
Abstract
Background:
Biocompatible circuits (BCC) are intended to decrease the activation of blood to the artificial cardiopulmonary bypass (CPB) surface. Typically, the coatings are made of various inert substances or molecules physiologically similar to endothelium.
Thromboelastography (TEG) graphically represents clot formation, strength of clotting and fibrinolysis. TEG analysis was undertaken to determine if coagulation could be preserved by the BCC.
Methods:
Five different BCC were studied in clinical applications. These five coated circuits were then compared to an identical circuit where only the oxygenator was coated. A pre- and post-bypass TEG was done for comparison. Six well-studied parameters of TEG analysis were compared: R time, Angle, K, Maximum Amplitude (MA), LY30% and Clot Index (CI). Postoperative bleeding and transfusion requirements were compared to TEG results for comparison.
Results:
All postoperative TEG results were significantly different from preoperative parameters except LY30%. No BCC circuit was able to prevent the significant disruption of the observed TEG coagulation parameters R, K, angle, MA and CI. Of note, the postoperative TEG parameters resulting from the Control and Trillium™ groups – which had the same type of oxygenator – were practically identical. The oxygenator, which represents the largest surface area in the CPB circuit, is the single most important factor influencing coagulation.
Conclusion:
While not harmful, BCC are ineffective in preserving TEG coagulation parameters post CPB. Clinical findings support laboratory TEG results in that there were no differences in bleeding or transfusion requirements between groups.
Keywords
Introduction
Upon initiation of cardiopulmonary bypass (CPB), the entire circulatory system is suddenly and intensely exposed to the unnatural environment of the CPB circuit. Negative manifestations of inflammatory response to CPB can involve all organ systems1-4 and, although the intensity of the individual response cannot be predicted, the magnitude of risk increases the longer a patient is supported by CPB. 5
Biocompatible circuits (BCC) were developed to minimize the inflammatory response which occurs when blood comes into contact with the artificial surface of the CPB circuit. The introduction of heparin-coated circuits, in fact, led to the use of decreased circulating heparin levels for CPB in some centers. 6 In general, BCC have demonstrated decreased fibrinogen deposition, decreased complement activation, decreased platelet activation and decreased inflammatory response compared to uncoated CPB circuits.7-9 A meta-analysis involving 36 randomized controlled trials and 4360 patients concluded that patients undergoing CPB with a BCC had fewer red blood cell (RBC) transfusions, lower rates of atrial fibrillation and spent a shorter time in the intensive care unit postoperatively. 10 Baksaas et al., in 1999, found lower levels of myeoloperoxidase in a fully coated circuit when compared to a uncoated circuit with a coated oxygenator. 11 Interestingly, they described the exact same scenario as in our study, with identical products. Finally, research has demonstrated the efficacy of heparin-coated circuits over other non-heparin-coated BCC circuits. 12 Heparin-coated and non-heparin-coated BCC were included in this study for comparison.
The science involved in thromboelastography has been well studied and can be used to guide the transfusion of hemostatic component therapy.13,14 Thromboelastograph (TEG) analysis differentiates and graphically reproduces the various elements of clot formation and fibrinolysis. 14 Patients who are coagulopathic show impaired clot formation when TEG analysis is done. TEG technology determines if a patient’s coagulopathy is due to low levels of clotting factors or low numbers and/or impaired platelet function.
One hundred and sixty-five patients underwent CPB-assisted cardiac surgery between July 2007 and April 2008. This was a prospective cohort study in which patients were assigned to the control group or one of the 5 coated-circuit groups: 40 Control; 33 Trillium™; 32 Phosphorylcholine; 34 Bioline™; 33 PMEA; 11 GBS. TEG parameters R time, Angle, K, Maximum Amplitude (MA), LY30% and Clot Index were compared pre and post bypass.
