
Abstract
The purpose of this study was to investigate the management of health records in the Bulawayo and Matabeleland South provinces in Zimbabwe. The objectives of the study were to understand how health records were being managed in the two hospitals, to establish the availability of, and analyse standard procedures and guidelines that informed both the National Archives of Zimbabwe (NAZ) and hospitals in managing health records. The study also sought to establish the level of professional training for health records management staff in hospitals under study. A qualitative case study design was employed and data was gathered through questionnaires, interviews, observation and document analysis. Data was analysed thematically based on the objectives of the study. The study revealed that the strategies for the management of health records in hospitals were inadequate. There were no documented health records management standards to guide the management of these records in hospitals. It was also established that the majority of health records personnel in hospitals did not possess records management qualifications. As a recommendation, the hospitals and NAZ should draft and implement health records management standards to provide guidance on the management of health records. Hospitals should employ staff with the requisite records management qualifications and offer them continuous training.
Keywords
Background to the study
Health records are key to the protection of the health of humanity. Many studies in Africa demonstrate a general neglect of the management of these records and their related counterparts in the medical field (Chikuni and Mnjama 2010; Khumalo, Dube and Mnjama 2017; Katuu 2015; Marutha 2011; 2017; Marutha and Ngulube 2012; Masuku and Ngulube 2013). The area of health records management is an important field which has not been given much attention by researchers in Zimbabwe as shown by limited literature on the subject matter. A study by Chikuni and Mnjama (2010), based on the Gwanda Provincial Hospital in Matabeleland South Province indicated that the hospital did not have proper records management procedures, policies, file referencing and appraisal procedures for the health records, resulting in the accumulation of health records of ephemeral value and a chaotic system of managing such records. Such a situation results in lack of accessibility, poor quality information, poorly organised patient notes and misfiling in hospitals (Medical Protection Society of South Africa 2010:11).
The dearth of clearly defined and documented health records management policies, standard practices and procedures is characteristic of the hospitals in the two provinces. Whilst on attachment at Mater Dei Hospital from 2006 to 2007 and from a records management workshop that the first author facilitated at the United Bulawayo Hospitals in 2009 it was noted that hospitals did have medical/health records sections but were not equipped with records management facilities such as adequate storage areas or purposefully built records rooms.
The need for qualified medical records personnel in hospitals cannot be overemphasised. Educational advancement of medical records personnel enables them to improve records management practices in hospitals. This study also sought to understand the records management qualifications possessed by the health records personnel at the hospitals under study as well as the nature of continuous education and training offered by the hospitals to such personnel.
Zimbabwe has a National Archives, which is expected to work with health records administrators to improve health records management practices in hospitals. The National Archives of Zimbabwe (NAZ) in Bulawayo is the recipient and subsequent custodian of health records from all hospitals in the Bulawayo and Matabeleland South provinces. However, there was limited evidence of collaboration between NAZ and hospitals in areas of health records standards, policies and training. This study sought to investigate the management of health records in both public and private hospitals in the Bulawayo and Matabeleland South provinces and NAZ (Bulawayo), with the aim of understanding how hospitals in the afore-mentioned provinces managed health records throughout their life cycle.
Statement of the problem
Hospitals produce vast amounts of health records as they attend to patients on a day-to-day basis. Health records are invaluable as they protect human rights and facilitate research by medical practitioners and scholars. However, such crucial records have been managed without clearly outlined and documented standard procedures on creation, filing and disposal throughout their life cycle. Lack of suitably qualified records management personnel who can effectively manage health records throughout their life cycle appeared to have further complicated and exacerbated the predicament of health records in hospitals in the two provinces. As a result, volumes of valuable patient records in these hospitals were unsystematically destroyed, yet some of them were misplaced, incomplete and retained unnecessarily. Such a situation does not only jeopardise lives of innocent patients, but it also compromises the efficiency of hospitals in the two provinces. The predicament of health records in these two provinces also spilled into NAZ where it emerged, at an all-stakeholder meeting in 2011, that medical records were accumulating at an alarming rate resulting in the institution suspending deposits of such records from hospitals in Harare. Although NAZ in Bulawayo had not yet suspended deposits of health records, it was also being affected by the same problem.
In view of the statement of the problem, the objectives of the study were to: Understand how hospitals in the Bulawayo and Matabeleland South provinces and NAZ managed health records. Establish the availability of, and analyse standards and guidelines that guided both NAZ and hospitals in the management of health records. Establish the level of professional training and qualifications for health records management staff in hospitals in the two provinces. Find out the ways in which NAZ was assisting health records departments in hospitals to manage their records throughout their life cycle.
Following the procedure advised by Ngulube (2018), the research problem was conceptualised using concepts from the records life cycle theory.
Literature review
Health records are the backbone of a sustainable and effective healthcare delivery system and their sound management is a desideratum. By definition, a health record is “any relevant record made by a health practitioner at the time of or subsequent to a consultation and/or examination or the application of health management” (Health Professions Council of Zambia 2016:1) According to Luthuli and Kalusopa (2017), sound records management is at the core of service delivery and this comes with the need for proper records and information management in healthcare facilities. Properly managed records provide information that is accurate, valid, reliable, timely, relevant, legible and complete in support of a safe and reliable healthcare. Thus, it is imperative that medical records be managed properly in order to enable citizens to receive proper healthcare (Marutha and Ngoepe 2017).
As observed by the National Health Services Education for Scotland (2012), “without high quality records and efficient flow of information by health records staff, the quality of patient care would be severely compromised”. In the words of Attah (2017:1), the amount as well as quality of health information that healthcare professionals have at their disposal has a bearing on the both the outcome as well as continuity of patient care.
A patient record serves as a communication instrument in healthcare facilities in the sense that it communicates a whole range of patient information, including the patient’s medical history and treatment amongst physicians (Ngidi 2015:3). It is without proper clinical medical history of patients, their allergies, medication and other related health information about patients that medical mistakes could occur when making decisions (Alyami et al 2017:265). The Northamptonshire Healthcare Foundation (2016:6) summarises the key functions of health records as follows: Support patient care and continuity of care. Support evidence-based practice. Meet legal requirements and regulatory requirements including requests from individuals under subject access provisions of data protection and Freedom of Information Acts. Assist clinical and other types of audits. Support improvements in clinical effectiveness through research. Support archival functions by taking account of the historical importance of material and the needs of future research. Support patient choice and control over treatment and services designed around patients.
Health records do not only serve as reference materials for those rendering medical care but also offer administrative and legal support to healthcare organisations, their staff and patients. The Lincolnshire Community Health Services (2018: 4) buttresses this point by stating that other than anchoring direct healthcare to patients, clinical records also serve other wider purposes such as teaching, research, and clinical audits as well as the provision of evidence in the event of litigation. Buttressing the medico-legal value of medical records, Ngidi (2015:3) stated that a patient record functions as a legal document such that it can be used as evidence in courts of law.
The records life cycle concept
The life concept of the records life cycle is important in records management as it is a way of viewing how records are created and used (Northwest Territories Government 2012). According to Chachage and Ngulube (2006), records pass through various conceptual stages during their life. The basic conceptualisation of records according to the records life cycle concept is that records go through three stages, namely, active, semi-active and inactive stages. At the active stage, records are first created or received in both physical and electronic forms with the semi-active stage involving records being maintained, used, distributed to others and filed, whilst the final stage is the one where the records lose their immediate value such that the activity of the record drops, thereby necessitating their storage or transfer to less expensive storage offsite in order to fulfil the stipulated retention periods (University of Wisconsin Madison 2015). The records life cycle theory, according to Chachage and Ngulube (2006), is just a conceptual visualization and not necessarily a way of compartmentalizing the life of records into distinct stand-alone spaces and time.
