
Abstract
Simulation for perfusion education has been used for at least the past 25 years. The earlier models were either electronic (computer games) or fluid dynamic models and provided invaluable adjuncts to perfusion training and education. In 2009, the *North Shore-LIJ Health System at Great Neck, New York, opened an innovative “Bioskill Center” dedicated to simulated virtual reality advanced hands-on surgical training as well as perfusion simulation. Professional cardiac surgical organizations now show great interest in using simulation for training and recertification. Simulation will continue to be the direction for future perfusion training and education. This manuscript introduces a cost-effective system developed from discarded perfusion products and it is not intended to detail the actual lengthy process of its construction.
Simulation for perfusion training has been used for at least 25 years. The earlier models were either electronic or hydraulic fluid dynamic model. These models were as simple as a fluid-holding reservoir with tubes simulating inlet and outlet into the “patient” in addition to smaller diameter tubes simulating suctioning, venting and transfusions. Instructors, hidden behind a curtain with the reservoir, would use various clamping methods to simulate fluid dynamic changes during cardiopulmonary bypass. This was commonly known as the “bucket” model.
An electronic model such as the “**Jostra” simulator was sophisticated. The Jostra simulator was an electronic game-type program. It was diverse in demonstrating fluid dynamics, blood gases, blood chemistry, drug interactions and perfusion hazards with animation. It was reactive, but lacked realism because it was formatted and designed as an electronic computer game without a fluid dynamic component.
Over the years, various fluid dynamic models were developed with some sophistication, but none with automated responses 1 . The term “high fidelity” was developed by Tallman and Austin at Midwestern University, U.S. Here, “high fidelity” connotes realism; it does not necessary mean simulator “sophistication”. Realism may be achieved with less sophisticated equipment. In essence, the “bucket” model, when properly arranged and designed, may simulate a high level of realism or high fidelity.
There is strong evidence that practice of simulation improves performance and safety 2 . Whether high fidelity has significant benefits over “low fidelity” simulation has yet to be studied. There is strong evidence, however, that simulation of any kind is of great value and has been proven to have a significant effect on safety and performance. This should be a compelling reason for all educational programs to have simulation, since cost is not a factor 4 . However, the “ bucket” model is labor intensive. In order to effectively utilize high fidelity simulation, a low cost sophisticated unit is developed as the RPSS. Evolution to a more sophisticated model, however, appears to be the present trend. Therefore, integration of an electronic model such as the “**Jostra” with a fluid dynamic model will bring a high level of sophistication. The Orpheus3,5 and the CPB-SIM 6 are such models that have been recently developed.
The American Association for Thoracic Surgery (AATS) and the Society of Thoracic Surgeons (STS) are considering using simulation for recertification of surgeons. 7 Airline and military pilots already have this certification process in place. Coincidentally, many training centers for medical education also have sophisticated simulation education centers as an essential modality for training. For example, recently, the *North Shore-LIJ Health System, in New York, opened a “Bioskill Center” dedicated to simulated virtual reality for advanced hands-on surgical training. Movement for sophistication of cardiopulmonary bypass simulation training certainly then should be a priority educational goal of the perfusion profession.
