
Abstract
Research findings have reported lack of reliable health data and poor management for district health information systems in low and middle-income countries (LMIC). This paper aims to review the literature on problems with health data quality management and health information evidences and evidences of best practices and use at community and district levels in LMIC, with a view to making recommendations for future research. Research citations, conference proceedings and diseases surveillance reports from 2000–2011 were accessed in PubMed, Medline, LISTA (EBSCO), CINAHL, Cochrane, and Google. Relevant studies were selected, the methodologies critiqued and synthesized. The researchers accessed 1383, and 38 were reviewed by three reviewers. Poor quality health data, low level of health information use, and poor management of health information systems were found. These findings hinder evidence-based decisions based and planning at community and district levels in LMIC. Though poor practices were found, improved health care services delivery with improved health data efficiency was found to be possible.
Keywords
It is feasible to design, implement and utilize health information systems that fit into local contexts.
Introduction
Reliable health data are the foundation of credible evidence of the health status of patients, and can assist policy makers in making decisions and plans to improve health care services delivery for better health (Haux, 2006). This review focuses on the available evidence of strategies that could facilitate data quality management and the utilization of health information in low and middle-income countries (LMIC) (Lippeveld et al., 2000; Kerr and Norris, 2010).
Data quality has to be ensured through all phases of data collection and utilization (World Health Organization, 2003). The utilization of health information includes making health information available to intended users through feedback and data sharing; and using the data for evidence-based decisions, policy-making, and planning interventions. To facilitate data management and utilization, health information management systems (HIMS) are essential. These systems refer to the components and procedures to organize data and include two entities: (1) health information data collection and utilization processes, and (2) health information system management structures.
The process of data quality management includes ensuring the reliability of data collected from data input, which includes data acquisition and verification; data management or processing, which comprises data storage, aggregation, classification, data update and data computation; and data output, that includes data retrieval and data presentation (Tan, 2001 p.9). Health professionals and policy makers rely on available data as reported from healthcare facilities to make decisions and the decisions they make depend directly on the quality of the data they receive (AbouZahr and Boerma, 2005).
Globally, research findings have reported poor quality of health data (Calle et al., 2000; Goeree et al., 2009) and underutilization of health information for planning and decision-making (Corrao et al., 2009). These problems have hindered decision-making, planning processes and the performance evaluation of health care programs and diseases outcomes (Corrao et al., 2009). It is also of particularly major concern in LMIC, where health information systems are newly initiated within resources constrained contexts (World Health Organization, 2006; Bosch-Capblanch et al., 2009).
In most LMIC, the health information systems are also paper-based and often decentralized at district level (LaFond and Siddiqi, 2003). The district level information systems (DHIMS) are used to compile monthly reports on geographical, clinical and administrative from routine health services data, as well as disease notification from epidemiological surveillance data (Lippeveld et al., 2000). Most LMIC use paper-based data collection processes at primary health care level and paper and computer-based health information systems at district level (Haux et al., 2007; Heywood and Rhode, 2001). However, paper-based information systems are often found to generate data with poor quality and are underutilized within the health information management (Lium et al., 2008).
It is important to strengthen health systems in LMIC through good data management and data availability for better decision-making (Lippeveld et al., 2000, Haux, 2006). As there are concerns that quality health information is lacking and evidence-based planning and decision-making might be affected, the reported progress towards Millennium Development Goals by LMIC may be questionable (AbouZahr and Boerma, 2005; Kerr et al., 2007). It is in the light of these concerns that we reviewed and summarized the literature on data quality management and health information use at community and district levels in LMIC.
Purpose of the review
The objectives of the review were to:
Identify and review studies that evaluated health data quality management processes, health information use, and health information system management issues in LMIC. Critique research methods used in those studies. Describe problems with health data quality management and health information use in LMIC and identify reported best practices for implementation.
Methods
MeSH terms in the PubMed and their synonyms were identified to extensively search and retrieve relevant literature on quality management, health information use, and health information management structures in LMIC from 2000 to early 2011.
The following search terms were used:
Relevant published papers, reports and conference proceedings were retrieved. No manual searching was performed. Only studies reporting on data quality management and health information in or relevant to LMIC in the English language were included. Two reviewers independently screened the titles and abstracts of all retrieved studies and disagreements were referred to the third reviewer to resolve. Once the studies were selected, the full articles were retrieved, reviewed for quality of study design type and relevant information extracted.
Results
The reviewers identified 1383 studies from the initial search. Of these, 253 (18.3 percent) were selected after the exclusion of irrelevant studies. A further 70 (5.1 percent) studies remained after studies not applicable to LMIC were also excluded. Based on the quality of the study designs, 38 studies (2.7 percent) were selected for full review (See Figure 1), though the 38 studies included three low quality design studies due to the nature of the information provided by these studies.
