
Abstract
Background:
Red blood cell (RBC) transfusion is used in the critically ill with low hemoglobin concentrations to optimize oxygen utilization and delivery imbalance. Data suggest that RBC transfusion is also independently associated with significant morbidity. We seek to characterize RBC transfusion volumes among patients receiving extracorporeal membrane oxygenation (ECMO) support and test the hypothesis that red blood cell transfusion volume is an independent risk factor for mortality.
Methods:
Records of all patients receiving ECMO support from 2001 through 2010 at a university-affiliated children’s hospital were retrospectively reviewed.
Results:
Among 484 ECMO runs reviewed, indications for ECMO were classified as cardiac (40%), non-cardiac (42%) or institution of ECMO during cardiopulmonary resuscitation (CPR) (18%). Median duration of ECMO support was 4.6 days, with overall survival to hospital discharge significantly higher among non-cardiac patients (60%) relative to patients supported for cardiac (37%) or external CPR (ECPR) indications (34%, p<0.001). Median RBC transfusion volumes with respect to ECMO indication were significantly greater among cardiac (105 mL/kg/day ECMO) and ECPR patients (66 mL/kg/day ECMO) relative to patients supported for non-cardiac indications (20 mL/kg/day ECMO, p<0.001). Among patients supported with ECMO for non-cardiac indications alone (n=203), independent of covariates, including weight, venoarterial mode of ECMO support, presence of congenital diaphragmatic hernia and complications, including hemorrhage, neurologic injury, and renal insufficiency, each RBC transfusion volume of 10 mL/kg/day ECMO was associated with a 24% increase in the odds of in-hospital mortality (OR 1.024, 95% CI 1.004-1.046, p=0.018).
Conclusions:
Greater red blood cell transfusion volumes among patients supported with ECMO for non-cardiac indications are independently associated with an increase in odds of mortality. A prospective investigation of restrictive RBC transfusion practices while receiving ECMO may be warranted in this population.
Keywords
Introduction
Red blood cell (RBC) transfusion is often used in the critically ill child in an attempt to improve an imbalance between oxygen utilization and delivery. 1 Established risks associated with RBC transfusion include acute lung injury, transmission of blood-borne infection and intravascular volume overload.2–4 Recent evidence has also demonstrated transfusion-associated increases in morbidity among critically ill children, including central-line-associated bloodstream infections, prolonged duration of mechanical ventilation and prolonged duration of hospitalization.5–7
Mechanical support in the form of extracorporeal membrane oxygenation (ECMO) represents an alternative modality of improving oxygen delivery in patients with cardiorespiratory or isolated respiratory failure. The use of ECMO is also associated with coagulopathy related to platelet dysfunction and consumption of thrombostatic factors.8,9 Hemorrhagic complications, including cannula and surgical site bleeding, are also relatively common among both pediatric and adult populations supported with ECMO.10,11 While alternative hemostatic strategies exist, including the use of antifibrinolytic agents or heparin-coated ECMO systems, attempts to follow current consensus guidelines for blood component therapy in ECMO patients may result in an increased transfusion volume among those with hemorrhagic sequelae.12 –17
As evidence continues to emerge supporting the association between increased red blood cell transfusion volumes and morbidity among the critically ill, we sought to characterize red blood cell utilization among a population of patients requiring extracorporeal membrane oxygenation. We hypothesized that, independent of established risk factors and accounting for covariates, including patient weight and duration of ECMO support, red blood cell transfusion was independently associated with an increase in hospital mortality.
Methods
The records of all patients receiving ECMO at Monroe Carell Jr. Children’s Hospital at Vanderbilt from January 2001 through December 2010 were retrospectively reviewed. The Vanderbilt University Institutional Review Board for Research on Human Subjects approved this study.
