
Abstract
The use of cardioplegia solution has substantially increased the safety of cardiac surgery. It protects the myocardium by inducing a rapid and complete diastolic arrest, minimizing myocardial energy requirements, preventing ischaemic damage during the arrest phase and minimizing or preventing reperfusion injury once coronary blood flow is restored.
This article is a summary of important information that has accumulated in the literature about cardioplegia and describes how our understanding of cardioplegia has evolved. The basic principles of myocardial ischaemia and reperfusion injury and how they relate to myocardial protection are described. Blood and crystalloid cardioplegia are compared with respect to biochemical and physiological differences.
Recent patient demographic changes, with surgeons operating on older, more complex patients who have more severe and diffuse disease, are discussed. This cohort of patients potentially requires prolonged elective ischaemia; hence, improved myocardial protection would be of benefit. We highlight areas of study that have demonstrated a new concept of myocardial protection, known as polarized arrest. Many pharmacological agents have been shown (in experimental studies) to have the ability to induce a polarized arrest and to provide improved protection.
History
Myocardial protection during cardiac surgery has evolved over many years. The development of extracorporeal circulation techniques allowed cardiac procedures to proceed without the threat of haemodynamic collapse. However, performing complicated procedures on the heart was made difficult by its continuous motion. Ischaemia was known, ultimately, to achieve cardiac arrest through the depletion of high-energy phosphate stores, on which cardiac contraction depends. However, myocardial ischaemia led to necrosis and a hypo-contractile, stone heart 1 on reperfusion from which recovery was impossible. Once the limitations of ischaemic (anoxic) arrest were recognized, attempts were made to arrest the heart chemically, in theory, to preserve high-energy phosphate stores lost during ischaemia. Chemical arresting agents were first used by Melrose and associates in 1955. 2 The concept of elective cardiac arrest was soon abandoned in the United States, following reports of high morbidity and pathologic complications in chemically arrested hearts. 3
The use of chemical cardioplegia as a concept was revived in the United States by Tyers et al 4 who found that the constituents in the Melrose formulation were inappropriate rather than the concept of chemical cardioplegia in itself was ineffective. These reports popularized the use of potassium-based cardioplegia to achieve electromechanical arrest.
However, the use of cold cardioplegic solutions only became common practice after the clinical study by Bretscheineder, 5 which stimulated the development of numerous cardioplegic solutions and studies in the 1970s by Roe 6 and Gay and Ebert. 7
In 1978, cold blood cardioplegia was introduced by Buckberg 8 who demonstrated the superiority of this modality over conventional crystalloid cardioplegia, as the presence of blood ensures an oxygen supply to the myocardium and causes less systemic haemodilution. This results in a really effective buffer system as the presence of proteins ensures better control of the oncotic pressure and free radicals. 9 Finally, the last phase in the development of these various myocardial protection techniques was initiated by Braimbridge 10 and consisted of preventing ischaemia by perfusing the coronary arteries throughout the duration of aortic clamping.
Myocardial protection
Protection of the myocardium during cardiac surgery is necessary because of two different forms of injury: ischaemia during cross-clamping of the aorta and a secondary injury during reperfusion after the cross-clamp is removed. A basic understanding of the metabolic and ultra-structural changes that occur during these injury processes is necessary to fully comprehend the current role of cardioplegia in cardiac surgery.
Myocardial ischaemia
Severe hypoxaemia during myocardial ischaemia results in the following series of reactions: rapid cellular conversion from aerobic to anaerobic metabolism, high energy phosphate (i.e., adenosine diphosphate and adenosine triphosphate (ADP, ATP) 0 depletion and intracellular acidosis which causes loss of normal trans-membrane ionic homeostasis. An influx of calcium results in intracellular calcium ion deposition and phosphate crystals. Superoxide free radicals are produced, which has deleterious intracellular effects and is thought to act as a neutrophil chemo-attractant and causes membrane disruption that may be responsible for deposition of complement. This facilitates neutrophil adhesion to ischaemic endothelium.
