
Abstract
Introduction
Cardiac surgery is associated with an inflammatory response, mainly caused by the trauma of surgery, contact of blood with the artificial surface of the circuit, and reperfusion injury 1 . Cardiopulmonary bypass (CPB) induces an immune reaction, primarily by contact of blood with the foreign materials 2 . The inflammatory reaction includes an activation of the humoral and cellular immune system, with enhanced release of cytokines 1 . Their contribution to the development and maintainance of the systemic inflammatory response (SIRS) in cardiac surgical patients is now well established 3 . Some authors have proven that complex technological innovations in mini-invasive systems can reduce the immune response in comparison with standard CPB4,5. The use of more biocompatible materials and minimalization of surfaces (integrated systems) can partly reduce the adverse immune reaction 2 .
Interferons (IFN) are pleiotropic cytokines exhibiting their regulatory effects on the hematopoietic cells. There are two major classes of IFNs: Type I and Type II. The family of Type I IFNs includes three different interferon subtypes: IFNα, IFNβ and IFNω, while there is only one Type II IFN – IFNγ. In order to exert their biological effects, interferons require binding to respective cognate receptors. All Type I interferons bind to the same receptor (Type I IFN R), while IFNγ binds to a distinct Type II IFN receptor. It is composed of two subunits, IFNγR1 and IFNγR2. The major ligand-binding subunit is the 90kDa IFNγR1. IFNγR2 is a 62 kDa protein with a minimal role in ligand binding. Both subunits exert important roles in the IFNγ signaling process 6 . Signaling pathways activated by IFNγ include multiple signaling cascades with pleiotropic biological effects (Jak-Stat pathway, Pyk2 and Fyn tyrosine kinases activation, to name only a few) 7 .
IFNγ is a potent immunomodulator for all immunocompetent cells. Its fundamental role in inflammatory reactions based on TH1 lymphocytes and monocyte/macrophage cells cooperation is well documented. IFNγ is produced by TH1 cells and NK cells 8 . The wide spectrum of IFNγ effects on monocyte activation has already been discovered, including major histocompatibility complex (MHC) class II molecule upregulation9,10. Moreover, monocytes and macrophages activated by IFNγ upregulate the expression of CD14, HLA-DR, and IFNγ receptor on their surface11,12. It has been shown on human peripheral blood mononuclear cells in vitro that treatment with exogonous IFNγ led to the significant enhancement of CD80 costimulatory molecule expression 13 . However, the IFNγ impact on granulocyte functions is yet only scarcely known.
Cardiopulmonary bypass is known to provoke cytokine release to such an extent that a body reaction ressembling systemic inflammation described in sepsis develops in some cardiac surgical patients 14 . Some strategies identifying patients at increased risk of SIRS have already been delineated. The most promising prognostic indicators are serum levels of cytokines IL-12, IL-10, IL-6, IL-2 and IFNγ. Each of the two last mentioned cytokines can be recognized as the indicator of TH1 activity 15 . There are studies demonstrating that IFNγ concetrations did not show any association with a cardiac surgical patient’s clinical parameters or outcome and did not change during the postoperative period14,16,17. On the contrary, some studies of peripheral blood mononuclear cells of patients after cardiac surgery using CPB showed reduced TH1 cell function relative to decreased IFNγ synthesis18,19. The aim of our study is to analyze IFNγ receptor expression on peripheral blood monocytes and granulocytes of patients undergoing cardiac surgery using either standard CPB or modified “miniaturised” CPB.
Methods and Patients
A group of twenty-six patients (4 females and 22 males) was enrolled to this study. Patients were assigned by a cardiac surgeon outside of the research team to undergo coronary artery bypass grafting (CABG), using either standard cardiopulmonary bypass (CPB), “on-pump” surgery, or miniaturised CPB, miniaturised “on-pump” surgery. Thirteen patients underwent “on-pump” surgery (the OP group, 3 females, 10 males; mean age 66.2 ± 8.3 years). Thirteen patients underwent “miniaturised on-pump” surgery (the MOP group, 1 female, 12 males; mean age 65.8 ± 8.6 years). Exclusion criteria consisted of urgent operation, reoperation, combined operation, operative risk more than 5% (according to logistic EuroSCORE), preoperative level of creatinine above 130 mmol/L, hepatic disease and malignancy. Patients in both groups were comparable in age and preoperative ejection fraction and other clinical parameters. The study protocol was approved by the Ethics Committee of the University Hospital in Hradec Kralove, Czech Republic, No. 2005 05 S11P. All participants were informed in detail about the purpose of the study, both orally and in writing. All active subjects gave written informed consent.
