
Abstract
The ideal cardioplegic strategy in thoracic aorta operations requiring long cardiopulmonary bypass and cross-clamp time has not been established. Suboptimal myocardial protection may lead to myocardial damage and possible post-operative complications. We evaluate post-operative cardiac Troponin I (cTnI) release, low cardiac output syndrome (LCOS) and mortality, using a cold crystalloid single-dose intracellular or cold blood multidose cardioplegia in 112 elective or emergent thoracic aorta operation patients. Fifty-four patients (HTK group) received Custodiol® cardioplegic solution and 58 received cold blood cardioplegia (CB group). Cross-clamp time, cardiopulmonary bypass (CPB) time and cTnI peak release were similar in both groups. No differences were found for atrial and ventricular arrhythmias, inotropic support, LCOS and in-hospital mortality. Two-way ANOVA analysis revealed an interactive effect on cTnI peak (p=0.012) of cardioplegic solution type across the cross-clamp time quintile. In the fifth quintile, cross-clamp time patient (>160 min) cTnI peak value was higher in CB patients (p=0.044). HTK and CB cardioplegic solutions assure similar myocardial protection in patients undergoing thoracic aorta operations. In long cross-clamp times, the lower post-operative cTnI release detected using HTK may be indicative of a better myocardial protection in these extreme conditions.
Introduction
The optimal strategy for myocardial protection during ischemic diastolic cardiac arrest is still debated, especially in complex aortic surgery requiring a long cross-clamp time. The combination of hypothermia and the potassium-induced electromechanical cardiac arrest represented the basis of cold crystalloid cardioplegia strategy1,2. Subsequently, blood was frequently used as a vehicle for potassium delivery 3 and myocardial protection with continuous or intermittent warm blood cardioplegia provided satisfactory results in coronary artery bypass grafting4-6. In thoracic aorta operations, a single-dose strategy providing 2–3 hours of myocardial preservation may be attractive and helpful, especially in acute aortic dissection, while normothermic cardioplegia is not applicable in aortic procedures, since deep hypothermic circulatory arrest or mild-to-moderate hypothermia is often required. The Bretschneider-HTK solution is nowadays widely used for multi-organ preservation in transplantation, but it is also used as a valid cardioplegic solution that allows single-dose administration in valve operations or coronary artery bypass grafting7-9. The efficacy of this crystalloid cardioplegia in thoracic aorta operation has never been assessed.
Suboptimal cardioplegic protection leads to myocardial damage, causing myocardial necrosis or stunning. Cardiac Troponin I and T (cTnI and cTnT), myocardial cell proteins, in association with echocardiography, are used to detect myocardial damage, to diagnose acute coronary syndrome (ACS) and to predict mortality risk in ischemic heart disease10,11. After cardiac operations, cTnI values are related to the amount of peri-operatively damaged myocardium and higher levels of cTnI are associated to short- and mid-term mortality and morbidity after CABG or cardiac surgery12,13.
Several studies, based on experimental models and biochemical and clinical evaluations, assessed the efficacy in myocardial protection of different cardioplegic solutions, but, at the moment, no study has compared histidine tryptophan ketoglutarate (HTK) and cold blood cardioplegia in thoracic aorta operations8,9,14,15.
Methods
The design of the study was single-centre, retrospective. The approval of the local ethics committee was obtained before the study protocol was conducted. According to local ethics committee policy, individual consent was waived. We performed a retrospective analysis of prospectively collected data.
From January 2003 to March 2008, 112 patients underwent thoracic aorta surgery at our institution; among these, 45 patients underwent emergency surgery for Stanford type A acute aortic dissection and 67 patients underwent elective surgery for thoracic aorta aneurysm.
Patients were divided in two groups on the basis of the cardioplegic solutions used: the Custodiol (Custodiol® HTK Bretschneider, dr. Franz Kohler Chemie GMBH, Bensheim, Germany) cardioplegic solution was used in 54 patients (HTK group) and the cold blood cardioplegia was used in 58 patients (CB group). Six patients underwent aortic arch replacement (5 HTK, 1 CB), thirty-six patients ascending aorta replacement (5 HTK, 31 CB), seventy patients Bentall operations (44 HTK, 26 CB). Associated procedures also were performed: hemi-arch replacement in ten patients (2 HTK, 8 CB), E®-Vita open (Jotec®, GMBH, Hechingen, Germany) endo-prosthesis implant in two patients (1 HTK, 1 CB), innominate artery re-implantation in two patients (2 HTK). All patients were also classified for the type of operation performed (elective or emergent, see Table 1).