Health records are different from any other records in the sense that it is difficult to determine their semi-active and in-active stages as long as patients are still alive. This is so in light of the fact that the patient’s illness is unpredictable, thereby making it difficult to ascertain the stage that a patient record is at at any given point in time. However, this does not mean that these records do not have a life cycle. To quote Quinsey (2007) “a health record’s life cycle is made up of stages with certain actions that occur at each stage.” Katz (2004:4) understood a record to be going through a number of stages, right from admission up to the point where the record has to be archived. Katz (2004:4) was appreciative of the fact that a medical record acquires different values as it moves from one point to the other. Concerning the stages that a health record passes through, there are five stages: creation, use, storage, retrieval and disposal (Claeys 1996:2).
Methodology
This study employed a case study design. Literature reveals the widespread application of case study methods in many disciplines (Zainal 2007; Verschuren 2003). The use of a case study design enabled the researchers to gain an in-depth understanding of how hospitals in the Bulawayo and Matabeleland South provinces managed their health records using a variety of data sources. This ensured that the issue was explored through a variety of lenses, thereby allowing for multiple facets of the phenomenon to be revealed and understood (Baxter and Jack 2008:244).
In that regard, this study employed questionnaires, consisting of open ended questions, as the major data gathering tool. Interviews, observations and document analysis were also used, although to a lesser extent. The questionnaires were personally administered by the researchers. Retention and disposal schedules for health records as well as the mission statement of NAZ were examined.
The study focused on two out of the ten provinces in Zimbabwe, thereby limiting the study to a reasonable size which enabled the application of the case study design This is because the researchers were interested in gaining a detailed understanding of the health records management issues both at the hospitals and NAZ such that the population of the study had to be kept reasonably small and manageable. This is commensurate with Zainal’s statement that case studies focus on small geographical areas or a very limited number of individuals (Zainal 2007:1).
The present study was concerned with gaining a detailed appreciation and understanding of how health records were being managed in the Bulawayo and Matabeleland South Provinces in respect of the stated objectives. The study focused on all public and private hospitals in the Bulawayo and Matabeleland South Provinces and NAZ. A list of the hospitals was obtained from the Provincial Medical Director’s office. A total of 16 hospitals were targeted. However, out of the 16 targeted hospitals, only 11 were accessible to the researchers due to a lack of response or refusal of the request. Of the 11 hospitals, 2 were private and 11 were public.
Purposively selected respondents that were “information rich” were involved in the study. The information rich cases were those informants in hospitals and NAZ who were involved in the management of health records, or in policy issues relating to health records management.
At the hospitals, the study sample included all the health records clerks, health records assistants and heads of the health information departments. These were targeted by the study as they were the ones handling health records in hospitals. These totalled 25 in all the 11 hospitals to which access was granted. Permission to gather data from the hospitals was requested from the Provincial Medical Director (Bulawayo) and the Chief Executive Officers who were in charge of some hospitals. Participants in the hospitals were identified with the help of the hospital administration which directed the researchers to the health records/information departments. It is important to note that each hospital had its own number of health records/information management personnel and there was no uniformity in terms of staffing levels among the hospitals.
From the side of NAZ, the Director of NAZ, the Chief Archivist (Bulawayo) and 4 records management officials at NAZ (Bulawayo) were included in the study. The Director, despite being stationed in Harare, was selected and became part of the study population as the study was interested in administrative and policy issues regarding how NAZ managed health records. This saw 6 respondents participating from NAZ. Thus, 5 questionnaires were distributed and received from NAZ (4 from the records personnel and 1 from the Director) with 1 interview conducted with the Chief Archivist. Permission to gather data at NAZ was sought from the Director of NAZ and the parent government ministry.
Questionnaires for data gathering
The study used pretested open ended questionnaires that allowed respondents to give qualitative responses. Three sets of questionnaires were administered by the researchers, with all the sub themes and subsequent questions based on the research objectives. These research instruments were pretested among seven staff members in the Faculty of Communication and Information Science and 16 4th year students in the Department of Records and Archives Management at the National University of Science and Technology in Zimbabwe. The same group was used to pretest the interview guides. The questionnaires and interview guides are available from the corresponding author on request.
The first questionnaire targeted 25 general records management staff at all the hospitals that were part of the study, of which 17 responded. Table 1 shows the number of the questionnaire responses per hospital-type. The second questionnaire targeted 4 records management staff at NAZ in Bulawayo of which all the 4 responded. This questionnaire had 30 questions which were divided into three sections covering general health records management issues, health records management standards, and use of health records by third parties (researchers, historians, scholars). The third questionnaire was issued to the Director of NAZ as it also addressed some administrative issues that required the input of the Director of NAZ. This is because NAZ was headed by the Chief Archivist who reported to the Director in Harare.
Questionnaire respondents by type of hospital.
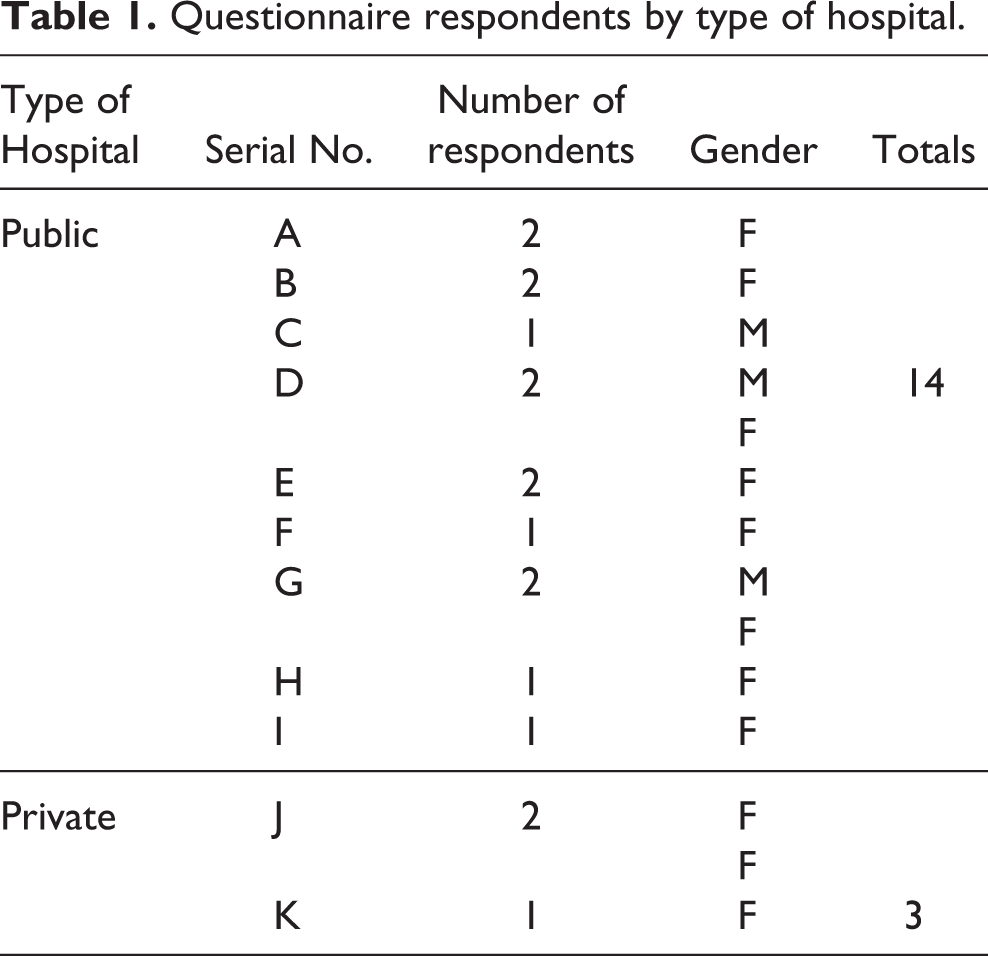
As shown in Table 1, of the 14 questionnaire respondents from public hospitals, 3 were male and 11 were female. All the three respondents from the private hospitals were female. All the five respondents from NAZ completed the questionnaires making the overall response rate (from the hospitals and NAZ) 73%.
