
Abstract
This paper reports on the Mobile Healthcare Information For All By 2015 (mHIFA) initiative led by the Health Information For All 2015 (HIFA2015) 2012-2015 Challenge Working Group. It discusses the preliminary findings of a scoping exercise to identify global current, completed and planned projects that use mobile phones to provide healthcare information, particularly maternal, child and first-aid, in low- and middle-income countries, that appear to be aligned to the mHIFA Goal. Despite a plethora of mHealth projects on a wide range of mHealth topics, only nine projects were closely related to the mHealthcare Goal. Findings of the scoping exercise were made available on the HIFA2015 Discussion Forums to instigate feedback from key healthcare and telecom stakeholders. An assessment tool was created to help telecom providers and potential providers to assess relevance to the mHIFA Goal.
There is a gap in the provision of mobile applications that provide maternal, child health and first-aid information.
Introduction
There is an urgent need to improve the availability and use of healthcare information in developing countries. This need was highlighted in three of the United Nations Millennium Development Goals (MDGs) (2000) that specifically addressed health: MDG 4 ‘Reducing child mortality’, MDG 5 ‘Improving maternal health’ and MDG 6 ‘Combat HIV/AIDS, malaria and other diseases.’ Rapid advances in mobile technologies and applications and the continued growth in coverage of mobile cellular networks are all driving a change to improve healthcare (mHealth Alliance, 2014). Many health care applications have been created for mobile platforms in developed countries and in developing countries there are great opportunities for mHealth to use mobile devices (Martinez-Perez, de la Torre-Diez and Lopez-Coronado, 2013; Vital Wave Consulting, 2009). mHealth is of particular interest in developing countries, where widespread mobile networks and access to devices are connecting people like never before (Goel et al., 2013). There is no standard definition of mHealth; as defined by the Global Observatory for eHealth (GOe) of the WHO, it is “medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants (PDAs), and other wireless devices.”
This paper reports on the Mobile Healthcare Information For All By 2015 (mHIFA) initiative led by the Health Information For All 2015 (HIFA2015) 2012–2015 Challenge Working Group. It discusses the preliminary findings of a scoping exercise to identify global current, completed and planned projects that use mobile phones to provide health information, particularly maternal, child and first-aid information, in low- and middle-income countries, that appear to be aligned to the mHIFA Goal described below, and outlines future stages of the initiative.
Health Information For All 2015 (HIFA2015)
First, some background about HIFA2015. Ten years ago, Godlee et al. (2004), in the article “Can we achieve health information for all by 2015?” discussed how, despite the information revolution, there was little if any evidence that the majority of health professionals in the developing world were better informed than they were 10 years prior. The paper called for the World Health Organization (WHO) and others to champion the goal of Healthcare Information for All by 2015. The HIFA2015 knowledge network and campaign is a direct response to that challenge. The campaign has grown to become an ever-expanding “network of networks.”
HIFA’s 12,000 members include a diverse group of health workers, information professionals, policymakers, publishers, librarians, researchers, social scientists, journalists, and others – all working together towards the HIFA vision: a world where every person and every health worker has access to the healthcare information they need to protect their own health and the health of those for whom they are responsible. HIFA’s members come from 2,500 organizations in 174 countries worldwide. HIFA contributes to the broader goal of the Global Health Workforce Alliance: “All people everywhere will have access to a skilled, motivated and supported health worker, within a robust health system” (HIFA2015, 2014a).
HIFA members interact in five professional online Global Discussions Forums: HIFA2015, CHILD2015, HIFA-Portuguese, HIFA-EVIPNet-French and HIFA-Zambia in collaboration with the WHO and others. These discussions contribute to an experiential multilingual database, HIFA VOICES, which concerns information needs and how to meet them. This database has full functional linkage to the Human Resources for Health Global Resource Center, the world’s leading database on Human Resources for Health. HIFA has also helped to inform WHO policy guidelines (HIFA2015, 2014b). Over 190 international health and development organizations have officially expressed their support for HIFA.