The protective effects of free radical scavenging enzymes are lost. Adenine nucleotides, endothelial-derived relaxation factor and prostacyclin levels are depleted. The resulting effect is impaired cell ability to regulate microvascular vasomotor tone and explosive myocardial swelling.
Reperfusion
The pathogenesis of reperfusion injury is multifactorial. 11 Due to the loss of protective free radical scavenging enzymes, the cell is vulnerable to oxidant injury during the burst of free radical production during reperfusion. As a result of increased washout of adenosine, cyclic adenosine monophosphate (AMP), endothelial-derived relaxation factor and prostacyclin, the loss of vasodilatory reserve is augmented and the neutrophil accumulation is increased during reperfusion. Other granulocyte-related mechanisms that could be involved in myocardial reperfusion injury include significantly increased neutrophil adherence with the release of potent proteolytic enzymes, vasoactive substances and free radicals and capillary plugging by the granulocytes themselves. Continued neutrophil-endothelial interactions result in the loss of the structural integrity of the endothelium. The limitation of anaerobic ATP production leads to increased cell membrane permeability to calcium, causing intracellular calcium to increase. Longer periods of ischaemia followed by normo-calcaemic reperfusion may cause massive cellular calcium deposits, myocardial contracture and irreversible damage that results in cell death.
Physiology of cardioplegic arrest
The high potassium concentration present in most cardioplegic solutions decreases the membrane resting potential of cardiac cells. The normal resting potential of ventricular myocytes is approximately -90mV.
When extracellular cardioplegia displaces the blood surrounding the myocytes, the cell depolarizes more readily, i.e. at a less negative membrane potential. The depolarization causes contraction, intracellular calcium is sequestered by the sarcoplasmic reticulum via ATP-dependent calcium pumps and the cell relaxes (diastole). However, the high potassium concentration of extracellular cardioplegia prevents re-polarization. Raising the potassium concentration to 16.2 mmol/L raises the resting potential to -60mV, a level at which muscle fibres are inexcitable to ordinary stimuli. When the resting potential approaches -50mV, sodium channels are inactivated, resulting in a diastolic arrest of cardiac activity.
Composition of cardioplegia solutions
Cardioplegia solutions are essentially made up of chemical components that cause diastolic arrest and additives that help minimise myocardial energy requirements. These components are delivered by a vehicle, i.e. crystalloid or blood.
Discussed below is the molecular and cellular impact these vehicles have on myocardial protection and prevention of reperfusion injury at different physiological conditions.
Physiologic basis for crystalloid and blood cardioplegia
Oxygen delivery
At normothermia, haemoglobin carried by red blood cells provides an effective system for delivery of oxygen to the tissues, but, as the temperature is reduced, the oxy-haemoglobin dissociation curve shifts to the left so that oxygen is less readily available and requires increasingly reduced tissue oxygen tension before oxygen is released. At 20°C, blood cardioplegia releases 50% of its total oxygen content and, at 10°C, only 37% to 38%, in contrast to oxygenated crystalloid cardioplegia which releases all of its oxygen at either temperature.