Demographics and outcomes
Patient demographic data collected included patient age at cannulation, weight at cannulation and gender. ECMO indication was classified as either cardiac, non-cardiac or ECPR, which is defined by the Extracorporeal Life Support Organization (ELSO) as “extracorporeal cardiopulmonary resuscitation in which extracorporeal life support was used as part of the initial resuscitation from cardiac arrest.” 18 The “cardiac” support classification included patients supported for postoperative low cardiac output syndrome, as well as patients with primary myocardial disease, including myocarditis and cardiomyopathy. Among non-cardiac indications, all congenital diaphragmatic hernia patients receiving ECMO support, both preoperatively and postoperatively, were included in our primary analysis. The mode of ECMO support was dichotomously characterized as either venoarterial (VA) or venovenous (VV). Patients converted from VA to VV were classified as VV support while patients converted from VV to VA were categorized as VA support. The total volume of packed red blood cells was noted and, in turn, normalized for both patient weight at time of cannulation and duration of ECMO support (mL/kg/day of ECMO support). Documented red blood cell volumes included priming volumes when applicable. Platelet administration was also noted and, again, normalized for both weight at the time of cannulation and duration of ECMO support (mL/kg/day of ECMO support). Fresh frozen plasma and cryoprecipitate were inconsistently available for analysis within the dataset over this same ten-year study period and were, thus, excluded from further analysis. Comorbidities, including renal insufficiency (creatinine >1.5 mg/dL), neurologic injury (evidence of infarct by head ultrasound or CT scan, new onset seizures apparent, either clinically or by EEG, or brain death), pulmonary hemorrhage, gastrointestinal hemorrhage, surgical bleeding and cannula site bleeding were all noted as is our institutional practice in preparing ELSO registry submissions. The definition of “bleeding” was coded at the discretion of the bedside ECMO specialist, characteristically referring to bleeding volumes prompting pharmacologic management (outside of anticoagulation regimen adjustment) or surgical intervention. As this cohort includes patients supported with ECMO over a decade, strategies to attain hemostasis varied over time and across providers and included administration of aminocaproic acid, aprotinin and activated Factor VII. Patient outcomes, including duration of ECMO support, hospital length of stay and survival to discharge, were also noted.
ECMO technique
The ECMO circuit consisted of a venous cannula that drained to a straight 6-inch silicone bladder through PVC tubing (Sorin, Milan, Italy). Blood was drawn from the bladder across S95 Tygon® raceway tubing (Saint-Gobain, Paris, France) inserted into a roller-head pump (Sorin Biomedical, Irvine, CA) and fed into a polymethylpentene hollow-fiber oxygenator system (Maquet, Hirrlingen, Germany). Oxygenators used from 2005 through 2007 included Minimax and Affinity polymethylpentene hollow-fiber oxygenators (Medtronic, Minneapolis, MN). Prior to 2005, silicone membrane oxygenators were used routinely. Blood then proceeded to an integrated water-bath heating system (Terumo Cardiovascular Systems, Ann Arbor, MI) within the oxygenator. Prior to 2005, blood heating was performed following the oxygenator, due to the lack of an integrated system. Blood then proceeded to the arterial inflow cannula and back to the patient. Heparin was administered at a concentration of 100 units/mL and dose-titrated to maintain an activated clotting time (ACT) of 180 to 220 seconds. In the setting of clinically significant hemorrhage, ACT goals were decreased to as low as 160 seconds at the discretion of the bedside provider. Flow rates of 100 to 200 mL/kg/min were maintained, depending on physiology, serum lactate levels and mixed venous oxygen saturation. Ventilator settings were titrated to maintain recruitment and to minimize barotrauma, routinely consisting of a rate of 10 breaths per minute, a positive end-expiratory pressure of 10 cm H20, ΔP of 10 cm H20,and 40% FiO2, with sweep gas flow used to adjust the CO2.
Blood product administration
Transfusion thresholds and product volumes administered were at the discretion of the intensivist for the duration of the observation period. Routinely, however, this included the transfusion of 10 to 15 mL/kg of leukoreduced packed red blood cells to maintain a goal hematocrit of 35% to 40%. This target was typically followed during the care of all ECMO patients, including those with cyanotic congenital heart disease. Platelets (either random-donor or single-donor apheresed at the discretion of the provider) were administered to target platelet counts greater than 80,000/µL. Cryoprecipitate (1 unit/10 kg) and fresh frozen plasma (10 to 15 mL/kg) were administered, targeting fibrinogen levels of at least 150 mg/dL and an international normalization ratio (INR) of less than 1.5, respectively.
All patients receiving mechanical support were administered sedation with benzodiazepines and analgesia with opioids, with neuromuscular blocking agents as indicated.