Pre-operative patient characteristics
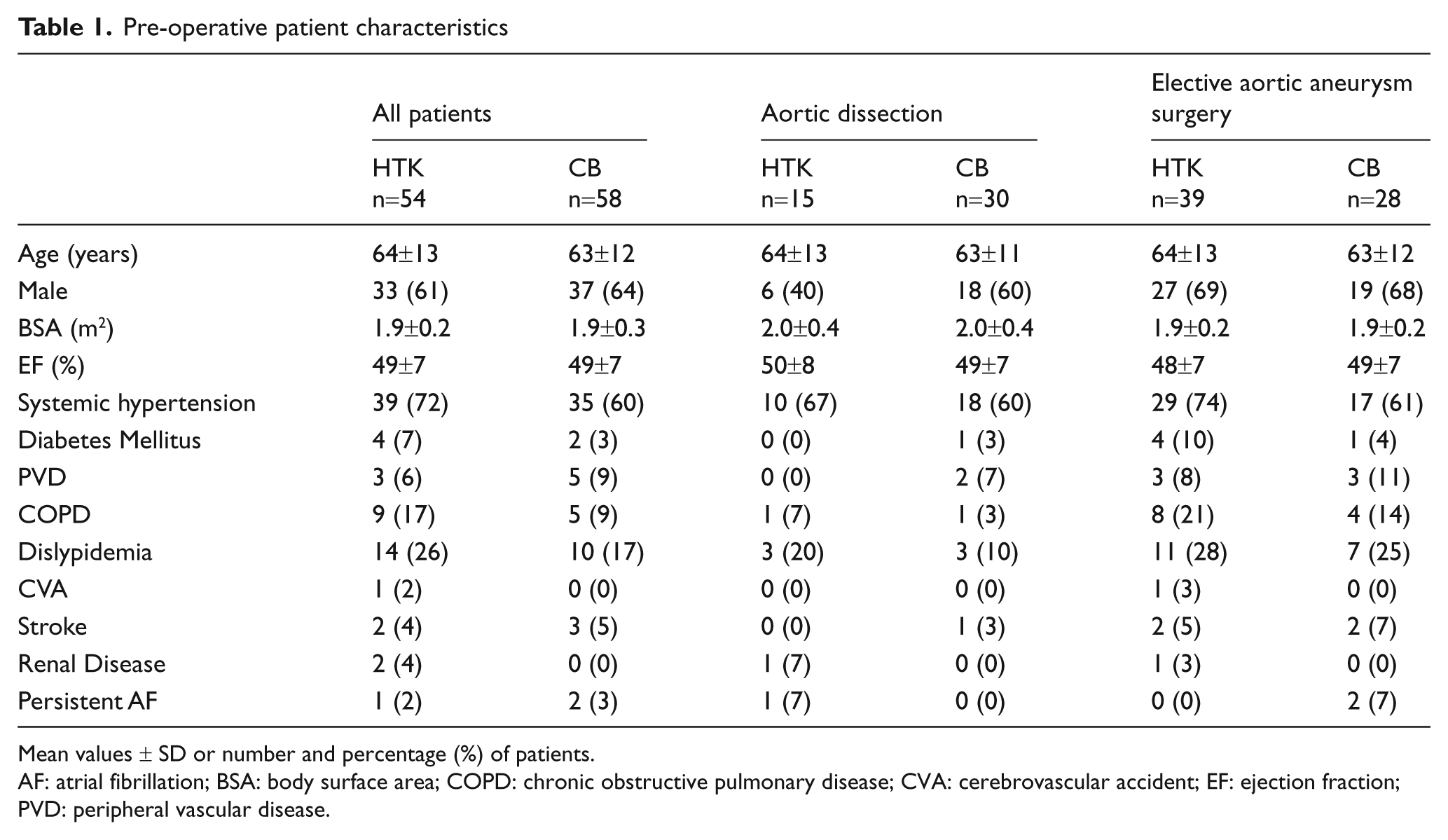
Mean values ± SD or number and percentage (%) of patients.
AF: atrial fibrillation; BSA: body surface area; COPD: chronic obstructive pulmonary disease; CVA: cerebrovascular accident; EF: ejection fraction; PVD: peripheral vascular disease.
The CB group patients were operated on from January 2003 to September 2005 because, in this period, the repeated cold blood cardioplegia was routinely used at our institution in these operations. From March 2005, the HTK–Custodiol® began progressively to be the cardioplegic solution used in thoracic aorta operations.
Patients with known coronary artery disease, mitral valve disease, acute myocardial infarction, cardiac tamponade, Child B/C hepatic failure, renal failure requiring haemodialysis or redo patients were excluded from the study.
Study end points
The primary end point of this study was to assess the efficacy in myocardial protection of a single dose of HTK-Bretschneider compared with repeated cold blood (CB) cardioplegia, both in elective and in emergent thoracic aorta operations, evaluating post-operative cardiac Troponin I (cTnI) release and low cardiac output syndrome (LCOS). The secondary end point is to evaluate clinical outcomes related to the different cardioplegic solutions used.
