in bold italic indicate significant difference at the level p < .05; BRIEF = Behavior Rating Inventory of Executive Function; CBCL = Child Behavior Checklist; CE = central executive; EF = executive function; GEC = Global Executive Composite; MI = Metacognition Index; TMT = Trail Making Test; TRF = Teacher Report Form; WM = working memory.
For the trained EFs 2 participants scored −1 SD or more below the normative mean for Dot Matrix, 3 for Walk Don’t Walk and 1 for TMT Number–letter switching. However, the average pre-test scores of the participants did not significantly differ from the normative mean scores for Dot Matrix, Walk Don’t Walk, and TMT Number–letter switching. None of the participants scored −1 SD below the normative mean for Spatial Span and the average pre-test score for this task was significantly higher than the normative mean.
On the untrained neurocognitive functions tasks the average pre-test scores of Digit Recall and Score! were significantly below the normative mean, with 7 of the participants scoring −1 SD or below on both tasks. The other pre-test scores did not significantly differ from the normative mean scores.
For the parental rating of EF behaviors (BRIEF), the average pre-test score of Working Memory was significantly higher than the normative mean, with 5 of the participants scoring +1 SD or more (a higher score indicates more problems). Scores on the other scales and indexes did not significantly differ from the norm. For the teacher’s rating of EF behaviors, average pre-test scores for GEC, MI, and Working Memory were significantly higher than the norm. Five participants scored +1 SD or more above the mean on GEC, 6 participants on MI and 6 on Working Memory. The scores for Inhibition and Cognitive Flexibility did not significantly differ from the normative mean.
