
Abstract
Perfusion quality during cardiopulmonary bypass (CPB) procedures can contribute to postoperative neurological complications and influence patient recovery and outcome. Gaseous microemboli generated in the circuit and hemodynamic properties of blood reaching the patient can be monitored during CPB to optimize perfusion. Oxygenators that oxygenate the blood during CPB can significantly influence the quality of blood reaching the patient by their manufacturing designs. New hollow-fiber membrane oxygenators are developed with integrated arterial filters to reduce priming volume and eliminate a separate arterial filter in the circuit. To evaluate the performance of these new oxygenators, we used a simulated model to compare the Quadrox-i Neonatal and the Capiox Baby FX05 neonatal oxygenators and to provide a review of these oxygenators with their respective counterparts which have separate arterial filters. We found that microemboli counts for the new Quadrox-i and Capiox FX05 oxygenators are similar in the arterial line, but different across the oxygenator for all experimental conditions. The arterial purge line diverting blood from the patient reduces microemboli count for the Capiox FX05, but is inconsistent for the Quadrox-i Neonatal. While hemodynamic energy delivered to the patient is similar for both oxygenators, shunted blood flow for the Quadrox-i Neonatal oxygenator is three times higher than the Capiox FX05 (103.6 mL/min vs 33.0 mL/min at 400 mL/min and 35°C) (p<0.001).
Keywords
Introduction
The cardiopulmonary bypass (CPB) procedure is a vital component in the repair of many congenital heart defects, but can cause morbidity and mortality through hypoperfusion or postoperative neurological complications. One of the underestimated factors of hypoperfusion is an open purge line on the arterial filter during the procedure 1 . A purge line is typically used during a CPB procedure to assist in the removal of gaseous microemboli from the closed circuit. However, it diverts oxygenated blood from reaching the patient, back into the cardiotomy reservoir. Depending on the circuit pressure, up to 80% of the pump flow may be diverted 1 . Shunted blood flow through the purge line is particularly important for neonates and infants during CPB due to the lower flow rate and higher risk of hypoperfusion of the vital organs 1 .
Gaseous microemboli formed in the closed circuit during CPB may cause postoperative brain injury and complications through blood vessel occlusion and neurological damage 2 . To monitor the amount of microemboli generated during CPB, transcranial Doppler (TCD) ultrasound is used to detect microemboli larger than 40µm in the middle cerebral artery of the patient 3 , and emboli detection and classification (EDAC) is used to detect microemboli larger than 10µm and classify them by size in the circuit4,5. Oxygenators, cardiotomy reservoirs and arterial filters in the circuit are designed with membrane filters to trap microemboli by size in order to reduce the amount of microemboli reaching the patient.