Surgical management
After premedication with lorazepam, anaesthesia was induced with a combination of fentanyl, midazolam and sodium thiopenthal and maintained with propofol. Muscular relaxation was obtained with pancuronium bromide. Surgical approach was always a median sternotomy. Transesophageal echocardiography was performed in all patients. In aortic arch replacement, patients received bilateral radial artery pressure and cerebral near-infrared cerebral oximetry monitoring. A moderate hypothermic cardiopulmonary bypass (CPB) was established after arterial and atrio-caval cannulation, except in 15 patients in whom a deep hypothermic circulatory arrest (DHCA) associated with antegrade selective cerebral perfusion (ASCP) was performed.
After aortic cross-clamping, myocardial protection was obtained by antegrade administration of the cardioplegic solutions. In the aortic dissection group, the ascending aorta was clamped and then removed. HTK single dose or CB first shot were administered into the aortic root if the aortic valve was continent or through the coronary ostia if aortic regurgitation was present.
HTK solution was cooled to 4-8°C and perfused as a single dose at a dosage of 20-25 ml/kg and at a pressure of 100 mmHg in the first minute and then at 50-60 mmHg. The CB cardioplegia first dose was constituted by cold blood and St. Thomas’ Hospital No. 2 solution (Plegisol®, Abbott Laboratories, Chicago, IL) in a 4:1 blood:cardioplegia ratio and delivered antegradely into the aorta or in the coronary ostia at a dosage of 10-15 ml/kg. As recommended by the manufacturer, 10 mEq of sodium bicarbonate were added to every 1000 ml of St. Thomas’ Hospital No. 2 solution for pH control. Thereafter, 7-10ml/kg of the same solution were given every 20-30 minutes until aortic declamping. Before aortic declamping, normothermic blood “hot shot” was administered. Tranexamic acid (3 g) and heparin (300 U/Kg) were administered in all patients. Intra-operative heparin monitoring was achieved using the standard activated clotting time (ACT, Medtronic Inc., Minneapolis, MN). Additional heparin boluses (5,000 U) were given if the ACT values were below 400 seconds. Protamine sulphate was administered to reverse heparin. All patients were admitted post-operatively to the intensive care unit.
Biochemistry
cTnI levels were measured according to the manufacturer’s recommendation by standard immunoassay technique (Cardiac Troponin-I Flex® Reagent Cartridge, Dade Behring, Newark, DE).
Blood samples for pre-operative measurements were collected the morning of the operation in elective patients or at O.R. arrival in emergent patients, while post-operatively, measurements were performed 6 hours, 12 hours, 24 hours and 36 hours after the operation and then daily until post-operative day (POD) 7.
Statistical analysis
The data are given as mean values and standard deviation (SD) unless otherwise specified; categorical variables are described as frequencies and percentages. Categorical data was tested with the Chi-square test or Fisher’s exact test. cTnI peak values showed a markedly skewed distribution and were transformed to natural logarithm. The linear correlation was assessed by using Pearson’s coefficient. Between-group comparisons were made using Student’s t-test for independent samples or analysis of variance (ANOVA) followed by the Newman-Keuls test for multiple comparisons. The non-parametric Mann-Whitney U-test was used when appropriate. Two-way ANOVA, with interaction term, was used to compare the cTnI peak between groups over quintiles of cross-clamp time. The analyses were made using Statistica 6.1 software (StatSoft Inc., Tulsa, OK), and p-values <0.05 were considered statistically significant.
Results
Pre-operative patients characteristics were similar between groups; only acute aortic dissection was more frequent in patients receiving cold blood cardioplegia (Table 1). Cross-clamp time, CPB time and minimum temperatures reached were similar in both groups (Table 2). In HTK patients, intra-operative ultrafiltration was applied in an higher percentages of patients to avoid excessive hemodilution. There were no differences for intra-operative blood transfusions, hemoglobin or hematocrit values at the arrival in ICU (Table 2). Post-operative data are shown in Table 3. The incidence of LCOS, atrial and ventricular arrhythmias, and the use of inotropic drugs were similar in both groups. One patient in each group required a definitive post-operative pacemaker implant for complete A-V blockade. cTnI release was similar in both groups (see Figure 1) and no difference was found for 30-days mortality.