On the rating scale for behavioral problems significantly more problems were reported by parents (CBCL) compared to the normative mean for the Total Score, Externalizing, Thought Problems, and Attention Problems. Five participants scored +1 SD or more above the mean on the Total Score, 6 on Externalizing, 5 on Thought Problems and 7 on Attention Problems. For the teacher rating (TRF), the average pre-test scores differed from the normative mean for Thought Problems, and Attention Problems, with 3 of the participants scoring +1 SD or more on Thought Problems and 4 on Attention Problems. The average pre-test scores on the other scales did not significantly differ from the normative mean.
2 Trained Executive Functions outcomes
The descriptive statistics for the trained EFs at pre-test, post-test and follow-up are displayed in Table 2. Analysis using nonparametric Wilcoxon signed-rank test showed that at post-test, the sample showed significant improvement on the TMT Number–letter Switching, with a medium effect size. The other EF measures did not show significant improvement, although a trend was found for Dot Matrix and Walk Don’t Walk, with small to medium effect sizes.
Mean standard scores (SS) on the trained executive functions at pre-test, post-test and follow-up, probability (p) and effect sizes (r) of comparisons between pre-test and post-test and between pre-test and follow-up.
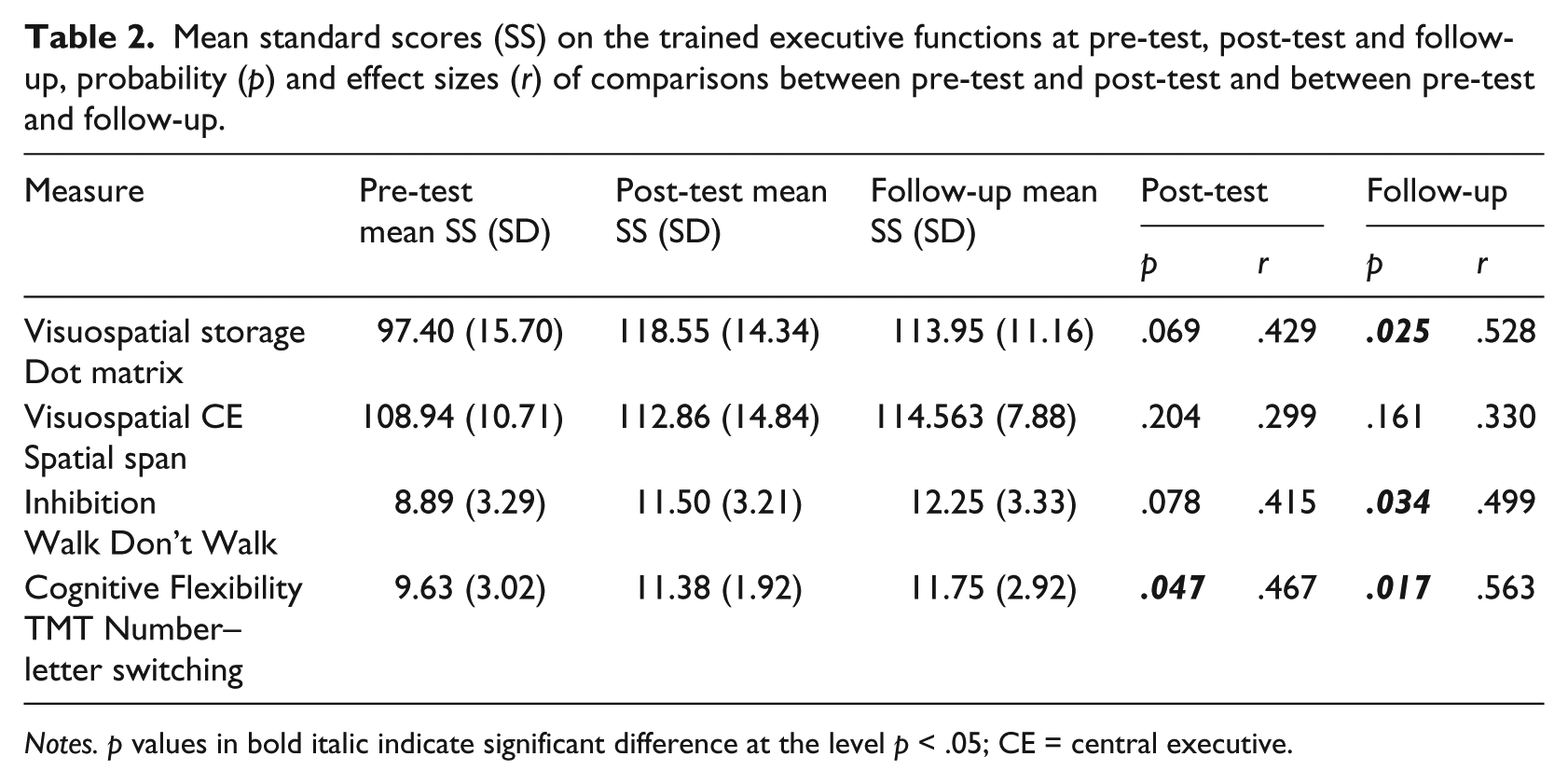
Notes. p values in bold italic indicate significant difference at the level p < .05; CE = central executive.
Between the pre-test and the follow-up, there was a significant increase in the standard scores of Dot Matrix, Walk Don’t Walk, and TMT Number–letter Switching with medium effect sizes. There was no significant change on the other measures.
3 Untrained neurocognitive functions outcomes
The descriptive statistics for the untrained neurocognitive functions and behavioral ratings at pre-test and follow-up are shown in Table 3. Analysis using nonparametric Wilcoxon signed-rank test showed significant improvement at the follow-up on Score! and Creature Counting correct, with medium effect sizes. There was no significant change on the other measures.
Mean and standard deviations of pre-test and follow-up standard scores (SS) on the untrained neurocognitive functions), probability (p) and effect sizes (r) of comparisons between pre-test and follow-up and between pre-test and follow-up.