The Real Patient Simulation System I
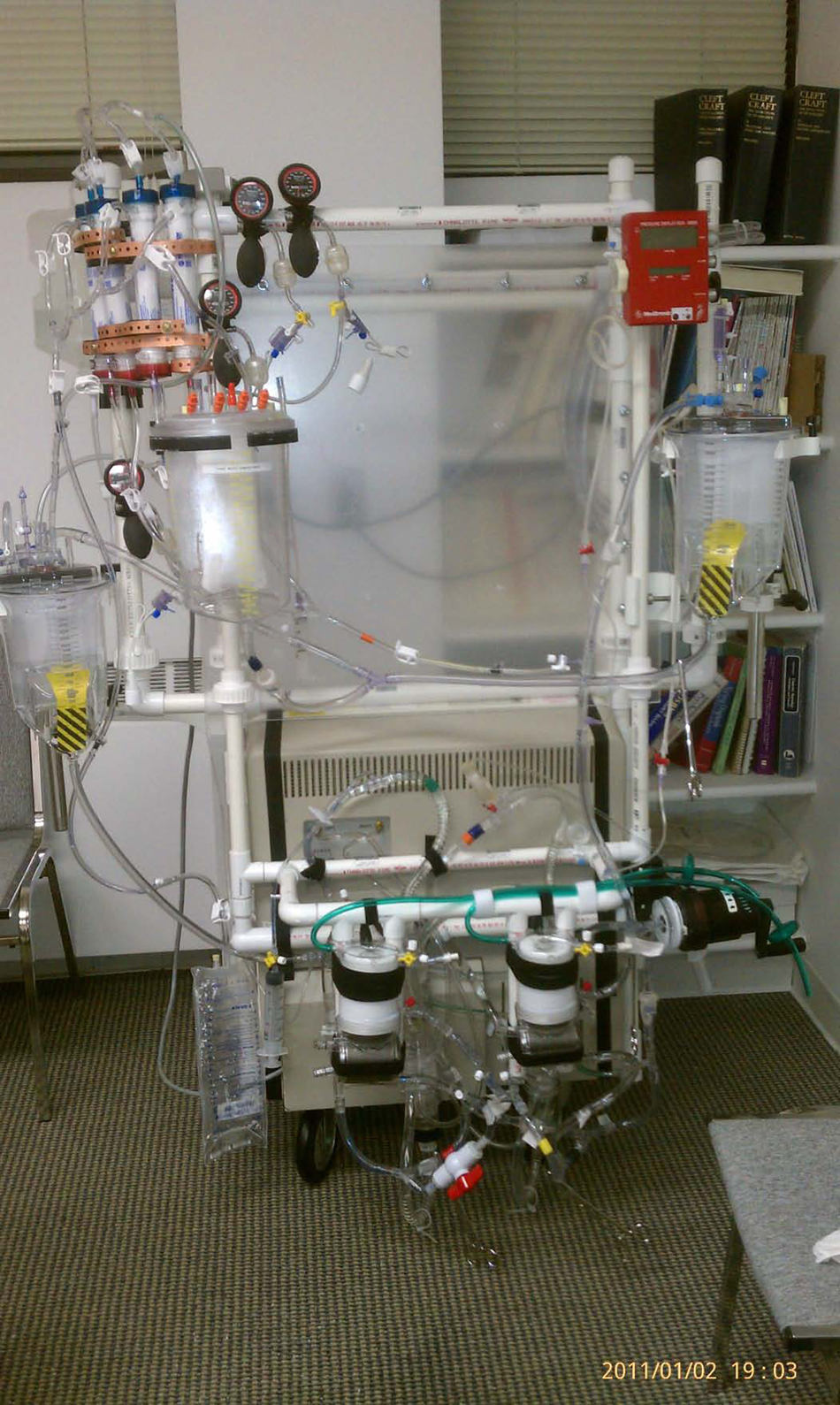
The concept of the Real Patient Simulation System (RPSS) was to simulate, hemodynamically, a human patient responding and reacting to changes during CPB in cardiac surgery. The changes are caused by the heart-lung machine along with the changes inside the patient, such as “fluid shift”. This simulator, mimicking the patient’s hemodynamic system, was constructed from a commercial pulsatile ventricular assist device that behaves similar to that of a human patient. The Real Patient Simulator System I (RPSS I) can produce many clinical scenarios, such as partial, total, weaning from and termination of cardiopulmonary bypass with automated responses. Each sub-system of the RPSS I had been tested previously with blood and the sub-systems were assembled and incorporated into this generation one fluid dynamic model (Figures 1 and 2).