Intra-operative data
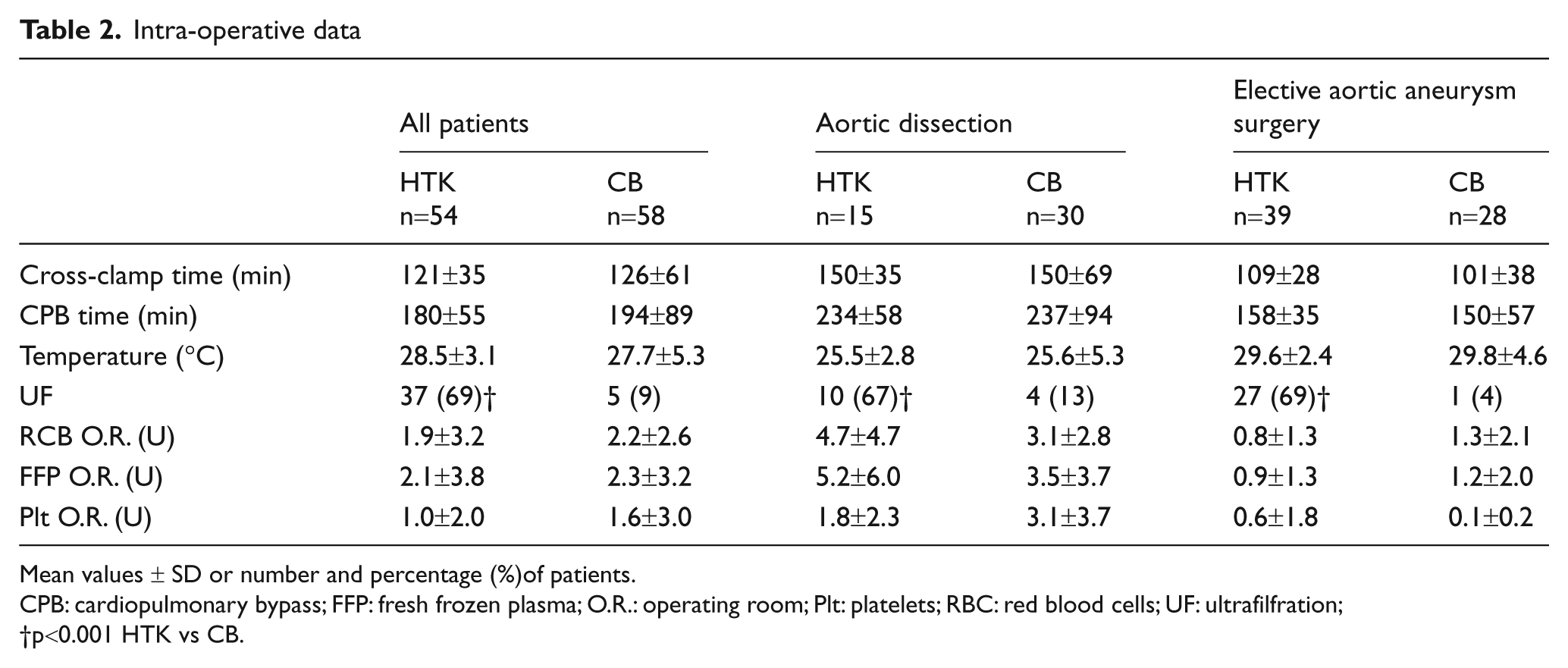
Mean values ± SD or number and percentage (%)of patients.
CPB: cardiopulmonary bypass; FFP: fresh frozen plasma; O.R.: operating room; Plt: platelets; RBC: red blood cells; UF: ultrafilfration;
p<0.001 HTK vs CB.
Post-operative data
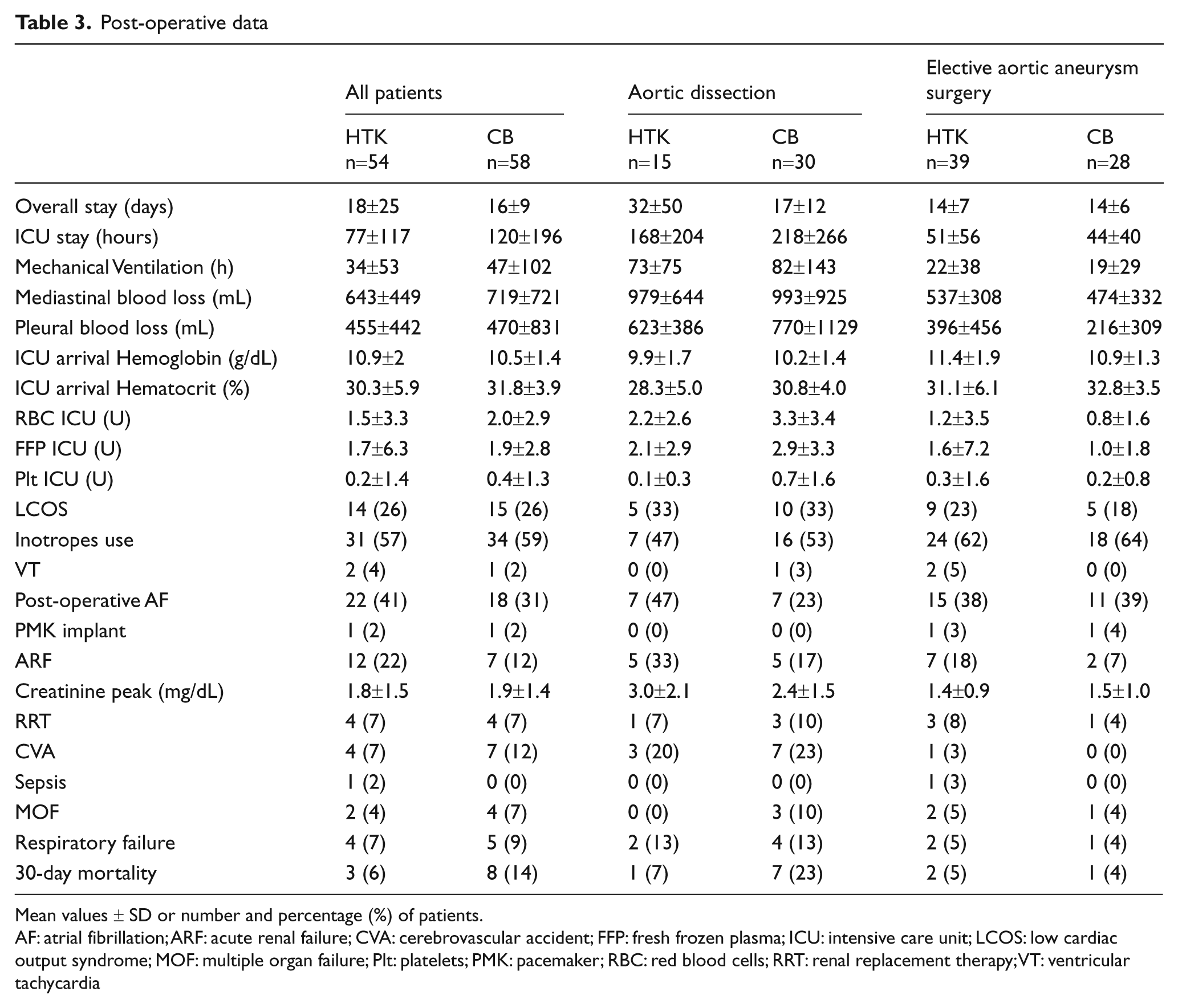
Mean values ± SD or number and percentage (%) of patients.
AF: atrial fibrillation; ARF: acute renal failure; CVA: cerebrovascular accident; FFP: fresh frozen