Interviews
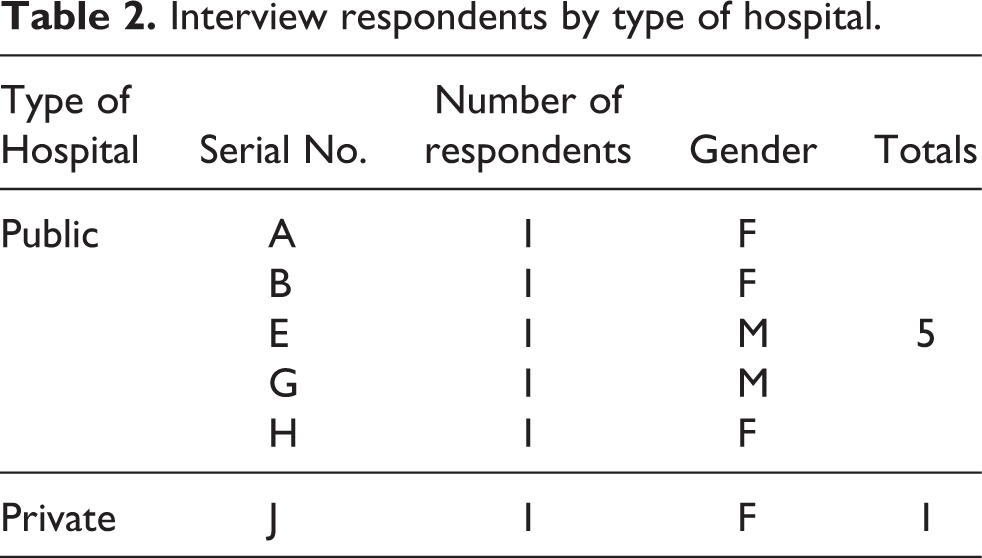
The heads of Health Information/Records Departments in hospitals were interviewed with the aim of complementing the questionnaires that were given to general records management personnel in the concerned hospitals. Of the 5 interview respondents from public hospitals, two were male and three were female, while one female was interviewed from the private hospitals. (see Table 2). The pretested interview guide for all the heads of the Health Information Departments in hospitals had 11 questions that sought to gather further understanding of the management of health records and how hospitals related to NAZ. The guides were based on all the objectives of the study so as to maintain relevance. The researchers stuck to the interview protocol to minimise bias. The researchers also avoided asking questions that were biased. The integrity of the data was also enhanced during the data presentation and analysis stage of the study where researchers also stuck to responses that were addressing questions that were in the interview protocol/guide and were answering research the study’s objectives.
Interview respondents by type of hospital.
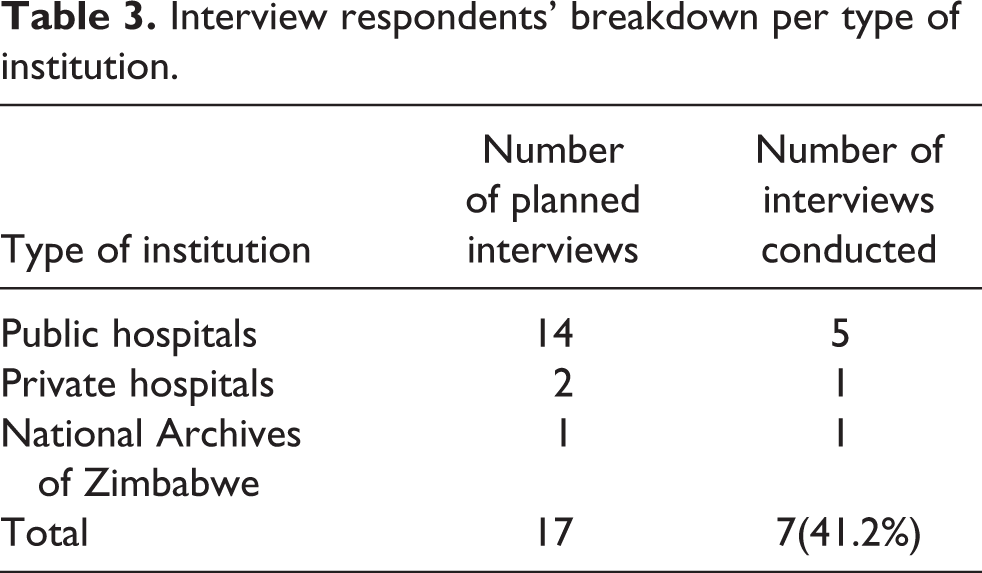
In addition to the six respondents from the hospitals, one interview was conducted with the Chief Archivist at NAZ in Bulawayo. The interview guide for the Chief Archivist at NAZ had 13 questions and also sought to gather a better understanding of health records management activities at NAZ as well as how NAZ related to hospitals regarding the management of health records. Regarding interviews, only seven of the planned 17 interviews were conducted giving a response rate of 41.2%. Table 3 outlines interview respondents per type of institution.
Interview respondents’ breakdown per type of institution.
Data analysis, presentation and discussion procedures
Questionnaire and interview data was presented, analysed and discussed in a thematic fashion, that is, the research objectives served as the major themes under which the sub-themes would emerge. Questionnaire and interview data was presented, analysed and discussed concurrently as per the order of the research objectives and the subsequent sub-themes. The approach allowed the researchers to exhaustively analyse and present the findings of each research objective.
How hospitals in the Bulawayo and Matabeleland South provinces and NAZ managed health records
The first objective of the study was to understand how hospitals in the two provinces and NAZ were managing health records. This objective gave rise to issues of records management such as the types, ownership and storage of health records generated by hospitals, strategic planning for health records management, policy and procedure manuals, and the management of active and semi-active records in hospitals, disaster management and the management of electronic records.
Types of records created, their ownership and storage
Data from the questionnaires and interviews with heads of health records management departments revealed that the types of records created in hospitals included patient case notes, X-rays and patient bills. Patient case notes were the predominant type. Data showed that all the 11 hospitals had internal storage facilities for their active and semi-active health records. These were being referred to as “Health Information Departments” in the 9 government hospitals. It was further revealed that the two private or mission hospitals did not have health information departments and records were stored in storerooms. It also emerged from the findings that in all the 11 hospitals that constituted the study’s population, patient health records remained the property of the hospital.
Inclusion of health records in hospitals’ strategic plans
Questionnaire respondents in hospitals were asked if records management was part of their hospitals’ strategic plans. There were mixed responses to this question, as questionnaire data revealed that 8 hospitals did not have records management as part of their hospital’s strategic plans, two indicated that their hospitals had records management as part of their hospital’s strategic plans, whilst respondents from one hospital expressed uncertainty about this matter. Data from all the six interviews that the researchers managed to conduct revealed that records management was not part of the hospitals’ strategic plans. This implies that the hospital did not treat records as a strategic resource.
Availability of the policy and procedures manuals
A policy and procedures manual is critical for effective records management. According to the University of Melbourne (2005), the purpose of a records policy and procedures manual is to identify the function and purpose of records and recordkeeping, including the roles and responsibilities of staff in maintaining access to such records. The manual further clarifies the rules of assessment for the frequency of the creation of records and the requirements for capturing and maintenance of such records over time and space (University of Melbourne 2005).
Since this study also aimed at finding out whether there were any health records management procedures and guidelines that indicated the duties and responsibilities of records personnel in hospitals, questionnaire respondents in hospitals were asked if their departments had policy and procedure manuals. Data revealed that the health information/records departments of all the 11 hospitals did not have records policy and procedure manuals. The absence of records management policies and procedure manuals in these hospitals was thus against best health records management practices.
