
Abstract
Introduction:
Retrograde autologous priming (RAP) of the cardiopulmonary bypass (CPB) circuit could reduce the degree of haemodilution associated with priming with acellular solutions. However, there is no strong evidence to prove that the practice of RAP reduced intraoperative packed red cell (PRC) or blood product transfusion.
Objective:
To evaluate the effect of RAP on intraoperative PRC usage in coronary artery bypass grafting (CABG).
Methods:
This study is a prospective, observational study on patients who underwent first-time, isolated CABG using CPB between April 2012 and July 2012. Two groups of patients were identified: 1. Non-RAP group (n=128) and 2. RAP group (n=73). The primary outcome for the study was the amount of PRC and blood product usage between the induction of anaesthesia and the cessation of CPB.
Results:
Use of PRC and blood products in the operating room was comparable in both groups. Univariate logistic regression showed that RAP was not an independent predictor of PRC or blood product transfusion (p=0.43). Multivariate logistic regression showed that CPB time, preoperative haemoglobin (Hb) levels and creatinine clearance were independent predictors of blood product transfusion.
Conclusion:
Practising RAP with mean volumes of 300 ml does not necessarily reduce PRC and other blood product transfusion requirements during CABG. In our practice, RAP was performed, aiming at displacing CPB circuit prime volume with which the perfusionist felt comfortable and dictated by haemodynamic parameters prior to commencing CPB. We presume this is the case in many units around the world. This practice, in our opinion, is not enough to achieve the benefits of RAP, if any, in the form of a reduction of packed red cell transfusion requirements. The true advantages of RAP in cardiac surgery need to be studied in a prospective, randomized, controlled trial.
Introduction
Conventionally, cardiopulmonary bypass (CPB) circuits are primed with acellular solutions. Various studies have shown that priming the CPB circuit with crystalloid reduces colloid osmotic pressure (COP)1-5 and exacerbates haemodilution, adding to post-CPB end-organ dysfunction. Partially priming of the cardiopulmonary bypass circuit with the patient’s own blood at the initiation of bypass, known as retrograde autologous priming (RAP), has been shown to reduce the deleterious effects of haemodilution.1-10 RAP is thought to maintain COP, reduce pulmonary oedema and haemodilution upon the onset of CPB, which has been shown to improve clinical outcomes, reduce ventilator times in the postoperative period and may reduce the requirements for autologous blood transfusion after cardiac surgery.6-10,11-13
A significant trend towards reduced postoperative weight gain (an indicator of third-space fluid sequestration) demonstrated in the RAP group of patients has possibly contributed to reduced length of postoperative hospital stay after cardiac operations.9,10 Although RAP appears to offer clinical advantages, there is a lack of data pertaining to its safety. 14
We conducted this study to investigate whether the practice of RAP resulted in a reduction in transfusion of packed red cells and the other blood products during cardiac surgery. 15 This study represents a prospective, non-randomised, observational study based on cardiac surgical practice in a large volume university teaching hospital in the United Kingdom.
Patients & Methods
Patient population and study design
This study represents a prospective, observational study on patients who underwent first-time, isolated coronary artery bypass graft surgery using cardiopulmonary bypass support between April 2012 and July 2012. Two groups of patients were identified in this cohort:
Control: Non-RAP group (did not have RAP performed).
Test: RAP group (had RAP prior to the institution of full CPB)
All patients undergoing coronary artery bypass grafting as elective or urgent procedures were included in the study. In order to maintain uniformity of the nature of the surgery, patients undergoing other types of adult cardiac surgery, including emergency coronary artery bypass surgery, ventricular assist device implantation, heart transplantation, redo-operations and pulmonary thromboendarterectomy were excluded from this analysis.
Detailed demographic and intraoperative information was obtained from the anaesthetic and perfusion records (Table 1). The primary outcome for the study was defined as the amount of blood product usage between the times of the induction of anaesthesia and the cessation of cardiopulmonary bypass. Transfusion of blood or blood products following the cessation of bypass was not included in this study as other confounding factors, like postoperative surgical bleeding, could have been implicated. Packed red cells were transfused during CPB if the haemoglobin level was less than 7.5 g/dL or the haematocrit on CPB fell below 24%.
Demographic and clinical details of patients.