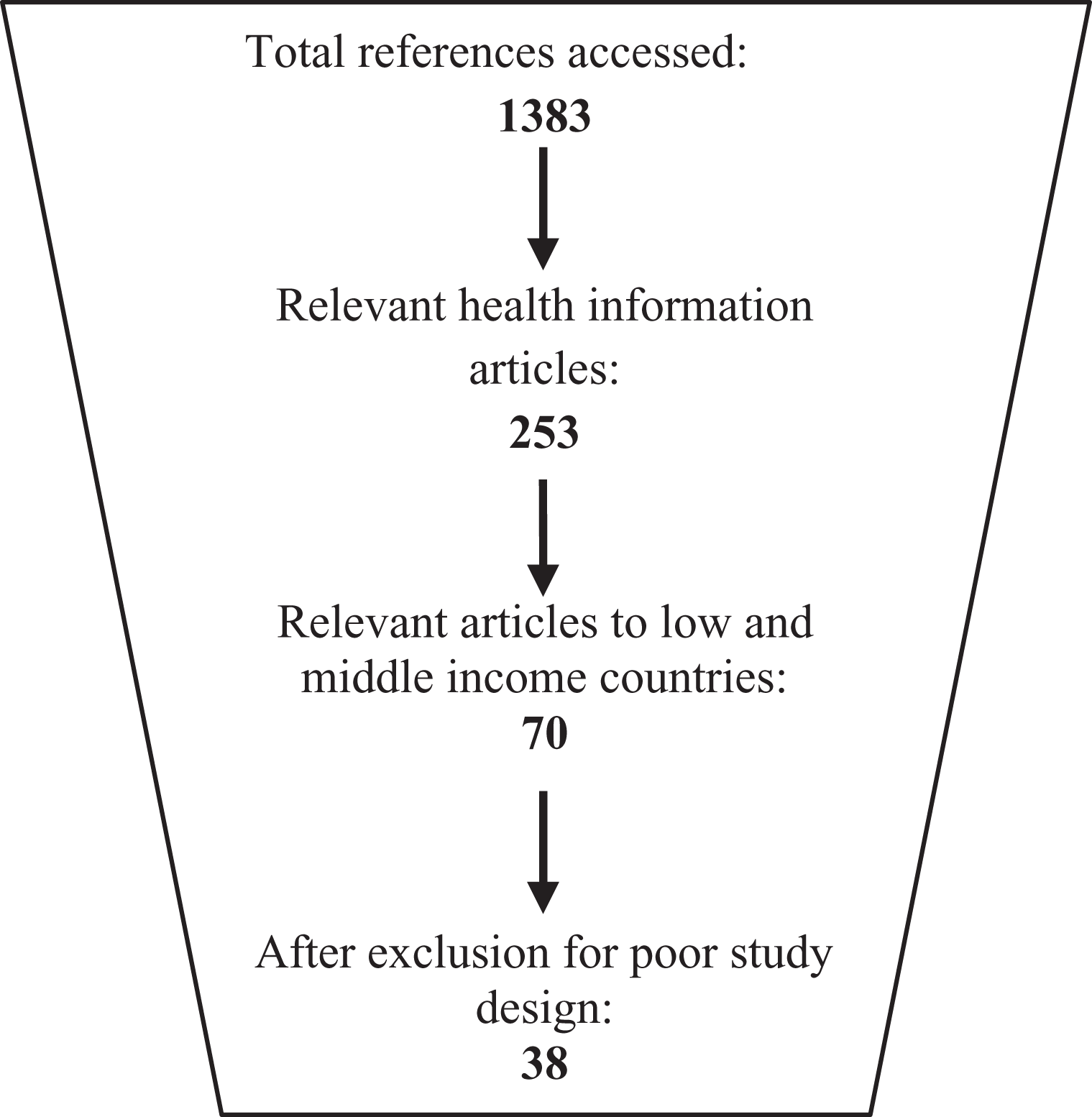
Flow diagram for study selection.
Characteristics of reviewed literature
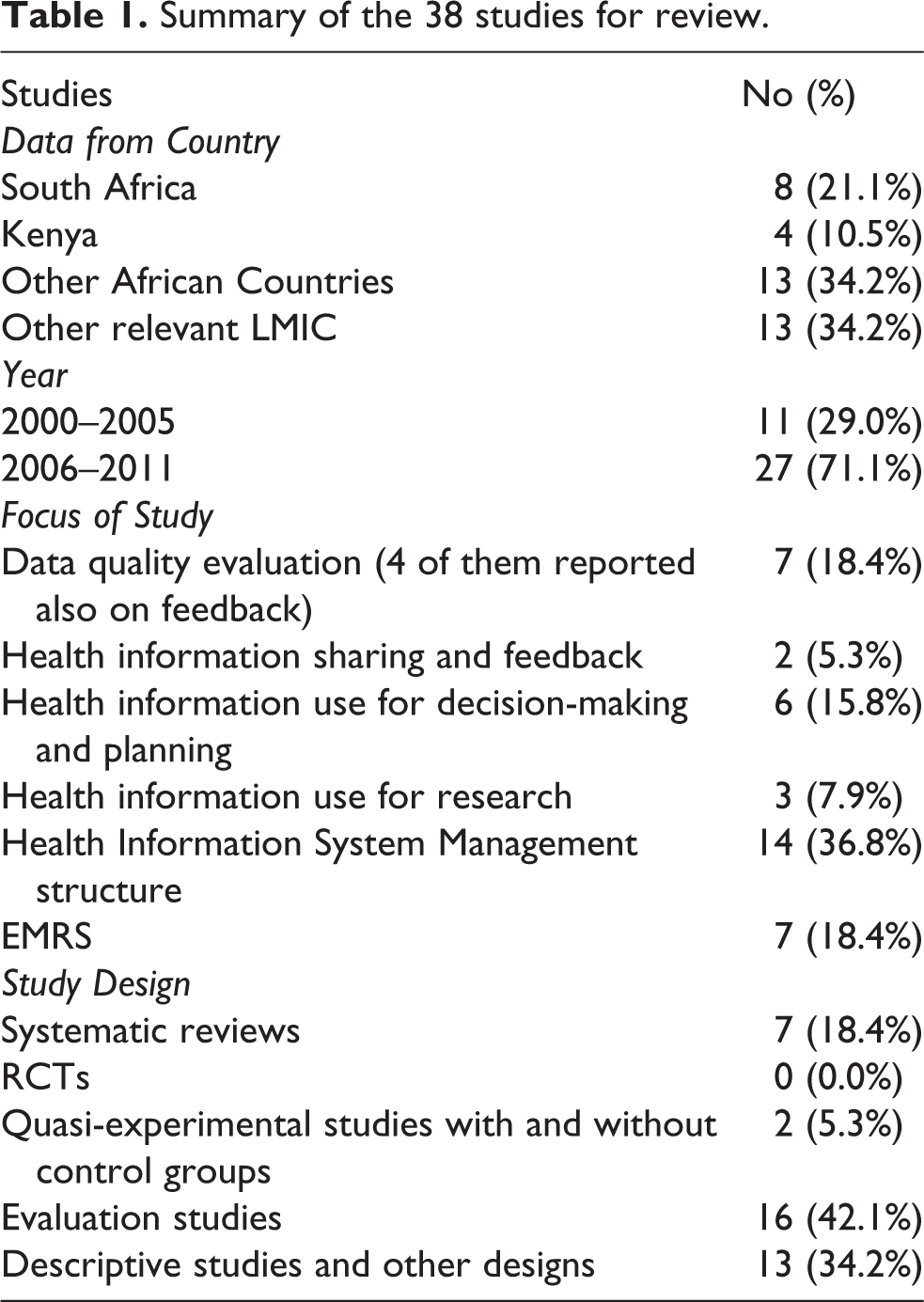
Twenty-five of the 38 studies (65.8 percent) were conducted in Africa, 16 (42.1 percent) were evaluation studies, 13 (34.2 percent) were descriptive studies and seven (18.4 percent) were systematic reviews (Table 1).
Summary of the 38 studies for review.