Statistical considerations
Continuous data are reported as median (25th and 75th percentiles) and categorical variables are reported as frequencies with percentages. Demographic and clinical data were compared using the Mann-Whitney U test for continuous variables and the χ 2 or Fisher’s exact test, where appropriate, for categorical variables. All-cause mortality comparisons were achieved with the use of multivariate logistic regression analysis, with survival to hospital discharge as a binary dependent variable. The number of covariates included within the model was limited to 1 covariate for every 10 events. 19 Among secondary analyses, in order to avoid model overfitting, all covariates with a univariate significance of p<0.2 were considered for inclusion within the multivariate model. Data from multivariate logistic regression analyses are reported as estimated odds ratios (OR) with 95% confidence intervals (CI). Data were analyzed with SPSS (v.18, SPSS Inc, Chicago, IL).
Results
From January 2001 through December 2010, 505 patients received ECMO support at our institution. Of these, records were incomplete in 21 patients (3%), allowing for analysis of 484 patients. The baseline demographic characteristics of the cohort are summarized in Table 1. Over half of the patients supported with ECMO in this cohort were neonates. All patients in this cohort supported with ECPR were patients with primary cardiac diagnoses. Among those patients with primary cardiac disease (n=285, 58%), the most common anatomic diagnoses included hypoplastic left heart syndrome (n=81), Tetralogy of Fallot (n=20), total anomalous pulmonary venous return (n=16) and truncus arteriosus (n=15). Among patients supported for non-cardiac indications, the most common diagnoses included congenital diaphragmatic hernia (n=57), meconium aspiration syndrome (n=21) and persistent pulmonary hypertension of the newborn (n=20).