Material and Methods
Circuits groups
The present study compared five different BCC groups to a control group where only the oxygenator was coated. Clinical and laboratory parameters were compared to determine if any of the BCC were able to preserve hemostasis as measured by TEG analysis and improve clinical outcomes as determined by postoperative bleeding and transfusion requirements.
TEG
The Thrombelastograph® (TEG®) Hemostasis System 5000 series (Haemonetics, Braintree, MA, USA), a non-invasive diagnostic instrument, is intended to provide a quantitative and qualitative indication of the overall coagulation profile interpreted in terms of the hypo-, normal, or hypercoagulable state of the sample and the degree of lysis. The TEG parameters included in this study are defined with normal values as follows: “R” (4 – 8 min), time to initial fibrin formation, representing the effectiveness of the clotting enzymes; “K” (0 – 4 min), time required to achieve clot strength of 20 mm; “α” (47 – 74 degree) speed of fibrin build-up and cross-linking – directly related to fibrinogen level; MA (54 – 72 mm), demonstrates maximum dynamic properties of fibrin and platelet bonding via GPIIb/IIIa, representing platelet function/aggregation; LY30% (0 – 8 %), percentage of clot lysis 30 minutes after MA; CI (-3 – 3), relative to clot strength whereby negative value indicates a hypo-coagulable state and positive value indicates a hyper-coagulable state.
Patient and Study protocol
Patients were enlisted into this prospective cohort study between July 2007 and April 2008. Ethics approval and informed consent was obtained for one hundred and eighty-one patients undergoing coronary artery bypass grafting and/or valve surgery. A small number of the TEG curves were unavailable or flawed. Consequently, 16 patients were removed from analysis: 1 Bioline™; 4 Control; 0 Hyaluronan; 5 Phosphorylcholine; 2 Trillium™; 4 PMEA.
Patients, emergent or afflicted with a chronic inflammatory disorder (rheumatoid arthritis, systemic lupus erythematosus, Crohn’s disease, Wegener’s granulomatosis, sarcoidosis, osteoarthritis, debilitating chronic obstructive pulmonary disease, ulcerative colitis, psoriasis and multiple sclerosis), were excluded from the study. Subjects who had suffered a recent stroke, seizures or who were afflicted with a neurodegenerative disease such as Alzheimer’s or Parkinson’s disease were also excluded. Patient demographics were noted upon entering the operating room. Postoperative data was collected until discharge from hospital.
Anesthesia
Patients were pre-medicated with 1-2 mg per os of ativan (Biovail Pharmaceuticals Canada, Mississauga, ON) and 3 L/minute of oxygen. Intravenous induction medications consisted of midazolam (2 mg) (Biovail Pharmaceuticals Canada), sufentanil (50 μg) (Biovail Pharmaceuticals Canada), lidocaine (50mg) (Astra Zeneca Canada Inc, Mississauga, ON), propofol (50-100 mg) (Novopharm Limited, Toronto, ON), rocuronium (50 mg) (Organon Canada Ltd, Scarborough, ON) and cefazolin (2 g) (Novopharm Limited, Toronto, ON). Maintenance of anesthesia was achieved using isoflurane (0.5-1.0%) (Pharmaceutical Partners of Canada (PPC), Richmond, ON) or sevoflurane (0.5-1.0%) (Abbott Laboratories Limited, Saint-Laurent, PQ), with a sufentanil infusion (0.5 μg/kg/hour) (Biovail Pharmaceuticals Canada). Six milliliters of blood was drawn from the arterial line for blood gas analysis, activated clotting time (ACT), heparin dose response (HDR) and TEG analysis. An HDR cartridge (Medtronic, Minneapolis, MN) was used to determine patient sensitivity to heparin (Pharmaceutical Partners of Canada) and to calculate a heparin-loading dose. Upon initiation of bypass, the patient received furosemide (20 mg) (Sanofi-Aventis, Laval, PQ), midazolam (2 mg) (Biovail Pharmaceuticals Canada) and rocuronium (50 mg) (Organon Canada Ltd). When patients were weaned from CPB, they received magnesium sulphate (2 g) (Abbott Laboratories Limited) calcium gluconate (2 g) (Pharmaceutical Partners of Canada), dopamine (5 μg/kg/minute) (Novartis Pharmaceuticals, Dorval, PQ) or epinephrine (0.05 μg/kg/minute) (Hospira Inc., Lake Forest, IL) and cephazolin (2 g).