Data quality management studies
In reviewing the studies that reported on the quality of data found in LMIC, the following criteria identified by the reviewers were used: accuracy or correctness, completeness, timeliness, comprehensiveness, consistency, accessibility, reliability and acceptability of data. Out of the 38 studies, seven (18.4 percent) studies (Odhiambo-Otieno, 2005; Ronveaux et al., 2005; Garrib et al., 2008; Bosch-Capblanch et al., 2009; Mate et al., 2009; Harper et al., 2011; Heunis et al., 2011) specifically evaluated the quality of health data (see Table 2). Of the seven studies, four (57.1 percent) were descriptive case studies evaluating the quality of the data collected in health facilities (see Table 2).
Summary of studies evaluating health data quality.
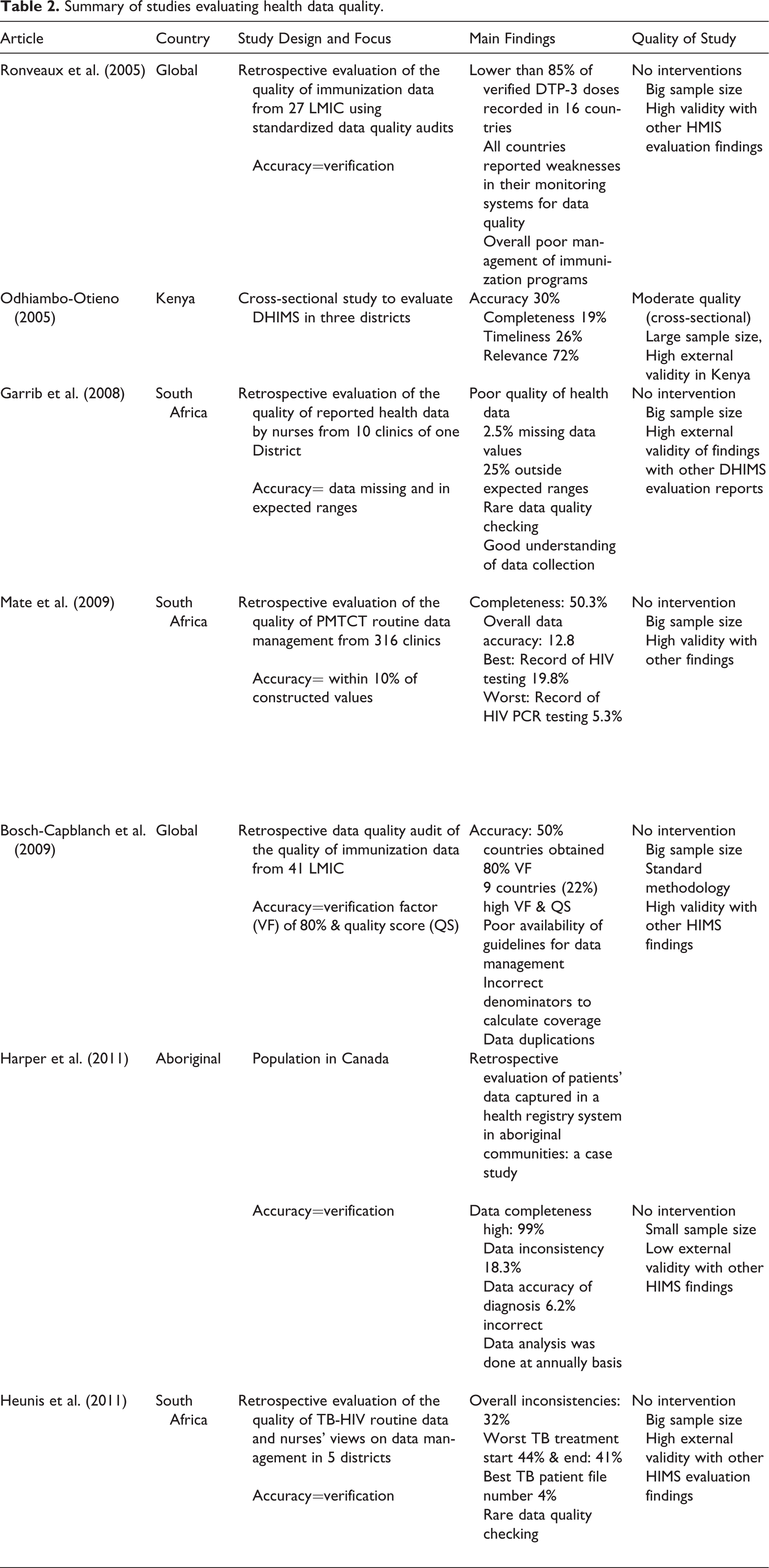
None of the studies reported on all the criteria of data quality. Overall, the seven studies reported poor health data quality management in three domains. These include: (1) Incompleteness of data: Though 99 percent completeness was reported in a health registry for an aboriginal community in Canada (Harper et al., 2011), data completeness was poor in LMIC with missing data ranging from 19 percent (Odhiambo-Otieno, 2005) to 50.3 percent (Mate et al., 2009). (2) Inconsistencies in data collection and processing:Levels of inconsistency were reported for country immunization programs with only nine (22.0 percent) out of 41 countries reporting consistent data (Bosch-Capblanch et al., 2009). There were also inconsistencies in general for TB data (32.0 percent) (Heunis et al., 2011) and diagnosis data in health registries (18.3 percent) (Harper et al., 2011). (3) Inaccuracy or incorrectness: Though inconsistent definitions of accuracy were used, the study using a verification factor to assess accuracy showed that only 50 percent of the countries obtained 80 percent accuracy (Bosch-Capblanch et al., 2009). Likewise, in a study on HIV data accuracy, only 12.8 percent of PMTCT (Preventing Mother-to-Child Transmission) data, 19.8 percent of HIV Counselling and Testing (HCT) data and 5.5 percent of HIV PCR testing data of babies born to HIV mothers were reported as accurate (Mate et al., 2009). Other issues identified were poor usage of standard data collection tools, data duplications, multiple registers (Garrib et al., 2008; Bosch-Capblanch et al., 2009), poor and infrequent data quality checking procedures (e.g. tally sheets) and inconsistencies in the use of denominators to estimate coverage (Bosch-Capblanch et al., 2009). Though a lack of guidelines for data quality management was reported (Bosch-Capblanch et al., 2009), one study reported good understanding of the data collection and data collation processes (Garrib et al., 2008).