Baseline demographic characteristics of ECMO cohort (n=484).
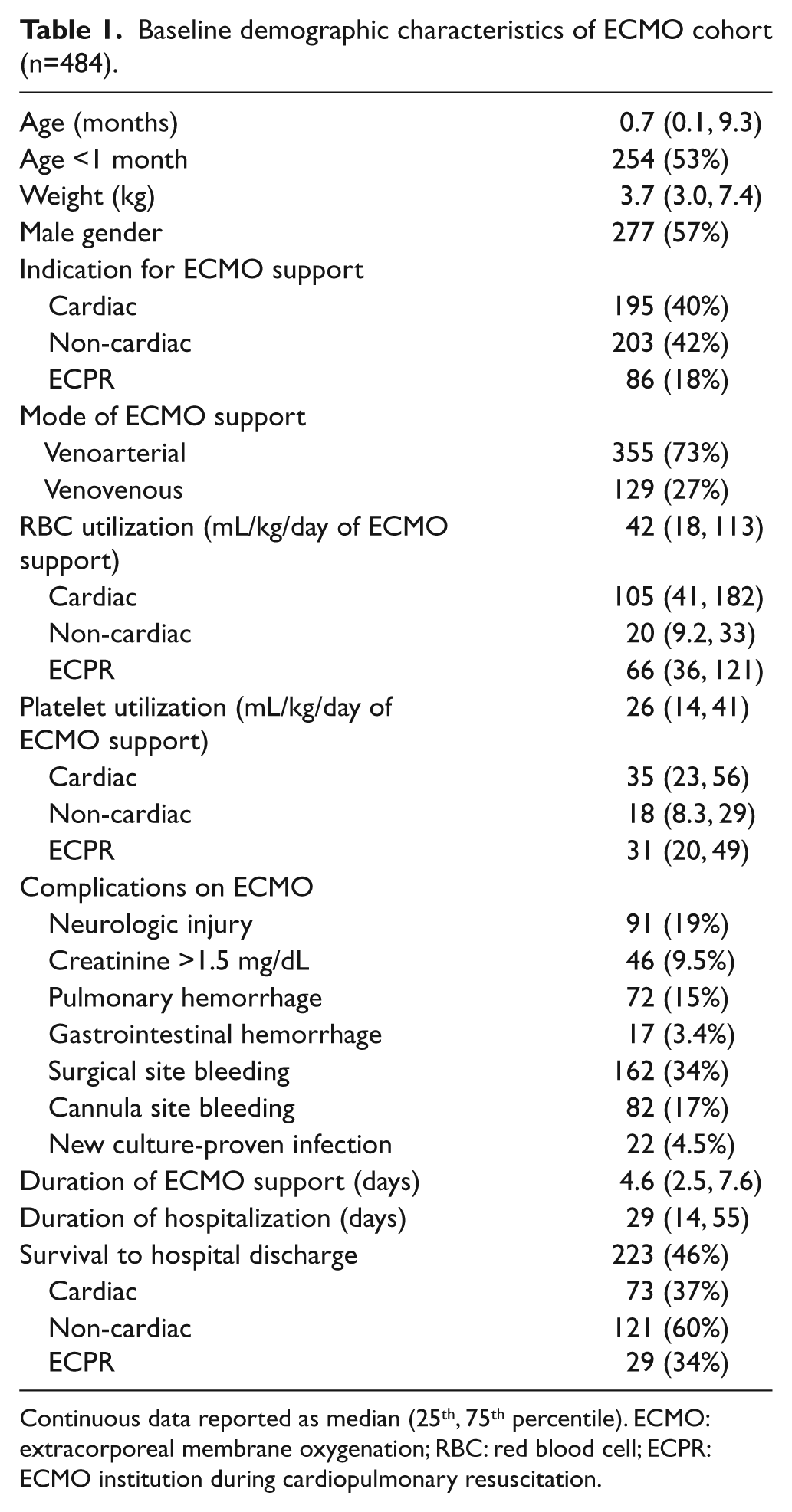
Continuous data reported as median (25th, 75th percentile). ECMO: extracorporeal membrane oxygenation; RBC: red blood cell; ECPR: ECMO institution during cardiopulmonary resuscitation.
Packed red blood cell utilization varied greatly with respect to ECMO support indication. Median RBC volumes among those supported secondary to cardiac (105 mL/kg/day of ECMO) or ECPR indications (66 mL/kg/day of ECMO) were significantly greater relative to those supported for non-cardiac indications (20 mL/kg/day of ECMO, p<0.001). Among those supported for non-cardiac indications, both RBC transfusion volumes (28.2 v. 16.6 mL/kg/day ECMO, p<0.001) and platelet transfusion volumes (24.6 v. 13.4 mL/kg/day ECMO) were significantly greater in those with primary ECMO indication of congenital diaphragmatic hernia.
Given notable differences in transfusion volumes between patients supported for cardiac and non-cardiac indications, as well as potential operative factors that remain unaccounted for among cardiac patients, an analysis of non-cardiac patients alone (n=203) was conducted. Data and univariate analyses with respect to all-cause hospital mortality among this cohort are summarized in Table 2. Patients failing to survive to hospital discharge following ECMO support were more frequently patients with congenital diaphragmatic hernia, as well as those supported with venoarterial ECMO. Complication rates, including neurologic injury, renal insufficiency and hemorrhagic complications, were all significantly greater among those who did not survive to hospital discharge. Red cell transfusion volumes among survivors were significantly lower than non-survivors (16.3 v. 27.1 mL/kg/day ECMO support, p<0.001).
Characteristics of patients receiving ECMO support for non-cardiac indications with respect to survival to hospital discharge (n=203).