Surgery and CPB
The S3 or the S5 heart-lung machines (Stöckert, Munich, Germany) were used for all patients. All CPB circuits had open venous reservoirs and uncoated cardioplegia systems. The priming volume consisted of: a combination of crystalloid and colloid; 50-300 mL normosol; 500 mL pentastarch 10%; 2.5 mL/kg of mannitol 20%; 50 mL of sodium bicarbonate and 10,000 IU of heparin. A pre-bypass filter, effective to 0.2 µm, was used for priming of the CPB circuit. A cell saver was in use throughout the entire procedure, minimizing shed blood return through the pump suckers back to the patient. The volume of blood collected to the cell saver and returned to each patient was not significantly different between the groups.
CPB was initiated once the ACT reached 480 sec and the circulating heparin concentration within the patient reached 3mg/kg of body weight (300 IU/kg). Patients were cooled to 32-33oC and supported using a non-pulsatile roller-pump. A cardiac index of 1.8-2.4 L/min/m2 was maintained. Patients were transfused if the hemoglobin level fell below 75-80 mg/L. All efforts were made to maintain the mean arterial blood pressure within 60-80 mmHg. Shortly after initiation of CPB, a cross-clamp was applied to the aorta and the heart was arrested with warm blood and KCl (20-30 mEq/L). Cardioplegia was cooled upon cardiac quiescence and maintenance blood and KCL (5-10mEq/L) were given intermittently. Once the technical aspects of surgery were completed, de-airing and a final dose of warm KCL-free blood was given to the heart. Upon spontaneous return of the heart’s own cardiac rhythm and adequate systemic rewarming to 36.5oC, the patient was weaned from CPB.
Following decannulation, a measured protamine dose was given to reverse all circulating heparin. The remaining hemodiluted contents of the CPB circuit were processed by the cell saver and the resulting concentrated volume of RBC suspended in saline was infused into the patient.
Data collection
Patient demographics included for comparison were: weight, body mass index (BMI), age, sex, ejection fraction, smoking history and cardiac risk factors. Aspirin (Bayer HealthCare, Bayer Inc, Toronto, ON), plavix (clopidogrel bisulphate, Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership, New York, NY), aprotinin (Trasylol, Bayer HealthCare Inc., Pittsburg, PA) and tranexamic acid (Sandoz, Boucherville, PQ) use were included because of their effect on bleeding. Aprotinin dosage never exceeded 3 million kallikrein international units (KIU). Total tranexamic acid dosage never exceeded 2 grams. Biometric data included type of surgery, CPB time and cross-clamp time. Two blood samples were drawn and immediately analyzed for thromboelastography: a preoperative sample before surgical incision and a post-protamine sample after heparin neutralization. Four channels were run to assure accuracy and reproducibility of the TEG analysis. A heparinase cup and a standard non-heparinase cup were always used to check for residual heparin. Recorded data included: total postoperative chest tube drainage at 14 hours, ventilation time, time spent in intensive care (ICU) and hospital length of stay. All transfusions were tracked to patient discharge from hospital. Finally, the volume processed by the cell saver and autologous red cell volume returned to the patient were documented.
Statistical analysis
A sample size of 150 patients was determined sufficient to detect an observed effect size of 0.5 (medium effect) for statistical analysis using a one-tailed test with an observed power of 0.802. Descriptive statistics were used to summarize the data. A t-test or analysis of variance (ANOVA) was used for continuous variable and categorical variables, respectively. A p-value of less then 0.05 was considered statistically significant. Analyses were carried out with the PASW Statistics 18.0 (SPSS Inc., Chicago, IL).