Studies on utilization of health information
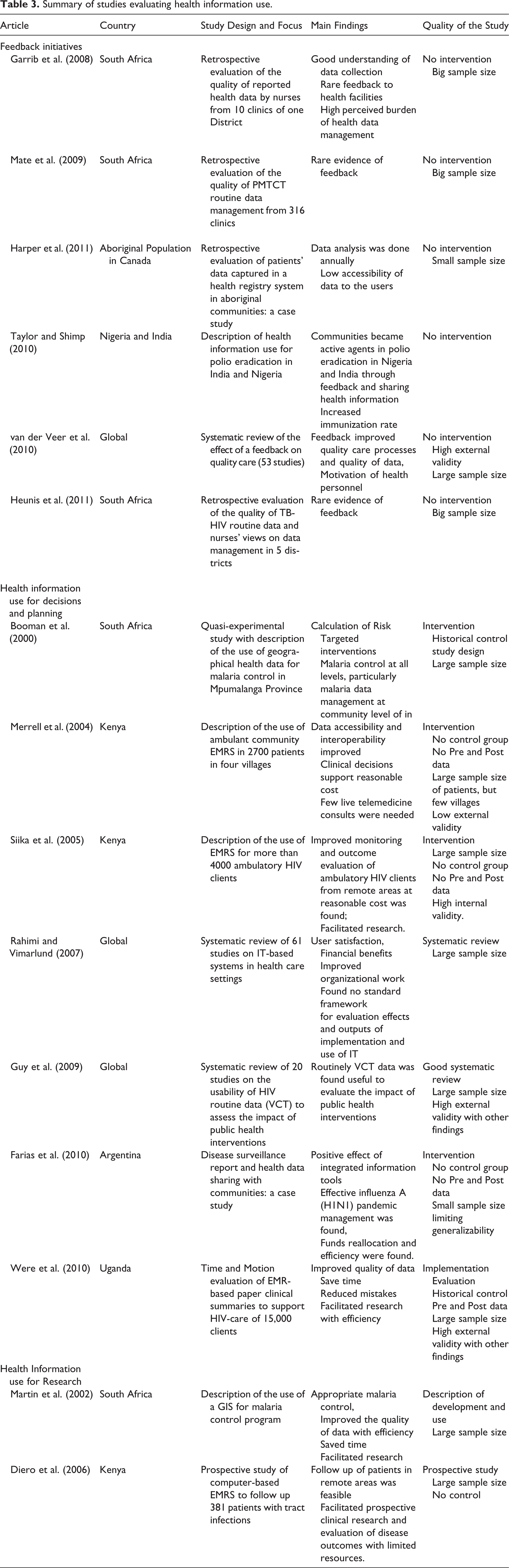
Fifteen studies were found that reported on the utilization of health information, six on evidence of feedback initiatives and nine on the utilization of health information (see Table 3).
Summary of studies evaluating health information use.
Health information sharing and feedback.
Of the six studies reporting on feedback initiatives (Garrib et al., 2008; Mate et al., 2009; Harper et al., 2011; Taylor and Shimp, 2010; van der Veer et al., 2010; Heunis et al., 2011) (see Table 3), two studies specifically reported infrequent evidence of feedback (Garrib et al., 2008; Heunis et al., 2011). Garrib (2008) reported incorrect usage of data collation tools, little analysis, interpretation or utilization of data and infrequent feedback to clinics (Garrib et al., 2008). Similarly, the study by Heunis et al. (2011) found lack of supervision to address data quality issues resulted in clinic personnel being unaware of their performance.
Overall, factors associated with effective feedback in the reviewed studies were: improved quality of data, motivation of the health care personnel and their expectations, and the availability of necessary equipment that enforce quality improvement.
The improvement of data quality as a result of feedback was reported from three studies. A systematic review on how medical registries provide feedback to health care providers found that feedback initiatives could positively influence the process and quality of care (van der Veer et al., 2010). This was also illustrated in a study in India and Nigeria which found that by sharing health information with the community, there was a significant increase in immunization (Taylor and Shimp, 2010). Similarly, in clinics where health information was shared among health care providers and the clinic received feedback, TB data were used for planning, monitoring and evaluation of the performance and outcome of the TB programs (Heunis et al., 2011).
Utilization of health information for decision-making and planning
Two systematic reviews (Rahimi and Vimarlund, 2007; Guy et al., 2009) and two studies (Booman et al., 2000; Farias et al., 2010) reported on practices in using health information for public health interventions planning (see Table 3). These included: A systematic review of moderate quality on the application of IT-based systems in health which showed positive results in user satisfaction, financial benefits and improved organizational work (Rahimi and Vimarlund, 2007); A good systematic review on the usability of HCT data in assessing the impact of public health interventions which concluded that data from routinely collected data was useful for public health interventions in resource limited settings (Guy et al., 2009); Geographical data used for targeted risk identification and malaria control in South Africa (Booman et al., 2000); and Influenza (H1N1) pandemic control which used an integrated IT-based HIMS to evaluate program performances and disease outcomes in Argentina (Farias et al., 2010).
Three studies of high to moderate quality reported on evaluations of utilization of electronic medical records systems (EMRS) and diagnosis supporting tools to improve patients’ management by using patient-specific clinical summaries in Uganda and Kenya (Merrell et al., 2004; Siika et al., 2005; Were et al., 2010). In Kenya health care providers in remote areas reported getting clinical decision support through health data sharing with medical experts (Merrell et al., 2004); and in Uganda and Kenya, the use of EMRS were shown to be efficient in managing HIV/AIDS patients, monitoring and evaluation of diseases outcome, tracking missing patients and infants enrolled in PMTCT from remote areas, saving time spent on care and facilitating research (Siika et al., 2005; Were et al., 2010).
Health information use for research
Four studies (Martin et al., 2002; Siika et al., 2005; Diero et al., 2006; Were et al., 2010) reported on the utilization of health information for research (see Table 3). Reports of prospective clinical studies using EMRS which could be undertaken at larger scale were useful to evaluate disease outcomes in Kenya (Siika et al., 2005; Diero et al., 2006) and Uganda (Were et al., 2010). Lastly, the study by Martin et al. (2002) described the efficiency in undertaking a research-based, Geographical Information System (GIS) for disease surveillance to influence health programs planning for Malaria Control Programs in South Africa (Martin et al., 2002).