RPSS I
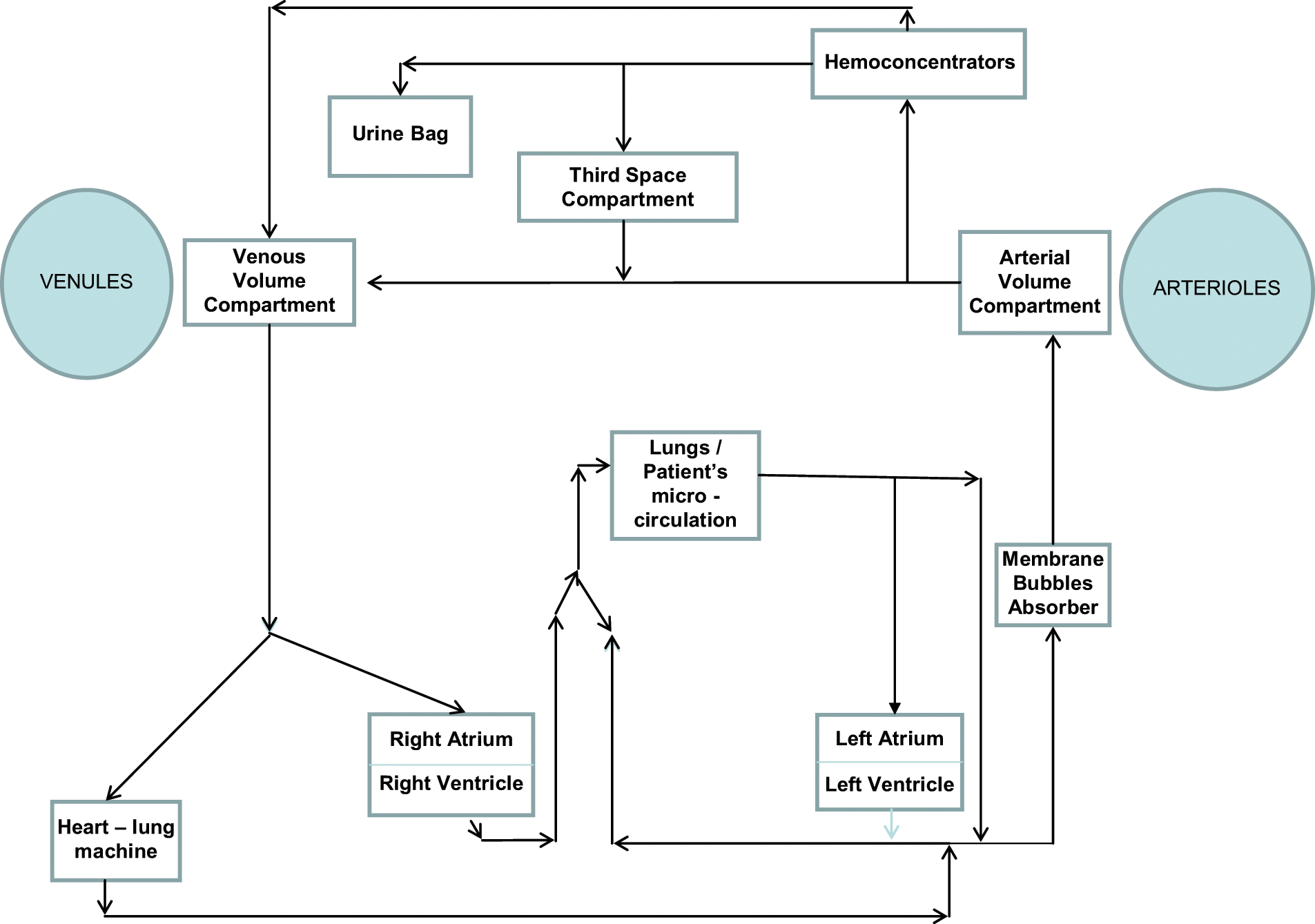
Diagram of the RPSS I simulator.
The RPSS I was made of extracorporeal perfusion products and accessories. It mimics a patient’s hemodynamic reaction to changes during cardiopulmonary bypass. When integrated with a software program in the future, this simulator will simulate and demonstrate extensive clinical scenarios for training and testing of cardiovascular students and perfusionists.
The RPSS I was made from a commercially available ventricular assist device system, two oxygenators, three reservoirs (3,500 ml capacity each), four hemoconcentrators, disposable transducers, a centrifugal pump head, mechanically operated valves, clamps, manometers and polyvinyl chloride tubings. The ***Abiomed BVS 5000i is an automated pulsatile cardiac support system. Each Abiomed unit is a two-chambered disposable device. A trileaflet artificial mechanical valve separates the two chambers. A single unit is intended to support one side of the heart. Therefore, two units will support the right and the left side, making it a bi-ventricular assist device. The unit’s pump rates, and systolic and diastolic intervals are determined automatically (sensitive to filling volume / pressure of the upper chambers) with airflow from the console to the unit. The console drives and adjusts the left and right units independently of each other.