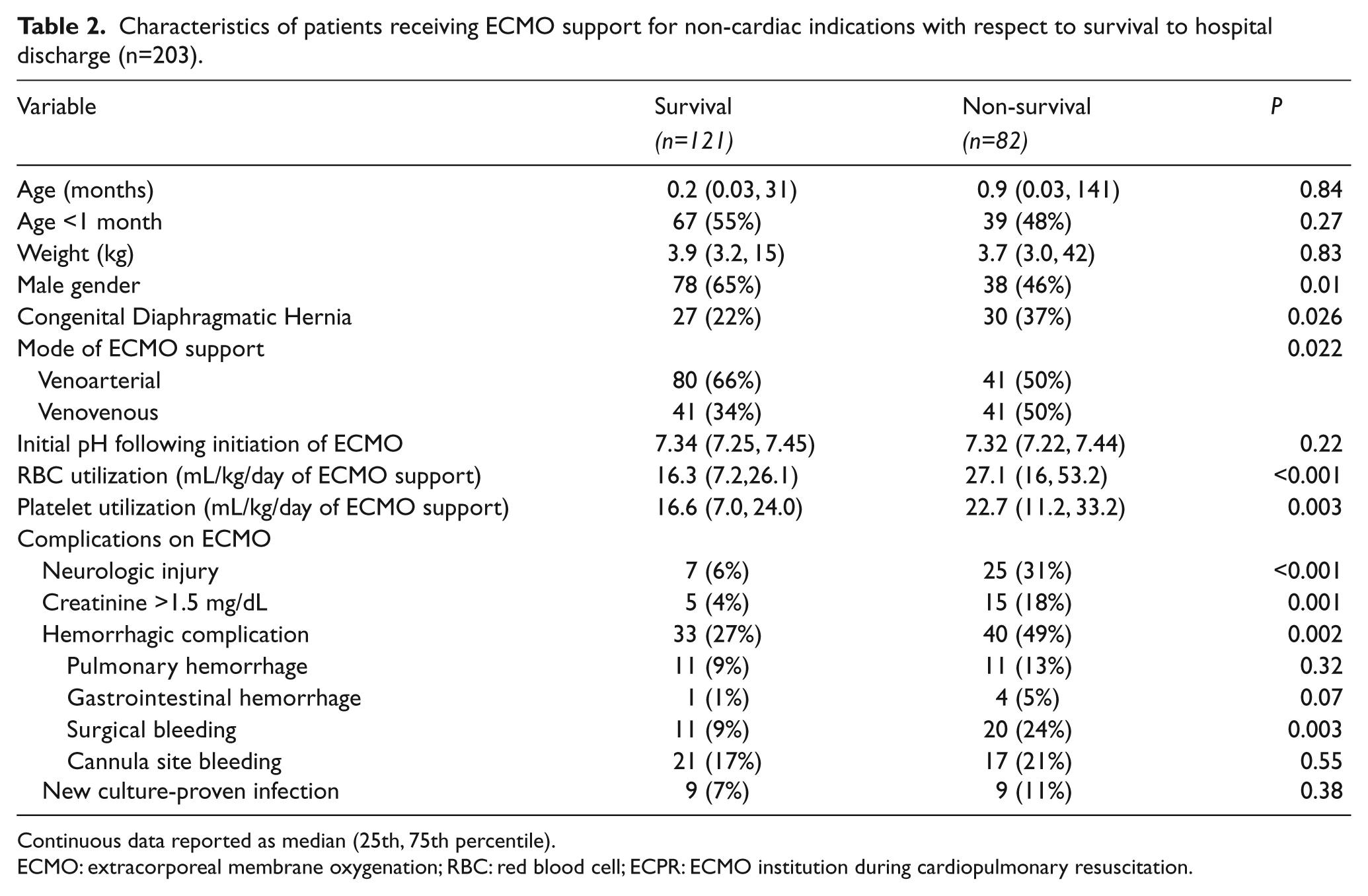
Continuous data reported as median (25th, 75th percentile). ECMO: extracorporeal membrane oxygenation; RBC: red blood cell; ECPR: ECMO institution during cardiopulmonary resuscitation.
A multivariate logistic regression analysis of all-cause mortality is detailed in Table 3. Independent of patient weight, gender, venoarterial mode of ECMO support, presence of congenital diaphragmatic hernia, platelet utilization and hemorrhagic complications, as well as complications including neurologic injury and creatinine > 1.5 mg/dL, RBC transfusion volumes remained an independent predictor of in-hospital mortality among patients supported with ECMO for non-cardiac indications. For every RBC transfusion volume of 10 mL/kg/day ECMO, there was a 24% increase in the odds of in-hospital mortality among patients supported with ECMO for non-cardiac indications. This model was subsequently utilized in demonstrating the predicted probability of in-hospital mortality with respect to RBC transfusion volumes and is detailed in Figure 1.