Studies on practices for health information management system structure
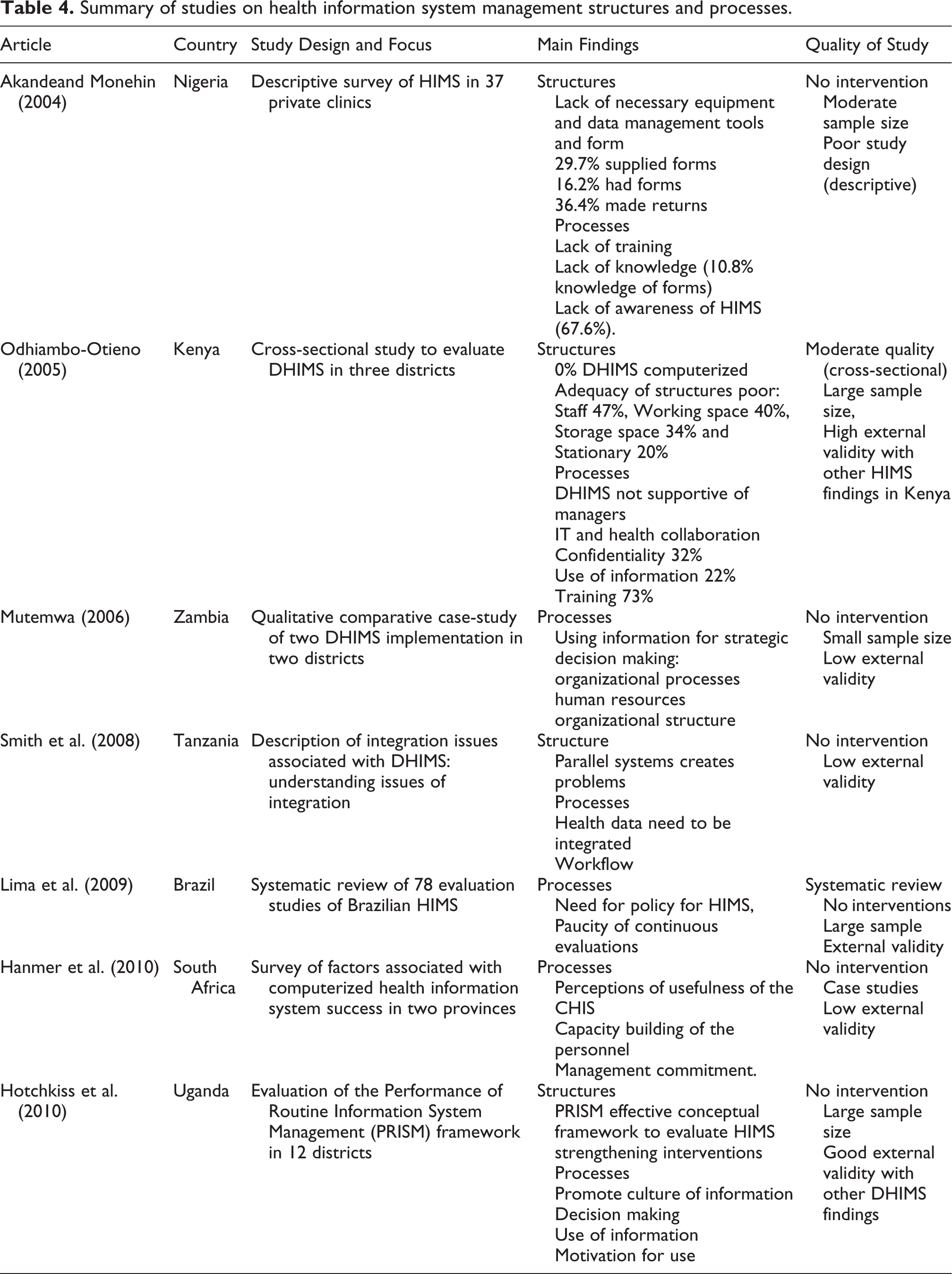
Ten studies were found on Health Information Management System (HIMS) structure and processes. Seven studies evaluated structural factors and processes in DHIMS in South Africa, Kenya, Tanzania, Zambia, Mozambique and Nigeria (see Table 4), while three studies reported on interventions to improve data quality and feedback (see Table 5).
Summary of studies on health information system management structures and processes.
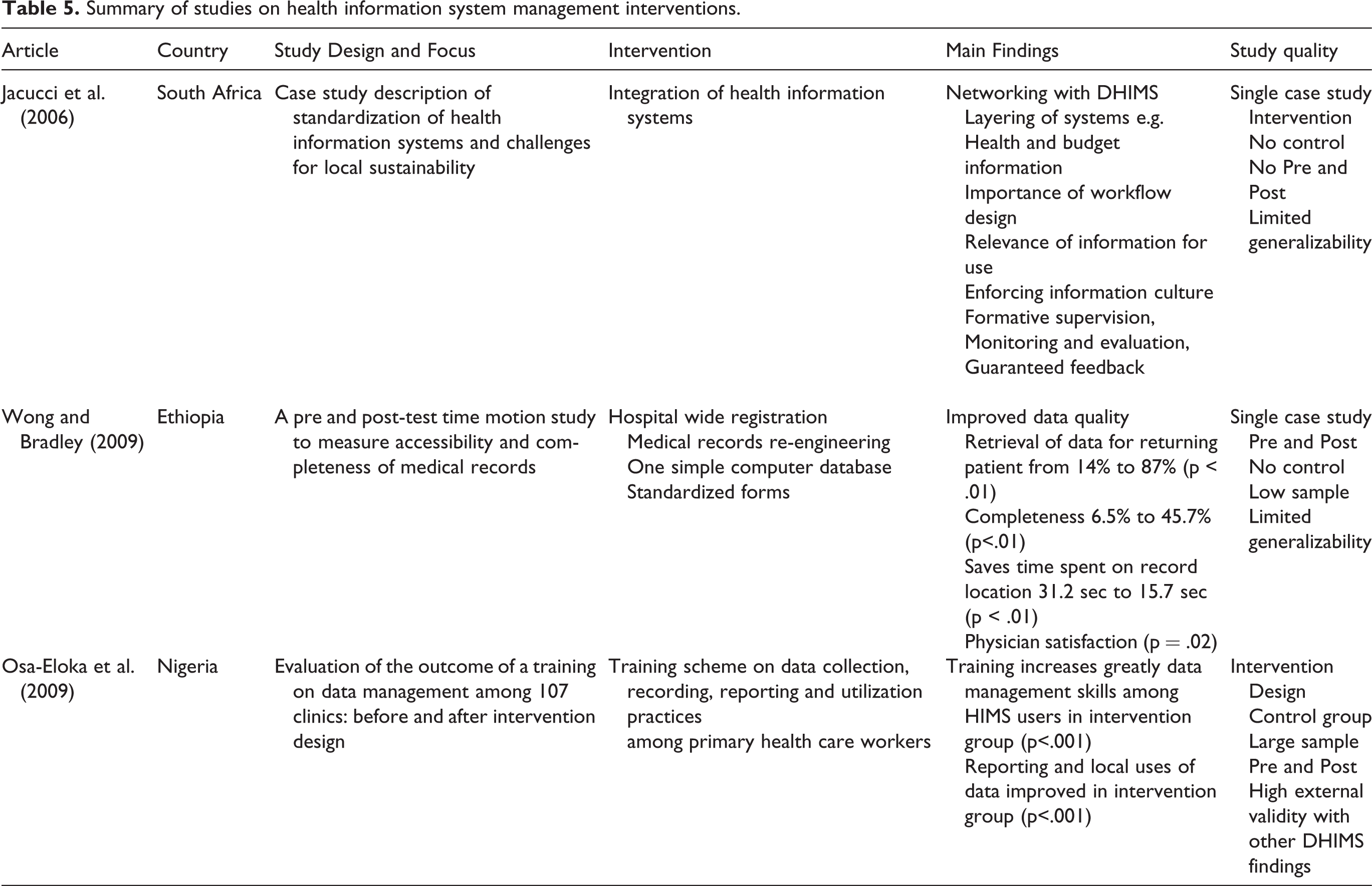
Summary of studies on health information system management interventions.