In order to reduce the priming volume and eliminate a separate arterial filter in the circuit, manufacturers recently developed new hollow-fiber membrane oxygenators with integrated arterial filters. We have previously evaluated the Quadrox-i neonatal oxygenator (Maquet, Hirrlingen, Germany) and the Capiox Baby FX05 without a venous reservoir (Terumo Corporation, Tokyo, Japan) separately6,7, but we are interested in comparing the effectiveness of these neonatal oxygenators in the flow range of neonatal patients in terms of reducing microemboli load delivered to the simulated patient and the hemodynamic properties of each oxygenator. We would also like to compare the performance of integrated versus non-integrated arterial filter oxygenators.
Materials and Methods
CPB circuit design
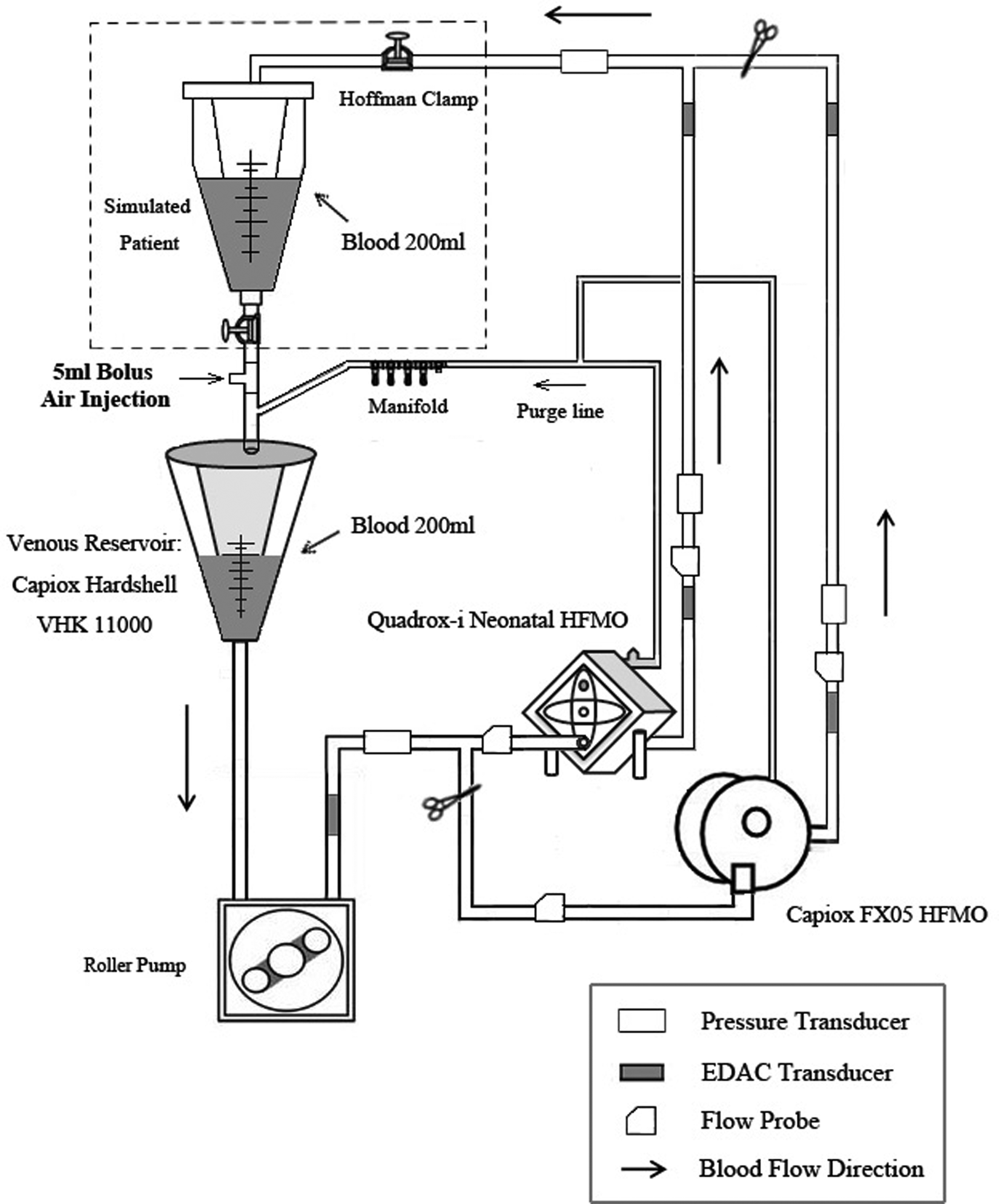
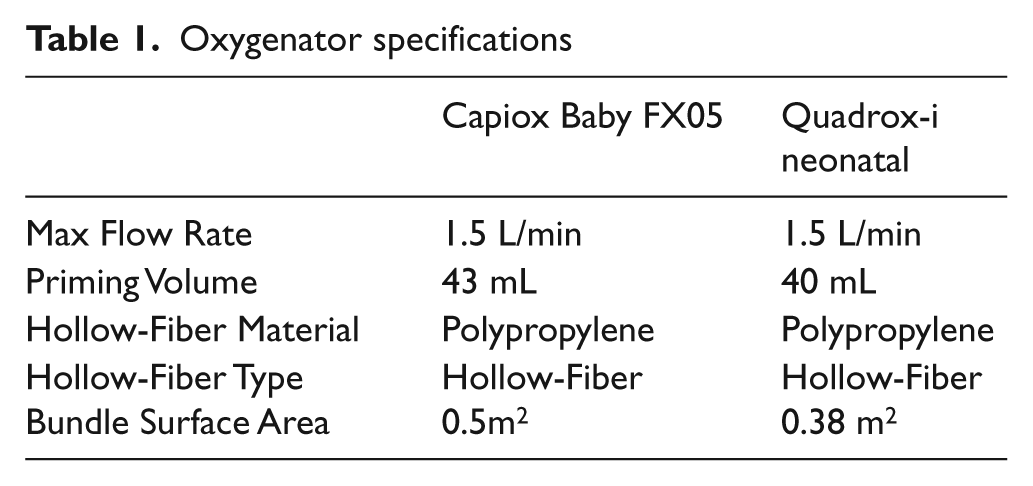
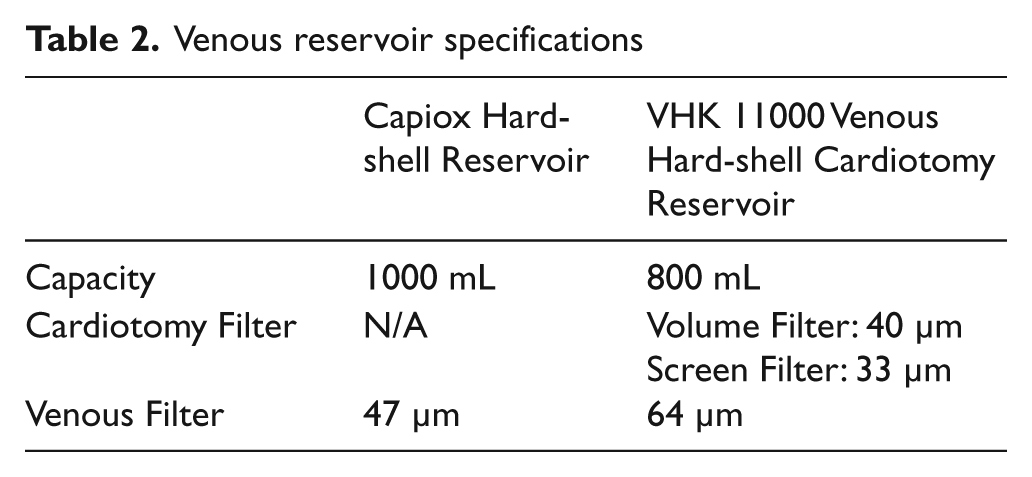
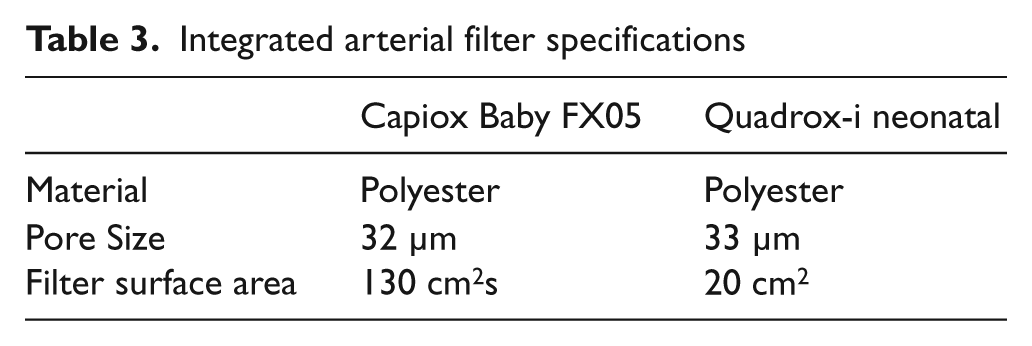
The circuit used for our experiments was arranged to identically model a clinical neonatal CPB circuit (Figure 1). The circuit included an HL-20 heart-lung machine (Maquet, Hirrlingen, Germany), a Jostra-30 heat-cooler system (Maquet, Hirrlingen, Germany), a Capiox CR10 hard-shell reservoir (Terumo Corporation, Tokyo, Japan) serving as the pseudo-patient, 6 feet of ¼ inch venous tubing, 5 feet of ¼ inch arterial tubing, a purge line, an oxygenator with an integrated arterial filter, and a venous hard-shell cardiotomy reservoir. The two different hollow-fiber membrane oxygenators with integrated arterial filters used in this experiment included the Quadrox-i Neonatal (Maquet) and the Capiox Baby FX 05 (Terumo Corporation). Each oxygenator was used with its specific venous reservoir. The specifications for the oxygenators, venous reservoirs, and integrated arterial filters can be seen in Tables 1, 2, and 3, respectively. Although most of the characteristics are very similar between the two oxygenators, the surface areas of the integrated arterial filters are quite different. The Capiox FX has a 6.5-fold greater surface area compared to the Quadrox-i (130 cm2 vs. 20 cm2). In addition, the venous reservoir filters with the Capiox FX and the Quadrox-i were also significantly different ( 47 μm vs 64 μm, respectively). The purge line of the Quadrox-i Neonatal was composed of 48-inch long tubing (1/8-1/32 inch) without a one way valve, but with a COBE 5-port manifold (Sorin Infant Perfusion Pack, Sorin Cardiovascular Inc., Arvada, CO) connecting the oxygenator via the pre-filter de-airing port to the venous reservoir whereas the Capiox FX05 purge line (two 24-inch long tubing) was assembled so that a stopcock connected our tubing to the purge line (1/8-1/32 inch) of the oxygenator with a one-way valve and a COBE 5-port manifold. The purge line was directly connected to the post-filter de-airing port of the oxygenator and the venous reservoir.
Experimental Circuit Design.
Oxygenator specifications
Venous reservoir specifications
Integrated arterial filter specifications