Standard cardiopulmonary bypass surgery
Cardiopulmonary bypas was established by standard aortic cannulation and two-stage venous cannulation of the right atrium. Target activated clotting time (ACT) time was over 480 seconds. Cardiac arrest was instituted by antegrade infusion of cold crystalloid cardioplegia (St. Thomas’ Solution, Ardeapharma, Sevetin, Czech Republic) or cold blood cardioplegia (blood to St. Thomas’ Solution in a ratio 4 : 1), repeated every 20 minutes, and topical cooling for myocardial protection was employed. The extracorporeal circuit consisted of a membrane oxygenator (Polystan Safe Maxi, Maquet Cardiopulmonary AG, Hirrlingen, Germany) and a roller pump with non-pulsatile flow (Stöckert S3, Sorin Group, Munich, Germany). The oxygenator and tubing were primed with a mixture of Hartmann’s solution, 10 % Rheodextran solution (molecular weight 40,000), 10% mannitol solution, 8.4% sodium bicarbonate, magnesium sulphate, and 5,000 IU of heparin. Normothermic perfusion with a calculated blood flow of 2.4 ml·l−1·m−2 was used.
Miniaturised cardiopulmonary bypass surgery
Mini-CPB was established using a small 22F two-stage venous drainage and ascending aortic return. Minisystem Synergy® (Sorin Group SrL, Mirandola, Italy) consisted of a centrifugal pump, a membrane oxygenator, a 40 µm arterial line filter and a venous bubble trap. Cardiotomy suction was not used. The whole system, in a closed loop with the surface treated with the PH.I.S.I.O® phosphorylcholine coating (Sorin Group SrL, Mirandola, Italy) and very short tubing, was placed close to the operating field. The priming solution, heparinization, pump flow, temperature and surgery technique were identical with the conventional CPB procedure described above. Cardioplegic arrest, induced according to the Calafiore warm blood-cardioplegia protocol, was administered antegradely into the aortic root. At the beginning of CPB, crystalloid priming solution was flushed retrogradely together with the blood coming from the arterial line to minimize the hemodilution of the patient.
Anesthesiological management
All patients were anesthetized according to the current protocol of the department. Anesthesia was induced using thiopental and midazolam. Muscular relaxation was achieved with cisatrakurium. Anesthesia was maintained with isoflurane and intermittent use of sufentanyl. Continuous infusion of propofol was used as a supplement if needed. Volume-controlled ventilation with FiO2 0.5 was employed. Mean arterial pressure was kept above 50 mmHg with norepinephrine administered as required.
Blood sampling
Blood samples were withdrawn from the subclavian vein before and during surgery, and from the antebrachial vein in the post-surgery period. Samples were collected into Vacutainer tubes treated with lithium heparin (Becton Dickinson, Oxford, UK). In all “on-pump” and “miniaturised on-pump” groups of patients, blood was withdrawn at the following time points:
introduction to anaesthesia, which, in both groups, represented the baseline or reference value for all parameters measured thereafter
termination of operation
1st postoperative day
3rd postoperative day
7th postoperative day
Laboratory analysis
The standard immunofluorescence whole blood staining method was used. Briefly, 25 µl of heparinized venous bood was incubated with monoclonal antibodies for 20 minutes at room temperature. Afterwards, subsequent lysis of the red blood cell (Optilyse C, Immunotech, Marseille, France) samples were washed by buffered saline solution (BSS) and resuspended in phosphate buffered saline (PBS) with sodium azide. The following combination of monoclonal antibodies was used: CD119-FITC/CD14-PE/CD45-APC. Monoclonal antibody reacting with IFNγ receptor was purchased from AbD Serotec, Kidlington, OX, UK (FITC conjugated mouse antihuman IgG2a monoclonal antibody against CD119, clone BB1E2). Anti CD14 mouse monoclonal antibody (clone RMO52 - purchased from Beckman Coulter, High Wycombe, UK) and anti CD45 mouse monoclonal antibody (clone MEM-28 - purchased from Exbio, Praha, Czech Republic) were used to distinguish monocyte and granulocyte subpopulations. Isotypic control IgG2a-FITC/IgG2a-PE (Beckman Coulter) and IgG1-APC (Caltag, Little Balmer, Bucks, UK) were used to identify non-specific staining. Measurements were performed using the FACSCalibur flow cytometer and data were acquired by CellQuest software (BD Bioscience, NY, USA). Monocytes and granulocytes were identified on the basis of different CD45 v. CD14 expression (leukogate). The data analysis was done using FlowJo software (Tree Star Inc., Ashland, OR, USA). Results of flow cytometric analysis of CD119 expression were expressed as median fluorescence intensity (MFI) in a given population.