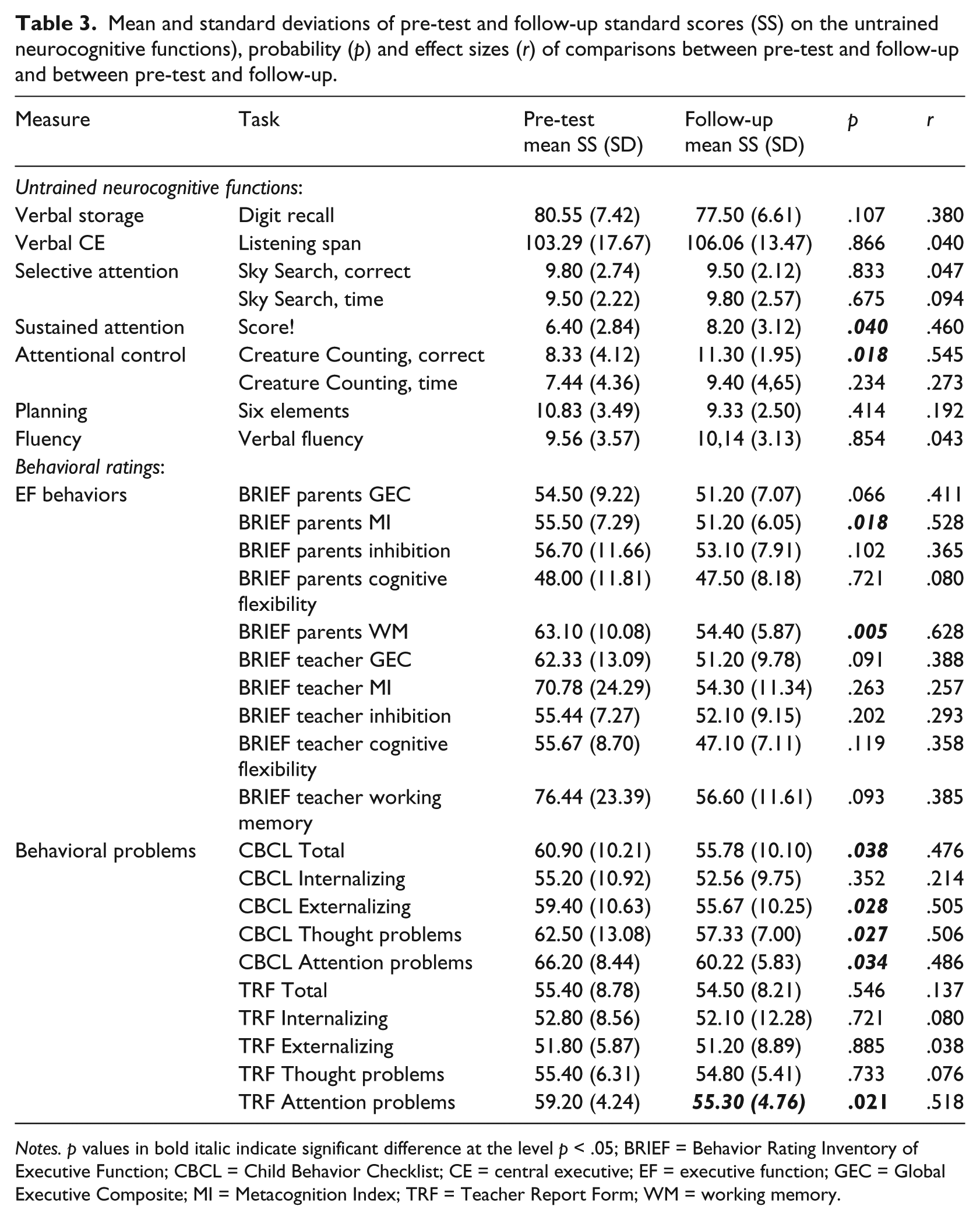
Notes. p values in bold italic indicate significant difference at the level p < .05; BRIEF = Behavior Rating Inventory of Executive Function; CBCL = Child Behavior Checklist; CE = central executive; EF = executive function; GEC = Global Executive Composite; MI = Metacognition Index; TRF = Teacher Report Form; WM = working memory.
4 Behavioral ratings outcomes
For the behavioral rating of EF, analysis using nonparametric Wilcoxon signed-rank test showed that parents reported significantly fewer problems at follow-up on the Metacognition Index and Working Memory scale of the BRIEF (see Table 3), with medium effect sizes. The other scales and indexes of the parents’ version of the BRIEF did not show significant improvement. There was no significant difference in any of the scales or indexes of the teacher version of the BRIEF.
