
Abstract
Objective:
Acute mesenteric ischemia (AMI) is an infrequent, but complicated, life-threatening condition. Given this poor outcome, an estimation of mortality would aid in decision making for physicians, patients and their families. Red cell distribution width (RDW) is reflective of systemic inflammation. RDW is a remarkable prognostic marker for determining the risk of mortality in a wide range of clinical manifestations. The objective of this study was to investigate the association between RDW and mortality in patients with AMI.
Methods:
The medical records of patients who underwent laparotomy with a preoperative diagnosis of AMI were reviewed retrospectively. Primary outcome variable was the hospital mortality rate.
Results:
Estimating the receiver operating characteristic area under the curve showed that RDW has good discriminative power for mortality (area under the curve = 0.713; 95% confidence interval, 0.584–0.841). With a cut-off value of 14.85 for RDW, mortality could be correctly predicted in approximately 70% of cases.
Conclusions:
Increased RDW at admission was a predictor of the extent of necrosis and mortality in AMI patients. Further prospective studies are necessary to more accurately assess the importance of RDW in these patients.
Introduction
Acute mesenteric ischemia (AMI) is an infrequent, but complicated, life-threatening condition. It is mostly seen in elderly patients. Despite the advances in diagnosis of AMI, morbidity and mortality rates remain high. 1 Early identification of patients at greater risk of mortality may determine a more rational use of diagnostic studies and prompt early institution of interventional or medical treatment, leading to decreased mortality rates and an estimation of mortality would aid in decision making for physicians, patients and their families.1,2
Red cell distribution width (RDW) is a quantitative measure of variability in the size of circulating erythrocytes. RDW is an easy, inexpensive, routinely reported parameter as a part of the complete blood count test used in the assessment of the patient’s disorder. Recent studies have shown that RDW is a remarkable prognostic marker to determine the risk of mortality in a wide range of clinical manifestations, such as community-dwelling older adults with or without age-associated diseases, critically ill patients, intensive care unit patients, acute dyspnea, community-acquired pneumonia and acute pancreatitis.3-10
The aim of this study was to examine whether RDW on admission could be a predictor of prognosis in patients with AMI.
Material and Methods
The study was designed as a retrospective cohort study. The medical records of patients who underwent laparotomy for suspected AMI between January 2008 and December 2011 were reviewed according to International Statistical Classification of Diseases and Related Health Problems (10th revision) codes. Preoperative diagnosis was based on a combination of clinical evaluation, biochemical tests and radiological studies. Biochemical tests (complete blood count, hepatic function, renal function, amylase, lipase and arterial blood gas) were performed in each patient with clinically suspected AMI. RDW was routinely measured as part of the automated complete blood cell count using a hematology analyzer (Coulter Hmx; Beckman Coulter [UK] Ltd, High Wycombe, Bucks, UK). The reference range for RDW at our institution was 11.5% to 14.5%. Unless contraindicated, all patients underwent contrast-enhanced abdominal computed tomography scans. Ultrasonography and direct abdominal radiography were also used for diagnosis on admission. Conventional computed tomography was primarily used for the final diagnosis. Appropriate resuscitation with fluid-electrolyte replacement was considered preoperatively on an individual basis. Anticoagulant therapy administered subcutaneously was routinely started in all patients.
All operations were performed under general anesthesia. A midline incision was preferred for explorative laparotomy in all cases.
According to the operative findings and procedure, “massive intestinal resection” was defined as the resection of small bowel in-between the proximal 30th–40th cm of the jejunum and the middle of the transverse colon, whereas “open and closed laparotomy” was defined as the necrosis of entire bowel segments from the duodenojejunal junction to the transverse colon. Other resections performed during surgery were defined as “limited resections”.
Outcome variables were the extent of intestinal necrosis and the in-hospital mortality rate.
Statistical analyses
Data were tested for normality and were found to be non-normally distributed. Accordingly, continuous data are presented as median value and interquartile range (IQR), with non-parametric analyses being used to assess differences. The Mann-Whitney U test and χ2 test were used to assess differences when appropriate.
We measured the prognostic performance of the RDW using receiver operating characteristic curves and calculated sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (+LR) and negative likelihood ratio (−LR) for different cut-off values.
All statistical procedures were performed with SPSS 15.0 (SPSS Inc, Chicago, Illinois). p<0.05 was considered significant.