These facts have led to the conclusion that blood cardioplegia does not effectively deliver oxygen to the myocardium during hypothermic arrest. On the other hand, there is little doubt that some myocardial uptake of haemoglobin-bound oxygen occurs during hypothermic blood arrest using blood cardioplegia. 12 The release of haemoglobin-bound oxygen causes mild myocardial acidosis that develops during blood cardioplegia arrest. This results in local red blood cell acidosis, with a shift to the right of the oxy-haemoglobin dissociation curve (Bohr effect). Additionally, hypothermia results in a greater tissue affinity for oxygen. Others have not found un-favourable oxy-haemoglobin dissociation kinetics at temperatures of 30°C 13 and 20°C. 14 The potassium-paralyzed heart maintained at 22°C has a myocardial oxygen consumption (MVO) of 0.3 mL/100 g/minute 15 and, when the temperature is reduced to between 10°C and 12°C, the MVO is 0.135 mL/100 g/min. 16 Experimental studies conducted at a myocardial temperature of 27°C indicated that haemoglobin-mediated oxygen delivery to the myocardium was important for cardioplegic myocardial preservation. 17 When myocardial temperature was reduced to between 10°C and 12°C, haemoglobin transport of oxygen was not critical to myocyte preservation provided the cardioplegia solution was fully oxygenated and at 4°C. Blood was associated with reduced preservation of left ventricular function despite more oxygen delivery with blood than with crystalloid. Either vehicle (blood or crystalloid) will carry more dissolved oxygen as the temperature is lowered to 4°C and the solution fully oxygenated. The studies cited above have many variables, but, in aggregate, they indicate that haemoglobin-mediated delivery of oxygen during blood cardioplegia becomes less important as the myocardial temperature is reduced to between 5°C and 20°C, where oxygen requirements are small and dissolved oxygen can meet these needs.
With regard to the issue of whether oxygen delivery is necessary for the success of blood cardioplegia, it has been clearly demonstrated in a recent report that this component is necessary for optimal myocardial protection by comparing three levels of oxygen content (1.1, 4.3 and 10.2%), with a cardioplegic temperature of 4°C and a myocardial temperature of 10°C to 12°C.
Buffering capacity
Buffering capacity of blood is primarily a function of the histidine component of plasma proteins and haemoglobin. Haemoglobin has approximately six times the buffering capacity of the plasma proteins in blood due to its high concentration.
A further contribution to the effectiveness of haemoglobin as a blood buffer is the fact that deoxygenated haemoglobin has imidazole groups with a somewhat higher pH than oxygenated haemoglobin. Thus, once haemoglobin becomes deoxygenated in the capillaries, it is better able to bind the hydrogen ions that diffuse into the red blood cells from the tissues or are formed when carbon monoxide (CO) enters the red blood cells from the tissues. Another mechanism for tissue buffering which also facilitates oxygen delivery is through the activity of red blood cell carried carbonic anhydrase, which catalyzes the reaction creating bicarbonate (HCO) a weak acid that ionizes to H+ and HC0-, lowering red cell pH. The increase in hydrogen ion concentration decreases the oxygen affinity of the haemoglobin (Bohr effect) and facilitates oxygen delivery to the tissues. The increased HC0- ions diffuse out of the red cell and are replaced by chloride ions (chloride shift). The removal of CO creates a gradient with the tissues and promotes diffusion of CO from the myocytes across the freely permeable sarcolemma. Although the same reaction of CO with water occurs in the plasma and tissues, the rate is much slower, thereby, limiting the formation of cellular H+ and consequent tissue acidosis.
Other major sources of hydrogen ion accumulation in the ischaemic myocyte are from the hydrolysis of adenosine triphosphate and from the accumulation of lactic acid during anaerobic glycolysis. Myocardial pH and the pH of the coronary venous effluent are indicative of the degree of tissue acidosis and correlate with other indicators of the adequacy of myocardial preservation during cardioplegia
Free radicals
There is increasing evidence that oxygen free radicals contribute to the myocardial damage occurring with ischaemia and reperfusion. 18 Superoxide appears to be generated by the enzyme xanthine oxidase, which is synthesized as xanthine dehydrogenase and converted to the former in ischaemic tissue. Superoxide dismutase, a ubiquitous mammalian enzyme, can dis-mutate the superoxide anion to hydrogen peroxide; catalase and glutathione peroxidase catalyze reactions that reduce hydrogen peroxide to water and oxygen. The major danger of superoxide anion and hydrogen peroxide accumulation is the potential for the production of hydroxyl radicals (OH) through the Haber-Weiss and Fenton reactions. Allopurinol, which can block xanthine oxidase and mannitol, which can react with the hydroxyl radical, has been of demonstrated value in reducing injury where there was potential for free radical generation. In addition to the protective mechanisms already mentioned, human plasma has free radical-trapping antioxidant activity provided by urate (35% to 65%), plasma proteins (10% to 15%), ascorbate (0% to 24%) and vitamin E (5% to 10%). Vitamin E (a-tocopherol) is the only lipid-soluble antioxidant in the plasma and is, therefore, able to trap peroxyl radicals present in or at the interface of the lipid phase. Vitamin C (water soluble) appears to be the only plasma antioxidant capable of regenerating vitamin E from the a-tocopherol radical. Thus, human plasma is highly resistant to peroxidation.