Statistical analysis
The expression of IFNγ receptor was analysed separately in the population of monocytes and granulocytes. The expression was characterized by median fluorescence intensity (MFI) for each population. The expression of IFNγ receptor was expressed as changes in the MFI value in the postoperative period. The preoperative MFI value was considered as a baseline level. Differences within each group of patients were detected using the Friedman test and the Wilcoxon pair test. Differences between the groups of patients were assessed using the Kruskal-Wallis test. The Bonferroni correction was applied when the Wilcoxon and Kruskal-Wallis tests were used for multiple comparisons. Clinical data were analyzed by Fisher’s exact test, the Mann-Whitney U test and a t-test. Differences were considered significant at p<0.05. Data are expressed as medians and interquartile ranges in plots. Plots also display the range of non-outlier values.
Results
The expression of IFNγ receptor on monocytes and granulocytes in cardiac surgery patients followed a similar trend. All patients samples displayed the rise of IFNγ receptor expression in the early postoperative period and subsequent drop to the preoperative value during the late postoperative phase. It is apparent from results shown in Figure 1 that INFγ receptor expression on monocytes peaked on the 1st postoperative day, both in the standard “on-pump” and the “miniaturised on-pump” patients.
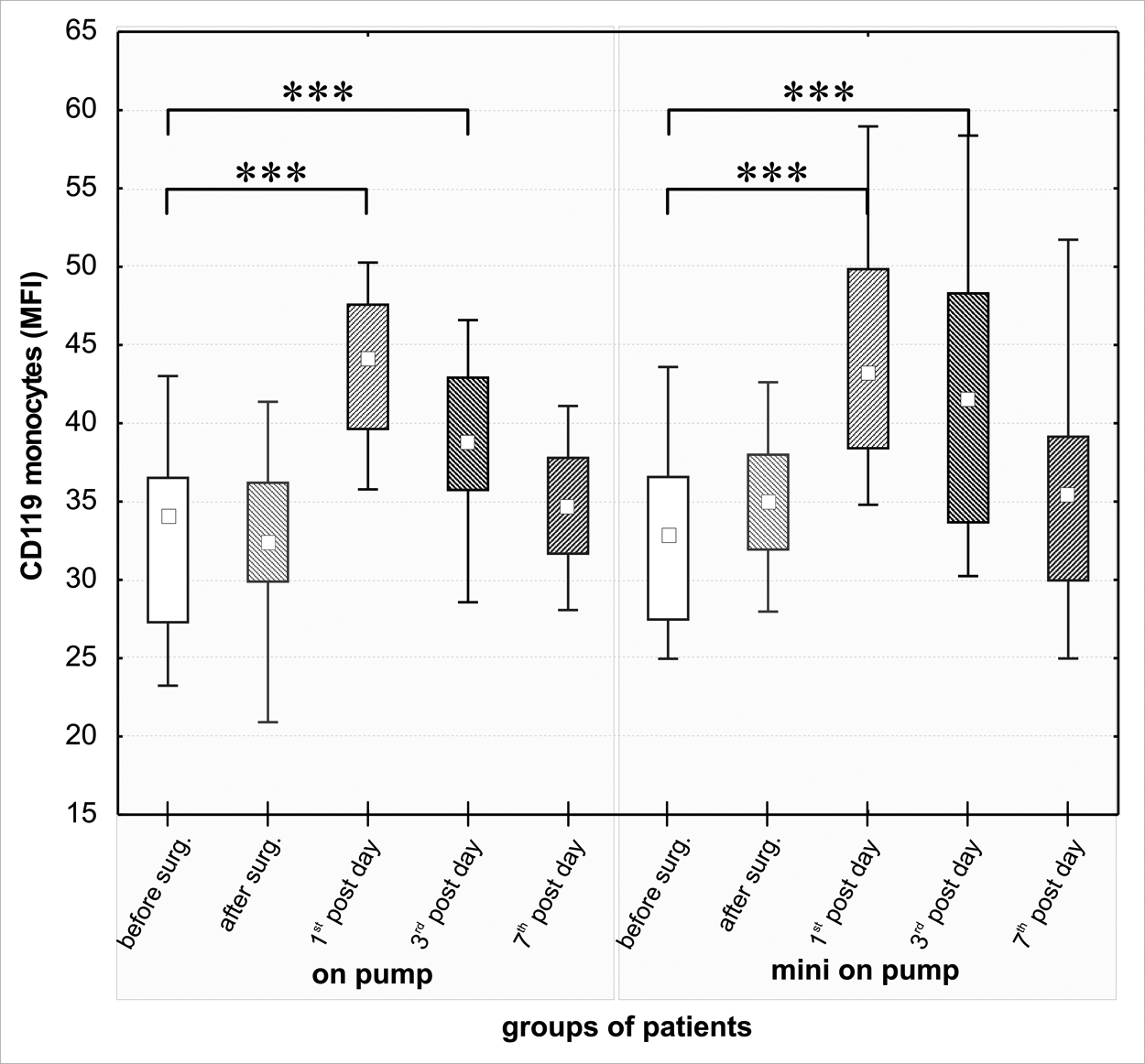
Expression of IFNγ receptor (CD119) on monocytes of “standard” CPB patients and “miniaturised” CPB patients (square: median; boxes: quartiles; whiskers: non-outlier range; significance: *** p < 0.001)
The statistically significant increase of IFNγ receptor expression on monocytes with respect to preoperative value (“on-pump”: median MFI 34, IQR 28 - 36; “miniaturised on-pump”: median MFI 33, IQR 27 - 36) appeared both on the 1st (“on-pump”: median MFI 44, IQR 40 – 47; “miniaturised on-pump”: median MFI 46, IQR 39 - 49) and 3rd postoperative days (“on-pump”: median MFI 39, IQR 36 – 43; “miniaturised on-pump”: median MFI 42, IQR 34 – 48) (p<0.001). Any difference between “on-pump” and “miniaturised on-pump” patients in monocyte IFNγ receptor expression was not found (Fig1).