District Health Information System management structures and processes
Issues and problems with DHIMS described in the studies included: (1) Structural problems, namely: lack of clear policy for health information systems (Lima et al., 2009), lack of resources and facilities, lack of management commitment, pressure for good results, overloading forms to complete for different programs and parallel reports (Mutemwa, 2006), lack of feedback and poor collaboration between information technology experts, managers and users, especially in the conception phases (Odhiambo-Otieno, 2005), and parallel health information systems and lack of integration (Smith et al., 2008); (2) Behavioural issues, namely: lack of information culture and few evaluation studies which hindered comprehensive data quality assessments (Akande and Monehin, 2004; Hotchkiss et al., 2010); and (3) Technical issues, namely: use of inappropriate and complex technology, lack of training, lack of skills, lack of pre-operational and post-implementation evaluation (Odhiambo-Otieno, 2005).
Interventions to improve data quality and feedback
Specific interventions to improve data quality were reported in studies in South Africa (Jacucci et al., 2006), Ethiopia (Wong and Bradley, 2009) and Nigeria (Osa-Eloka et al., 2009). One district in South Africa overcame problems associated with poor quality data management through formative supervision, monitoring and evaluation, guaranteed feedback to increase the quality of health data and the integration of data management and networking actions at all district levels (Jacucci et al., 2006). The following outcomes from their interventions were reported: improved quality of reported data from health facilities, increased accessibility of data, enhanced skills in the use of data collection tools and data analysis software, increased utilization health information use, and tangible management commitment to enforce good practice culture (Jacucci et al., 2006). In addition, daily quality data checks, utilization of health information to plan health interventions, and the use for financial negotiations with the district were observed (Jacucci et al., 2006). A study conducted in Ethiopia found that using hospital wide registration, one computer database, medical records re-engineering and standardized forms improved the retrieval of records, time spent on retrieval and improved records completeness (Wong and Bradley, 2009). And lastly, a study in Nigeria showed that training greatly increases data management skills and reporting and local use of data among HIMS users (Osa-Eloka et al., 2009).
Studies on practices for Electronic Medical Information System Management
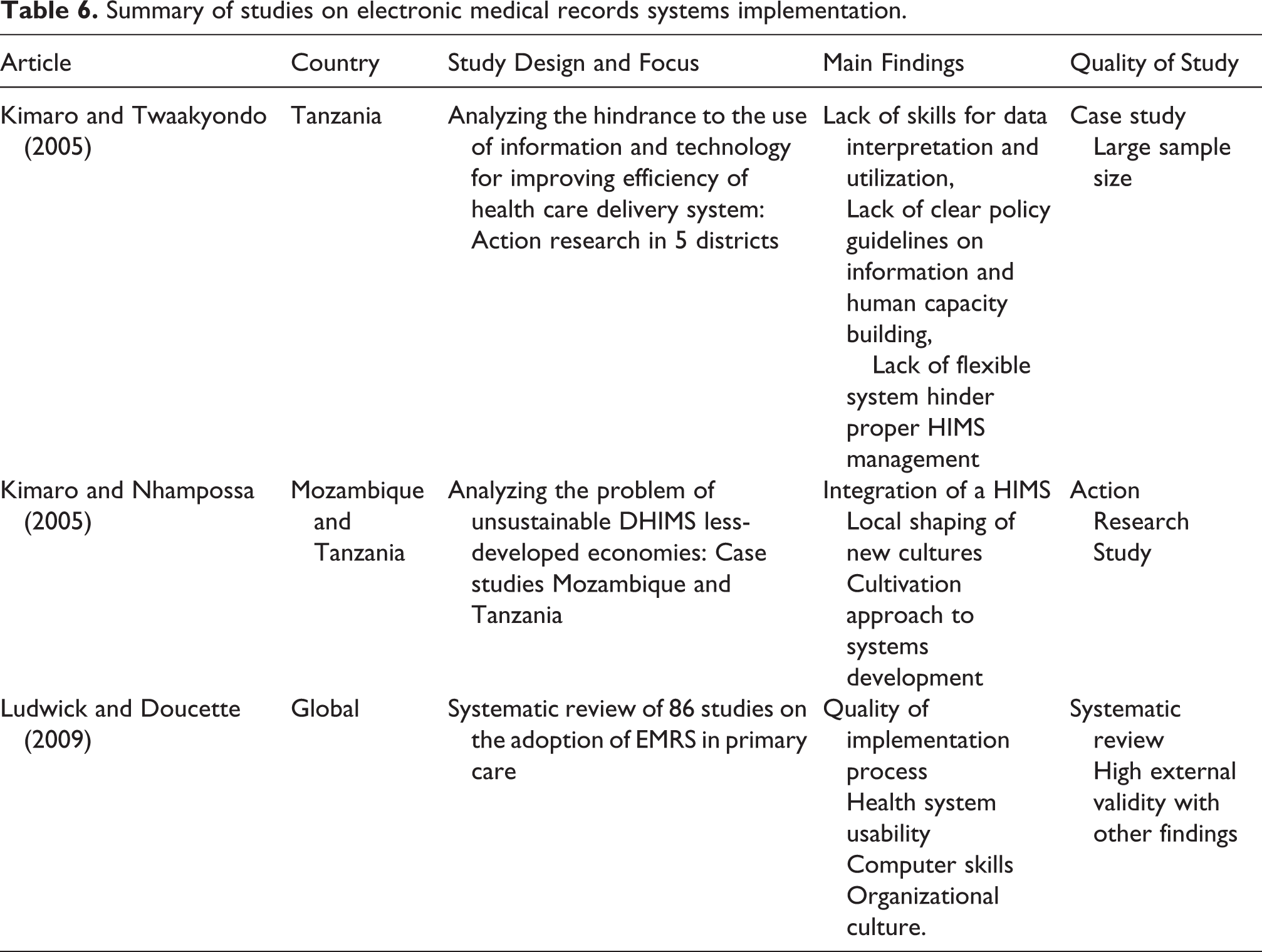
Internationally there has been a dramatic increase in the use and popularity of technology to develop electronic medical record systems (EMRS) for health data management. Though the context of LMIC makes the application of these systems difficult, 10 studies were found on the use of EMRS in LMIC. Three studies focused on factors affecting EMRS implementation in LMIC (see Table 6) and seven studies evaluated the effectiveness of the EMRS interventions in LMIC (see Table 7).