Both dual-channel Transonic ultrasound flow probes, model 6XL (Transonic Systems, Inc., Ithaca, NY, USA) and Maxxim disposable pressure transducers, model 041500503A (Maxxim Medical, Inc., Ithaca, NY, USA), were placed upstream and downstream of the oxygenator with an integrated arterial filter. An additional pressure transducer and a Hoffman clamp were placed on the arterial line to monitor and maintain a constant arterial pressure, respectively. A Hoffman clamp was also placed on the venous line distal to the pseudo-patient. The pressure transducer and flowmeter outputs were linked to a custom-made data acquisition device (NI USB-6521, National Instruments, Austin, TX) and then connected to a computer via a universal serial bus (USB) port. A custom-user interface based on Labview 7.1 software with a sampling rate of 1000 samples/sec was used to gather data two minutes post-injection of a five milliliter bolus of air.
The EDAC quantification system (Luna Innovations Inc., Roanoke, VA) was used to collect data regarding the volume, size, and number of the microemboli. Three transducers were connected to the circuit at three positions; pre-oxygenator, post-oxygenator, and post-arterial filter just proximal to the Hoffman clamp. Ultrasound-coupling gel was used to insure connection integrity. Data was collected for 5 minutes after each injection of air so that EDAC could return to baseline and the emboli could be cleared. The EDAC system was connected to a Windows PC via a USB for data analysis. According to the manufacturer specifications, the EDAC system is capable of counting emboli at rates up to 1,000 emboli per second, with diameters of 10 microns and greater, and at flow rates between 200 ml/min and 6 L/min 8 .
Experimental design
Following priming of the circuit with lactated Ringer’s solution, heparinized human blood was added to the circuit as some Ringer’s lactate was removed. We intentionally used human blood with our clinical circuit in this study. The main advantage is it mimics the clinical scenario as close as possible because these oxygenators will be used in patients. The target hematocrit was 30%. The total volume of the circuit during the experiments was 700 ml, with both the pseudo-patient and the venous reservoir volume kept at 200 ml. Five milliliters of bolus air were injected during a 30 second interval at a site just proximal to the venous reservoir at flow rates of 400 ml/min and 700 ml/min. The injections were done at each flow rate at normothermic (35°C) and hypothermic (25°C) conditions, with both an open and a closed arterial purge line. Six injections were completed for each oxygenator at each experimental condition for a total of 64 experiments per oxygenator (128 total injections).
Statistical analysis
A linear mixed-effects model was fit to the continuous outcomes (e.g., total emboli count) to compare the oxygenators (Quadrox-I Neonatal and FX05) and purge line status (open and closed) at a given location (pre- or post-oxygenator or arterial line), flow rate (400 and 750 ml/min), and temperature (25 and 35 degrees). The linear mixed-effects model is an extension of linear regression that accounts for the within-subject variability inherent in repeated measures designs 9 . In this study, the repeated factor is the location. For each outcome, p-values were adjusted for multiple comparisons testing, using the Tukey-Kramer procedure. All hypotheses tests were two-sided and all analyses were performed using version 9.2 of the SAS System for Windows (SAS Institute Inc., Cary, NC).