As stated by the World Health Organisation [WHO] (2002), all procedures should be put in writing, describing, in detail, each of the stages of records policies and procedures, employees should be given a written copy and a copy of all procedures should be filed in a loose-leaf binder in the Medical Record Department, for reference and updating. Further buttressing the importance of records manuals and policies in organisations, the Information Governance Alliance (2016) opined that each organisation should have an overall policy statement spelling out how it manages all of its records, including electronic records.
Management of active and semi-active health records in hospitals
Data from the questionnaires and interviews with heads of health records management departments revealed that health records were managed by the records staff who were referred to as Health Information Assistants in all government hospitals, except for the one in which health records were managed by nurses. Active records were kept in internal storage facilities within hospitals until they reached the semi-active stages. Data from the all the respondents in hospitals revealed that semi-active records were kept within the hospitals’ records rooms before being deposited with NAZ. Interview and questionnaire data from respondents at NAZ revealed that health records in semi-active stages were deposited with NAZ, where they were kept in the Bulawayo Records Centre for an indefinite period of time without being processed into public archives due to their sensitivity and the patient privacy and confidentiality requirements.
Health records disposal in hospitals
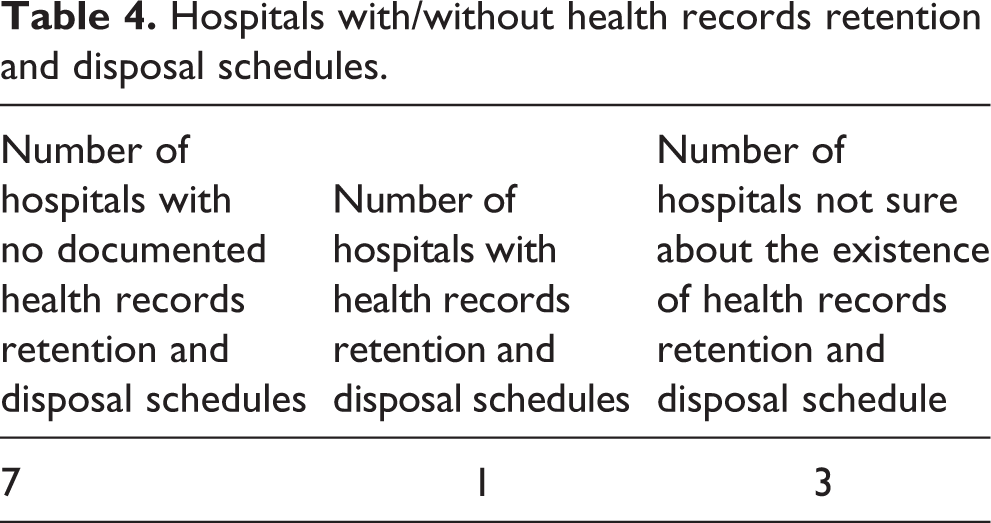
Respondents were asked about the disposal of health records. Data revealed three scenarios. Respondents from 7 hospitals indicated that they had never seen documented retention and disposal schedules for health records; 1 hospital had a schedule whilst respondents from 3 hospitals indicated uncertainty about the availability of such schedules. Table 4 shows the data pertaining to the availability of health records retention and disposal schedules in hospitals. The hospital whose respondents indicated that there was a disposal schedule was a public one. A study that was conducted by Marutha (2011) in some hospitals in South Africa revealed a situation that is almost similar to the findings of the present study. Marutha (2011) revealed that only three (2%) respondents said there were disposal authorities, whilst a staggering 137 (85%) respondents indicated that there were no disposal authorities for their electronic records, with 22 (13%) not answering the question.
Hospitals with/without health records retention and disposal schedules.
Interview data from 6 out of 11 hospitals in the present study indicated that such hospitals had once deposited their health records with NAZ. This meant that disposal schedules could have been in existence but were not distributed to new members of staff. For example, one interviewee in a government hospital revealed that all health records that were over 10 years old were deposited with NAZ, whilst one interviewee from one private hospital indicated that their hospital transferred all health records to NAZ after every seven years.
Interviews with Heads of the Health Information Departments in hospitals revealed that there had been extremely high staff turnover in hospitals during the past decade. The Chief Archivist, during an interview, also explained that there was high staff turnover at hospitals and each time NAZ staff from Bulawayo Records Centre conducted records surveys at hospitals, they would find new staff in the Health Information Management Departments. This, the Chief Archivist lamented, impacted negatively on records management in hospitals as there was no proper handover between the predecessors and those who assumed duties of records management. That resulted in improper knowledge of the existence and whereabouts of important records management tools such as disposal schedules.
Some inconsistencies were noted where respondents from the same hospital would give different responses, with some respondents indicating that their hospitals had disposal schedules, whilst others indicated that their hospitals did not have schedules, owing to a lack of adequate knowledge about the existence of records management procedures and policies amongst records staff in some hospitals. It also emerged that in those hospitals where disposal schedules were said to be available, these were not documented. Overall, it emerged from the data that all the hospitals under study deposited their health records with NAZ.
Retention and disposal of health records at NAZ
Staff at NAZ confirmed that they received semi-active records from all hospitals in the two provinces for safe keeping and permanent preservation. However, it emerged from the data that the permanent preservation of health/medical records at NAZ was done in the records section, as health records were not taken to the Public Archives section due to their sensitive nature. Medical records were kept for an indefinite period of time at NAZ records section.
The researchers further asked participants at NAZ about the existence of retention and disposal schedules for health records that were deposited with them. All the 4 participants at NAZ indicated that NAZ had retention and disposal schedules for health records, which were, however, inadequate for the management of health records. It emerged from the interview with the Chief Archivist that no maximum number of years was prescribed for the retention of medical records, hence they were retained indefinitely. The interview with the Chief Archivist at NAZ indicated that there were retention and disposal schedules for health records, including medical records (patient case notes) whose standing instruction was “Preserve”. It further emerged from the participants at NAZ that the current standing instruction of “Preserve” for all medical records resulted in the shortage of storage space as well as increased storage costs on the part of NAZ. The shortage of storage and filing space for medical records was not only predominant at NAZ but some hospitals were also experiencing the same problem.
The researchers also conducted a document analysis of the retention and disposal schedules for health records at NAZ. The major problems observed included the following: The schedules were out-dated and were no longer adequate for the large volumes of medical records that were being generated by hospitals, for example schedules dated back to as early as 1972. All health records cannot be kept indefinitely because the health sector has expanded since independence in 1980 and the population has increased; and The schedules were torn to the extent that it was difficult to read them.
A study conducted by Tavakoli, Saghaiannejad and Habibi (2012) in Iran, concluded that the lack of a complete, transparent and up-to-date medical records retention schedules led to confusion in hospitals as some hospitals would retain health records for more than the period required whilst others destroyed medical records prematurely (Tavakoli, Saghaiannejad and Habibi 2012).
The “preserve” status of medical records at NAZ was not best practice when compared to other countries, including the United States of America, New Zealand, and Britain, which have clear retention and disposal schedules for all types and classes of medical records (Tough and Lihoma 2017).
Existence and management of electronic health records in hospitals
The researchers also sought to find out how computers were being used in the management of health records in hospitals. It emerged that 4 out of 11 hospitals used computers in their health records/information departments. Of these, one was a private hospital whilst the other three were public. The remaining 7 hospitals were not yet using computers in the management of health records (Figure 1). Hospitals that were using computers in their health records management activities indicated that they were used to capture and store patient information in the form of databases. Computers were also used to produce statistics which were forwarded to the Provincial Medical Director or for basic functions such as typing and printing. The adoption of electronic health records systems was still very low in the hospitals under study. Some hospitals in countries such as South Africa, Kenya and Zambia have made significant strides in the use of ICTs to manage health records. For example, in Kenya, the Ministry of Medical Services and the Ministry of Public Health and Sanitation (2010) were already reporting on the existence of Electronic Medical Records (EMR) systems whilst the Department of Health, Republic of South Africa (2008) was already reporting on Electronic Health Records (EHR).