Summary of studies on electronic medical records systems implementation.
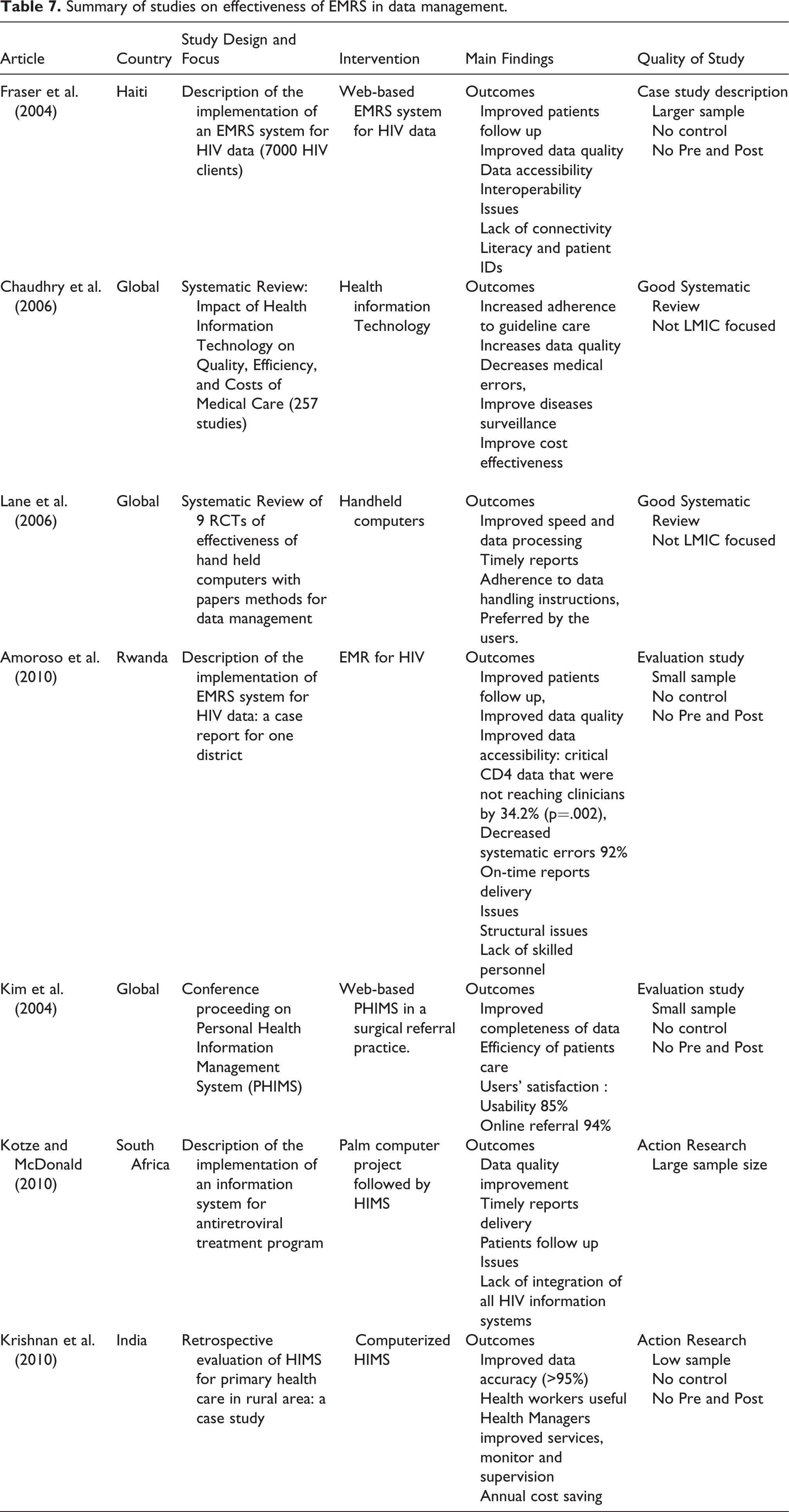
Summary of studies on effectiveness of EMRS in data management.
Electronic Health Information System implementation processes
The studies reviewed identified a number of factors which may encumber an EMRS implementation (Table 6). A case study in Tanzania found that poor information literacy, unclear policies and inflexible systems hindered the implementation of an EMRS (Kimaro and Nhampossa, 2005). A systematic review conducted on the adoption of EMRS implementation in primary care showed that the quality of the implementation process is as important as the quality of the EMRS (Ludwick and Doucette, 2009). Other important factors identified were personnel satisfaction, usability and interoperability of EMRS for patient care and data sharing for clinical support and referrals (Ludwick and Doucette, 2009), and integration of HIMS systems (Kimaro and Nhampossa, 2005). Ludwick and Doucette (2009) also found that strong leadership, sound management, well established standards, staff training and due consideration of the technical and social context are fundamental to the success of any HIMS implementation.
Evaluation of effectiveness of EMRS in data management
Studies evaluating the effectiveness of technological interventions to improve data collection focused on EMRS (6 studies and a systematic review) and hand held devices for data collection (1 systematic review) (see Table 7).