Multivariate logistic regression analysis of death among all patients supported with ECMO for non-cardiac indications. b
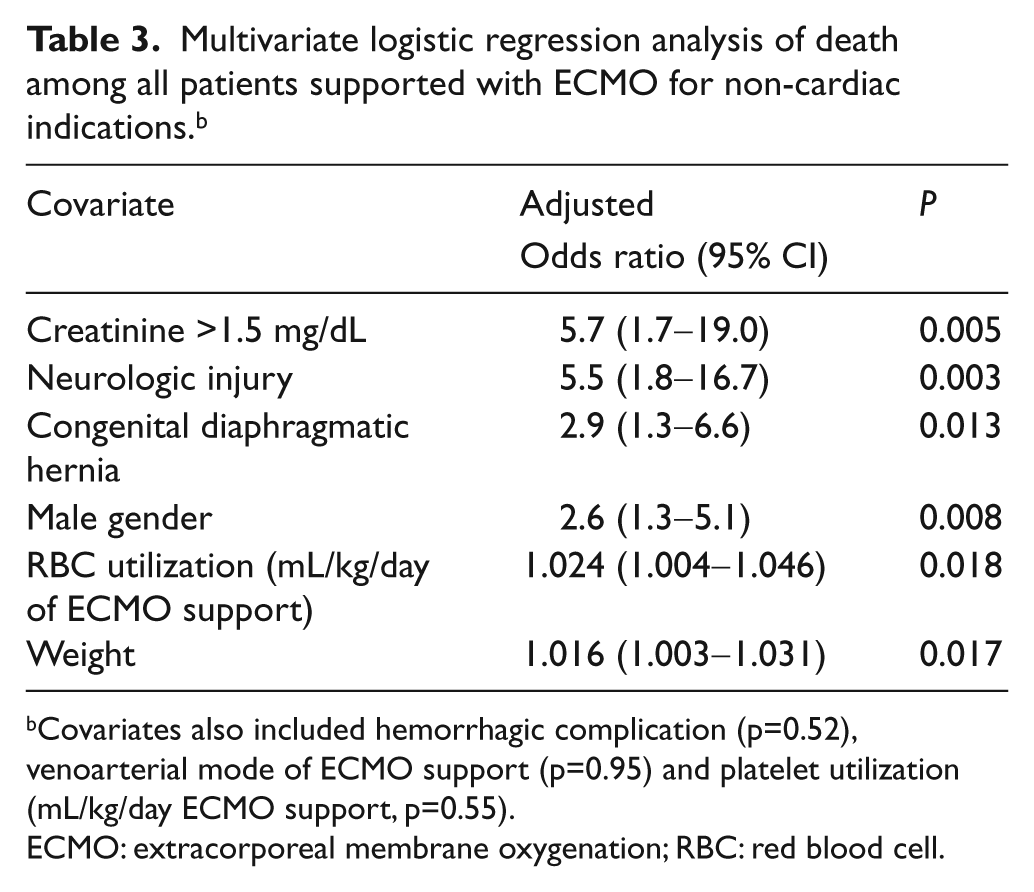
Covariates also included hemorrhagic complication (p=0.52), venoarterial mode of ECMO support (p=0.95) and platelet utilization (mL/kg/day ECMO support, p=0.55).
ECMO: extracorporeal membrane oxygenation; RBC: red blood cell.
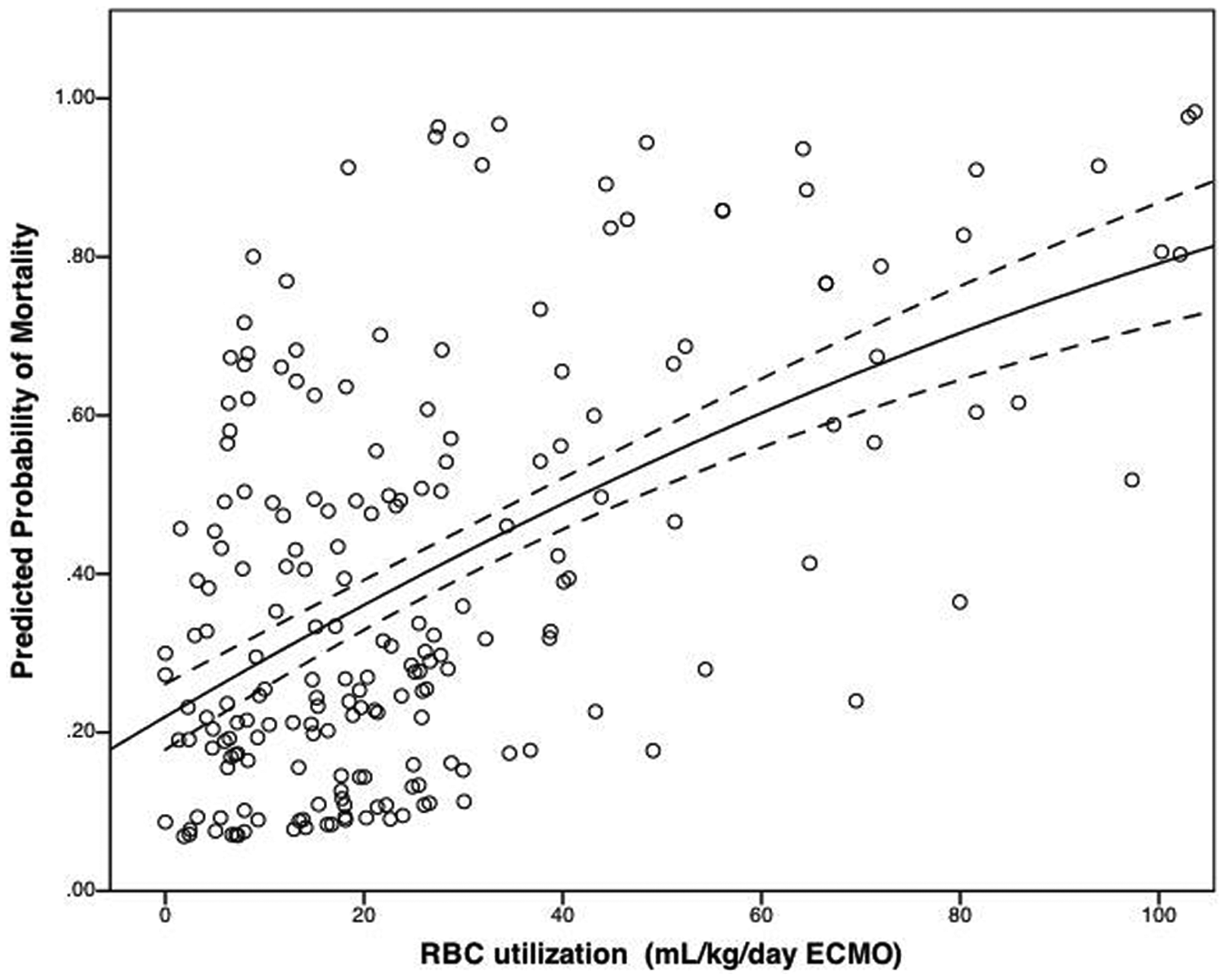
Predicted probability of mortality as a function of RBC transfusion volume during ECMO course. Quadratic polynomial line best of fit (R2=0.33) with 95% CI, adjusted for gender, weight, congenital diaphragmatic hernia, renal dysfunction, neurologic injury, hemorrhagic complications, venoarterial mode of ECMO support and platelet utilization.
Discussion
We report a retrospective, observational study of nearly 500 patients supported with ECMO over a ten-year period. We quantify red blood cell and platelet use among patients supported for cardiac and non-cardiac indications alike. Finally, we demonstrate here an independent increase in odds of mortality among patients receiving greater volumes of packed red blood cells among patients supported with ECMO for non-cardiac indications.