Results
Preoperative demographics and perioperative clinical data are compared in Table 1. No significant demographic differences or bleeding and transfusion requirements were observed between any of the groups.
Patient demographics and surgical outcomes ( ± standard deviations in parenthesis).
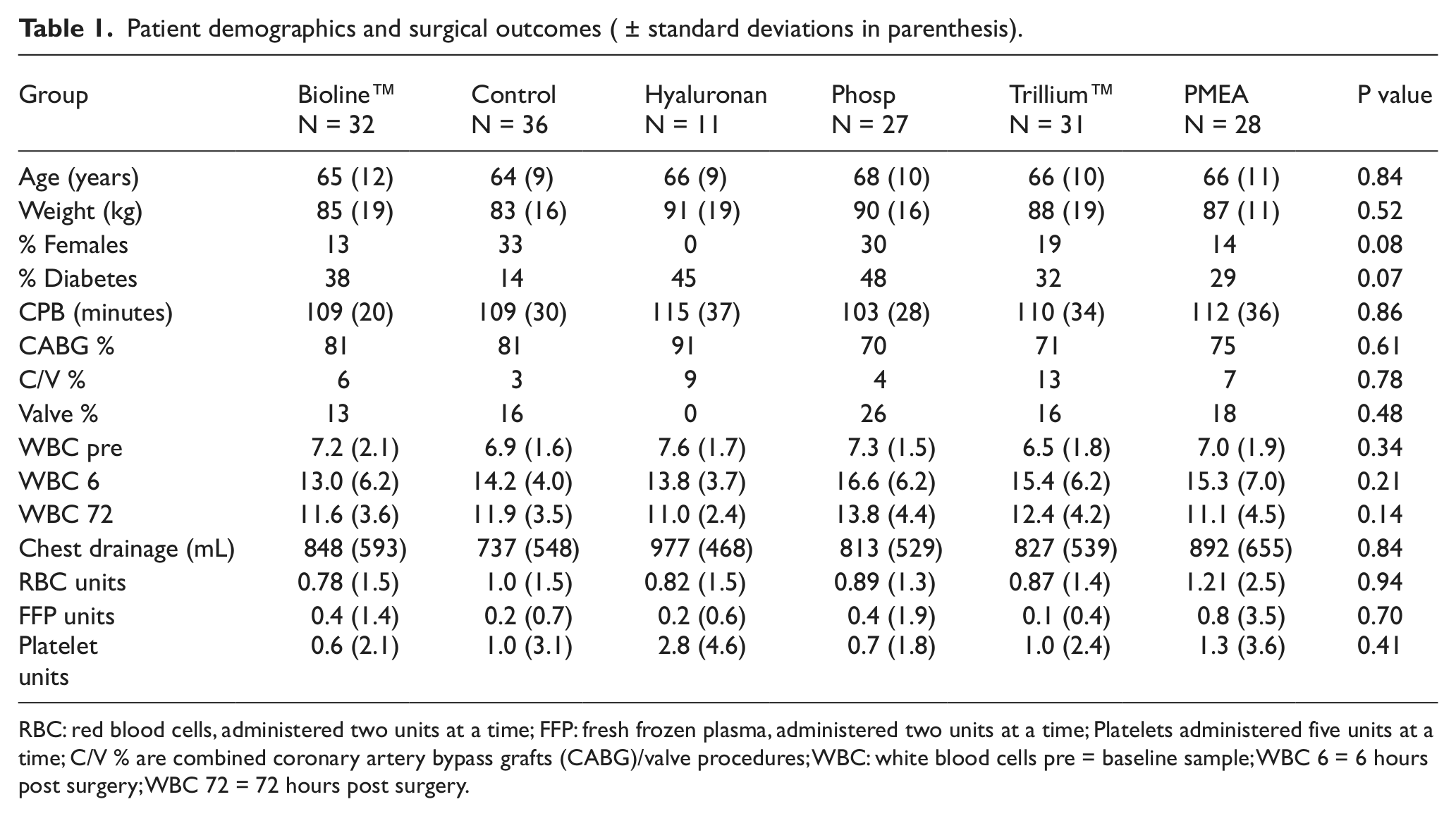
RBC: red blood cells, administered two units at a time; FFP: fresh frozen plasma, administered two units at a time; Platelets administered five units at a time; C/V % are combined coronary artery bypass grafts (CABG)/valve procedures; WBC: white blood cells pre = baseline sample; WBC 6 = 6 hours post surgery; WBC 72 = 72 hours post surgery.