Results
Gaseous microemboli
For both oxygenators, the amount of microemboli increases as the flow rate increases at both temperatures (Tables 4 and 5). Purge line status also shows differing trends between the two oxygenators. Both the Capiox FX05 and the Quadrox-i show almost 100% elimination of post-oxygenator and arterial line microemboli at 400 mL/min, regardless of temperature and purge line status, even with the presence of pre-oxygenator emboli. At 700 mL/min and 35°C, the Capiox FX delivers less emboli to the simulated neonatal patient while the Quadrox-i delivers significantly more emboli with the purge line closed than opened (p<0.001). At 700 mL/min and 25°C, the FX05 delivered more microemboli than the Quadrox-i with a closed purge line while, with an open purge line, the Quadrox-i delivered more microemboli (p<0.001). In addition, pre- and post-oxygenator microemboli count for the Quadrox-i is almost five times higher with the purge line open than closed (p<0.001). However, the amount of microemboli is significantly reduced in the distal arterial line for both oxygenators. In fact, the microemboli loads in the distal arterial line are very similar for both oxygenators, which does not show significant changes with purge line status at this condition.
Microemboli counts (Mean ± SD) of integrated arterial filter oxygenators at 35°C
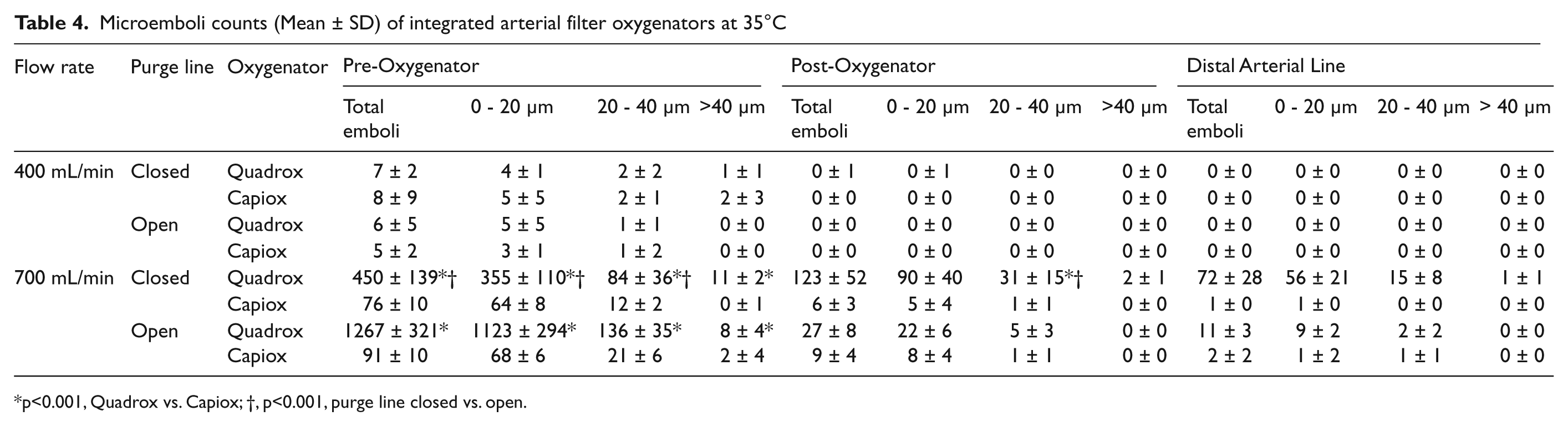
p<0.001, Quadrox vs. Capiox; †, p<0.001, purge line closed vs. open.
Microemboli counts (Mean ± SD) of integrated arterial filter oxygenators at 25°C
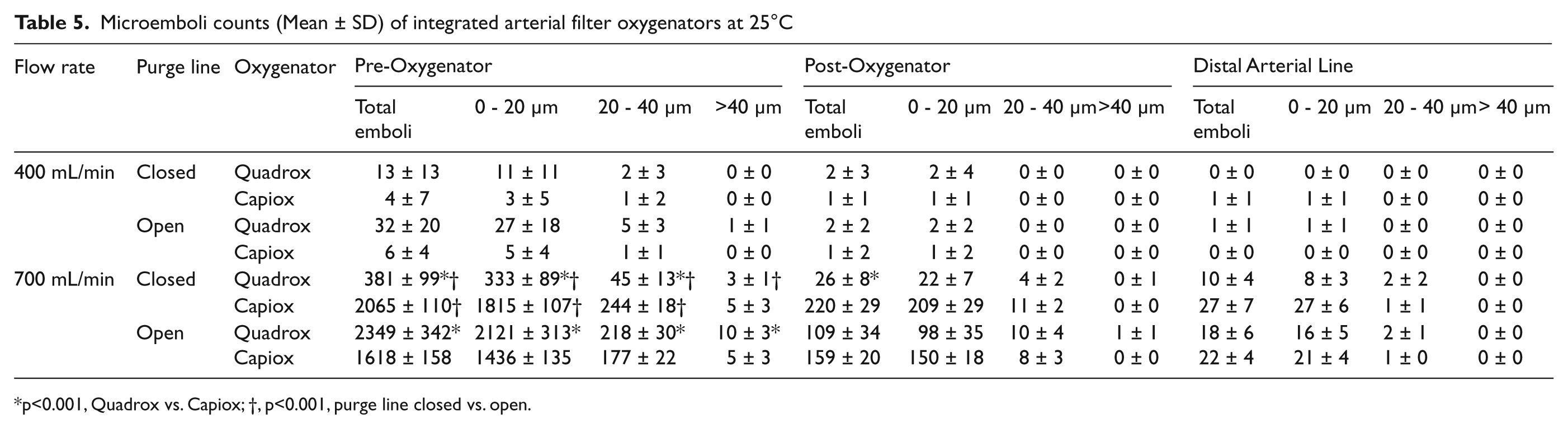
p<0.001, Quadrox vs. Capiox; †, p<0.001, purge line closed vs. open.
Pressure drop and hemodynamic energy
Mean pressure drop across the oxygenator is independent of purge line status (Figure 2). At both temperatures, the mean pressure drop increases with higher flow rates. The Quadrox-i shows a slightly lower mean pressure drop than the Capiox FX05 at both temperatures and flow rates (p<0.001).