Results
The median age of the patients was 72 (IQR, 64–78) years (range, 40–91 years). There were 36 men (59%) and 25 women (41%). The clinical characteristics of the overall study group are listed in Table 1. Hypertension (41 patients) was the most common comorbidity, followed by ischemic heart disease (32 patients), atrial fibrillation (21 patients) and diabetes mellitus (12 patients).
Summary of the demographic and clinical characteristics of the study group. Data are presented as median value (interquartile range).
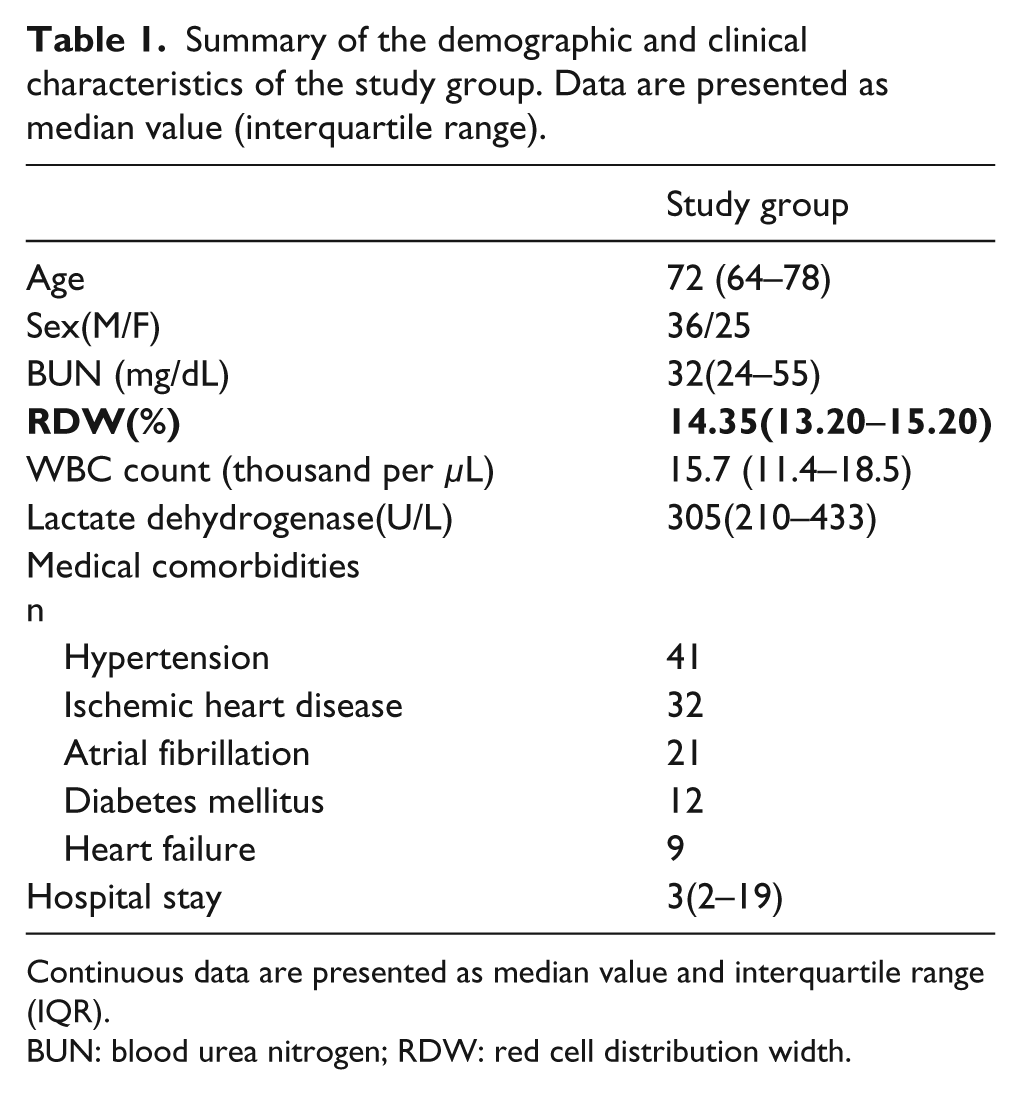
Continuous data are presented as median value and interquartile range (IQR).
BUN: blood urea nitrogen; RDW: red cell distribution width.