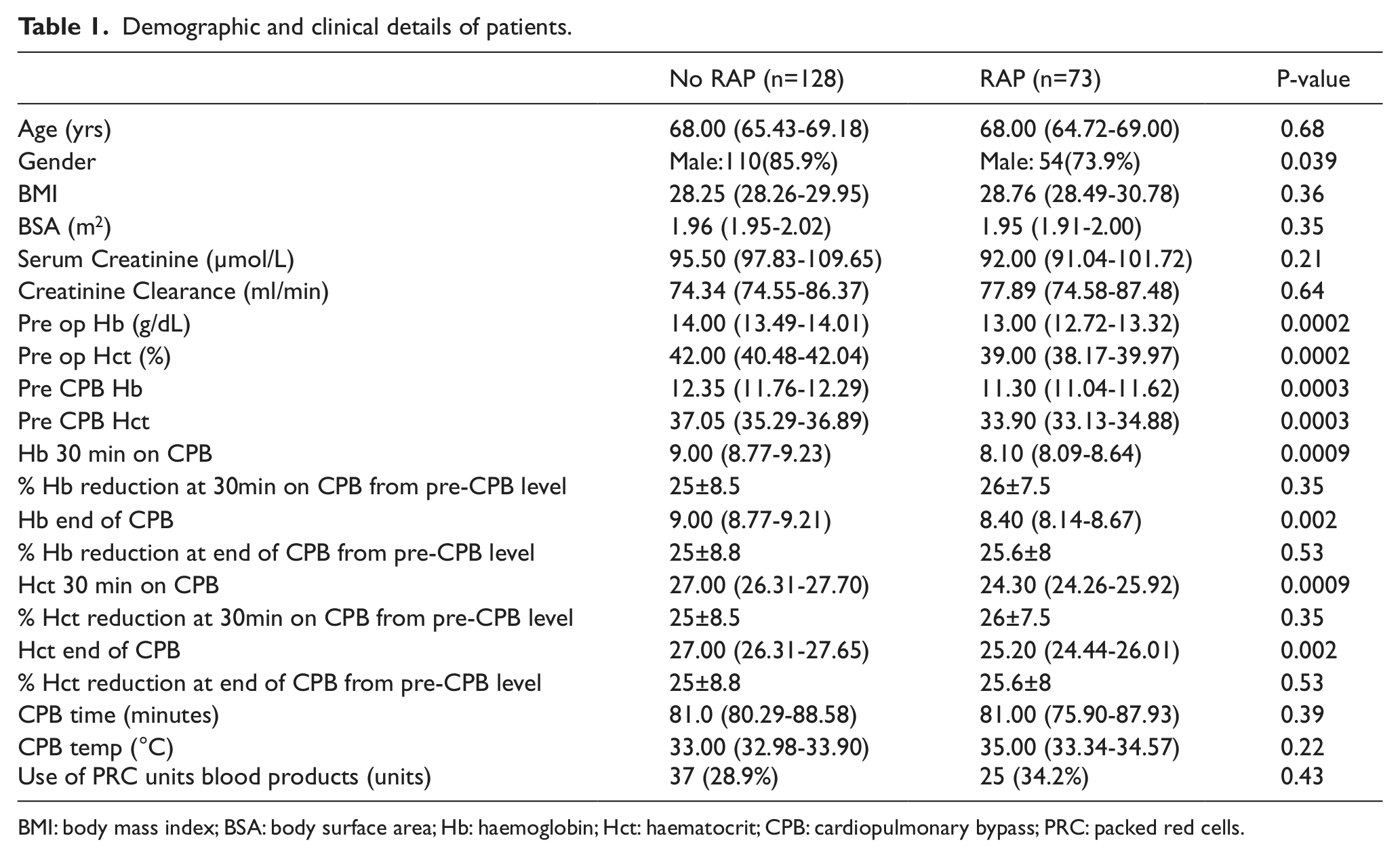
BMI: body mass index; BSA: body surface area; Hb: haemoglobin; Hct: haematocrit; CPB: cardiopulmonary bypass; PRC: packed red cells.
Anaesthesia
In both groups, general anaesthesia was induced with midazolam, propofol and morphine. Standard invasive monitoring, including an arterial line and central venous line, was performed in all patients. General anaesthesia was maintained during the operation with isoflurane, propofol and neuromuscular blockade. Anticoagulation for cardiopulmonary bypass was achieved by the administration of unfractionated heparin at a dose of 300 U/Kg bodyweight. The activated clotting time (ACT) was maintained >480 sec during the course of the operation. After weaning from CPB, heparin was reversed with protamine sulphate, administered at a dose of 1mg/100 U of the total dose of heparin.