The HIFA 2012–15 Challenge Working Group (members are listed in the Acknowledgements) proposed and leads the mHIFA Goal.
mHIFA Goal and Problem
The mHIFA Goal is that: “by 2015, at least one telecoms provider, in at least one country, will endorse the vision of Health Information For All, and will provide free access to essential healthcare knowledge in the local language, preloaded on all new mobile phones they may sell and freely downloadable to all those who already have mobile phones.”
The Goal addresses the problem that everyone needs affordable access to timely, reliable, easily assimilated and actionable healthcare knowledge and healthcare information. This is especially important in low- and middle- income countries, where health workers may not be available. Often the fate of people who become ill or injured is highly dependent on the decisions and actions of their fellow citizens or family members. These decisions and actions are largely dependent on the availability of basic healthcare knowledge and information (HIFA2015c). For example, worldwide, over a quarter of a million women die each year, many in sub-Saharan Africa, from mostly preventable complications related to pregnancy and childbirth. The knowledge, decisions and actions of citizens have the potential to save the lives of these women. Another example is childhood malaria, where fast and appropriate diagnosis and treatment of malaria is extremely important in reducing child mortality.
The Goal is specifically concerned with the health information needs of citizens, parents and children, in recognition of the huge and largely unrealized potential of mobile phones to meet basic healthcare information needs. The ubiquity of mobile devices in developing countries presents an opportunity to improve healthcare. According to the International Telecommunication Union (ITU), the United Nations specialized agency for information and communication technologies’ Facts and Figures 2013, mobile phone penetration rates in developing countries stand at 89 percent (International Telecommunication Union, 2013). Increasingly, there is the realization that “Mobile communications can help bridge a huge knowledge gap and reimagine healthcare across Africa…But what is unexpected is the life-saving role these handsets are beginning to play in helping to bridge gaps in our knowledge” (Berkeley, 2013). Oyeyemi and Wynn (2014) in the ‘Safe Motherhood’ project in Nigeria, concluded that giving cell phones to pregnant women could increase their utilization of the primary healthcare system.
The HIFA Challenge Working Group’s role in the Goal is to encourage discussion around the Goal, to catalyze and advocate for action. It is not itself aiming to implement a practical initiative. The role of the Group is to provide the impetus and enabling environment for HIFA members and others to come together and form independent collaborations. The mHIFA Goal also hopes to contribute to the evidence base collected by the mHealth Alliance, a non-profit organization hosted by the United Nations Foundation, that champions the use of mobile technologies to improve health throughout the world.
Methodology
The first phase of the mHIFA initiative was
Over 1700 resources were scanned manually by one research assistant. As the scoping exercise continued, an annotated bibliography of relevant peer-reviewed articles and other professional reports was developed, identifying literature that specifically addressed barriers to mHealth implementation in developing countries, lessons learned from pilot studies, controlled trials investigating health information delivery formats or technologies. This bibliography will be used to help formulate the future directions of the mHIFA initiative.
In addition to the starting points listed in Appendix 1, other resources scanned included posts on the HIFA forums, non-governmental organizations’ website blogs and press releases, mHealth related conference presentations, technology innovator competitions, and YouTube project promotion videos.
The challenges of searching for very specific projects were many, and included: searchability and usability of the resources, accessing non-English language resources, currency of information and broken web links. Where resources were searchable, using the terms “mobile phone” and “health information” was found to retrieve the most relevant results.
Findings
There is a plethora of mHealth projects on a wide range of topics based in low- to middle-income countries. Topics included sexual, reproductive, and general health concerns such as family planning, maternal and newborn care (both routine and emergency situations), childhood immunizations, HIV/AIDS, tuberculosis, and basic nutrition. A large number of these projects focus on data collection, patient monitoring, health education or appointment reminders. Although such projects may be important, they do not appear to empower people with actionable lifesaving information. The scoping exercise confirmed the findings by a survey carried out by the World Health Organisation (WHO) (2011). that the dominant form of mHealth today is characterized by small-scale pilot projects that address single issues in information sharing and access. It also confirmed the statement by (Health Unbound, 2014) that many of the mHealth projects taking place are isolated from one another, and are unable to share information and best practices.