plasma; ICU: intensive care unit; LCOS: low cardiac output syndrome; MOF: multiple organ failure; Plt: platelets; PMK: pacemaker; RBC: red blood cells; RRT: renal replacement therapy; VT: ventricular tachycardia
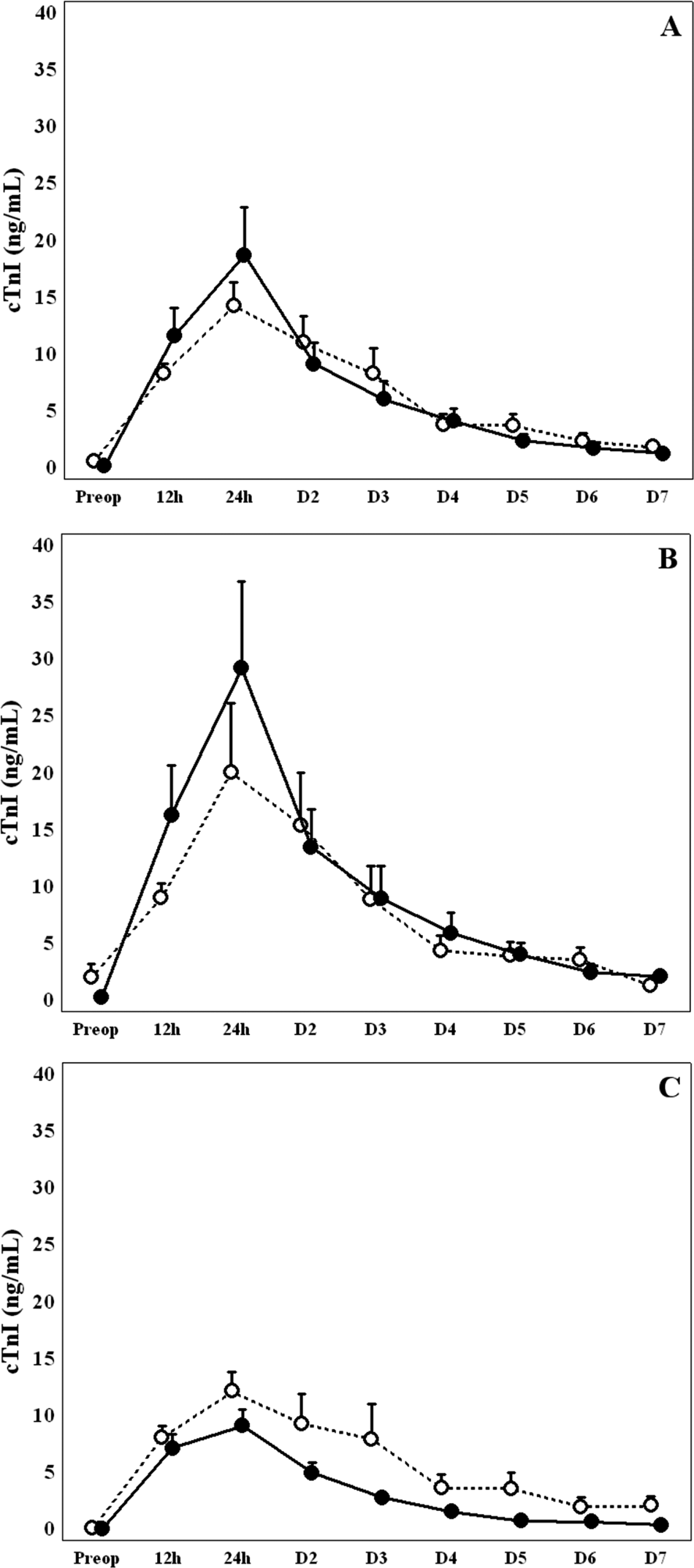
Mean values (Standard Error) of cardiac Troponin I (cTnI) in all patients (panel A), aortic dissection (panel B) and elective aortic aneurysm surgery (panel C) according to HTK (open circle) and CB (closed circle). (D = days; h = hours.)