Over 14 million units of allogeneic red cells are transfused annually in the United States. 20 Red blood cell transfusion remains a frequently used means of optimizing oxygen delivery in the critically ill patient. Among adult populations, red blood cell use is relatively high among patients undergoing cardiac surgery; several observational studies in this population have established an increase in adverse outcomes, including morbidity, resource utilization and hospital mortality.21,22 Furthermore, despite evidence of adverse outcomes associated with increasing RBC administration within this population, there remains a significant degree of variation with respect to transfusion practices among adult providers. 23
The critically ill pediatric population is also at a significant risk for both anemia and receiving RBC transfusions. Indeed, nearly half of all critically ill children in one prospective, observational investigation of nearly 1000 patients received an RBC transfusion. Despite adjusting for age and illness severity, children in this cohort receiving at least one red cell transfusion demonstrated a longer duration of mechanical ventilation, greater nosocomial infection incidence and greater overall mortality. 1 As is the case in adults, RBC transfusion is a frequent means of therapy in critically ill children following cardiac surgery, prompting recent investigation within this patient population. Among pediatric cardiac surgical patients, greater RBC transfusion volumes are associated with prolonged duration of mechanical ventilation, an increase in nosocomial infection rates and duration of hospitalization.5–7
Extracorporeal membrane oxygenation is employed as a means of support in the setting of either cardiorespiratory or isolated respiratory failure among both pediatric and adult populations.24–27 While patients receiving ECMO anecdotally often receive numerous blood transfusions during their course, there is little literature detailing blood product utilization among this population.28–30 Retrospective investigation of nearly 100 neonates revealed a mean daily blood utilization of 250 mL, substantially greater than the cohort described here when adjusting for variable weights. 29 A recent, single-institution investigation demonstrated the administration of at least 10 units of RBCs in over half of adults supported with ECMO. 31 Bleeding, both surgical and at a cannula site, were frequent complications associated with ECMO support in our cohort and may, indeed, provide much of the impetus for RBC transfusion through a patient’s ECMO course. In addition to a reduction in hemoglobin and oxygen-carrying capacity, continued hemorrhage related to an inability to obtain surgical control of bleeding can, in turn, perpetuate coagulopathy, resulting in additional difficulty in ensuring hemostasis. We demonstrate here that, independent of hemorrhagic complications, however, patients exposed to greater red cell transfusion volumes while supported with ECMO for non-cardiac indications demonstrate an increased probability of in-hospital mortality.
There are no published prospective data describing the utility and safety of restrictive transfusion protocols among patients receiving extracorporeal support for cardiorespiratory or isolated respiratory failure. However, among general medical patients, a recent, prospective, randomized, non-inferiority investigation demonstrated that a restrictive transfusion strategy, while leading to a 44% reduction in transfusions, did not result in an increase in end organ dysfunction or mortality, supporting the safety of a relatively restrictive transfusion strategy in the general pediatric intensive care unit. 32 Given relative differences in transfusion volumes among subgroups in this study, restrictive practices may, indeed, result in a differential impact upon mortality as well. That said, the authors also contend that conservative transfusion practices may not impact mortality among any population of patients supported with extracorporeal membrane oxygenation or may, indeed, increase the odds of mortality, thus, providing the impetus for a randomized, prospective assessment of such a practice. These practices may include decreasing arbitrary hematocrit thresholds for transfusion, advocating for lower volume thresholds for surgical intervention or, through more liberal application of alternative medical means of promoting hemostasis, through antifibrinolytic administration or factor replacement.
There were several limitations to this study. First, this investigation is subject to the biases associated with any retrospective review. Importantly, given the limitations of study design, the relationship described here between greater RBC transfusion volumes and mortality is an association and does not definitively demonstrate causality. Furthermore, while an attempt was made to compare groups through both multivariate analysis and secondary sub-group analyses, there remains the possibility that the demonstrated increase in mortality associated with greater RBC transfusion volume is confounded by unaccounted covariates. Indeed, inclusion of populations with significantly discrepant transfusion volumes, indications for ECMO support and pathophysiological processes in our primary analysis did not demonstrate a significant increase in the odds of mortality with respect to RBC transfusion volume among this population as a whole. This may reflect the relative importance of other unaccounted-for covariates among the cardiac surgical population, including cardiopulmonary bypass, operative hemostatic strategies or the patient’s primary physiologic state. Blood product utilization outside of packed red blood cells and platelets, including cryoprecipitate and fresh frozen plasma, were accounted for inconsistently in this cohort of interest and may, indeed, play a contributory role for the findings we describe.
In conclusion, we describe here a large cohort of patients supported with ECMO and characterize associated packed red cell transfusion volumes. We demonstrate that, independent of established risk factors and among patients without hemorrhagic complications, greater red cell transfusion volumes among patients supported for non-cardiac indications are associated with an independent increase in the odds of all-cause hospital mortality. A prospective assessment of restrictive RBC transfusion strategies among those supported with ECMO may be indicated to investigate the safety and utility of such an approach in this specific population of critically ill patients.
Footnotes
Acknowledgements
The authors appreciate the assistance of Lee Ann Hassler, Myron Norman and Anesa Willoughby in the preparation of this manuscript.
Funding
National Center for Research Resources/NIH 1 UL1 RR024975
Conflict of Interest Statement
None declared.