Technique for initiation and maintenance of cardiopulmonary bypass
In the majority of cases, a size 24 Sarns cannula (Terumo Cardiovascular Systems, Ann Arbor, MI) was used for cannulation of the ascending aorta. A 2-stage MC2 venous cannula (Medtronic Inc. Cardiac Surgery, Minneapolis, MN) was used for right atrial cannulation.
The CPB circuit was comprised of a Sorin Evo oxygenator and integrated hard-shell venous reservoir (Sorin Group Italia, Mirandola, Italy). Venous and arterial lines were 1/2” and 3/8” calibre, respectively, with a 3/8” calibre pump boot.
The ACT was checked at regular intervals and further doses of unfractionated heparin administered to maintain a value >480 seconds. Antegrade, intermittent cold blood cardioplegia was used for myocardial protection. CPB flows were maintained at a rate of ≥2.4 L/m/m2. The temperature on CPB varied between 32.0-36.9°C. Shed mediastinal blood was re-circulated through a cardiotomy sucker into the venous reservoir.
Non-RAP group
In the Non-RAP group, the CPB circuit was primed with 1500 ml of fluid, consisting of Hartmann’s solution (1200 ml) and mannitol 10% (300 ml).
RAP Group
In the RAP group, the CPB circuit was initially primed with the same volume and consistency of fluid as the Non-RAP group. However, once the CPB cannulae were secured, RAP was commenced by a controlled displacement of prime into an empty intravenous fluid bag attached to the venous line proximal to the reservoir. In order to optimize the prime displacement and RAP, the reservoir prime level was reduced to 50 ml. This was followed by the controlled release of the venous clamp to allow blood to slowly enter the venous reservoir whilst paying close attention to systemic arterial and venous filling pressures. Blood was allowed to fill the reservoir as long as the central venous pressure (CVP) remained positive and the systemic blood pressure did not fall below a mean arterial pressure of 55 mmHg. The blood collected in the reservoir was used to displace prime volume by slowly turning the pump on and allowing prime to be displaced into an intravenous fluid bag attached to the arterial recirculation line. When the reservoir volume was reduced to a point just above the level sensor safety device, displacement was stopped and CPB commenced. RAP was not performed if the pre-CPB Hb was greater than 14 g/dL or if the patient was haemodynamically unstable.
Statistical analysis
Statistical analysis was performed by an independent statistician, blinded to data acquisition. Minitab® 16.2.1 (2010 Minitab Ltd., Coventry, West Midlands, UK) statistics software was used. All departures from normality for the acquired data were assessed using the Anderson-Darling test. The median with interquartile range (IQR) was used for reporting continuous variables. For comparison of continuous variables with non-normal distribution, the Mann-Whitney U test was used. An unpaired t test was used for comparing continuous variables with normal distribution. Fisher’s exact test was used for comparing categorical variables. All p-values are two sided and the α level was set at 0.05.
To identify statistically significant predictors (continuous or categorical variables) for a binary outcome, univariate binary logistic regression (LR) analysis was used. The binary outcome was transfusion of blood products in the operating room (coded as 1) or no transfusion (coded as 0). Predictor variables with a p-value less than 0.25 obtained from univariable LR analysis were used to fit a multivariable LR model16,17 to obtain maximum likelihood estimates of the parameters. Goodness of fit (GOF) of the overall fit of a model was assessed by the deviance GOF Chi-square test and the Hosmer-Lemeshow test. 17 Co-linearity between continuous predictor variables, which can increase the variance of the regression coefficients making them unstable and difficult to interpret, was assessed visually by matrix plots and quantified using the variance inflation factor (VIF). 18 Interaction between independent continuous variables, represented as “product terms”, was also assessed. The absence of statistical significance for the “product term” in the LR model excluded it from the final model. 17 A bootstrap procedure was used to cross-validate the confidence intervals calculated for odds ratios derived from the fitted LR model, using StatsDirect statistical software version 2.7.8 (StatsDirect Ltd., Altrincham, Cheshire, UK). The bootstrap confidence intervals used here are the ‘bias-corrected’ type. The bias statistic shows how much each mean model parameter from the bootstrap distribution deviates from the observed model parameters.