The expression of IFNγ receptor on granulocytes displayed both the different intensity and timing in both groups of patients studied (Fig2). The change in granulocyte expression of IFNγ receptor is more rapid and pronounced. We found the highest intensity of IFNγ receptor staining immediately after surgery in “on-pump” patients (median MFI 35, IQR 27 – 42) in contrast to “miniaturised on-pump” patients in whom IFNγ receptor granulocyte expression peaked on the 1st postoperative day (median MFI 30, IQR 23 – 32). Nevertheless, the rise of IFNγ receptor expression was significant in both groups of patients (p<0.01) in comparison to the preoperative value (“on-pump”: median MFI 19, IQR 17 – 22; “miniaturised on-pump”: median MFI 19, IQR 17 – 20). In view of this fact, a statistically significant difference between “on-pump” and “miniaturised on-pump” patients in IFNγ receptor expression immediately after surgery was found (“on-pump”: median MFI 35, IQR 27 – 42; “miniaturised on-pump”: median MFI 23, IQR 21 – 28 (p<0.05). We found the divergence in IFNγ receptor expression during the first half of postoperative period in both groups of patients. Whereas, in the “miniaturised on-pump” patients, granulocytes demonstrated a slow and gradual increase in IFNγ receptor expression from preoperative levels to significantly increased expression at the end of surgery (median MFI 23, IQR 21 – 28) (p<0.01), on the 1st (median MFI 30, IQR 23 – 32) (p<0.05) and on the 3rd postoperative days (median MFI 24, IQR 20 – 28, p<0.05), the dynamics of IFNγ receptor expression is rather different in “on-pump” patients. It seems that the “on pump” patients restore more promptly the density of IFNγ receptor expression on granulocytes to the preoperative level compared to “miniaturised on-pump” patients.