Experimental studies of free radicals in cardioplegia 19 have centred on global and regional ischaemic and crystalloid cardioplegia, with a single report of free radical injury related to blood cardioplegia. 20 In addition to the antioxidants contained in plasma, red blood cells contain catalase, superoxide dismutase and glutathione, all of which participate in reactions to scavenge free radicals. Glutathione is synthesized in red blood cells and is mostly present in the reduced form; it may be important in the detoxifying of hydrogen peroxide through glutathione peroxidase, with the oxidation of glutathione which, in turn, is rapidly reduced by glutathione reductase. Although blood appears attractive from the standpoint of inherent mechanisms for the prevention of free radical generation and chain-breaking of their effects, it must be recognized that this whole phenomenon remains largely unexplored, particularly in a quantitative sense
Adjuncts in cardioplegia
Calcium entry blockers
Extensive laboratory evaluation of calcium entry blockers has revealed that they alone may be as effective as potassium cardioplegia, whether delivered in a vehicle based on crystalloid or blood. 21 Several investigators have found that a combination of hyperkalaemia and calcium entry blockade may provide better myocardial protection than either alone when used with crystalloid or blood cardioplegia. 22 They found that diltiazem was associated with the preservation of high-energy phosphates, improved postoperative myocardial metabolism and reduced ischaemic injury after elective coronary bypass. However, diltiazem was a potent negative inotrope and produced prolonged periods of electromechanical arrest, with the requirement for atrioventricular sequential pacing to discontinue cardiopulmonary bypass in all patients. When diltiazem was added to blood potassium cardioplegia, there was increasing time to atrioventricular function as the dose of diltiazem was increased.
Diltiazem at a dose of 100ng/kg (for each of three infusions) was associated with a reduction in peak creatinine kinase-MB (CK-MB) release. On the basis of these two reports, it is concluded that the risks of atrioventricular blockade and depressed ventricular function are of sufficient concern to outweigh the benefits achieved. Verapamil (0.1 mg/kg up to 10 mg), given systemically before aortic cross-clamping and cold blood potassium cardioplegia, was associated with lower CK-MB release compared with controls.
Local anaesthetics
Procaine has been added to crystalloid cardioplegia for membrane stabilization or used as an isolated cardioplegia agent, but has not been used in blood cardioplegia. Hypersensitivity or allergy may occur with ester-linked agents such as procaine, whereas amide-linked local anaesthetics, such as lidocaine, are singularly free of this complication. Adding lidocaine (0.1 mg/mL) to blood cardioplegia was associated with a spontaneous return of sinus rhythm in 74% of patients versus 22% of controls. 23 Left ventricular function was minimally depressed 30 minutes after reperfusion, but this effect was transient and of no clinical importance.