The RPSS I was made from two disposable units of the Abiomed system. One unit simulates the “right side” and the other unit simulates the “left side” of the heart. The top chambers of the units behave like “atriums” and the bottom chambers function like “ventricles”. Under normal operation as a ventricular assist device, in support of the patient’s heart, each unit is designed to produce pulsatile flow and to function and react to volume or filling pressures as seen in the Frank–Starling law of the heart. This well-recognized law states that the stroke volume of the heart will increase in response to an increase in the volume of blood filling the heart. This increased blood volume stretches the ventricular wall to cause cardiac muscle to contract more forcefully 8 . The BVS5000i’s mimicking of the Frank-Starling law is well published in various literatures and this mimicking makes the BVS5000i the perfect model for simulating the fluid dynamic transitions of partial, total, weaning from, and termination of cardiopulmonary bypass clinical scenarios (Figure 3 and 4).
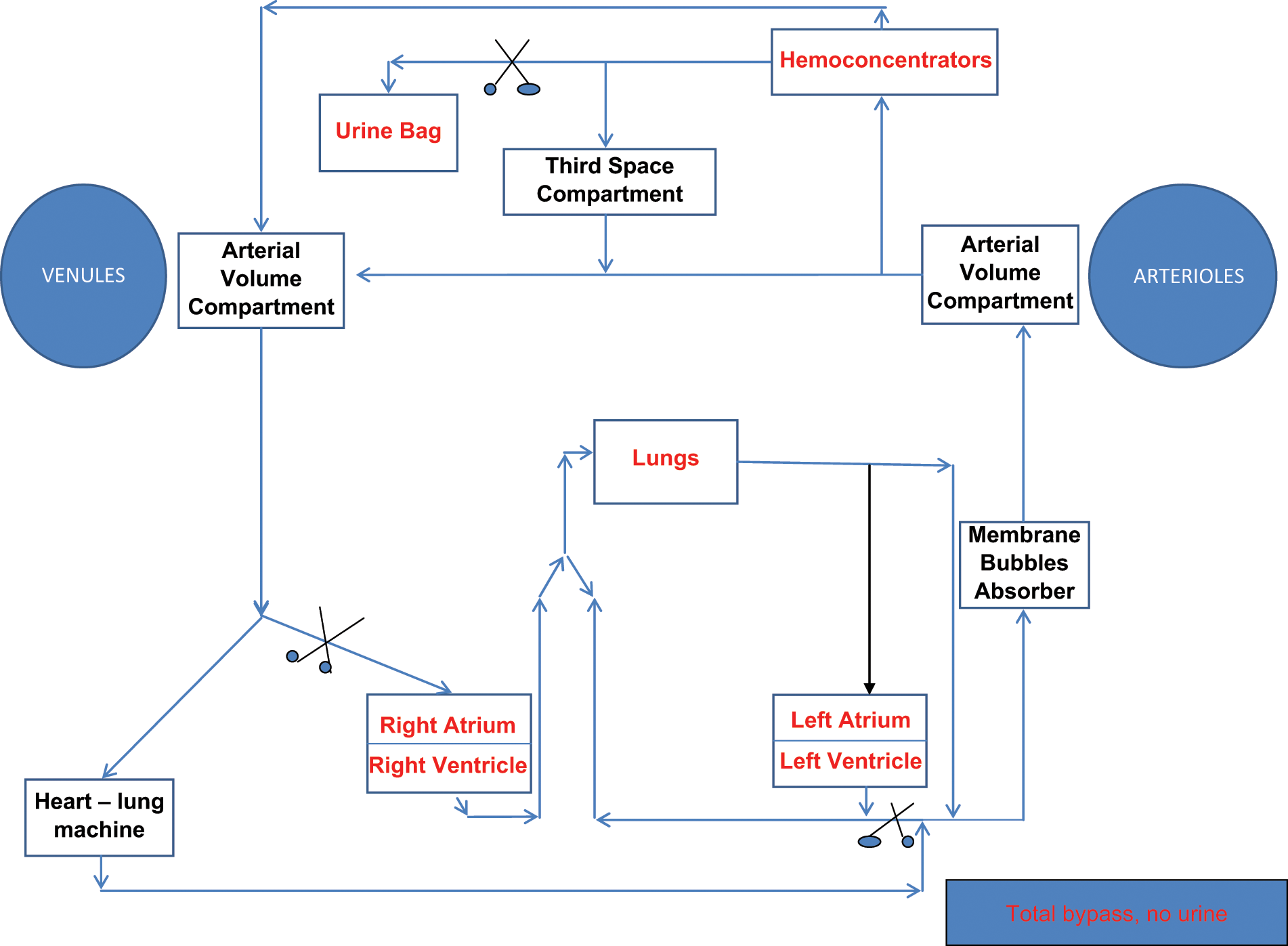
RPSS I simulating a total bypass scenario where the patient produced no urine on bypass.