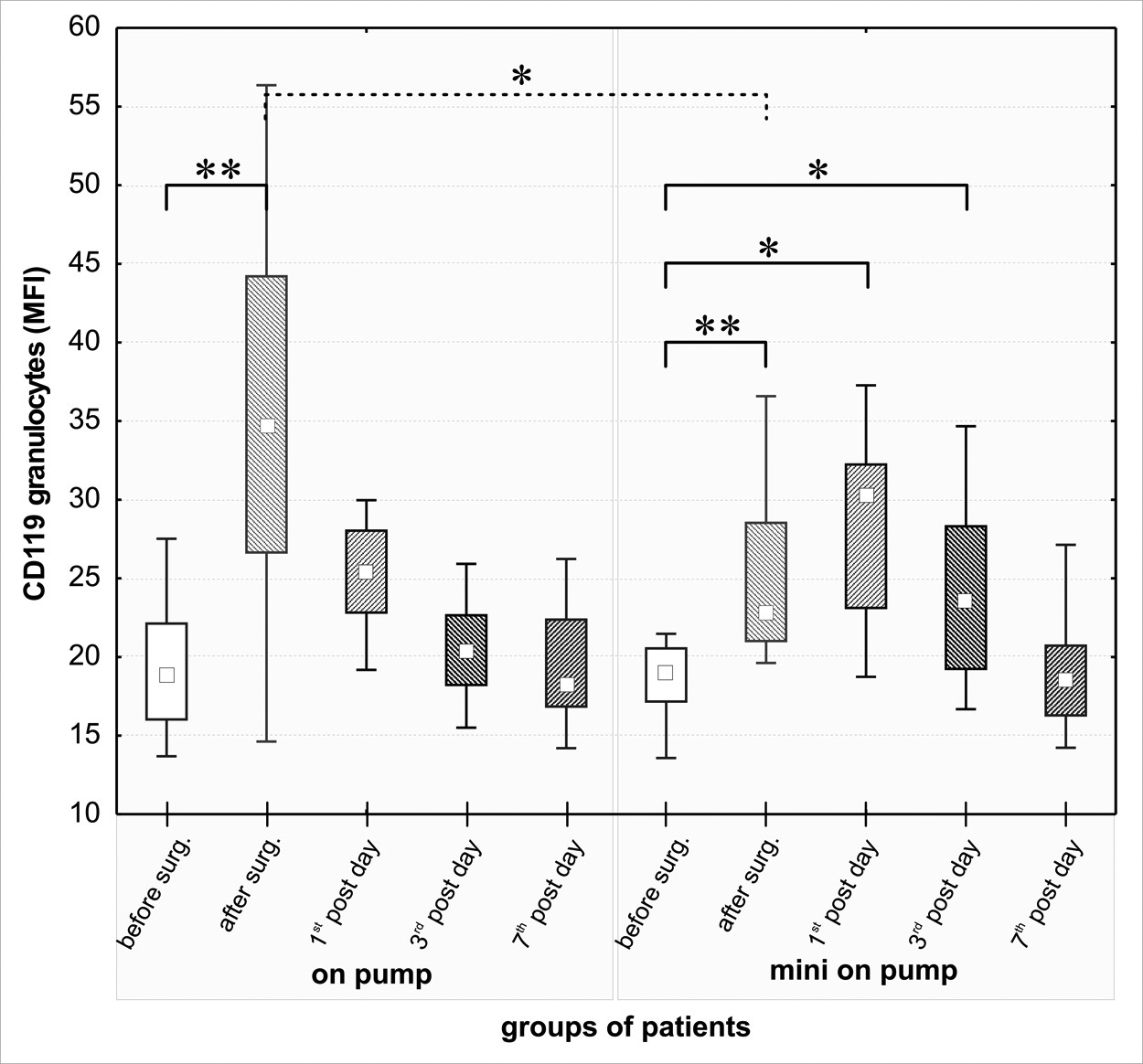
Expression of IFNγ receptor (CD119) on granulocytes of “standard” CPB patients and miniaturised” CPB patients (square: median; boxes: quartiles; whiskers: non-outlier range; significance: * p = 0.05 – 0.01; ** p = 0.01 – 0.001)
Discussion
Interferon γ is a prominent pro-inflammatory cytokine with a strong immunomodulatory effect on cell-mediated immunity. This cytokine is a potent activator of neutrophils and macrophages 20 . IFNγ, together with GM-CSF, is known to induce the production of other pro-inflammatory cytokines, such as TNFα, and is able to enhance some membrane molecule expression, such as HLA-DR and various costimulatory molecules11,21. As the effect of IFNγ is determined by the binding of this cytokine to its membrane cell receptor, its biological function can be modulated by both its entire production and by modulation of membrane receptor on target cells.