New advances: five decades of searching for alternatives to depolarizing potassium
Depolarizing potassium solutions remain the standard of care for cardioplegic arrest in cardiac surgery today.(Figure 1)
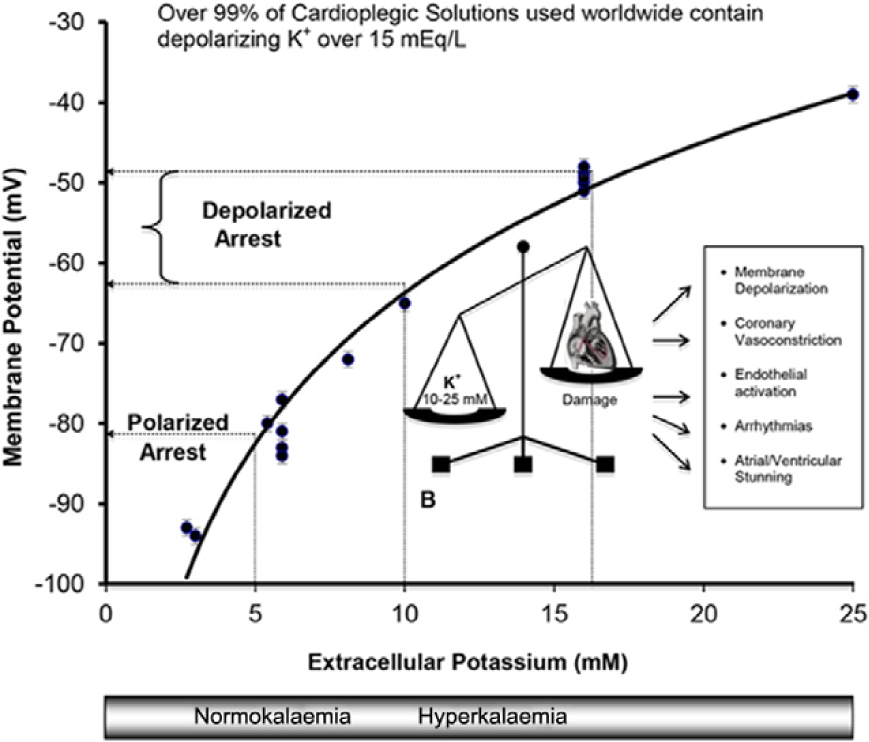
Highlights the detrimental cardiac effects of depolarizing hyperkalaemic arrest.
An alternative to inducing depolarized arrest by hyperkalemia is to induce a hyperpolarized or polarized arrest. This can be achieved by using specific agents that target the cellular components indicated in Figure 2 to induce arrest at membrane potentials closer to the normal resting membrane potential.
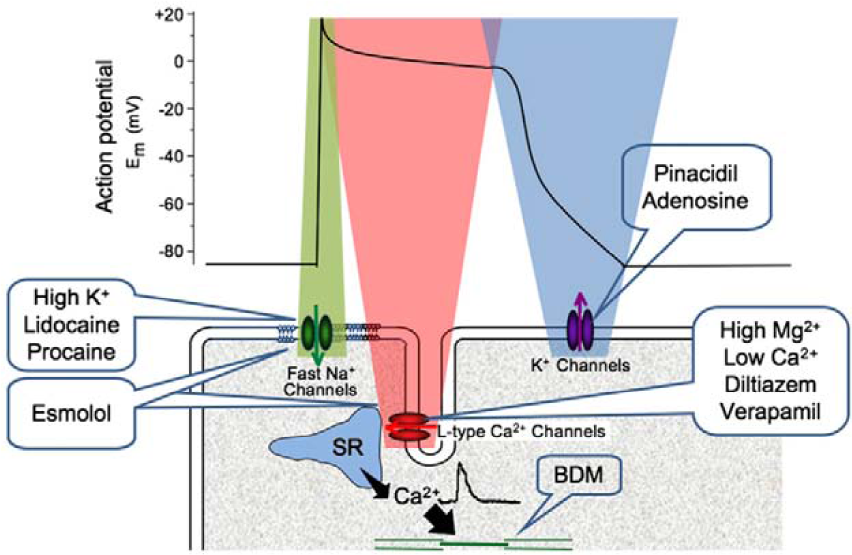
The cellular targets for cardioplegic arrest and their influence on the action potential with examples of pharmacological agents.