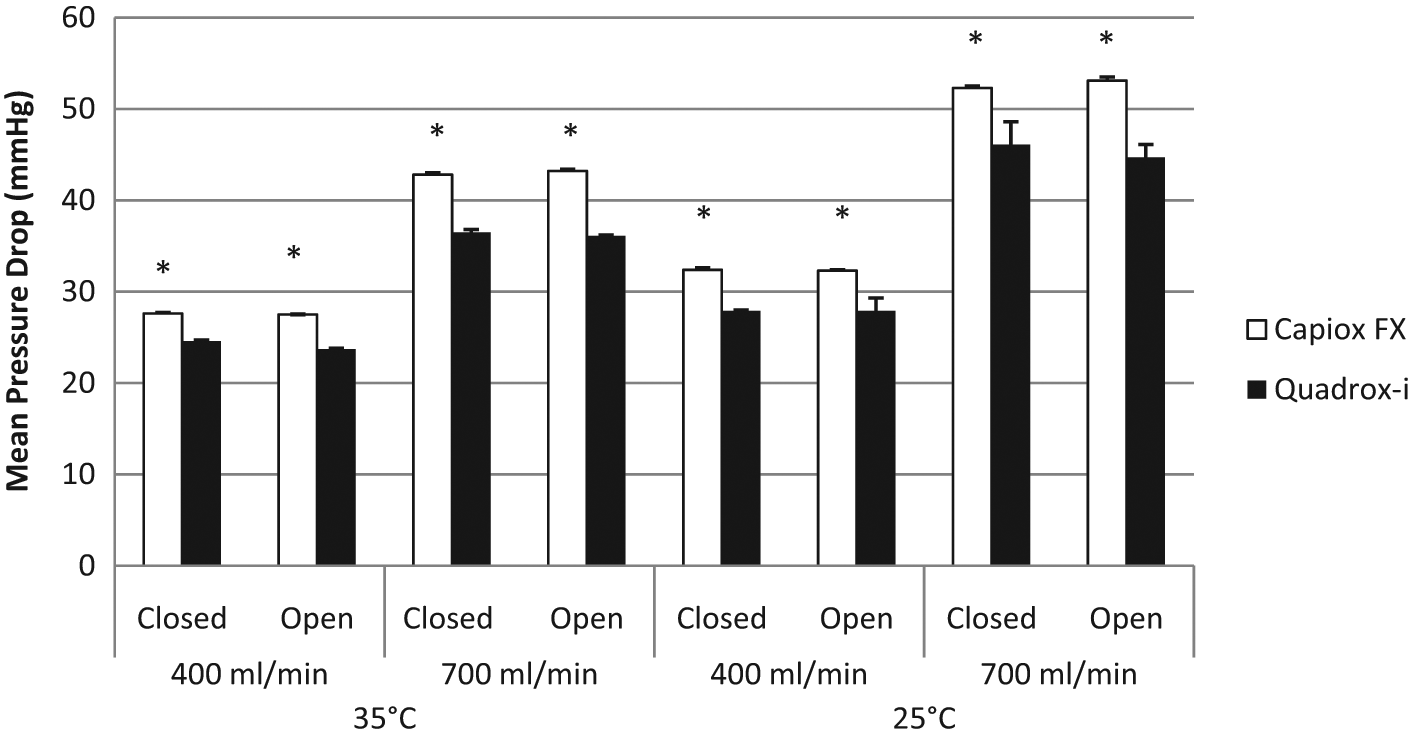
Mean Pressure drops (mmHg) across the oxygenators. (* p<0.001, Quadrox vs. Capiox)
Total hemodynamic energy (THE) also decreases across the oxygenator (Table 6). Pre-oxygenator THEs are higher at higher flow rates and lower temperatures. The Capiox FX05 has a slightly higher pre-oxygenator THE than the Quadrox-i with higher flow rates and lower temperatures (p<0.001). However, the post-oxygenator THEs are similar for both oxygenators across all experimental conditions.