All of the patients with AMI underwent surgery; 18 underwent massive intestinal resection, 35 underwent limited large/small bowel resection and 8 underwent open and closed laparotomy. The median RDW was 15.65 (IQR, 14.85–16.40) in the open and closed laparotomy group and was 15.05 (IQR, 14.0–15.40) in the massive resection group. The difference between the two groups was not significant. On the other hand, the median RDW in the limited resection group [13.40 (IQR, 13.0–14.60)] was significantly lower than that in the other groups (p = 0.01)
Thirty-five (57.4%) patients died. The median RDW was significantly greater in non-survivors than in survivors [14.60 (IQR, 13.40−15.90) versus 13.25 (IQR, 12.70–14.70); p = 0.005]. All eight patients in the open and closed laparotomy group died. Nine patients (50%) died in the massive resection group. The median RDW in the massive resection group was not significantly different between the survivors and non-survivors [15.10 (IQR, 14.40–15.40) versus 14.70 (IQR, 13.30–15.30)]. Eighteen patients (51.84%) died in the limited resection group. The median RDW in the limited resection group was not significantly different between the survivors and non-survivors [13.40 (IQR, 12.30−13.60) versus 13.80 (IQR, 13.20−15.20)].
Receiver operating characteristic curves were plotted for RDW to identify non-survivors, with a statistically significant area under the curve of 0.713 (95% confidence interval, 0.584–0.841) (Figure 1). We also calculated the PPV, NPV, +LR, and −LR for RDW at a cut-off value of 14.85, which predicted mortality in approximately 70% of patients (Table 2).
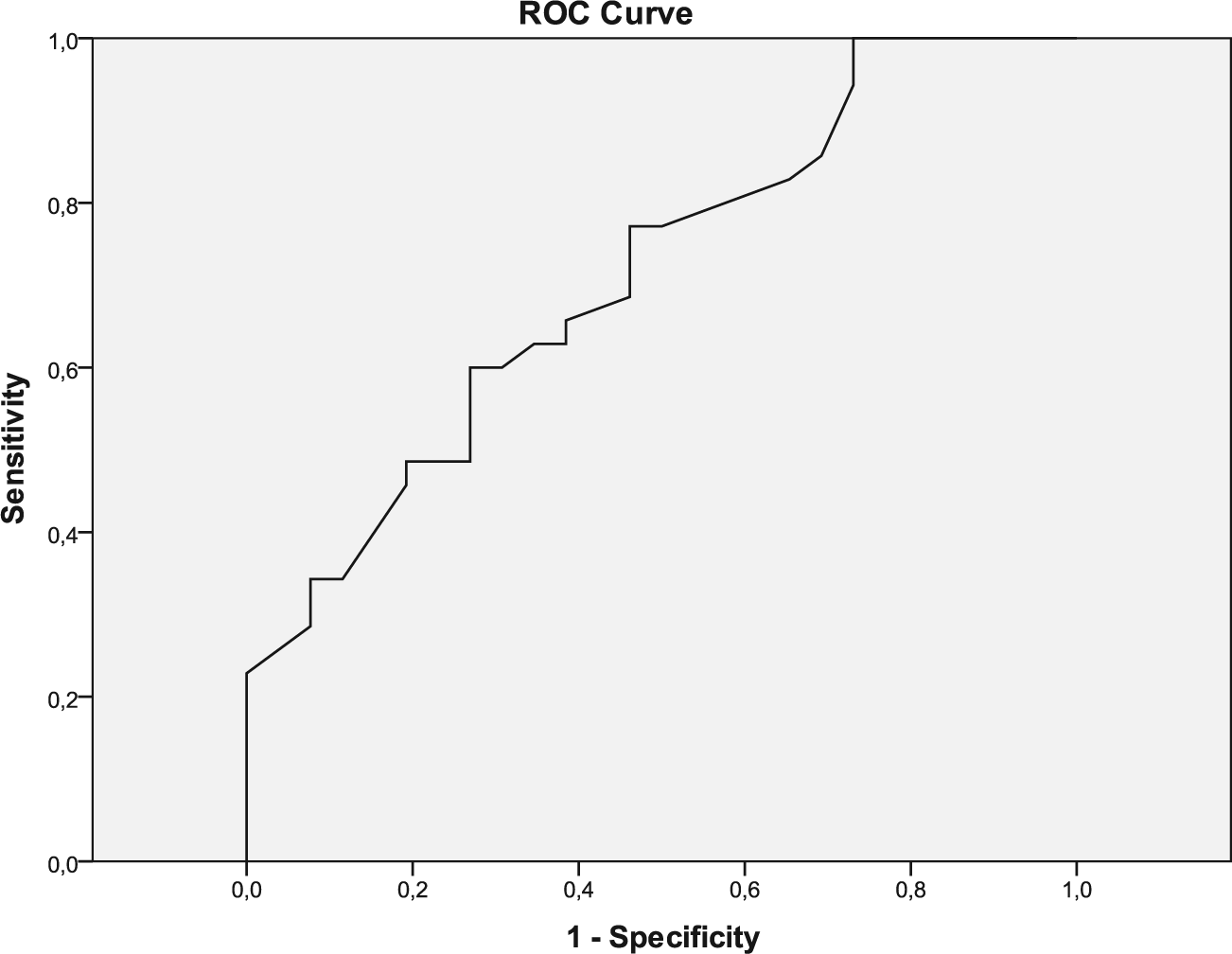
Receiver operating characteristic curves of RDW for mortality.