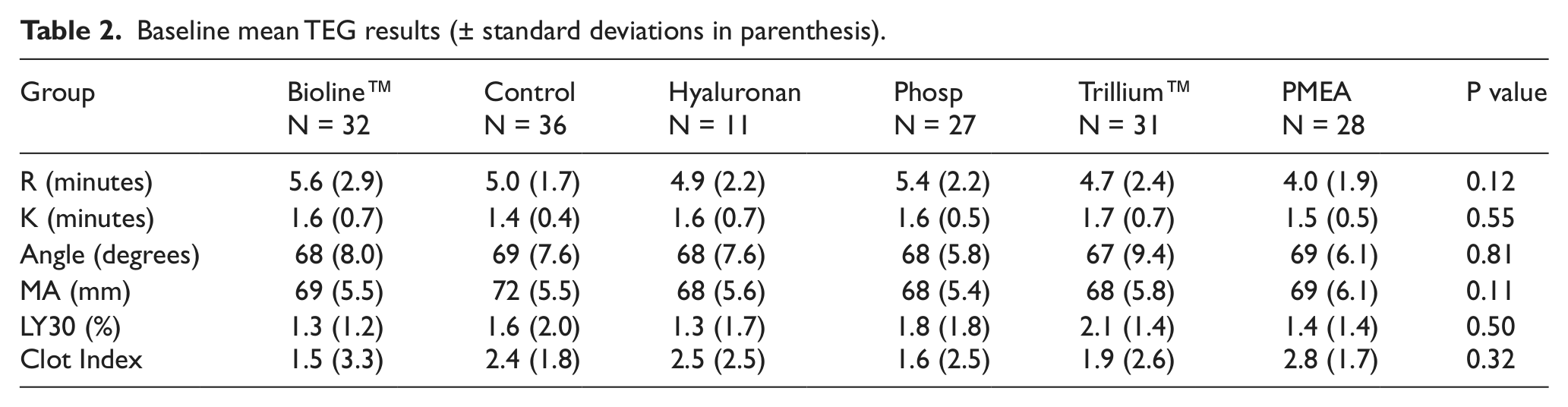
Preliminary baseline preoperative TEG analysis showed no significant differences between the groups, as demonstrated in Table 2.
Baseline mean TEG results (± standard deviations in parenthesis).