Results
Two hundred and one patients who underwent coronary artery bypass grafting during the study period were included in the analysis. Of these, 73 subjects (34.7%) underwent RAP during surgery and 128 (65.3%) underwent conventional crystalloid priming of the CPB circuit. Both study groups were comparable in terms of age, body mass index (BMI) and body surface area (BSA) (Table 1). The range of the retrograde prime volume in the RAP group was 200-1000 ml, with a mean of 312 ml ± a standard deviation of 118 ml. The non-RAP group had a higher proportion of male patients (Table 1). The two groups also differed in terms of their preoperative and pre-CPB Hb and haematocrit (Hct) levels, with subjects not receiving RAP having higher Hb and Hct levels compared to those in the RAP group. The use of packed red cells in the operating room was comparable in both groups.
In order to assess whether RAP was an independent predictor for the transfusion of blood products in the operating room, univariate logistic regression was used. Other relevant variables used in the univariate LR analysis are tabulated in Table 2. Univariate analysis ruled out RAP being an independent predictor of blood product transfusion (p=0.43). Variables which showed statistically significant association with the outcome (indicated by asterisk *) were included in the backward stepwise multivariable LR model. Careful assessment of the GOF of the model, along with the assessment of variable co-linearity and variable interaction, was carried out at each step. The final model showed that creatinine clearance, CPB time and preoperative Hb levels, were independent predictors of blood product transfusion in the operating room in patients undergoing CABG (Table 3). The VIF of the independent variables in the final model was small (average: 1.15), indicating minimum co-linearity. 