Sensitivity, Specifity, +LR and –LR, Positive Predictive Value, Negative Predictive Value of RDW for mortality at optimal cut-off level.

+ LR indicates positive likelihood ratio; – LR, negative likelihood ratio.
Receiver operating characteristic curves were also plotted for RDW to identify patients undergoing open and closed laparotomy or massive resection, yielding a statistically significant area under the curve of 0.769 (95% confidence interval, 0.648–0.890) (Figure 2). The PPV, NPV, −LR, and +LR for RDW at a cut-off value of 14.90 are summarized in Table 3.
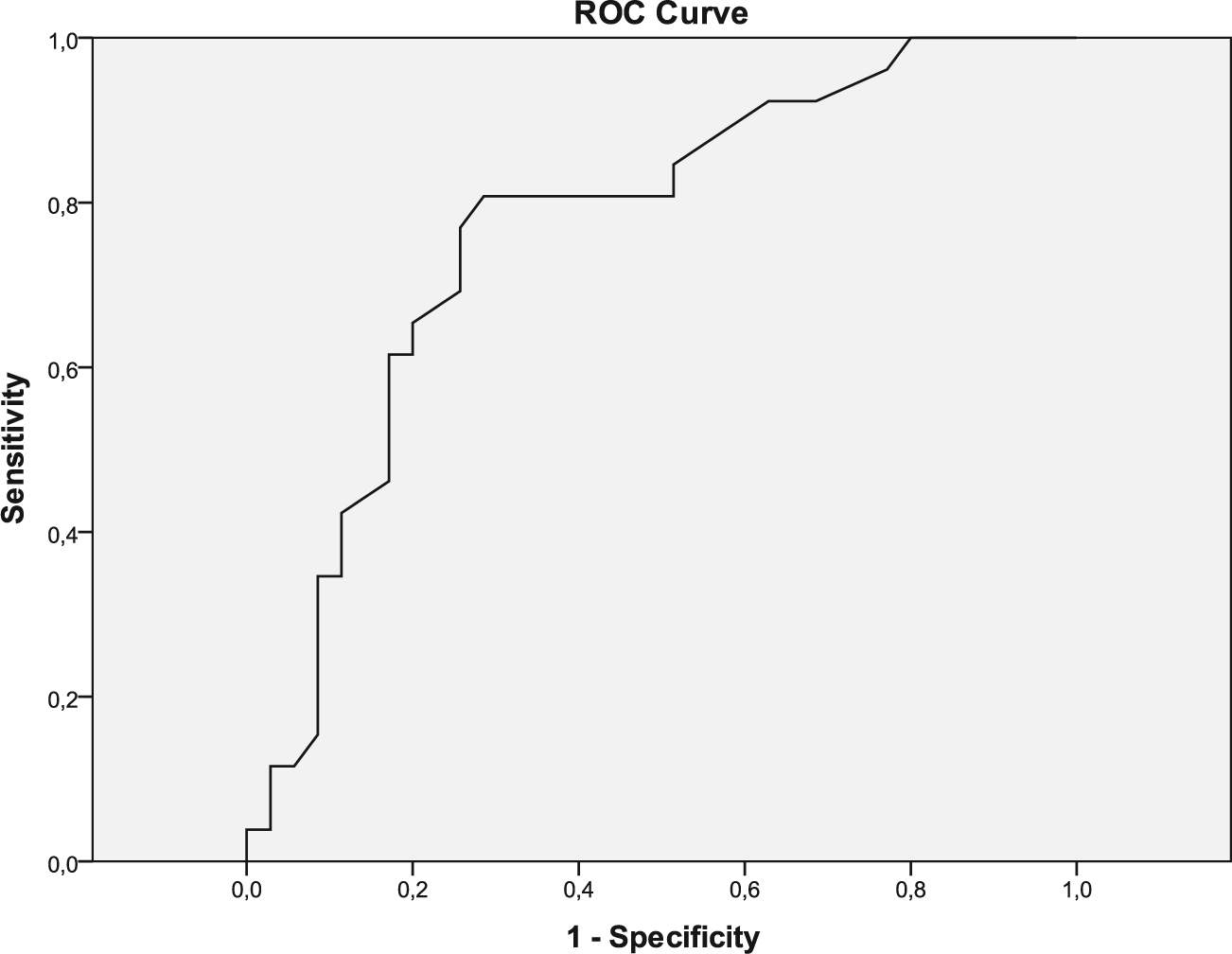
Receiver operating characteristic curves of RDW for extent of necrosis.