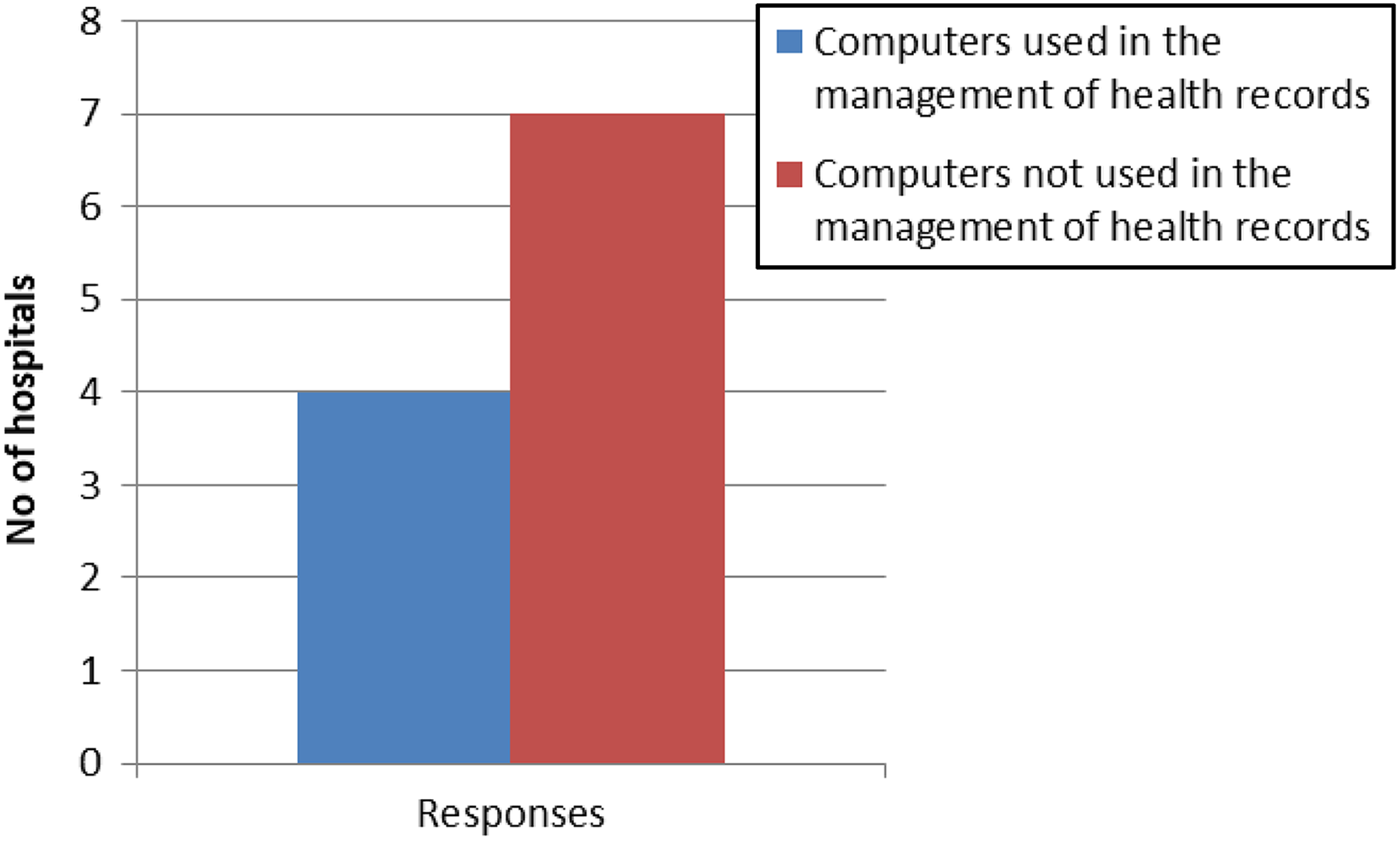
Use of computers in managing health records.
When asked about measures being employed to ensure the security of patients’ health information, all the respondents at the hospitals where computers were being used mentioned passwords as the only security measure in use. Data from the respondents at NAZ revealed that no electronic records were being deposited with NAZ by hospitals. All the informants at NAZ indicated that only paper health records were being accepted by NAZ. This was also confirmed by the Director of NAZ.
Disaster preparedness, response and recovery plans for health records
None of the 11 hospitals whose respondents supplied data had plans to deal with disasters. The findings of the present study matched those of Marutha (2011), in which he discovered that all the 40 hospitals he studied did not have disaster preparedness plans for their health records. Thus, whilst Wolter, Dolan and Dooling (2012) assumed that Health Information Management professionals understood the need for disaster preparedness plans, the situation on the ground showed that health records management staff in hospitals in the two provinces had not taken heed of this.
The respondent from one hospital indicated that their hospital had once been affected by disaster within the past 13 years, while 11 respondents, representing eight hospitals, were not sure whether their health records had been affected by disasters or not. Five respondents, representing two hospitals, indicated that their hospitals had never been affected by disasters that affected their health records. Wolter, Dolan and Dooling (2012), reported the case of Hurricane Katrina in the United States of America, where more than one million medical records were destroyed, and the case of the California State wild fires of 2008, together with the outbreak of the H1N1 virus, where health practitioners had to rely on patients’ memory to recall medical plans. The American Health Information Management Association (2010) stated that unexpected loss of patient records may be devastating, not only to the healthcare organisation but to patients as well.
It was also of interest to the researchers to find out if the storage areas for heath records were purposefully built rooms. Data from all the 11 hospitals indicated that buildings in which health records were kept were not purposefully built records rooms. They were either offices or delivery rooms or structures that were previously used for purposes other than records storage. Such storage areas were characterised by lack of necessary disaster response equipment such as fire extinguishers and smoke detectors.
Availability of standards and guidelines that guided NAZ and hospitals in the management of health records
All the respondents admitted that health records management standards were important, and gave acceptable reasons that demonstrated an understanding of the role that standards play in health records management. Responses such as the following were given: “the standards should be maintained so that the right procedures are always followed since the patients’ records contain confidential information…”; “to maintain the integrity of records and to ensure their long term preservation if they have enduring value…”; “because of uniformity it allows or equips professionals to work in any records department anywhere.”
However, data revealed that 8 out of 11 hospitals did not have documented health records management standards whilst only three hospitals had health records management standards. These were all public hospitals (Figure 2).