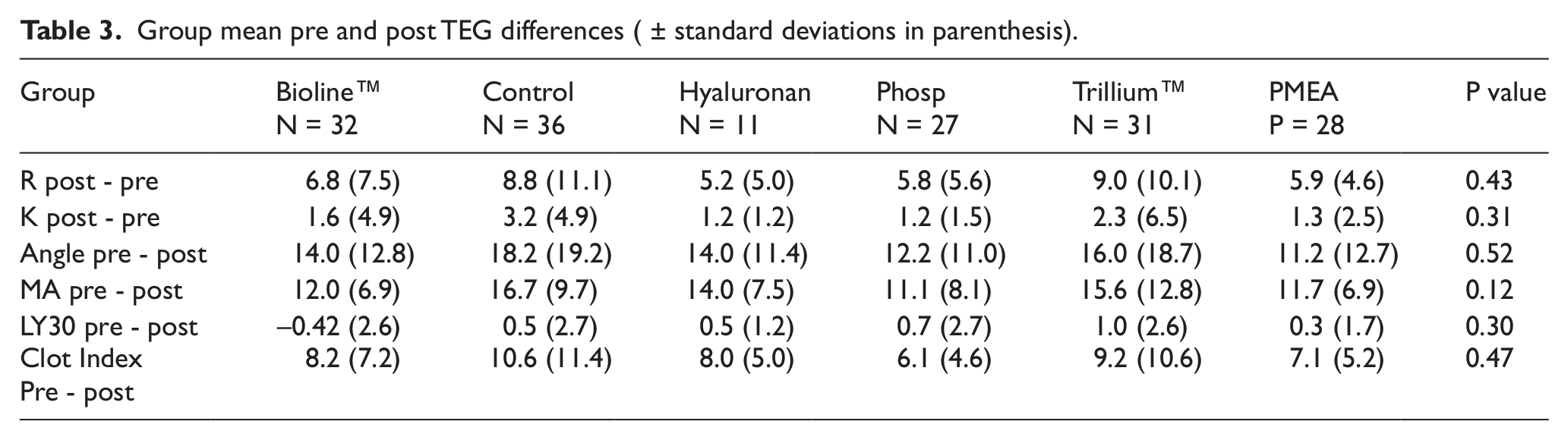
No significant differences were found between the groups when comparing postoperative TEG results (not shown). With the exception of LY30%, all postoperative TEG parameter values were significantly different from pre-bypass baseline values in a paired samples t-test analysis (p<0.009) (not shown). Between-group differences were not observed, as demonstrated in Table 3.
Group mean pre and post TEG differences ( ± standard deviations in parenthesis).
Figures 1, 2, 3 and 4 demonstrate the differences observed between the pre-and post-bypass TEG parameters R, K, angle and MA. Though no significant differences were observed, obvious trends are identified and more easily noted in Figures 1 through 4.
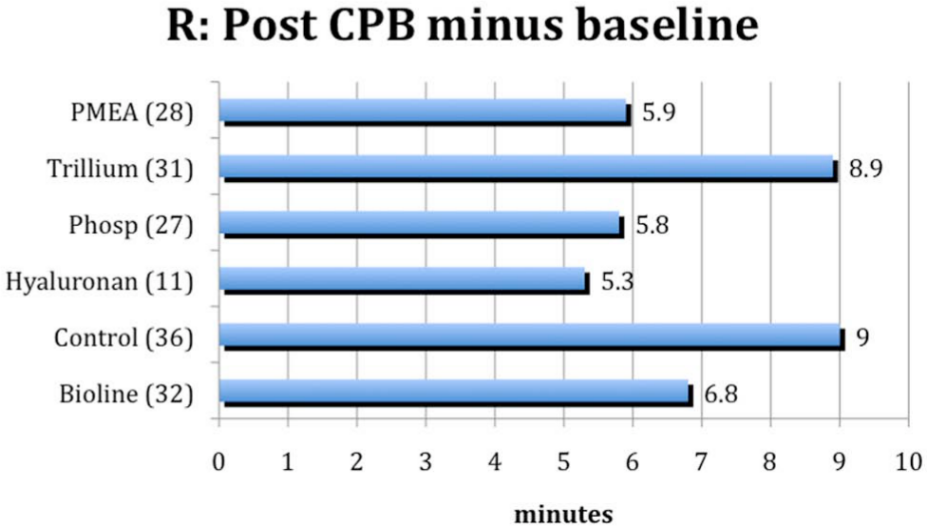
Pre- and postoperative R differences between the groups.