Sensitivity, Specifity, +LR and –LR, Positive Predictive Value, Negative Predictive Value of RDW for extent of necrosis at optimal cut-off level.

Discussion
AMI is a catastrophic illness and has a poor outcome. 2 Despite advances in diagnostic and therapeutic modalities and better understanding of the pathophysiology of the disease, there has been minimal improvement in outcomes of patients with AMI. 1
In our study, the hospital mortality rate was 57.4% in patients who underwent surgery for AMI. This compares with the higher mortality reported in single-center studies.1,11
Age is known to be associated with poor prognosis in patients undergoing bowel resection for AMI. In addition, a preoperative do not resuscitate order was associated with the largest risk for postoperative mortality. 2 Preoperative RDW levels in these patients may predict the overall risk so that appropriately selected patients can undergo surgery with a reasonable mortality risk.
Preoperative sepsis, cardiac disease and higher ASA (American Society of Anesthesiologists) class are associated with increased mortality. Mortality in these patients approached 50%.2,11 On the other hand, the relationship between type of resection (creation of ostomy vs. primary anastomosis) and mortality is not clear.1,2,11 Gupta et al. developed a mortality risk calculator for AMI patients. Pre- and intraoperative variables significantly associated with postoperative mortality included preoperative do not resuscitate order, open wound, low albumin, dirty vs. clean contaminated case and poor functional status. The area under the curve for the mortality model was 0.837. 2 In order to simplify the risk calculation for prediction mortality in AMI patients preoperatively, the discovery of a novel method, such as a laboratory test, might be useful.
In this study, we showed that preoperative RDW levels predict mortality and the extent of disease in AMI patients. According to our literature review, this is the first study about this subject.
Correlations between RDW and other inflammatory markers have been reported. For example, Lippi et al. reported that RDW was associated with two widely used inflammatory biomarkers: C-reactive protein levels and the erythrocyte sedimentation rate. 12 In another study, Jo et al. reported that elevated RDW was associated with pro-inflammatory cytokines, including interleukin-6 and tumor necrosis factor levels. 13 Meanwhile, Cakal et al. reported that elevated RDW was correlated with C-reactive protein levels, the erythrocyte sedimentation rate, fibrinogen levels and the platelet count in patients with active ulcerative colitis. 14
The pathophysiologic mechanisms for the association between higher RDW and mortality or the extent of necrosis in AMI patients are unclear. The major causes of death in AMI patients are the development and progression of ischemia/reperfusion injury, including the adhesion and activation of polymorphonuclear neutrophils, the release of pro-inflammatory cytokines, as well as the formation of reactive oxygen species and reactive nitrogen species. 15 Inflammation influences bone marrow function and iron metabolism and inflammatory cytokines suppress erythrocyte maturation, accentuated with sepsis, allowing newer, larger reticulocytes to enter the circulation, which is associated with RDW increase. 5 High oxidative stress can also lead to elevated RDW by reducing red blood cell (RBC) survival and the increasing release of large premature RBCs into the peripheral circulation. In addition, inflammation alters RBC membrane glycoproteins and ion channels which contribute to the change of RBC morphology.16,17
There are several limitations to this study. Our study was mainly limited by the retrospective nature and the small number of patients. Second, a heterogeneous group of patients were analyzed in a single center, so selection bias was inevitable. Further controlled and well-designed prospective studies with larger patient populations, involving multiple centers, are necessary to more accurately assess the importance of RDW in AMI patients.
Conclusion
Increased RDW at admission may be a predictor of the extent of necrosis and mortality in AMI patients. Clinicians can use increased RDW as a prognostic marker for AMI patients and should pay additional attention to patients with increased RDW.
Footnotes
Declaration of Conflicting Interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.