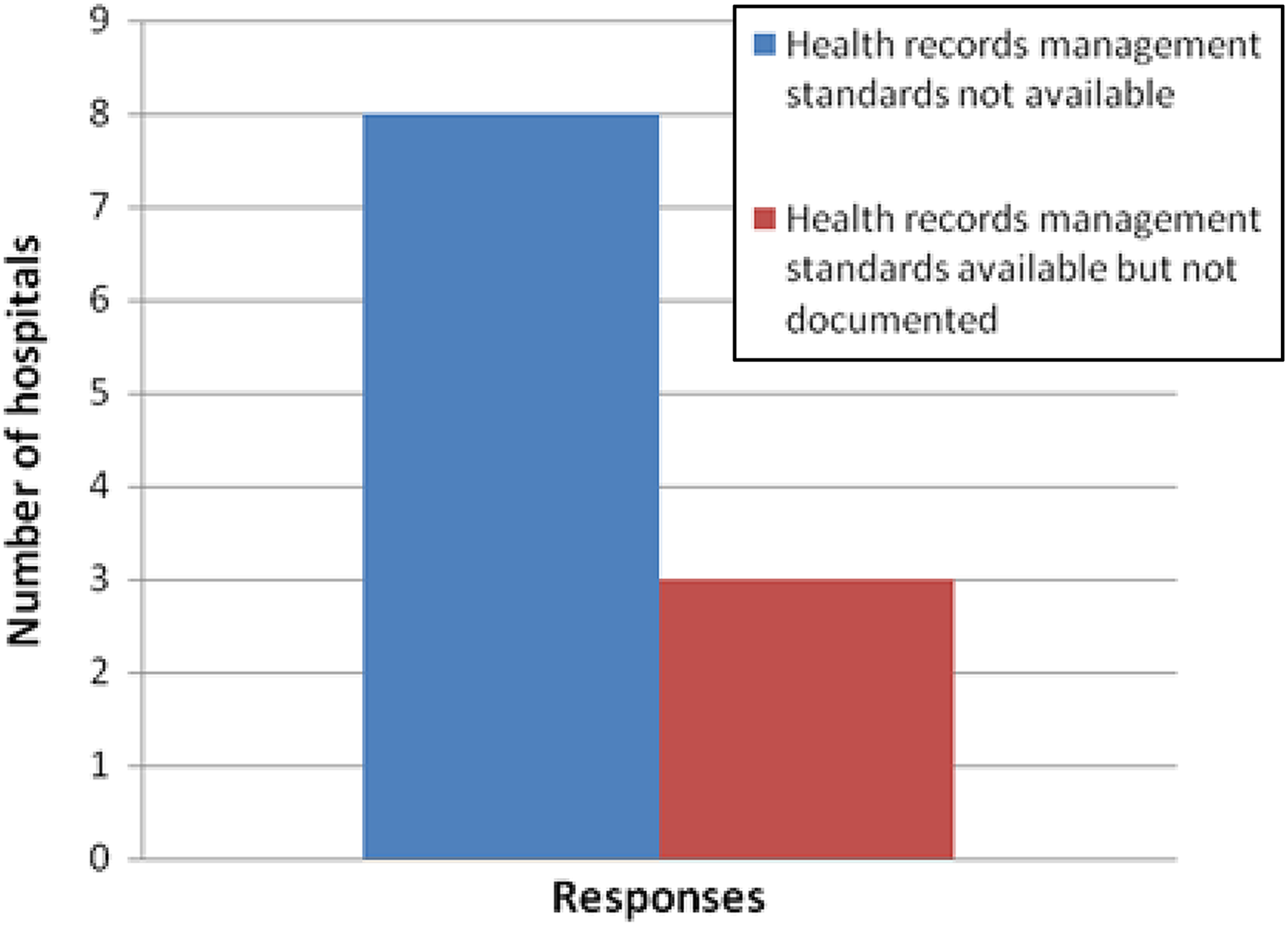
Availability of health records standards in hospitals.
Respondents who said there were no documented standards revealed health records management staff ensured that patient records were complete all the time. This was the only standard practice that was prevalent in the hospitals.
Two of the participants at NAZ said there were standards on health records management, whilst the other two indicated that there were no such standards at NAZ. An interview with the Chief Archivist confirmed that health records management standards were existent, but in bits and pieces, for example in the form of memos and circulars.
The Director of NAZ indicated that efforts were under way to draft and implement records management standards. When asked whether NAZ had the capacity to develop, implement and monitor health records management standards in hospitals, respondents at NAZ (Bulawayo) expressed mixed feelings, as three of them indicated that indeed NAZ had the potential and capacity to do this, one of the respondents felt that NAZ did not have the capacity to develop health records management standards.
When asked to explain this response, the respondent cited inadequate funding of the institution as the main constraint. The Director indicated that although NAZ had never drafted records management standards before, the institution had the obligation to oversee standards on records management. He stated, “to the extent this applies to government health records, NAZ has the statutory obligation to supervise the management of such records.”
The Chief Archivist also revealed that plans by NAZ were under way to develop records management standards, including those for health records management.
The dearth of health records standards in the hospitals studied in the present study were similar to those that were revealed by a similar study in Nigeria by Ivwighreghweta and Onoriode (n.d). It revealed that 76% of the respondents strongly agreed, and 20% of the respondents agreed that a lack of standards and policy was one of the problems of managing medical records in public hospitals in that country. A study by Marutha (2011) also unearthed a similar problem in which, when asked about the availability of policies, procedures, norms and standards, respondents in all the 40 hospitals that constituted the population of his study indicated that these were not existent at their work places. The revelation by the present study that eight out of eleven hospitals did not have health records management standards is thus a cause for concern as other hospitals around the world do have such standards (Marutha and Ngoepe 2017).
Level of professional training and qualifications for health records management staff in hospitals in the two provinces
In appreciation of the invaluable role played by professional and academic training of records management personnel in sound records management, respondents were asked through if they considered health records management required professionally qualified personnel to manage them. All the 17 respondents agreed that records management was important and required the services of professionally qualified personnel.
When asked to explain their responses, respondents indicated their understanding and appreciation of the importance of having records managed by professionally qualified staff. Some of the responses that the informants gave when asked to explain why health records needed to be managed by professionally qualified personnel included the following: “so that they can be able to deal with records from their creation phase up to their disposal…”; “so that required standards are met…”; to maintain the integrity of records and to ensure their long term preservation if they have enduring value…”; “there are many medical terminologies that need to be known and explained.”
Data pertaining to the professional qualifications of the records management personnel was also elicited through questionnaires. It emerged that the majority of the records management personnel did not have qualifications in records management. Other than the four respondents who possessed National Diplomas in Records and Information Science Management and two more who possessed Health Information Management Certificates, the majority did not possess qualifications in records management. One possessed a National Diploma in Information Technology, four possessed Diplomas in Nursing, one possessed an Advanced Level Certificate, one possessed an Ordinary Level Certificate and four did not indicate their highest qualifications (Figure 3).
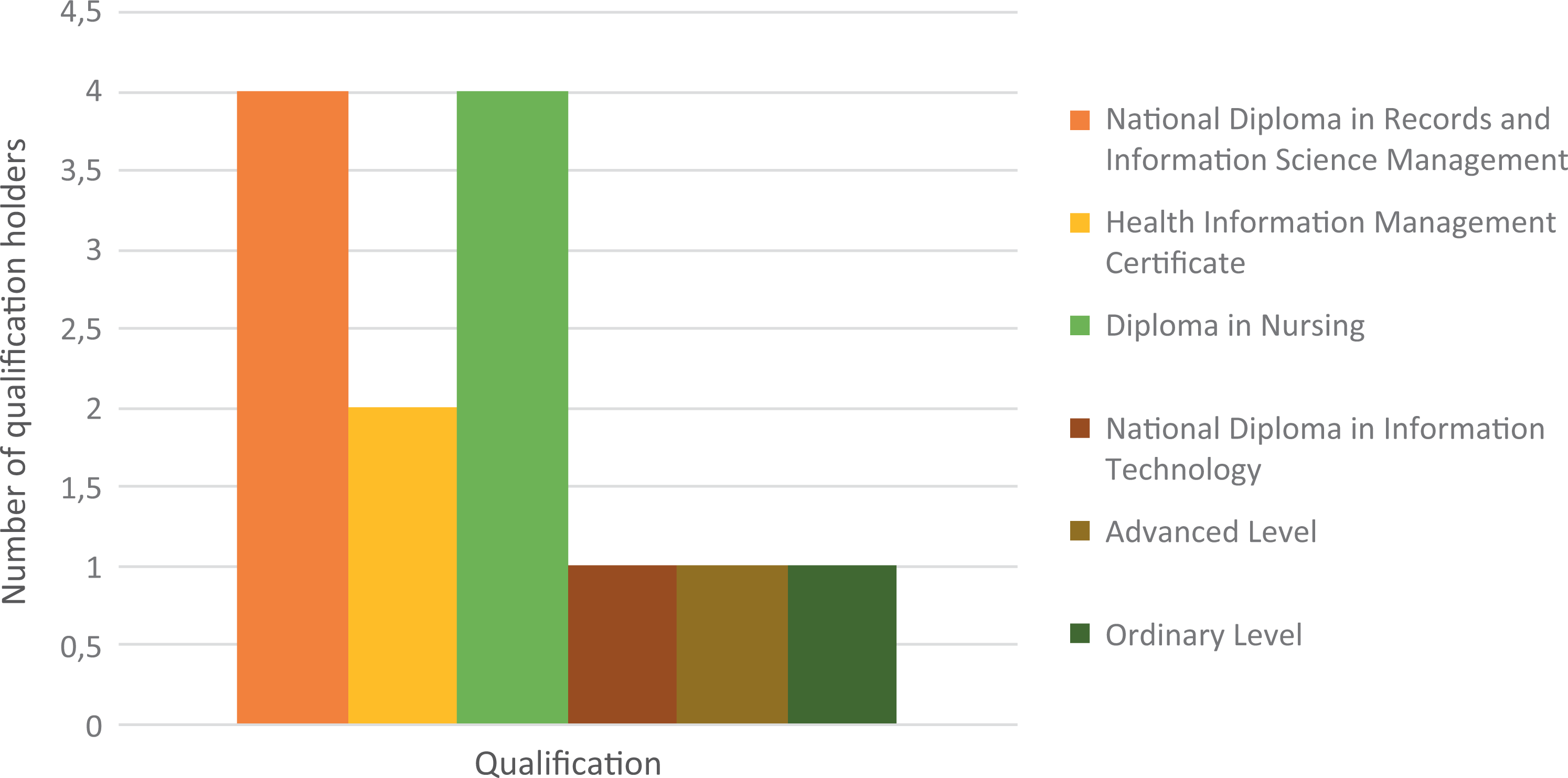
Qualifications held by health records management staff in hospitals.