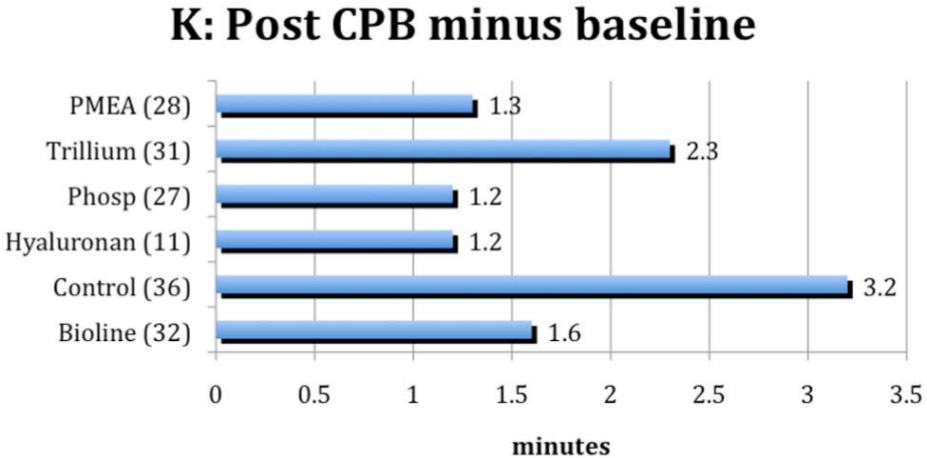
Pre- and postoperative K differences between the groups.
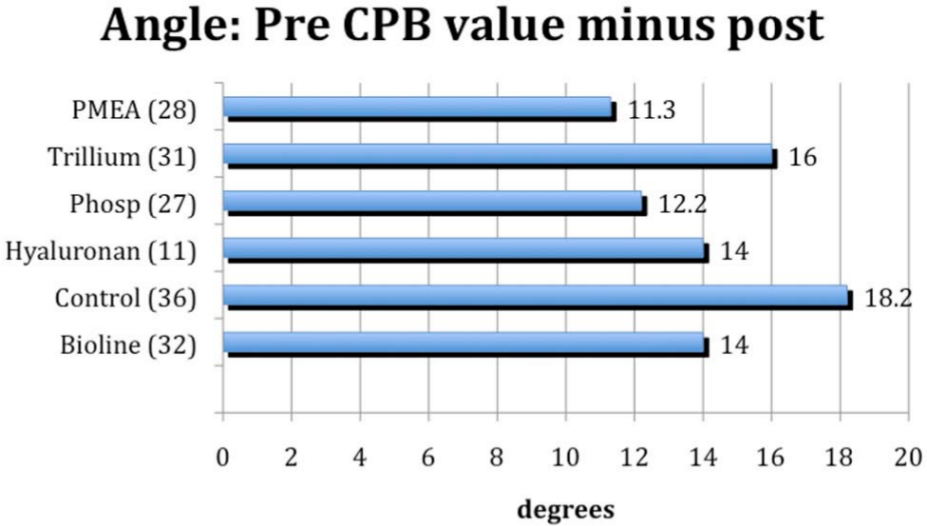
Pre- and postoperative angle differences between the groups.
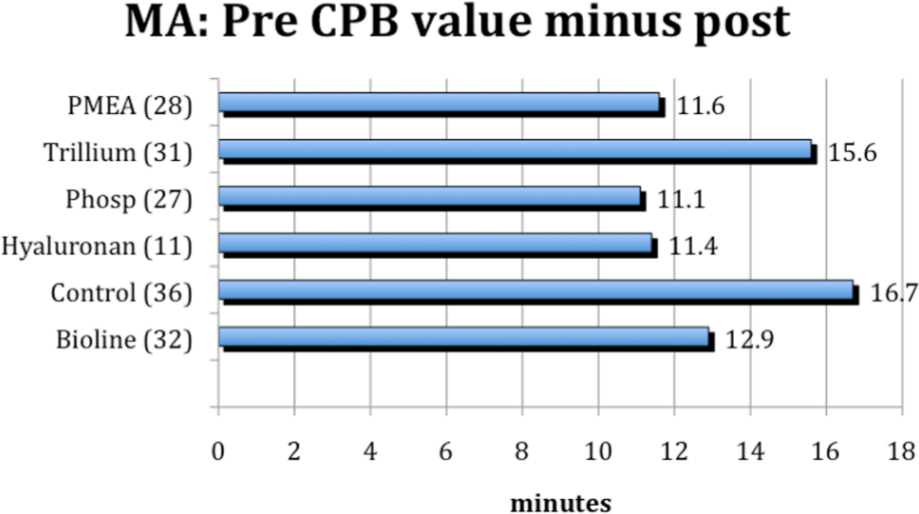
Pre- and postoperative MA differences between the groups.