At linear regression analysis, cTnI peak values correlate positively (r:0,43, p:<0.001) with cross-clamp time on natural logarithmic scale independently of the cardioplegia type used (Figure 2). Two-way ANOVA analysis revealed that cTnI peak values were associated with cross-clamp time quintiles (p<0.001), but not with cardioplegia type (p=0.10) and, particularly, that the type of the cardioplegic solution across cross-clamp time quintiles had an interactive effect on cTnI peak (p=0.012 for the interaction). Figure 3 shows mean cTnI peak values according to cross-clamp time quintiles and cardioplegia type. In the fifth quintile of cross-clamp time (>160 min), CB patients had significantly higher cTnI peak values than HTK patients (p=0.044 at Neuman-Keuls post hoc test). Within the CB group, patients in the fifth quintile of cross-clamp time had, on average, cTnI peaks significantly greater than those of patients with lower cross-clamp times (p<0.01 for each comparison at Neuman-Keuls post hoc test).
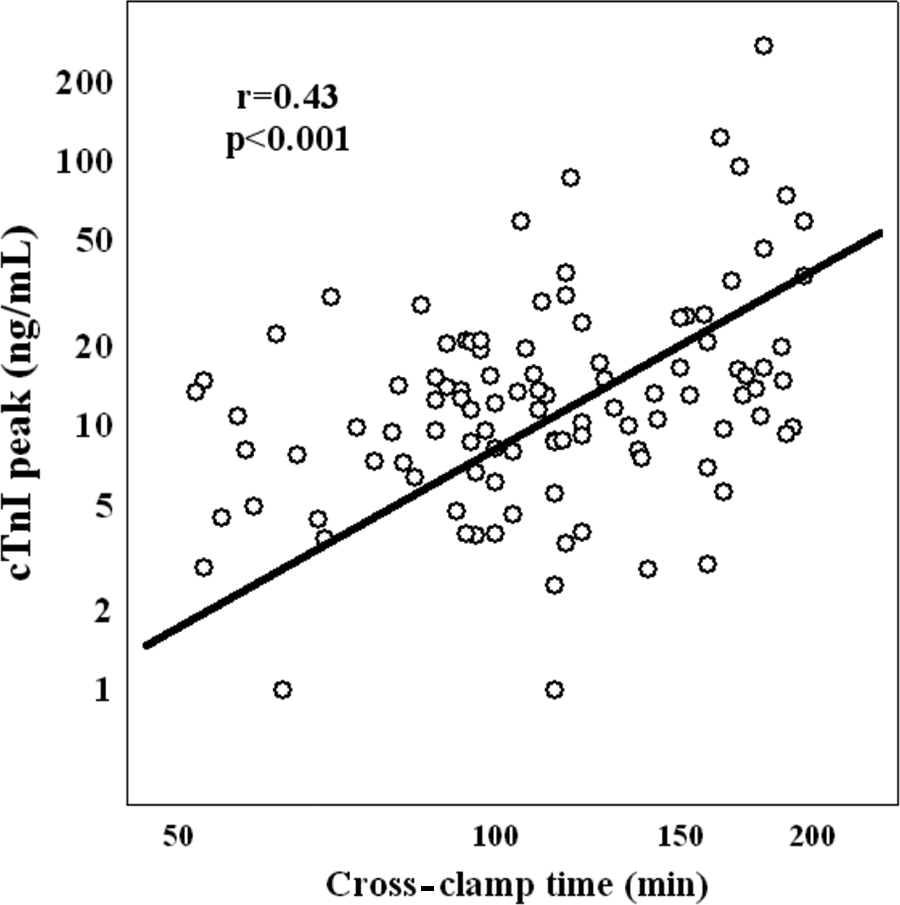
Linear correlation of cardiac Troponin peak values and cross-clamp times on natural logarithmic scale
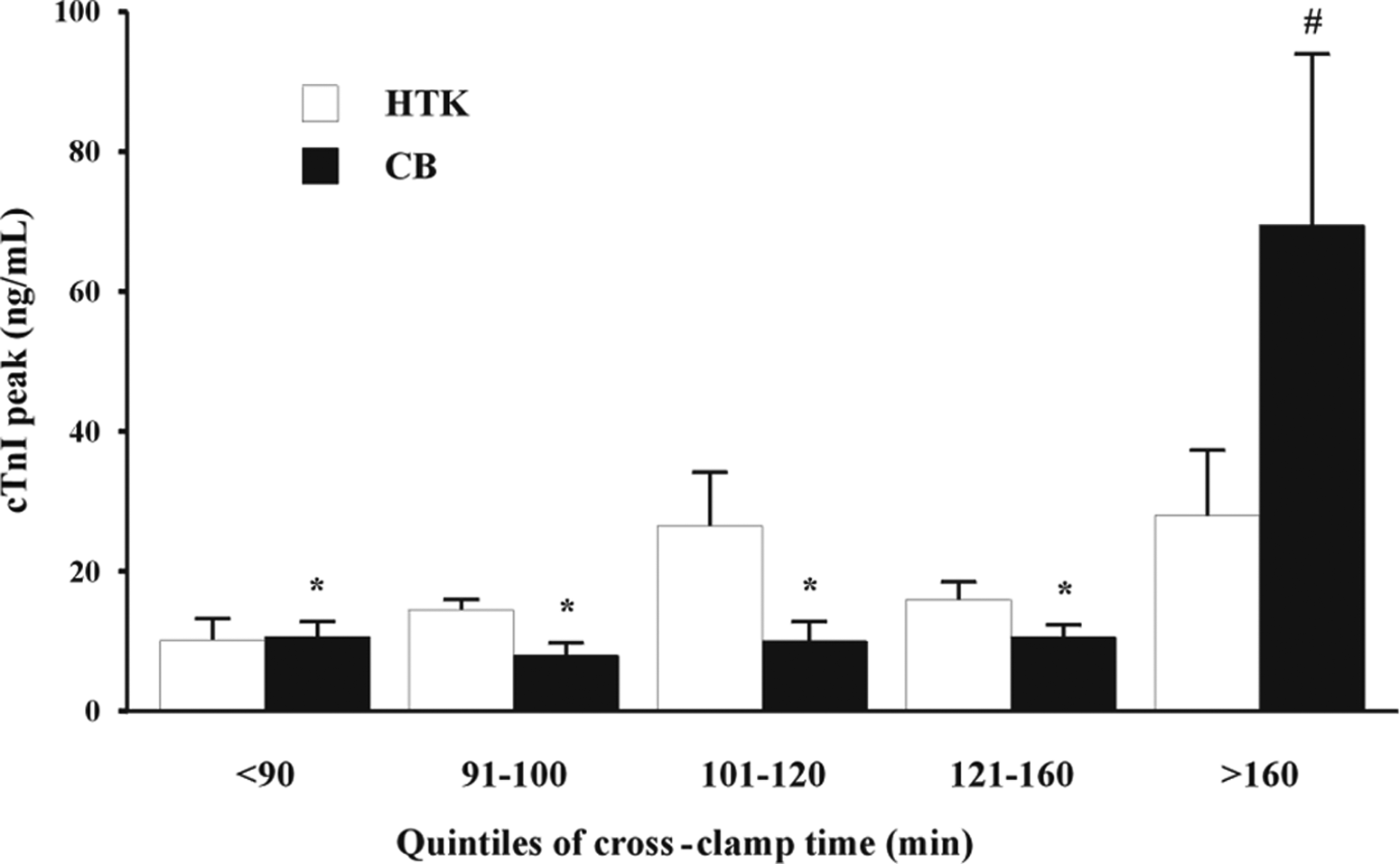
Mean values (Standard Error) of cardiac Troponin I peak values according to HTK (open square) and CB (closed square) cardioplegia and cross-clamp time quintiles. At two-way ANOVA, cardiac Troponin I peak values were associated with cross-clamp time quintiles (p<0.001), but not with cardioplegia (p=0.10). The model revealed that the type of cardioplegia and cross-clamp time had an interactive effect on Troponin I peak values (p=0.012).
Discussion
Myocardial protection during elective or urgent thoracic aorta surgery has never been specifically evaluated, probably because other aspects of this complex type of surgery have been considered more crucial for the clinical outcome analysis. Our study was focused on myocardial protection obtained with two different types of cardioplegia: a single-dose crystalloid and a multi-dose cold blood. The multi-dose strategy might not be the ideal solution for thoracic aorta surgery because it is time-consuming, it is a possible cause of coronary ostia injury and because surgeons tend to prolong the interval between different cardioplegia administrations. A validation of a single-dose cardioplegia administration strategy seems, therefore, warranted in order to simplify the surgical technique in this complex surgery.