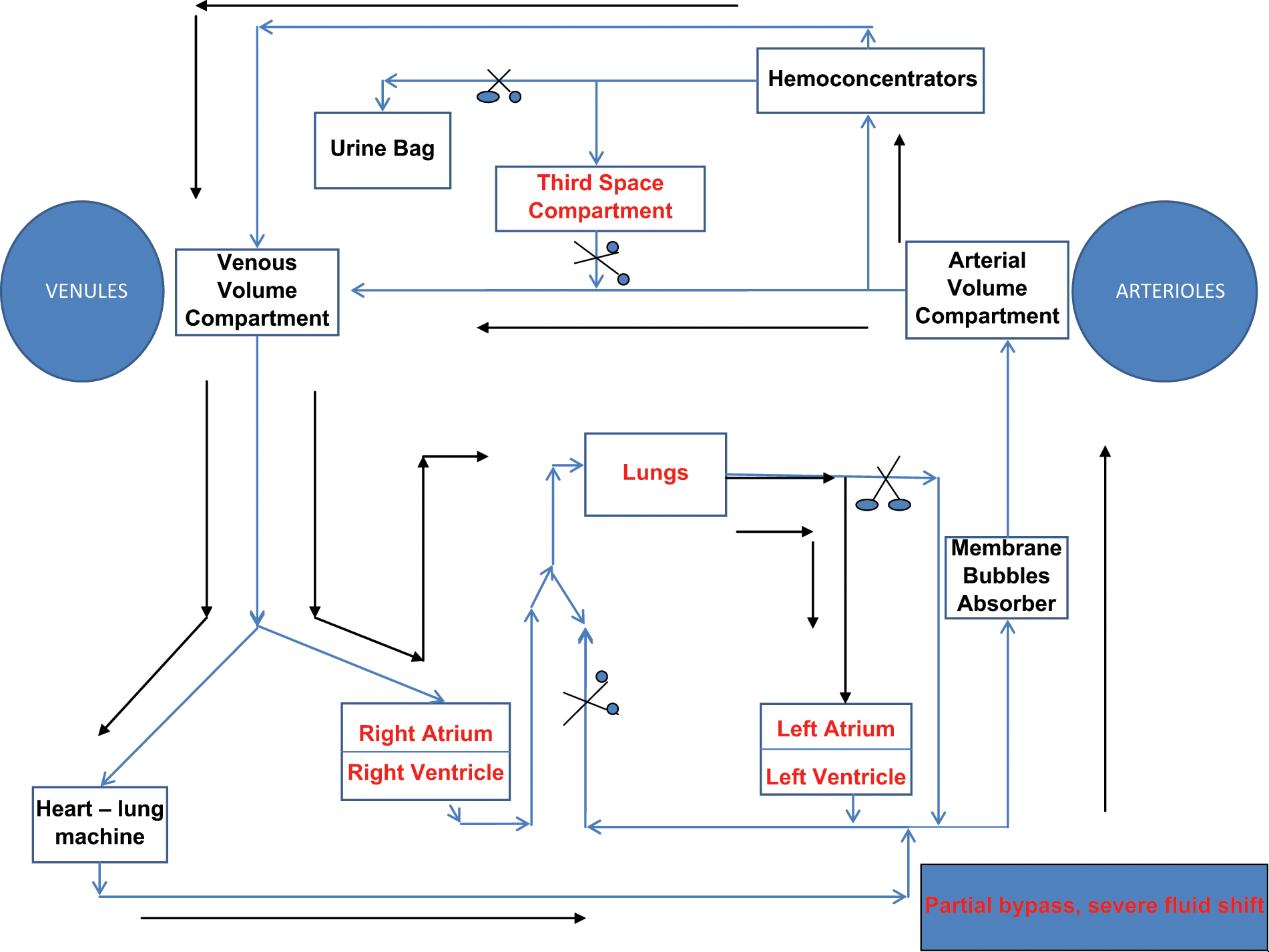
RPSS I simulating a partial bypass scenario where there was a severe fluid shift into the third space compartment.