Cardiopulmonary bypass is recognized as an integral part of a routine procedure in cardiac surgery, which reveals limited-harm side effects. However, a small number of patients undergoing cardiac surgery using CPB develop postperfusion syndrome – an exaggerated form of life-threatening systemic inflammatory response syndrome – SIRS 22 . This hyper-inflammatory response can be characterized by increased plasma levels of pro-inflammatory cytokines and acute phase proteins and leukocyte activation 20 . Numerous functions are altered in circulating leukocytes in SIRS patients. Together with pro-inflammatory status, anti-inflammatory regulatory circuits are adopted in these patients. It was proposed that circulating anti-inflammatory mediators contribute to the bodýs normal response to prevent systemic inflammation. On the other side this, the “Compensatory Anti-inflammatory Response Syndrome” (CARS) can enhance the susceptibility to nosocomial infections 23 .
To minimize the deleterious inflammatory response during the perioperative period in CPB patients, the modified mini-extracorporeal circulation method has been developed in the last decade. The “Miniaturised on-pump” system has been shown to reduce postoperative cytokine levels and the levels of other markers of inflammation, such as IL-6, TNFα, granulocyte elastase, and IL-10 in “miniaturised on-pump” patients in comparison with standard “on-pump” patients5,24. However, IFNγ serum levels showed no change during the postoperative period in cardiac surgical patients nor did IFNγ levels display any association with the clinical outcome14,16.
The monocyte-macrophage population is the principal regulatory cell component responsible for morbidity associated with CPB 25 . Previous studies have demonstrated activation of monocyte functions during CPB12,25. The activation of monocytes is naturally associated with altered membrane molecule expression and enhanced cytokines production. The monocyte-macrophage lineage has been proposed to have the functional heterogeneity characterized by pro- to anti-inflammatory status polarization after CPB 25 . Our observation suggests strong activation of the IFNγ receptor on monocytes in the early postoperative period, culminating on the 1st postoperative day and decreasing on the 7th postoperative day studied. These postoperative monocyte changes, comprising their early activation and subsequent suppression, were demonstrated by other studies12,25,26s. Our analysis did not reveal any differences in IFNγ receptor expression on monocytes with respect to the type of CPB.
The principal effector cell population in which number and function are substantially induced by cardiopulmonary bypass is the granulocyte population. Granulocytes play a central role in the early phase of systemic inflammation, the development of postoperative complications, and granulocyte-mediated tissue injury22,25,27. Postoperative granulocyte priming is documented as elevated respiratory burst, increased cell surface integrin CD11b/CD18 expression, granulocyte elastase release and reduced apoptosis20,22,23,27. Reduction of granulocyte apoptosis represents a major cause of granulocytosis and is responsible for the destructive potential of these cells during SIRS 28 . Our results demonstrated a rapid increase of IFNγ receptor expression on granulocytes of cardiac surgical patients undergoing surgery with the support of standard cardiopulmonary bypass, immediately after finishing the surgery. It is apparent that granulocyte IFNγ receptor expression in these patients is induced more quickly and more extensively compared to patients undergoing cardiac surgery using modified “miniaturised on-pump” surgery. It could be suggested from our results that it is caused by the entire differences between the standard and “miniaturised” cardiac surgical approaches. If we assume constant IFNγ levels during the peri- and post operative periods and no plasma level association with clinical outcome14,16, enhanced membrane IFNγ receptor expression on granulocytes could be associated with a stronger inflammatory response in cardiac surgical patients operated with the standard extracorporeal circuit. It was shown by Franke et al. in in vitro experiments that IFNγ synthesis is significantly reduced after major surgical trauma, but this IFNγ synthesis reduction in T cells can be reversed by IL-1218,19. Hence, the cytokine network in cardiac surgical patients can display considerable complexity, reflecting different antagonistic processes.
We found, to our knowledge for the first time, that IFNγ receptor expression on granulocytes of patients undergoing cardiac surgery is significantly modulated by the type of cardiopulmonary bypass. Our finding that IFNγ receptor expression is less expressed on granulocytes of “miniaturised on-pump” patients is in accordance with some other observations that the “miniaturised on-pump” surgery elicites lesser immune response than the standard one5,24,29.
Footnotes
Acknowledgements
This work was supported by Ministry of Education, Czech Republic, project No. MSM0021620812 and the grant SVV-2010, No. 260906 Charles University in Prague, School of Medicine Hradec Kralove.
None Declared.