Pressures and hemodynamic energies of integrated arterial filter oxygenators
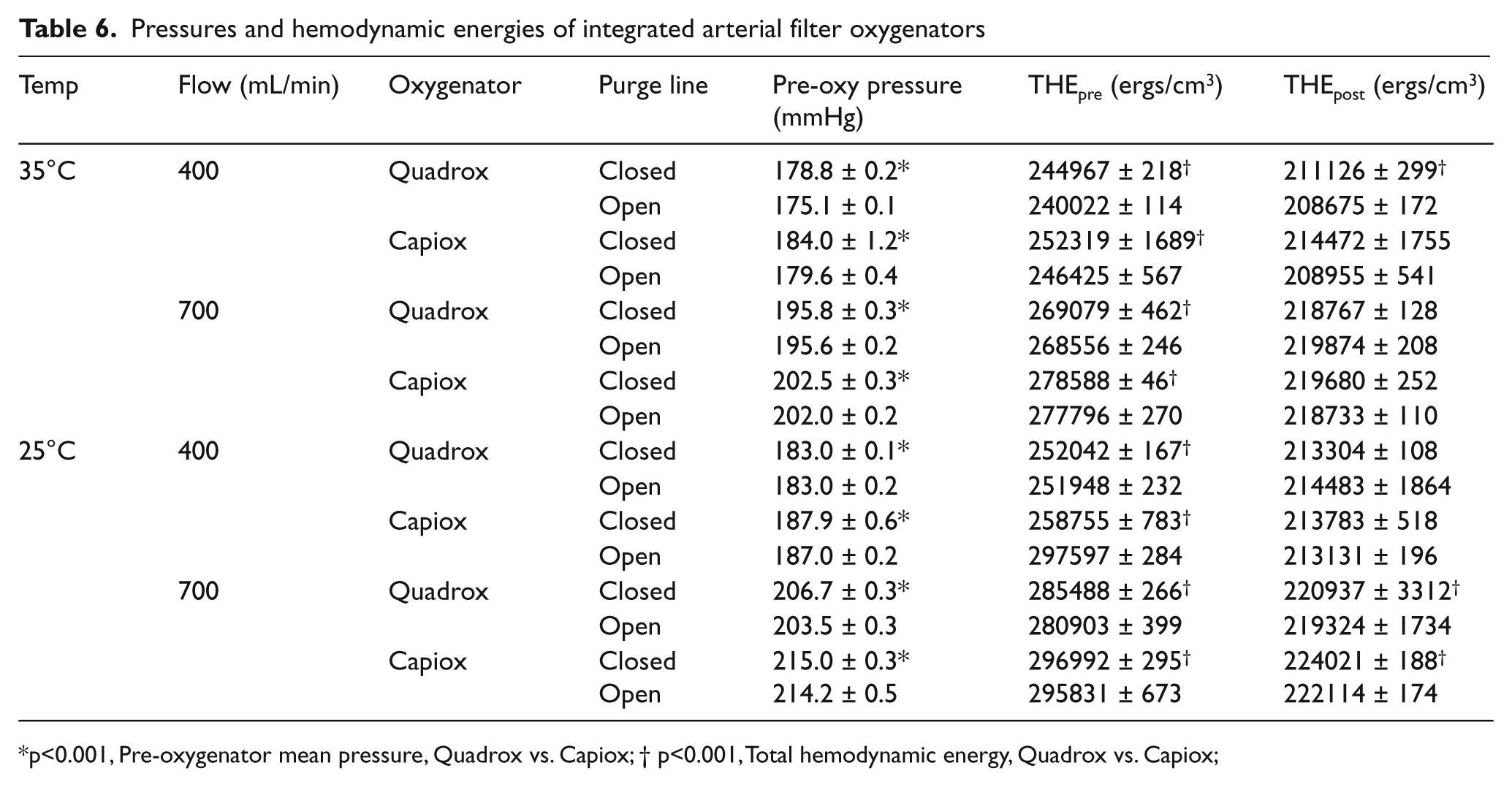
p<0.001, Pre-oxygenator mean pressure, Quadrox vs. Capiox; † p<0.001, Total hemodynamic energy, Quadrox vs. Capiox;
“Stolen” blood flow
Blood flow shunted via the purge line is almost three times higher for the Quadrox-i Neonatal than the Capiox FX05 at both temperatures and flow rates (Figure 3) (p<0.001). At 25°C, the blood flow diverted is slightly decreased for both oxygenators.
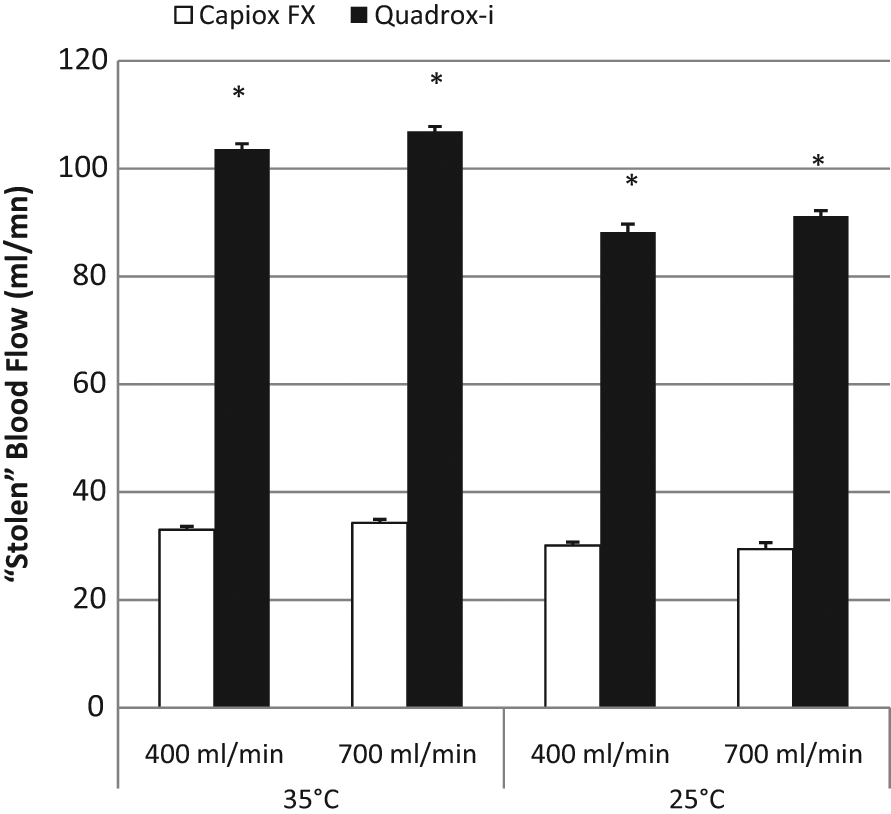
“Stolen” blood flow (ml/min) when the purge line is opened. (* p<0.001, Quadrox vs. Capiox)
Discussion
Oxygenators with integrated arterial filter
Microemboli load and hemodynamic properties are important for evaluating the effectiveness of the oxygenators, reservoirs and filters in reducing postoperative complications from cardiopulmonary bypass procedures. As predicted, total microemboli increases with higher flow rates because the high flow rate and circuit pressure can prevent effective trapping of microemboli across the filters. Lowering the temperature results in increased blood viscosity and microemboli count. Opening the purge line reduces blood flow to the patient by returning blood from the arterial line to the venous reservoir, thereby, filtering the blood a second time before it reaches the patient. However, shunting the blood also results in reduced hemodynamic energy and perfusion of the patient, which can significantly affect patient recovery after cardiopulmonary bypass procedures. This is especially true for neonates and infants, since blood flow during CPB is typically lower for these patients.