18 The final model had a good fit, as confirmed by the deviance Chi-square GOF test (p=0.91) and the Hosmer-Lemeshow test (p=0.09). The measure of association between the response variable and the predicted probabilities showed a concordance of 85% versus 14.7% discordance and 0.3% ties (Goodman-Kruskal Gamma = 0.70), which indicates that the predictive ability of the model was good. The final model was validated by bootstrapping to 1000 iterations (Table 4), which shows the bias to be very small for all variables included in the final model.
Univariate logistic regression: (beta) coefficient for each variable along with the standard error (SE), z (z= coefficient/SE) and p values. * indicates statistically significant p-values for inclusion in the multiple logistic regression model.
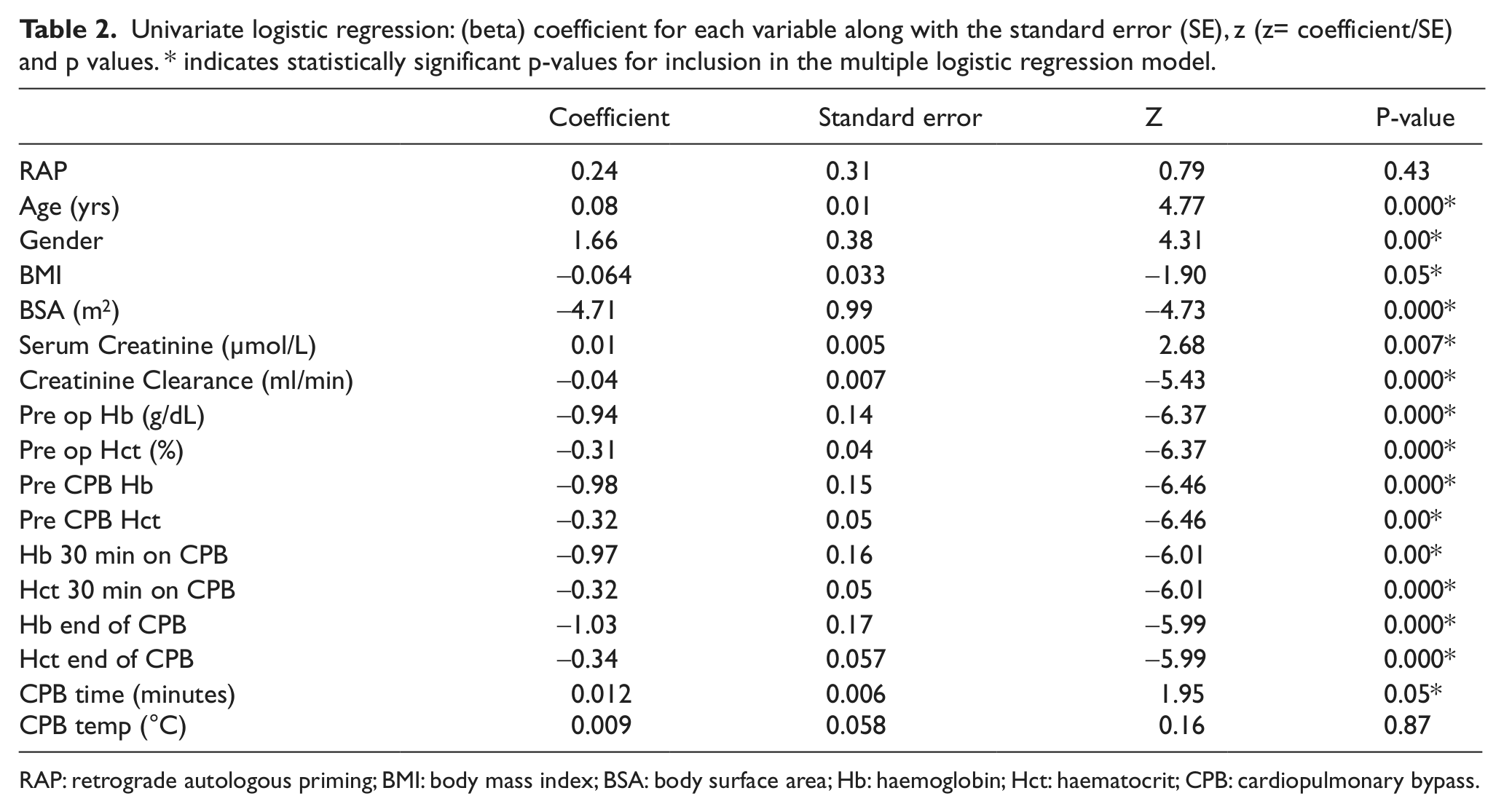
RAP: retrograde autologous priming; BMI: body mass index; BSA: body surface area; Hb: haemoglobin; Hct: haematocrit; CPB: cardiopulmonary bypass.
Final binary logistic regression model: (beta) coefficient for each variable along with the standard error (SE), z (= coefficient/SE) and p values. The Odds Ratio indicates the odds of having the blood product transfusion in the operating room per unit increase or decrease in the level of the variable. CI indicates the 95% confidence intervals. VIF is the variance inflation factor which indicates the co-linearity among the variables.
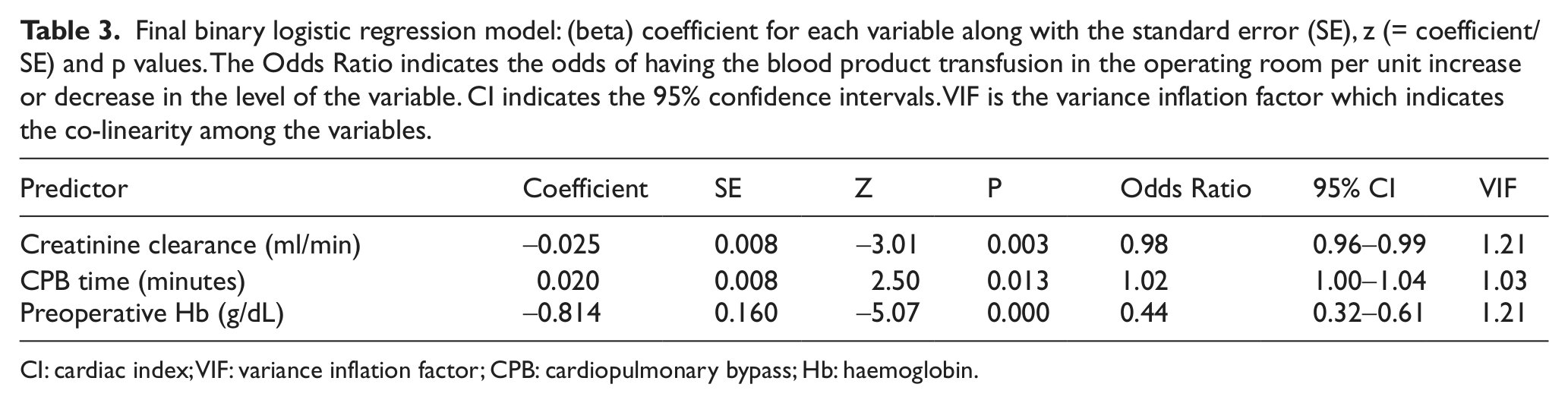
CI: cardiac index; VIF: variance inflation factor; CPB: cardiopulmonary bypass; Hb: haemoglobin.
Logistic regression - bootstrap Odds Ratio (OR) estimates (Re-sampled 1000 times).

CPB: cardiopulmonary bypass; Hb: haemoglobin.