Cardioplegic solutions can be classified on the basis of their composition (blood or crystalloids) or according to the temperature at which they are administered (cold or hot) and they may also be classified as extracellular (with high levels of potassium, magnesium and bicarbonates) or intracellular (low level of potassium). The HTK solution (Histidine, Tryptophan, Ketoglutarate) is an intracellular cardioplegic solution designed by Bretschneider in the 1970s and subsequently modified, containing histidine, acting as a buffer against acidosis during the ischemic period, ketoglutarate, an intermediate of Krebs’ cycle and a precursor of nicotinamide dinucleotide phosphate (NAD) which increases energy production during reperfusion, tryptophan, functioning as a membrane stabilizer, and mannitol as anti-edemigen and free radical scavenger7,16,17.
Intracellular crystalloid cardioplegic solutions were compared with extracellular crystalloid or blood cardioplegia solutions in various animal studies and clinical trials. Recently, Fannelop and coworkers found higher cardiac index and a lower cTnI release in the early hours after heart reperfusion in pigs receiving repeated oxygenated blood cardioplegia than in those receiving a single dose of HTK 14 .
Kober and colleagues evaluated, in an animal model, the effectiveness in protection from ischemia-reperfusion injury of three different cardioplegia solutions: HTK-Bretschneider (HTK), St Thomas’ Hospital (STH) and the National Institutes of Health (NIH). After cardioplegic arrest, they noted an increased coronary flow in the HTK group, no differences in cardiac output, a better cellular energy preservation and lower levels of creatinine kinase (CK) and lactate dehydrogenase (LDH) in the HTK and NIH groups, concluding that these solutions gave better protection during cardiac arrest at 25°C than the STH solution 15 .
In thirty elective patients with an average clamping time of 60-65 minutes, receiving HTK or conventional crystalloid cardioplegia, no differences were found for arrhythmias during reperfusion; however, in the postoperative period, HTK patients had a significantly lower incidence of arrhythmias, inotropic support need and lower length-of-stay in the intensive care unit 8 .
HTK solution was compared by Sakata and coworkers with multidose cold blood cardioplegic solution in forty-six patients operated for mitral valve disease. They found similar CK release, inotropic drug support and post-operative cardiac index in both groups, but a higher rate of spontaneous defibrillation and a lower temporary pacemaker stimulation in the HTK group 9 .
At the moment, there are no studies comparing HTK and cold blood cardioplegia in patients undergoing procedures requiring long ischemic time and hypothermia, such as aortic surgery. We decided not to include patients with a known history of coronary artery disease or previous coronary interventions in order to exclude possible bias related to adequacy of myocardial revascularization and delivery through the total myocardium.
Despite longer cross-clamp and CPB times compared to other studies, we found that the incidence of LCOS and post-operative cTnI release were similar in the HTK and CB groups, both for emergent and elective operations. Moreover, post-operative cTnI values in patients with longer cross-clamp times were significantly lower when HTK solution was used and they were similar to cTnI levels of shorter cross-clamp times for both cardioplegic solutions. This could be indicative of an improved protection offered by Bretschneider-HTK solution in longer ischemic times, probably related to its composition. Anaerobic glycolysis is self-limited by the accumulation of end products; histidine removes H+ ions, favoring anaerobic glycolysis and improves recovery of high-energy phosphates 18 , besides, the buffering capacity of proteins, such as histidine, is higher than that of bicarbonate, leading to a better ability to stabilize the cellular pH in ischemic conditions 19 . It has been demonstrated that ketoglutarate improves myocardial protection, enhancing oxidation 20 .
Therefore, we can speculate that repetitive oxygen free radical formation, induced by blood administration, hyperkalemia effects on the endothelium and the relative weakness of the buffer systems could explain why, during long periods of ischemia and hypothermia, there is a trend towards worse myocardial cell protection associated with multidose cold blood cardioplegia, suggesting a possible superiority of HTK solution in these extreme conditions.
Three major limitations should be considered for this study:
First, its retrospective design. Second, although the association between postoperative cTnI release and left ventricle functional changes has been demonstrated by radio-diagnostic methods21,22, the lack of instrumental assessment of post-operative cardiac function is another limitation of the study. Third, in the CB group, there is a higher percentage of aortic dissection, but analyzing patients divided into aortic dissection and elective cases, no differences in the clinical outcomes were observed based on the type of cardioplegia used.
Finally, our data demonstrate that both cardioplegic solutions evaluated in the present study provide satisfactory results. The HTK cardioplegic solution seems to better protect the heart when the cross-clamp time exceeds 160 minutes. The reasons for this result are not clear yet: it could be due to better cellular protection with the HTK solution related to its components or inadequate cold blood cardioplegia delivery for long-lasting and frustrating complex thoracic aorta repair. Adequately designed, prospective, randomized, controlled trials should be performed to corroborate our findings.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
None Declared