Discussion
No significant differences were observed between any of the BCC groups and the control group, as demonstrated by the TEG graphic analyses of parameters R, K, MA, LY30% and CI. The results complement postoperative clinical findings with respect to bleeding and transfusion requirements in that, once again, no significant differences were found.
Circuit coatings can have an effect on postoperative outcomes, as shown by many published results. Our study indicates that the oxygenator used has a greater effect on TEG parameters than the BCC, as evidenced by the similarity in TEG parameter results between the Trillium™ and the control groups. Both circuits had the same Trillium™-coated oxygenator. The consistently improved, but non-significant post-bypass TEG results shown in the Trillium™ group demonstrate the small, but beneficial effect of a fully coated circuit. Indeed, all post-bypass TEG results from fully coated circuit groups performed better than the control group (Figures 1-4). Unfortunately, these improvements were not realized clinically. The greatest surface area of the CPB circuit in contact with blood is the oxygenator and heat-exchanger (~2.95 m2). The tubing (0.28 m2), arterial filter (0.135 m2) and venous reservoir (< 0.135 m2) make up the rest of the CPB circuit. We wanted to compare all available coated CPB circuits in Canada to our currently used CPB circuit. Having had an uncoated oxygenator in the control group would have demonstrated conclusively the dramatic effect oxygenator choice has on outcome parameters, but as these results were not expected, it was not included in the design of the study.
The interruption of aprotinin usage during the study was a confounding factor. Midway through patient recruitment, aprotinin was removed from the market. Fifty percent of patients in the control group, 45% of patients in the Trillium™ group and 11% of patients in the phosphorylcholine group received aprotinin. Patients did not receive aprotinin in the hyaluronan, Bioline™ or PMEA groups. TEG parameter “R” isolates the contribution of clotting factors to clot formation. Aprotinin will prolong the “R” at therapeutic levels, presumably by its inhibition of kallikrein and factor XI, a contact system protein. 27 Though the longer R found in both the control and Trillium™ groups might be explained by the administration of aprotinin, it does not explain the similarly elevated angle, K and MA observed in these groups as well. One is led to conclude that oxygenator design, with its large surface area, plays a more important role on hemostasis than does the BCC coating. Hussaini et al., in 2009, described significantly different levels of white blood cell entrapment, using various arterial filters models on identical circuits. 28 Our findings demonstrating the impact of oxygenator type are unsurprising in this context if only based upon of the superior surface area of an oxygenator when compared to an arterial filter.
The desired outcome was to discover a coating which might lessen the activation of coagulation and inflammation for all patients undergoing CPB-assisted cardiac surgery. Our study results indicate that, while the BCC are not harmful, the effects on patient outcome are minimal. Within a CPB circuit, the oxygenator with its large surface area is the most influential component effecting hemostasis and the inflammatory response.
Footnotes
Acknowledgements
The authors would like to thank the Royal University Hospital Foundations, Maquet Dynamed Inc., Sorin Group Canada, Terumo and Medtronic of Canada Ltd. for financial assistance. The following individuals must be acknowledged for their invaluable assistance and support: E.D. McNaire; H. Prasad; M. Rosin, G. Smith and V. Uppal.
Conflicts of interest statement
The authors declare that there are no conflicts of interest.