With the exception of the Internalizing scale, parents reported significantly fewer behavioral problems on all the scales of the CBCL, with medium effect sizes. On the TRF, teachers reported significantly fewer Attention Problems, with a medium effect size. There was no significant difference on the other scales or indexes.
IV Discussion
This pilot study explores the effects of a computer-based EF training (Braingame Brian) in children with SLI. We examined whether EF training produced significant improvement on tasks of three trained EFs (visuospatial WM, inhibition, cognitive flexibility), other untrained neurocognitive functions (verbal WM, attention, planning and fluency), and/or parents and teachers’ ratings of EF and behavioral problems in a sample of 10 children with SLI.
To start, we examined the performances of the children with SLI at pre-test. The initial performances on measures of the verbal storage component of WM and sustained attention were significantly below average compared to peers of the same age. These results are in line with previous research showing clear impairments in verbal storage in children with SLI (Archibald and Gathercole, 2006b; Conti-Ramsden, 2003; Gray, 2006; Montgomery et al., 2010). Deficits in attention in children with SLI have also been reported in some previous studies (Finneran et al. 2009; Spaulding et al., 2008). Additionally, both parents and teachers reported more difficulties in WM, thought problems and attention problems on behavioral rating scales compared to the normative mean. Parents also reported significantly more overall and externalizing behavior problems, while teachers reported more overall problems in EF. Difficulties in everyday EF behaviors in children with SLI have been previously reported (Cuperus et al., 2014; Hughes et al., 2009; Vugs et al., 2013; Wittke et al., 2013).
However, it should be noted that the children with SLI performed within the normal range on a number of tasks measuring EF, namely inhibition, cognitive flexibility, verbal CE. Such performance on the measures of inhibition and verbal CE might be surprising, because significant group differences have been reported between children with SLI vs. TD children on inhibition and complex verbal span tasks in previous studies (Archibald and Gathercole, 2006b; Im-Bolter et al., 2006; Marton et al., 2007). It could indicate that the tasks included in the present study were less sensitive to detect possible impairments in inhibition or verbal CE, or that the sample size was too small to find significant group effects.
1. Does EF training produce significant improvement on tasks of trained EFs in children with SLI?
The results showed significant improvement on a task of cognitive flexibility directly after training and a positive trend for improvement in the visuospatial storage component of WM and inhibition. At 6 months follow-up the children performed significantly better on the visuospatial storage component of WM, inhibition and cognitive flexibility. The magnitude of improvement was moderate with medium effect sizes for all the outcome measures. As standard scores were used that would control for the effects of maturation this suggests a significant training effect. These findings replicate previous studies showing near-transfer effects (Gray et al., 2012; Holmes et al., 2010; Klingberg et al., 2002, 2005). Meta-analyses on the effectiveness of WM training in children with ADHD also reported medium effect sizes for visuospatial WM directly after training and at follow-up (Melby-Lervåg and Hulme, 2012; Rapport et al., 2013).
2 Does EF training produce significant improvement on other untrained neurocognitive functions or in parents and/or teachers’ ratings of EF and behavioral problems in children with SLI?
The second and third research questions concerned possible far-transfer effects on tasks of untrained neurocognitive functions and/or parents and teachers’ ratings of EF and behavioral problems in children with SLI. At 6 months follow-up, we found significant improvement on two tasks of neurocognitive functions that were not trained in the program: sustained attention and attention control. Regarding the behavioral ratings, both parents and teachers reported significantly fewer attention problems. Moreover, parents reported significantly fewer problems in WM and metacognition, thought problems, externalizing behavioral problems, and overall behavioral problems. The magnitude of improvement was moderate with medium effect sizes for all these outcome measures.