The Quadrox-i and the Capiox FX05 produced similar results for arterial microemboli count at 700 mL/min and 35°C, where total microemboli for the Quadrox-i is higher than the Capiox FX05. The Quadrox-i generally shows more total pre- and post-oxygenator microemboli than the Capiox FX05. However, the Quadrox-i has a slightly lower microemboli count than the Capiox FX05 when the purge line is closed at 700 mL/min and 25°C. The Capiox FX shows a decrease in microemboli when the purge line is opened except at 700 ml/min and 35°C, whereas the Quadrox-i shows the opposite. This is consistent with our previous experiment using the Quadrox-i with a separate arterial filter 10 .
The pressure drop across the oxygenators is a function of the hollow-fiber configuration of each specific oxygenator. At all flow rates and temperatures, the Capiox FX05 has a slightly higher mean pressure drop than does the Quadrox-i. A higher pressure drop across the membrane oxygenators increases the resistance and retains more microemboli. At the same time, blood is pushed at a higher pressure across the membrane, which may also increase the stress injury to the blood cells, activate the inflammatory response, increase cellular damage and affect patient recovery after surgery 11 . Therefore, a high pressure drop could affect the quality of perfusion and could imply a greater loss in total hemodynamic energy (THE) delivered to the patient. THE is defined as a function of pump flow rate and arterial pressure 12 , which was kept constant, so it is not surprising that pre-oxygenator THE shows more differences between the two oxygenators. The THE delivered to the patient (post-oxygenator THE) is comparable between the Capiox FX05 and the Quadrox-i (Table 6).
When the purge line is open, blood flow is diverted from the arterial filter to the cardiotomy reservoir and the amount of blood diverted is dependent, mostly, on the circuit pressure, with a higher circuit pressure leading to more diverted blood flow to the purge line 1 . The diverted blood flow also varies with temperature and flow rate 1 . At lower temperatures, diverted blood flow increases with increasing blood viscosity. Higher flow rates also increase blood flow through the purge line. We calculated shunted blood flow by taking the differences between post-oxygenator flow when the purge line is opened and when it is closed. When comparing the two oxygenators, we found that “stolen” blood flow is three times higher for the Quadrox-i than for the Capiox FX05 at all flow rates and temperatures. Although the length of purge line is identical in both circuits, the oxygenator and purge line design may play a major role in the amount of diverted blood flow. The Capiox FX05 purge line includes a one-way valve and the Quadrox-i does not. It is possible that the one-way valve increased the pressure in the Capiox FX05 purge line and allowed less blood to be diverted. The decrease in purge line blood flow decreases the amount of oxygenated blood diverted from the patient, which will, therefore, lower the risk of hypoperfusion.
In a previous experiment done in 2010, the “stolen” blood flow of the Quadrox-i with integrated arterial filter was found to be significantly lower than our current 2011 study 6 . In the 2010 experiment, using the Quadrox-i lot# 70229597, “stolen” blood flow at 35°C was 20.5 mL/min for a pump flow rate of 500 mL/min and 22.8 mL/min for a pump flow rate of 750 mL/min. In the current 2011 experiment, using lot# 70051992, “stolen” blood flow is almost five times higher, at 103.6 mL/min for a pump flow of 400 mL/min and 106.9 mL/min for 700 mL/min. The same pattern is observed at 25°C, as shown in Figure 4, with shunted blood flow as a percentage of pump flow rate. To confirm this finding, we kept our same setup, but replaced the oxygenator we used for this trial (lot# 70051992) with the one we used in the 2010 experiment (lot# 70229597) and the “stolen” blood flow was still much lower with the oxygenator from the 2010 trial (Figure 4). We then repeated our experiment with a third Quadrox-i oxygenator (lot# 70051992) and came up with the same results as the results presented in this manuscript. We attribute the differences in “stolen” blood flow to a change in the Quadrox-i neonatal oxygenator design since our last trial in 2010 6 .
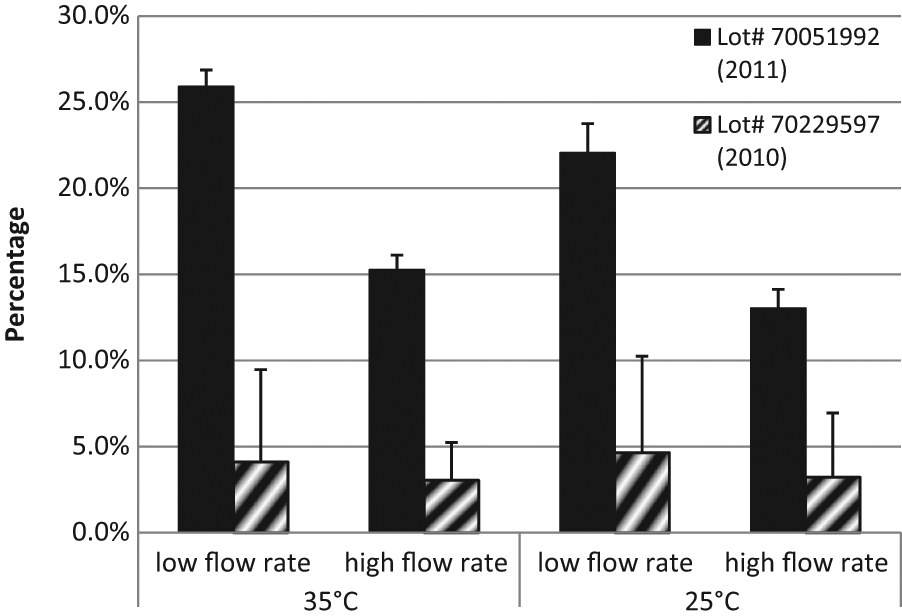
“Stolen” blood flow as a percentage of pump flow for 2011 and 2010 Quadrox-i oxygenators with integrated arterial filters at low flow rates (400-500 mL/min) and high flow rates (700-750 mL/min).