The majority of findings related to the Goal came from online repositories, in particular: Center for Health Market Innovation’s health program database, Washington, DC, USA: http://healthmarketinnovations.org/programs Global System for Mobile Communications Association mHealth Tracker, London, UK: http://www.mobileworldlive.com/mhealth-tracker Health Unbound (HUB) powered by the mHealth Alliance, Washington, DC, USA: http://healthunbound.org/resources/program mHealth Working Group Inventory of Projects coordinated by Kelly Keisling and FHI 360’s Laura Raney: http://www.mobileworldlive.com/mhealth-tracker Royal Tropical Institute’s mHealth Projects Database, The Netherlands: http://mhealthinfo.org/projects_table
Only nine projects, less than 1 percent of those scanned, were identified as being closely related to the Goal. This indicates a serious lack of mHealth projects that empower people with the information they need to deal effectively with acute healthcare situations. By contrast, there is a plethora of projects that push health education messages to citizens to change their behavior. These projects are undoubtedly important, but arguably do little to empower citizens with as-needed information for example when they need to give first aid, or take appropriate action with a sick child.
Two important findings the search revealed were: the trend towards SMS (text) based programs; and the majority of videos related to the Goal did not specifically target mobile phones.
The nine projects identified are listed below with a brief description:
Discussion
The findings of the scoping exercise were posted on the HIFA2015 Discussion Forum in order to raise awareness of the Goal and to engage HIFA members and key stakeholders involved with relevant mHealth projects. These discussions are ongoing and feedback will be incorporated into the next phase of the project. The Challenge Working Group suggested that a number of indicators about the applications identified in the nine projects needed to be determined. These are: Where is the application offered and available? e.g. country/state What local languages is it offered in? Suitable for which platform? (Basic phone, feature phone, smartphone) Is the knowledge provided in Text form? For what platforms/mobile phone (basic/feature/smart)? In what language(s)? Is the knowledge provided in the form of Images? For what platforms/mobile phone (basic/feature/smart)? Is the knowledge provided in the form of Videos? For what platform/mobile phone (basic/feature/smart)? In what language(s)? Is it an mHealth App? For what platform/mobile phone (basic/feature/smart)? In what language(s)? Does access to knowledge require connectivity? Does this connectivity cost the end user? Is the knowledge pre-loaded/embedded on mobile phones? Is it available on removable media – microSD memory card? Is the knowledge freely downloadable? From where? Are the audio and video downloads playable on low-end mobile phones? In what formats? Is the downloadable content free? If not, how much?
Building on the findings of the scoping exercise and the questions above, Dr. Geoff Royston, one of HIFA’s two expert advisors, suggested that telecom providers and potential providers of mHealth applications for supplying health and healthcare information in low resource settings, would benefit from having an assessment tool to help them indicate the relevance of their applications to the mHIFA Goal. Subsequently, an assessment template using a “traffic light system” was developed (Royston, 2014). The template can be used to indicate how well telecom providers and potential providers’ applications can meet users’ key needs. It will also assist providers and potential providers to assess and introduce successful new applications and to make desirable improvements to existing ones. For each component of each criterion listed in the template, attributes are described that broadly indicate increasing ‘fit’ of an application to the achievement of HIFA goals. An example of two of these criteria is shown in Table 1.
Example from the mHIFA assessment template.