It was noted that all the 6 respondents who possessed qualifications in records management were from public hospitals. It was impossible to follow up on those respondents who did not indicate their highest qualifications due to the anonymity of the respondents. All three respondents from private hospitals did not indicate their qualifications.
A further analysis revealed that the highest qualification among all the health records personnel in hospitals was a National Diploma whilst the lowest qualification was the Ordinary Level Certificate.
The findings of the present study where the majority of the health records personnel did not possess records management qualifications reveal an anomaly in health records management units of the concerned hospitals.
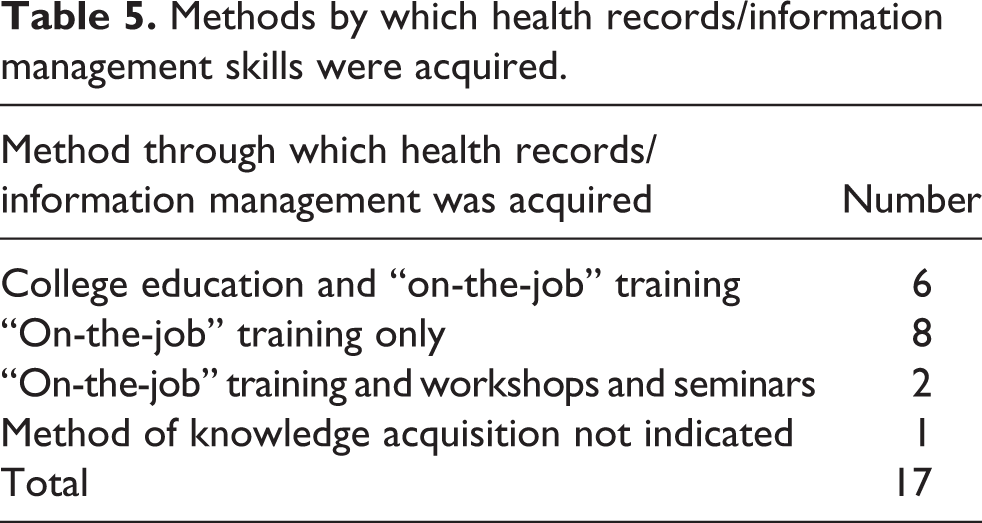
Respondents were further asked how they acquired knowledge of health records management. Data revealed that, of the 17 respondents, 16 indicated that they had acquired knowledge of health records management through “on-the-job” training whilet one did not indicate how they acquired knowledge on health records management. Workshops and seminars were another avenue of gaining the knowledge, as illustrated in Table 5.
Methods by which health records/information management skills were acquired.
None of the three respondents from private hospitals have records management qualifications from a college. Some health records management staff were just seconded to the health records section with no specific professional qualification being made a prerequisite. Results of the interviews with the heads of the health records management units revealed that in government hospitals, a Certificate in Health Information Management which was offered by the Harare Polytechnic was a prerequisite in order to be recruited as a Health Information Assistant.
When asked if the knowledge and skills that they possessed on health records/information management was adequate and enabled them to execute their duties adequately, 13 respondents indicated that they felt that their knowledge was limited and further training in health records management was necessary, with three respondents indicating that their knowledge of health records management was adequate and one respondent did not respond to this question. The three respondents who expressed contentment with their knowledge about health records management indicated that they had acquired their knowledge through both college education and “on-the-job” training. These respondents were from the same government hospital.
Respondents were further asked about the availability and frequency of training activities and workshops on health records management. Responses indicated that there were no training programmes for health information/records management staff in hospitals. Interview data from all 6 interviews conducted with the heads of health information offices or records offices revealed that there were no regular training programmes in place for their health records staff. The situation resembled that in South African healthcare facilities, where a study by Marutha and Ngoepe (2017) revealed that 88% of health records respondents indicated that they had never received formal education in records management and had acquired records management skills through in-house training.
The challenge of untrained or inadequately trained health records personnel characterised some hospitals and healthcare facilities in Blantyre, Chikwawa and Zomba in Malawi. A study by Tough and Lihoma (2017) revealed inadequate and inappropriate training of data clerks and other recordkeeping specialists, resulted in the occurrence of data errors. The findings of the present study, in which records in some hospitals were managed by former security guards who had not received any formal training and education in records management, were similar to those of Tough and Lihoma (2017), where it was learnt that in times of acute need, ward maids, cleaners, security personnel and volunteers from village health committees assisted healthcare facilities and hospitals with records management.
There are a number of reasons for providing education and training in information handling, including maintenance and improvement of services, respect to patients, as well as the unavoidable need to comply with legislation with regard to data collection, storage and use (Bennett 2015:9). According to Illich (1988:21), “a medical records staff that has been trained will be in an excellent position to take the lead, not only in education but also in other ways”, an educated medical records staff may have significant impact on the accuracy of medical records, the development of automation, the education of the hospital staff, and the financial viability of the hospital (Illich 1988:24).
Ways in which NAZ assisted health records departments in hospitals to manage their records throughout their life cycle
The researchers further sought data regarding the way in which hospitals related to NAZ and worked together in the management of health records. Data revealed that there was a strong relationship between NAZ and the hospitals, both public and private. This relationship was clear as medical records from hospitals were deposited at NAZ upon reaching their semi-active stages, where NAZ kept them for an indefinite period of time. When asked whether NAZ rendered any kind of service to hospitals regarding health records management, respondents from all the 11 hospitals indicated that NAZ provided professional records management advice to them. However, respondents indicated that the service was not offered at regular intervals.
Data from NAZ respondents further confirmed that professional records management advice was rendered to the hospitals by NAZ, in the form of records surveys and workshops. All respondents at NAZ (Bulawayo) indicated that this service was provided once every four years to each registry. This was also corroborated by the Director of NAZ. When further asked whether NAZ was consistent in the provision of such services, two respondents revealed that NAZ was inconsistent, whilst the other two indicated that NAZ was consistent. When further asked about the reasons behind NAZ’s inability to be consistent in the provision of this service, three respondents did not indicate the reason for this, whilst one respondent mentioned financial constraints and high staff turnover as the reasons.
In an interview with the Chief Archivist, it emerged that NAZ had experienced a critical shortage of staff and financial resources and this affected its ability to render satisfactory services to records creating agencies, including hospitals. The last time NAZ provided such services to hospitals had been in July of 2011. The Chief Archivist revealed that the provision of archival storage boxes to hospitals was another service that used to be provided by NAZ but it had since stopped providing such a service due to financial constraints.