Integrated vs. separate arterial filter
The results of this experiment using oxygenators with integrated arterial filters are compared to results from a previous experiment using the same oxygenators, but with separate arterial filters 10 . Integrated arterial filter designs are found to be either equally effective or better than separate arterial filters in reducing total emboli delivered to the simulated patient, even though the post-filter flow rate is lower. One exception is the Quadrox-i at 700 mL/min and 35°C, which does not follow trends predicted from either experiment. (Table 7)
Comparison of different oxygenators in microemboli count at 700 ml/min, 35°C
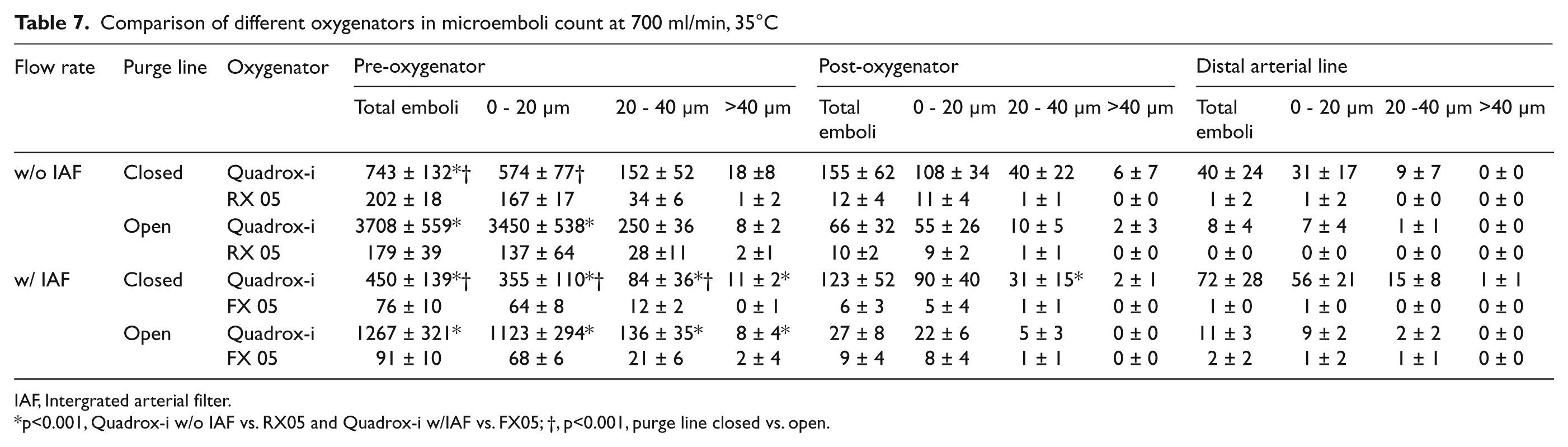
IAF, Intergrated arterial filter.
p<0.001, Quadrox-i w/o IAF vs. RX05 and Quadrox-i w/IAF vs. FX05; †, p<0.001, purge line closed vs. open.
“Stolen” blood flow for the new Quadrox-i oxygenator (Lot# 70051992) shows no apparent differences between integrated and non-integrated arterial filters. However, a three-fold decrease in shunted blood flow is observed for the Capiox FX05 compared to the RX05. While microemboli count for the Capiox FX05 and RX05 remain very similar, especially in the arterial line, the large decrease in the FX05 diverted blood flow allows better perfusion of the patient. In addition, the Capiox FX05 is the only oxygenator that produces a low diverted blood flow, distinguishing it, not only from the Capiox RX05, but also from the Quadrox-i for all experimental conditions. However, if ultrafiltration is performed from the purge line, a low “stolen” blood flow may not be ideal. If the purge line is opened throughout CPB, a low shunted blood flow may be more desirable to minimize the risk of hypoperfusion. If the purge line is opened only when necessary for purposes such as ultrafiltration, a higher shunted blood flow may be more efficient. Therefore, stolen blood flow from opening the purge line is an important factor to be considered during CPB, depending on clinical conditions.
Pressure drop increases at higher flow rates, but is relatively independent of temperature. For the Quadrox-i, we found that the integrated arterial filter gives a higher pressure drop and THE than the non-integrated arterial filter. Interestingly, the Capiox FX05 gives a slightly lower THE, but similar pressure drop to the Capiox RX05. However, the absolute values of THE differences are minimal. Therefore, other parameters should also be considered when selecting an oxygenator.
Conclusions
Both Capiox FX05 and Quadrox-i Neonatal oxygenators with integrated arterial filters are almost 100% effective in eliminating arterial microemboli at low flow rates, independent of temperature. At high flow rates, the Capiox FX05 is preferred at a normothermic temperature for delivering essentially zero arterial microemboli, but, at a hypothermic temperature, both oxygenators perform similarly. In this experiment, we also found that the Capiox FX05 gives a three-fold decrease in “stolen” blood flow over the Quadrox-i Neonatal. We strongly suggest that a flow probe after the arterial filter be placed in a clinical setting for accurate measurements of “real” blood flow to the patient.
Footnotes
Acknowledgements
Presented, in part, at the 2nd International Pediatric Perfusion Symposium, Dubai, United Arab Emirates, October 23-25, 2011 and at the Third Istanbul Symposiums on Neonatal/Pediatric Cardiopulmonary Bypass Procedures, American Hospital, Istanbul, Turkey, December 17, 2011.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
None declared.