A number of benefits should ensue; these include a reduced ionic imbalance, leading to reduced energy utilization and, hence, improved protection from a cellular perspective hyperpolarization/polarization (potassium channel openers).
The adenosine triphosphate-sensitive potassium channel (KATP channel) appears to have a role as a metabolic sensor, linking cytosolic energy metabolism to membrane electrical activity in response to stress such as ischaemia–reperfusion. High (millimolar) concentrations of KATP channel-opening drugs can induce arrest by maintaining hyperpolarization. KATP channel openers are also potent vasodilators, inducing hyperpolarization on vascular smooth muscle cells, 24 with some evidence that a ‘hyperpolarizing’ cardioplegia protects endothelial function compared to a hyperkalaemic ‘depolarizing’ cardioplegia.
Using isolated rabbit sino-atrial (SA) node cells, adenosine (an endogenous purine nucleoside) was shown to induce complete arrest (at 50 μmol/L) and a hyperpolarization of ∼12 mV via increased membrane potassium permeability. It appears to act via an adenosine receptor-activated potassium channel and, hence, could have similar effects to KATP channel openers. This cardioplegic property has been extended to whole hearts, with adenosine used either as an arrest agent (albeit at a high concentration of 10 mmol/L) or as an additive (at 1 mmol/L) to hyperkalaemic solutions; the addition of adenosine reduced the time to arrest and improved post-ischaemic recovery of function compared to hyperkalaemic cardioplegia alone.
Endogenous cardioprotective strategies, termed pre-conditioning and post-conditioning, may have a role in cardiac surgery to provide additional protection. Details of both these strategies have been the subject of many recent reviews. 25 The elective nature of cardiac surgery, with the known onset of ischaemia and reperfusion, lends it to the potential of these strategies. Ischaemic pre-conditioning involves one or more brief episodes of ischaemia followed by reperfusion prior to a prolonged ischaemia and induces a complex cascade of intracellular signalling mechanisms that protect the myocardium from the potentially lethal prolonged ischaemic duration. Similarly, various pharmacological agents can also induce these mechanisms. Recently, remote pre-conditioning (involving pre-conditioning another organ to remotely benefit the heart) may offer potential in the clinical arena. The use of limb ischaemia to activate hormonal and/or neural stimulation may be particularly relevant. However, large scale randomized clinical trials will be needed to confirm the potential of this interesting technique. The phenomenon of post-conditioning, whereby multiple short episodes of reperfusion and ischaemia at the start of reperfusion improves protection, is also a recent development.
Conclusion
Since the beginning of cardiac surgery in the early 1950s, it has been recognized that protection of the heart was a fundamental requirement to counteract the imposed elective global ischaemia used by the surgeon to provide optimal operating conditions. It took about 25 years to develop a consensus method; this was based around a moderate increase in extracellular potassium and these hyperkalaemic cardioplegic solutions provided good myocardial protection, which was relatively safe and easily and rapidly reversible.
This technique induces a depolarized arrest and has been the cornerstone of cardiac protection (albeit with a number of minor alterations - crystalloid or blood solutions, hypothermic or warm, with or without various additives) for over 30 years. However, during this time, the characteristics of patients who currently undergo cardiac surgery compared to those receiving operations 20-30 years ago have changed considerably. Patients are significantly older and have more severe and diffuse disease, as well as the increasing strategy of operating on high-risk patients with heart failure or acute coronary syndrome. The requirement for optimal, or improved, myocardial protection has never been greater, but this is unlikely to be achieved with current hyperkalaemic solutions. New concepts relating to myocardial protection may provide these improvements; these concepts need further examination and investigation to challenge the traditional view that hyperkalaemic arrest is best.
Footnotes
Declaration of Conflicting Interest
The authors have no conflicts of interest to declare
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.