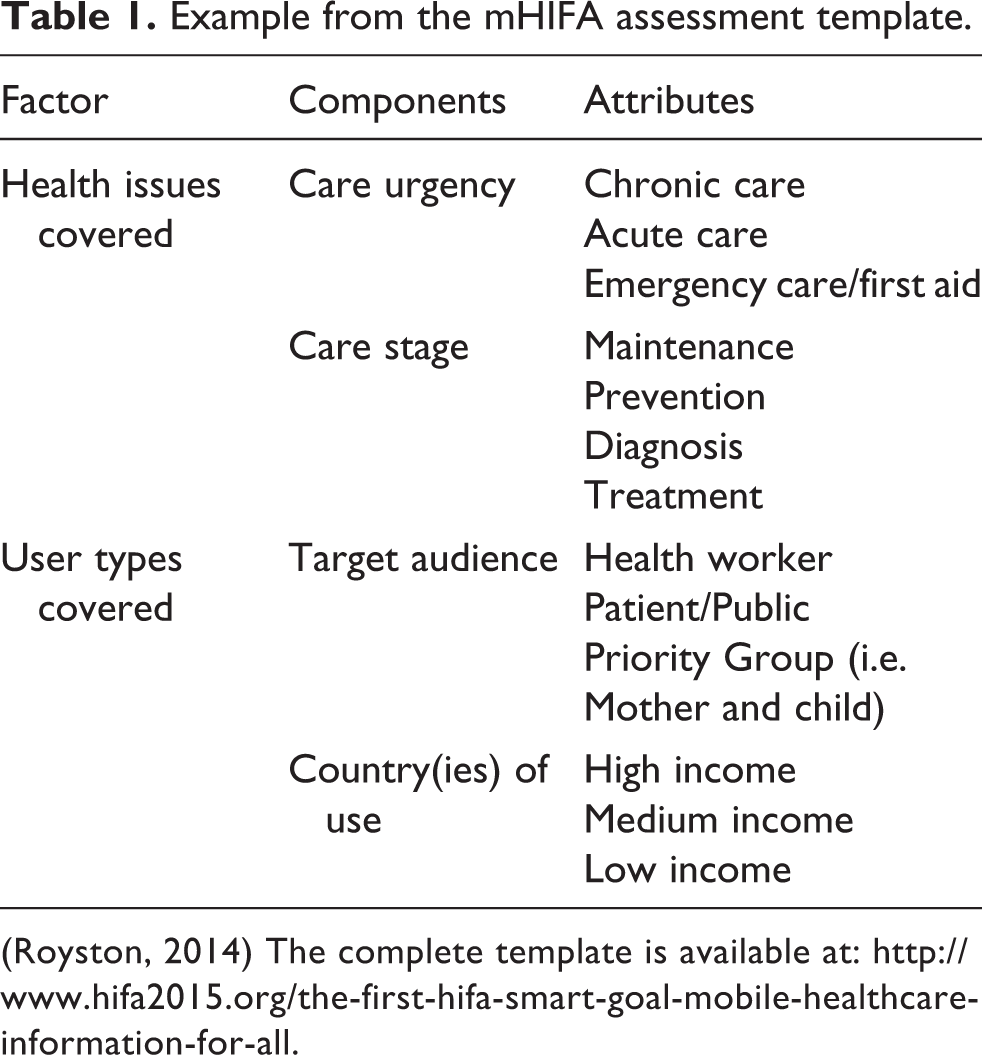
(Royston, 2014) The complete template is available at: http://www.hifa2015.org/the-first-hifa-smart-goal-mobile-healthcare-information-for-all.
Next phase
The next phase of the mHealth initiative will involve semi-structured interviews with key individuals from the nine projects identified. Interviews will also take place with telecom providers who show interest in the project and on their perceptions of the Goal, and the likely barriers and drivers to realize the goal by 2015. These providers include the mobile phone manufacturer who would provide pre-loaded healthcare information on new mobile phones and the mobile network operator / service provider who would provide free downloadable information.
The Challenge Working Group aims to assist one (or more) of the telecom implementing groups with planning and participation and to encourage feedback of lessons learned throughout. It will encourage the implementing group to develop the project in full consultation with the HIFA community, to draw upon other HIFA members’ experience, and to share lessons learned on HIFA forums and beyond. At the time of writing, HIFA is encouraged by the interest from one telecom provider. The Group invites feedback and suggestions on the work currently being done in relation to the mHIFA Goal. It encourages anyone interested in the project, health care professionals and telecom providers to contact HIFA2015 at hifa.org
Conclusion
There is a plethora of mHealth projects on a wide range of topics based in low- and middle-income countries, most of which are small and work independently. The few projects identified in the scoping exercise provided evidence that there is a gap in the provision of mobile applications that provide maternal, child health and first-aid information that empower people with the information they need to deal effectively with acute healthcare situations. The findings provided the impetus for the Challenge Working Group to pursue the Goal and to initiate discussions of the Goal within the HIFA2015 community. The creation of the assessment tool will help mHealth initiatives and mobile phone manufacturers and service providers and potential providers assess relevance to the Goal and will also help them to address users’ key healthcare information needs.
Footnotes
Appendix 1 Starting points for the scoping exercise
Acknowledgements