Discussion
Retrograde autologous priming is routinely performed in some units in the belief that it helps maintain an adequate haematocrit on CPB and, thereby, reduces transfusion requirements. In this study, we investigated the effect of retrograde autologous priming in reducing packed red cell or other blood product transfusions, specifically after first-time, non-emergency coronary artery bypass grafting.
This study demonstrated that patients who underwent retrograde autologous priming did not have a statistically significant reduction in packed red cell or other blood product transfusions during coronary artery bypass grafting. However, we identified several predictors of intraoperative packed red cell and blood product transfusion, which include low preoperative haemoglobin, abnormally low creatinine clearance and prolonged cardiopulmonary bypass times.
A low preoperative haemoglobin and prolonged CPB time can explain increased blood transfusion requirement as they result in increased haemodilution on bypass and increased platelet dysfunction, leading to bleeding and subsequent blood transfusion requirement. We are unable to explain why an abnormally low preoperative creatinine clearance results in increased blood transfusion requirement.
In 2002, Balachandran et al. demonstrated that retrograde autologous priming of the bypass circuit reduced homologous blood transfusion due to the reduction in bypass circuit priming volume. 6 Recently, Ševerdija et al. demonstrated a reduction in blood transfusion requirements in coronary artery bypass grafting with retrograde autologous priming. 7 In a prospective, randomized trial, Hou et al. also demonstrated a significant decrease in the intraoperative use of blood, particularly in patients with a small body surface area (<1.5m2). 8 In this study, they included patients with a body surface area <1.5m2 and excluded those with a preoperative haematocrit <33% and/or an estimated cardiopulmonary bypass time of more than 90 minutes. The total RAP volume in these studies was not expressed as a proportion of the total estimated circulating volume or bodyweight of the patient. Therefore, the findings of these studies cannot be simply extrapolated to the spectrum of patients we are engaged with on a daily basis.
In a small pilot study involving a total of 20 patients, Eising et al. demonstrated a reduction in extravascular lung water with RAP, but no significant effect on postoperative cardio-respiratory function. 9 In 1998, Rosengart et al., in their randomized, controlled trial, demonstrated a significant reduction in haemodilution and transfusion requirements in patients undergoing coronary artery bypass grafts if they underwent RAP compared to those who did not. 10 This was a randomized trial with a strict protocol to perform RAP, which resulted in a total RAP volume of a minimum of 1000 ml. In our opinion, to demonstrate the efficacy of RAP in reducing blood transfusion requirement, displacement of a significant volume of CPB circuit prime volume is important, as demonstrated by Rosengart et al.
In our prospective observational study, we have demonstrated that practising RAP with mean volumes of 300 ml does not necessarily reduce packed red blood cell transfusion requirements during coronary artery bypass grafting. In our practice, RAP was performed, aiming at displacing a CPB circuit prime volume with which the perfusionist felt comfortable and dictated by haemodynamic parameters prior to commencing CPB. We presume this is the case in many units around the world. This practice, in our opinion, will not be enough to achieve the benefits of RAP in the form of a reduction of packed red cell transfusion requirements. If RAP is to be used effectively, uniformity in practice, with the aim of displacing a minimum volume, is essential if any meaningful benefit is to be demonstrated.
In this study we also observed that there was no significant difference in the percentage reduction of either haemoglobin level or haematocrit at thirty minutes into cardiopulmonary bypass or at the end of cardiopulmonary bypass compared to the corresponding pre-cardiopulmonary bypass levels. This observation shows that retrograde autologous priming in the manner in which it is performed currently in our institute did not affect the haemoglobin or haematocrit level during or soon after cardiopulmonary bypass.
We wish to conclude that a prospective, randomised trial with strict inclusion and exclusion criteria for the patients, guidelines for packed red cell and other blood product transfusion, as well as standards to follow in the conduct of RAP, is necessary. In our opinion, the inclusion criteria should include complex cardiac procedures requiring long bypass times. The potential benefits of RAP in reducing blood transfusion might be more significant in this group of patients. Such a study will help us guide the future practice of RAP in cardiac surgical practice by confirming or refuting the advantages associated with it.
Limitations of the study
Our study has several limitations. Firstly, patients were not allocated to study groups randomly. However, data was collected prospectively on all patients who underwent first-time, non-emergency coronary artery bypass surgery. Secondly, the volume of retrograde autologous priming was not standardised to the bodyweight or body surface area of the patient. This might have affected our observations and conclusions, but also demonstrates that the ad hoc use of RAP alone is of little clinical benefit.
Footnotes
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.