A study conducted in India found that using a computerized HIMS assisted program managers in Primary Health Centres in the monitoring and supervision of their daily activities, funds allocation and resulted in time efficiencies, increased data quality, and improved health services delivery (Krishnan et al., 2010). A systematic review on the impact of health information technology on quality, efficiency, and cost of medical care (Chaudhry et al., 2006) concluded that the health information technology improves the quality care and efficiency through adherence to guidelines and protocols for decision support.
Three studies conducted on HIV/AIDS Management systems in South Africa (Kotze and McDonald, 2010), Rwanda (Amoroso et al., 2010) and Haiti (Fraser et al., 2004) showed improved monitoring and evaluation of antiretroviral data and HIV/AIDS treatment across the three countries (Fraser et al., 2004; Merrell et al., 2004, Amoroso et al., 2010). In Rwanda, the use of detailed HIV/AIDS and TB computerized data facilitated patient follow up, improved data accessibility and quality (92 percent reduction in systematic errors) and improved patient care (Amoroso et al., 2010). In terms of capturing data using hand held computers, the systematic review showed that hand held computers were better than paper use for data collection in terms of speed of data collection, ease of data processing, timely delivery of reports, adherence to data handling instructions, and were the most preferred by the users (Lane et al., 2006).
Structural problems in EMRS identified in Haiti and Rwanda included the lack of necessary infrastructure and equipment, inadequate program officers at different sites, and communication issues (Fraser et al., 2004; Amoroso et al., 2010).
Discussion
International evidence has shown that health information systems are fundamental to the delivery of quality health care (Chaudhry et al., 2006). In LMIC the burden of diseases such HIV/AIDS and the need for health information systems to coordinate care and treatment, is accompanied by concerns that paper-based records are no longer adequate and should be replaced by more efficient EMRS (Kalogriopoulos et al., 2009). Countries in Europe and the USA are increasingly using EMRS to improve healthcare service delivery quality (Williams and Boren, 2008; Ali et al., 2011). Unfortunately LMIC face many challenges in implementing and utilizing health information systems, including concerns about quality of data and inadequate communications technology, human expertise and financial resources (Williams and Boren, 2008).
For health decision makers in LMIC, these challenges are compounded by a lack of high quality evaluations of health information systems and effective data quality management strategies (Chaudhry et al., 2006). Similarly, in this review of health information system evaluation studies, study quality ranged from high quality systematic reviews to low quality descriptions of single case studies. Despite these limitations, the reviewed studies showed that the use of technology could improve both the quality and the use of health data in LMIC and could lead to good outcomes such as: improved patients’ follow up from remote areas, increased users’ satisfaction, adherences to data quality management standards, efficient management of health clinics, hospitals and public health programs and improved guideline adherence (Oluoch et al., 2012). In addition, the review showed that health information systems structures were found very helpful in overcoming problems associated with paper-based health information systems and facilitating clinical and health systems researches within limited resources contexts.
While the benefits of health information systems are clear, adapting new health information systems has proven difficult in the past and rates of use have been limited (Chaudhry et al., 2006). In LMIC, the overall aim of a health information system, which is to facilitate care, may not be reached, with the severe resource constraints hindering implementation, data quality management and utilization of health information. This review also supported this finding with studies identifying two major problems hindering data quality management: Firstly, technical infrastructure issues such as unreliable electric power and erratic Internet connectivity and clinicians’ limited computer skills (Oluoch et al., 2012); and secondly, data quality management issues such as the lack of policies and guidelines, training for health personnel, required equipment, good communication and networking actions among all stakeholders of HIMS, supervision, monitoring and continuous evaluations, and information culture at different levels of district health information systems.
There are also evidence that in LMIC data are incomplete, inaccurate, unreliable and not timely (Simba, 2004) and that poor data quality management have a major impact on the utilization of health data and the potential use of an EMRS. Against a 75th percentile standard for data quality, the reviewed studies reported poor quality of data from LMIC health facilities and district health information systems. One of the main problems was data incompleteness with no LMIC country reporting data completeness over 50 percent. Though accuracy was also measured using different verification methods, data inconsistencies and inaccuracies were common and often the reviewed studies did not report the standards against which they appraised the level of data quality. Inaccurate and incomplete data may result in data not being seen as reliable enough to inform on programs performance and disease outcomes or to be used for decision making and planning and that EMRS might expedite the dissemination of wrong or poor data (Simba, 2004)
However, with accurate data, feedback to users, information sharing, decision-making and program planning based on available health information could be good standards of quality usage of health information. Our review showed that good practices in data quality management and utilization of health information exist with a few studies reported using data for public health interventions and research. However, the review also showed that problems outweighed the good practices with health data being neither accurate (correct) nor reliable, poor evidence of feedback practices, district health information systems being poorly managed, a lack of information culture in LMIC, problems implementing HIMS and a failure to deliver reliable health information for better decisions and planning. To improve utilization of health information, it is believed that the establishment of strong leadership, using project management techniques, establishing standards and training their staff is essential for implementation success (Ludwick and Doucette, 2009) and more work needs to be done to overcome the barriers to implementation such as technical infrastructure and care providers’ computer illiteracy (Oluoch et al., 2012). Similarly, this review identified a number of key strategies to improve the implementation and utilization of health information systems. Specifically relevant for LMIC were the development of integrated health information systems, reengineering of work flow and medical records, management commitment to create an information culture and training of data collectors and users. In addition, the development of EMRS with open standards and sharable components using open source software should also be developed tailored to the population, location, and availability of resources (Kalogriopoulos et al., 2009).
Conclusion
This review reinforces the need for well-designed studies evaluating the role and feasibility of health information systems which are customized to LMIC localities (Ali et al., 2011). In these studies, factors specific to implementation of health information systems and EMRS in LMIC settings should be addressed before such countries can demonstrate their full benefits. Similarly, it is important that existing health information systems take significant steps to improve their data management processes so that quality health data is available timely to all users to improve health services delivery. However, despite the challenges faced by LMIC, it is believed that it is feasible to design, implement and utilize health information systems that fit into local contexts and can contribute to the delivery and monitoring of quality health care (Williams and Boren, 2008).
Footnotes
Conflict of interest
No conflict of interest associated with this work.
Contribution of authors
We declare that this work was done by the authors named in this article and all liabilities pertaining to claims relating to the content of this article will be borne by the authors. The authors conceived and designed the study together, and the first author collected and analysed the data.