The existence of professional relationships between NAZ and the hospitals regarding the management of health records management was in tandem with international practices where national archival institutions are at the centre stage and are expected to take the lead in cultivating good records management practices in government and even private institutions. For example, Archives New Zealand (2009) provides professional records management advice to the records management facilities in that country. Thus, NAZ, in this regard was at par with recommendations from the literature.
Records surveys in hospitals by NAZ (Bulawayo)
Questionnaire respondents at NAZ indicated that their institution conducted records surveys in hospitals. This was also confirmed by the Chief Archivist and the Director of NAZ. NAZ’s mission statement stated that it was the duty of NAZ to “carry out a records survey at every registry at least once during every four years” and this included hospitals. The Chief Archivist revealed during the interview that NAZ had conducted records surveys at the Gwanda Provincial Hospital, Beitbridge Hospital, Plumtree Hospital, United Bulawayo Hospitals, Mpilo Hospital and Ingutsheni Hospital within the past two years (note that this study was conducted in 2012). These hospitals were part of the population of this study.
It emerged during the interview that the records surveys conducted by NAZ were negatively affected by high staff turnover during the economic hardship that faced Zimbabwe from 2000 to 2009, coupled with limited funding for such projects. NAZ could no longer afford to conduct surveys at a four-year interval at the registries and funds were still a serious constraint to the institution. The Director of NAZ also cited the challenge of limited resources, coupled with problems of accessing institutions during surveys.
The financial constraints that were bedevilling NAZ were not peculiar to Zimbabwe but affected the national archives of other countries as well. Kaima (2000) reported on the negative impact of lack of financial and human resources that bedevil the National Archives and Records Services of Papua New Guinea. Although NAZ experienced challenges regarding meeting its obligations to extend records management services to the hospitals, its commitment to undertake records surveys and inspections was seen as in being line with the records management literature and international practices, which propose that national archival institutions take a lead in records management, especially public sector records. For example, the United States National Archives and Records Administration (NARA) (n.d) stipulated that was the duty of the archival institution to conduct inspections and surveys. In New Zealand, Archives New Zealand (2009) stated that “Archives New Zealand provides services and tools to support public offices and local authorities to create and effectively manage the records of their business activities”.
When asked about the findings of such surveys in the Bulawayo and Matabeleland South provinces, the Chief Archivist expressed unhappiness with the state of health records management in the hospitals: To put it in the words of the Chief Archivist “the state of health records in hospitals is shocking”; “the disorder in records is pathetic.” The Chief Archivist further explained that records surveys by NAZ in hospitals revealed that hospitals were incapacitated when it came to health records management. He explained that surveys conducted by NAZ revealed the following: In one of the hospitals visited, the records department did not have offices; The general value of records management had gone down gradually, resulting in poor health records management practices; and, The storage areas that were initially set aside for the storage of health records had been converted into offices for other departments.
The Chief Archivist further revealed that large volumes of records were trapped in an inaccessible underground storage in one of the hospitals in Bulawayo. The records surveys showed that most of the storage areas in hospitals were dirty and congested, with records piled on top of each other. The researchers observed that patient health records were stored in rooms that had inadequate shelving and storage facilities. This resulted in the records being stashed on top of each other, in some cases on the floor.
It further emerged in the interview that NAZ always offered advice regarding ways of better managing records in hospitals each time it made visits to registries. However, such efforts by NAZ were held back by: Weak archival legislation whereby NAZ had no power to compel the visited registries to implement its recommendations. This, according to the Chief Archivist, resulted in the visited registries, including hospitals, continuing with poor records management practices which also continued to deteriorate with time. High staff turnover in hospitals. This, the Chief Archivist further explained, resulted in the failure by registries, including hospitals, to implement the recommendations that NAZ had made regarding records management.
Implications of the research findings in the light of the records life cycle concept
The purpose of the study was to investigate the management of health records in the Bulawayo and Matabeleland South Provinces and NAZ, with the aim of understanding how hospitals in these provinces managed their health records throughout their life cycle. This was in the light of the problem of seemingly inefficient records management systems at the hospitals under study as well as the ever fast accumulating health records at NAZ, thereby presenting space and retention and disposal challenges. The records life cycle concept was used in the study to determine if health records were being managed according to this concept.
It can be concluded that the records life cycle was still being used to manage health records in hospitals in the two provinces. The study revealed that active records were being kept in internal storage areas in hospitals. Semi-active records from all hospitals were being deposited with NAZ’s records centre where they were being kept indefinitely as such records were not being put in the public archives section. Thus, it can be noted that health records in Zimbabwe were still being managed according to the records life cycle concept largely because hospitals were still dominated by traditional paper records as witnessed by very few EHR and EMR systems. However, efforts towards the development and implementation of electronic records management systems were noted in some hospitals.
Although the study revealed adherence to the life cycle concept by hospitals and NAZ in the management of health records in the Bulawayo and Matabeleland provinces, it was noted that the life cycle concept was only applicable up to the semi-active stage, with the inactive stage where records should ideally be found in the public archives section not applicable to health records. Thus, health records were not processed into public archives, owing to their sensitivity as they were not anonymised and they were, therefore, retained indefinitely at their semi-active stages at NAZ.
The indefinite retention of health records at NAZ, coupled with the out-dated retention and disposal schedules that had been overtaken by time and events, were seemingly responsible, not only for the partial application of the records life cycle concept in the management of this class of records, but for the shortage of storage space at NAZ and hospitals. In light of such findings, it was recommended that the outdated retention and disposal schedules for health records be revisited to enable health records to be appraised such that those that carry archival values can be transferred to the archives section for the benefit of researchers. However, such transfer of health records should be done on condition that there are tight anonymisation measures to respect and protect the privacy of the subjects of care.
Conclusions and recommendations
From the findings of the study, it can be concluded that health records in hospitals in the Bulawayo and Matabeleland South Provinces were not properly managed. Most hospitals did not have clear health records management procedures, disposal schedules and health records management standards. The study also concluded that the majority of the health records personnel at the hospitals in the two provinces did not have records management qualifications and needed further training in health records management. It can also be concluded that hospitals in the two provinces had a healthy relationship with NAZ in relation to records surveys and records management surveys in the hospitals, but there was a challenge regarding the implementation of the recommendations made by NAZ concerning records management by hospitals after the record surveys.
In light of the study findings, the following recommendations are made: Comprehensive records management programmes must be implemented in hospitals. The Government of Zimbabwe should ensure that all hospitals in the two provinces have proper records management programmes to support the healthcare system in the country. Hospitals should include health records management in their strategic plans. Health Information/Records Departments in hospitals should draft records policy and procedure manuals for use in their departments. Health records departments should liaise with NAZ and get copies of retention disposal schedules for health records. NAZ should revisit standing instructions on the retention of hospital records as it was now causing space challenges for NAZ. Thus NAZ should review the “Preserve” status of medical case notes and come up with a maximum number of years for which such medical case notes can be maintained before being destroyed. Hospitals should design disaster preparedness and recovery plans for their health records so as to ensure that health records can be salvaged in cases of disasters. Hospitals should draft and apply health records management standards to improve health records management. Hospitals should work closely with NAZ to develop and implement health records management standards. Health records management standards can also be obtained from the Standards Association of Zimbabwe which adopts them from ISO. Hospitals should invest in education and training for their health records management staff. Hospitals in the two provinces should ensure that they recruit records management staff with the requisite qualifications to work in the health information management sections of hospitals. Hospitals should provide continuous training programmes through workshops and exchange programmes for their health records management personnel. Hospitals should implement the recommendations of the NAZ surveys regarding the management of health records. NAZ and hospitals should tighten their communication strategies regarding the retention and disposal schedules for health records.