A membrane oxygenator simulates the “patient’s lungs”. The “right ventricle” (right ventricular assist device unit) connects to the inlet of the “patient’s lungs”. The outlet of the “patient’s lungs” returns volume to the top chamber of the “left side”, which functions like the left atrium. From the bottom of the “left side” unit, which functions like the left ventricle, volume goes into a reservoir called the “arterial volume compartment”. From the arterial volume compartment, volume may be directed to one of several different compartments: to a reservoir called the “third space compartment” and/or it may flow to another reservoir called the “venous volume compartment” and/or it may be diverted to the hemoconcentrators which simulate the “patient’s kidneys”. From the venous volume compartment, volume may drain into the venous reservoir and/or be directed to the top chamber of the “right side” which functions like the right atrium, depending on the simulation mode.
The second membrane oxygenator functions as a bubble absorber, like a “patient” would in absorbing microbubbles. This device simulates the patient’s absorption of bubbles and allows studies of gas emboli caused by devices found in clinical situations. Negative pressure is applied to the gas phase of the oxygenator and it becomes an effective bubble eliminator. The ability or amount of bubbles absorbed can be controlled. The inlet of this device can be connected to the outlet of the “left ventricle” and the outlet can be connected to the arterial volume compartment. This concept was tested in conjunction with experiments requiring effective microbubble absorption in a test circuit (Circulatory Technology, Oyster Bay, New York).
The bubble absorber is important, for example, in simulating gaseous microemboli, which can be demonstrated when an instructor loosens purse string sutures around the venous cannula to deliberately entrain air into the venous line to introduce a continuous stream of bubbles into the bypass circuit. The use of a bubble detection sensor at the outlet of the membrane oxygenator would detect and measure the bubbles in the circuit due to the Venturi effect. If the vigilant perfusionist exercises the proper corrective actions to discover and eliminate the source of the bubbles, then the instructor can use the absorber to control and absorb bubbles in simulating the reduction and successful resolution of the source of the gaseous microemboli.
The “patient’s kidneys” are the four hemoconcentrators. Mechanical partial occlusion is needed to control simulation of diuresis from the ultrafiltration output conduit. The hemoconcentrators are arranged in parallel and have an effective total ultrafiltration rate up to 700 mL per minute.
The “patient’s fluid spaces” are the three reservoirs: arterial volume compartment, venous volume compartment and third space compartment. The arterial line from the heart-lung machine is connected to the arterial volume compartment via the bubbles absorber. The arterial volume compartment is connected to the venous volume compartment and the venous volume compartment is connected to the venous line of the heart-lung machine. Some of the volume from the venous line is diverted to the “right atrium” when partial bypass is simulated. The third space compartment is connected in parallel to the arterial volume compartment and the venous volume compartment. Mechanical partial occlusion of the inlet of the third space compartment is needed to simulate fluid shift. The capacity of the three reservoirs simulates the blood volume of a patient up to 100 kg.
The construction of the RPSS I is completed. It was tested and functioned as expected in mimicking the Frank-Starling law of the heart. Diuresis, fluid shifts, heat exchange, circulatory arrest and many other clinical scenarios can be achieved with this simulator (Table 1). Realism and automated responses makes the RPSS I fluid dynamic model potentially a great training and testing tool. The RPSS I costs less than U.S. $1,000 dollars or approximately 700 Euros. It is cost effective and will provide high quality simulation for perfusion training and education.
A list of possible simulated scenarios with RPSS I
RPSS II
The evolution of the next generation simulator, RPSS II, which has not been built yet, will have additional automated responses as the goal. Integration of the RPSS I into the RPSS II will be tested in the near future. The RPSS II will use blood or a blood analog. It will simulate responses such as blood gases, oncotic changes from hemodilution, air emboli and diuresis. The RPSS II will “react” to many of the changing parameters during cardiopulmonary bypass as a real patient would.
Footnotes
*.
This innovative “Bioskill Center” is the only surgical training of its kind between Boston and Washington, DC in the U.S. The North Shore University Hospital – LIJ School of Cardiovascular Perfusion is part of the North Shore – LIJ Health System which developed cardiac simulation labs that included clinical perfusion simulation. The five million dollars spent to date demonstrates a major commitment of this institution and general trend of the healthcare system towards medical education simulation.