So, besides the near-transfer effects, some generalization of the training effects to other neurocognitive functions and behavior occurred in children with SLI in the current study. Although far-transfer effects were also found in some previous studies (Egeland et al., 2013; Klingberg et al., 2005), results concerning the generalization of trained task effects are not uniform. In contrast to the current findings, a recent meta-analysis showed negligible far-transfer effects of WM training (Melby-Lervåg and Hulme, 2012). This difference might be explained by the nature of the interventions. Whereas the interventions examined in the meta-analysis only included WM training, the training in the current study was a broad EF training for WM, inhibition and cognitive flexibility. In a recent study using the same EF training, Van der Oord and colleagues (2014) also found medium to large training effects for behavioral ratings of EF and attention problems in children with ADHD.
Closer inspection of the WM tasks in the current study showed only a significant training effect on the visuospatial storage task, which is closely related to the visuospatial WM task in the training. Tasks measuring the verbal storage, verbal CE and visuospatial CE components of WM did not show significant improvement after training. This suggests that the training effect on the visuospatial storage component of WM does not generalize to other untrained components of WM. Although previous research showed some limitations in visuospatial WM in children with SLI, deficits are definitely most profound in verbal WM in these children. In the current study, the largest impairment was also found on a verbal WM task: the participants scored significantly below the normative mean on Digit recall before and after the training. Therefore, the inclusion of a verbal WM training task in the training program should be considered for children with SLI. Such a domain-specific WM training might be more effective, but further research will be necessary to examine this (Kroesbergen et al., 2012).
3 Limitations
There are some important methodological limitations of this pilot study that should be considered in interpreting the results. First, the sample size was small, which makes the conclusions sensitive to random effects. It is also possible that some of the non-significant results (especially those showing a trend) would have reached statistical significance in a larger sample. Furthermore, as an initial pilot examining EF training in children with SLI, no control group was included. For this reason, test–retest effects and other experimental confounds like maturation effects cannot be ruled out (Shadish et al., 2002), although the use of standard scores would reduce maturation effects. Another concern is the use of unblinded raters. Parents and teachers were aware the children received the EF training, which may have led to biased reports. It is possible that improvement on behavioral ratings reflected expectations of outcome rather than changes solely produced by the training. On the other hand, however, it is often argued that parents are more biased in their ratings than teachers, because they are involved in supporting and motivating their child during the training while teachers are not. Previous studies on WM training in children with ADHD have not found significant effects on the behavioral ratings of teachers (Beck et al., 2010; Klingberg et al., 2005). Although the current results also showed most improvement in the behavioral ratings by parents, it is promising that we did find a significant effect on the teachers rating of attention problems.
4 Further research
Although the current pilot study must be considered exploratory due to the mentioned methodological limitations, the results support the importance of a large-scale, randomized controlled trial investigating the possible effects of the current training program in children with SLI. Further research with a robust study design should reveal whether EF training is really an appropriate and effective intervention for children with SLI. In the first place the current training effects have to be replicated, but future studies should also disentangle these effects in order to explore the specific contributions of the different trained EFs and to examine which children with SLI respond best to this intervention.
The substantial limitations in EF in children with SLI reported in previous studies, support the premise that EF training might be effective in this population. It seems plausible that good EFs are an important condition for the processes of learning various linguistic skills and that it is effective to improve these conditions. The ability to hold information in mind (working memory), to tune out irrelevant information (inhibition), and to switch the focus of attention between activities (cognitive flexibility) are involved in almost all everyday situations of learning new language abilities. If it is proven possible to improve EF in children with SLI by computerized training, this might also have an (indirect) effect on the linguistic skills of these children. Near transfer is namely the mechanism through which far transfer to other functions is hypothesized to occur (Shipstead et al., 2012). In the current pilot study however, no linguistic tasks were included. The inclusion of these tasks to examine whether the training effects generalize to nontrained language outcomes could be a valuable addition for future research.
Footnotes
Acknowledgements
We would like to thank all the children who took part in the study, and Pleun Huijbregts and Renske v. d. Wees for their assistence in the project. Further, we are especially appreciative of the assistance of Pier Prins and Albert Ponsioen from the foundation Gaming & Training.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.