
Abstract
Aim:
The retina and ocular vasculature are vulnerable to alterations in systemic hemodynamics, such as in open heart surgeries. Our aim was to investigate retinal vascular caliber (RVC), ocular pulse amplitude (OPA), peripapillary retinal nerve fiber layer (RNFL) and macular thickness in coronary artery bypass grafting (CABG) surgery patients.
Methods:
Twenty-six patients who had a history of CABG surgery and 26 age-sex-matched healthy participants were recruited for this prospective, cross-sectional and comparative study. The RVC, peripapillary RNFL and macular thickness measurements were taken with spectral-domain optical coherence tomography. The OPA, a surrogate of pulsatile ocular blood flow, was measured with the Pascal dynamic contour tonometer.
Results:
There were no statistically significant differences between the CABG surgery patients and the controls with regard to RVC, OPA, peripapillary RNFL thickness and macular thickness measurements (p>0.05).
Conclusions:
CABG surgery does not affect retinal structures and pulsatile ocular blood flow in the long-term follow-up.
Keywords
Introduction
Coronary artery bypass grafting (CABG) surgery is a cardiac operation in which vessels from the patient’s body are grafted to the coronary arteries to bypass atherosclerotic narrowing in order to improve the blood supply to the ischemic part of the heart muscle. 1 New developments and techniques in cardiac surgery have given the opportunity of performing less complicated CABG surgery. 2 Due to the rapid increase in the number of heart surgeries performed in the last few years, the possibility of various end-organ complications, including brain and eyes, also increases.
The most common mechanisms of visual pathway and ocular disease formation after CABG surgery are considered to be retinal microemboli, occipital infarct and ischemic optic neuropathy (ION). 3 The previous reports in the literature about blindness after CABG surgery mostly addressed ION as the most important etiologic factor.3,4 In cardiac surgical patients, additional risk factors of ION are hyperglycemia, hypertension, prolonged hypotension, vasospasm secondary to inotropes and anemia.4,5
Since the main reason of ocular problems after CABG surgery is decreased blood flow to the eyes and visual pathways, this condition might cause atrophy of the retina, choroid and optic nerve, as well as alterations in retinal vasculature. In this study, we aimed to reveal these effects by performing retinal vascular caliber (RVC) measurements, peripapillary retinal nerve fiber layer (RNFL) analysis, macular thickness analysis and ocular pulse amplitude (OPA) measurements.
Subjects and Methods
Twenty-six patients who had a history of CABG surgery and 26 age-sex-matched healthy participants were included in this prospective, cross-sectional, comparative study. The patients were first seen in the cardiology clinic and then referred to our eye clinic. All participants underwent an ophthalmic examination, including visual acuity assessment, biomicroscopy, air-puff tonometer, indirect retinoscopy, intraocular pressure (IOP) and ocular pulse amplitude measurements, retinal vascular caliber, peripapillary retinal nerve fiber layer and macular thickness analysis. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and was approved by the Institutional Ethical Committee.
Study Population
One of the eyes of each subject was included randomly. All the eyes had 20/30 or better Snellen chart best-corrected visual acuity. Exclusion criteria were any ocular surgery history and having ocular diseases that were diagnosed before CABG surgery. None of the patients had an ocular disease other than low-grade, age-related cataract. Patients having other possible causes of reduced thickness of the peripapillary retinal nerve fibers, such as optic disc drusen and previous retinal artery occlusion, were excluded. None of the participants were using ocular medications, including antiglaucomatous drugs. Patients had refractive errors between -1.50 and +1.50 diopters spherical equivalent. Higher ametropies were excluded. Systemic diseases, such as diabetes mellitus and systemic hypertension, that might affect ocular structures were also excluded.
All of the patients in the study group had undergone on-pump CABG surgery. The time interval between the heart surgeries and ocular examinations ranged between 1 – 20 years. Ejection fraction was >40% for all the CABG surgery patients. None of the patients was using positive inotropic agents. None of the CABG surgery patients had a history of poorly controlled arterial hypertension and visual problems before and after the surgery.
Measurement Techniques
Spectral-domain optical coherence tomography (Spectralis, Heidelberg, Germany) was used for RVC, peripapillary RNFL and macular thickness measurements. This is a non-invasive, non-contact, transpupillary imaging device for investigating fine retina-choroidal structures. For RVC analysis, the three largest retinal arterioles and venules passing through an area of one-half to one-disc diameter from the optic disc margin were measured (Figure 1). The mean thickness values of the retinal vessels were calculated for each subject and recorded for analysis. For macula analysis, only central macular thickness was assessed. For peripapillary RNFL analysis, the thicknesses of all the quadrants (superior, inferior, temporal and nasal) were recorded separately.
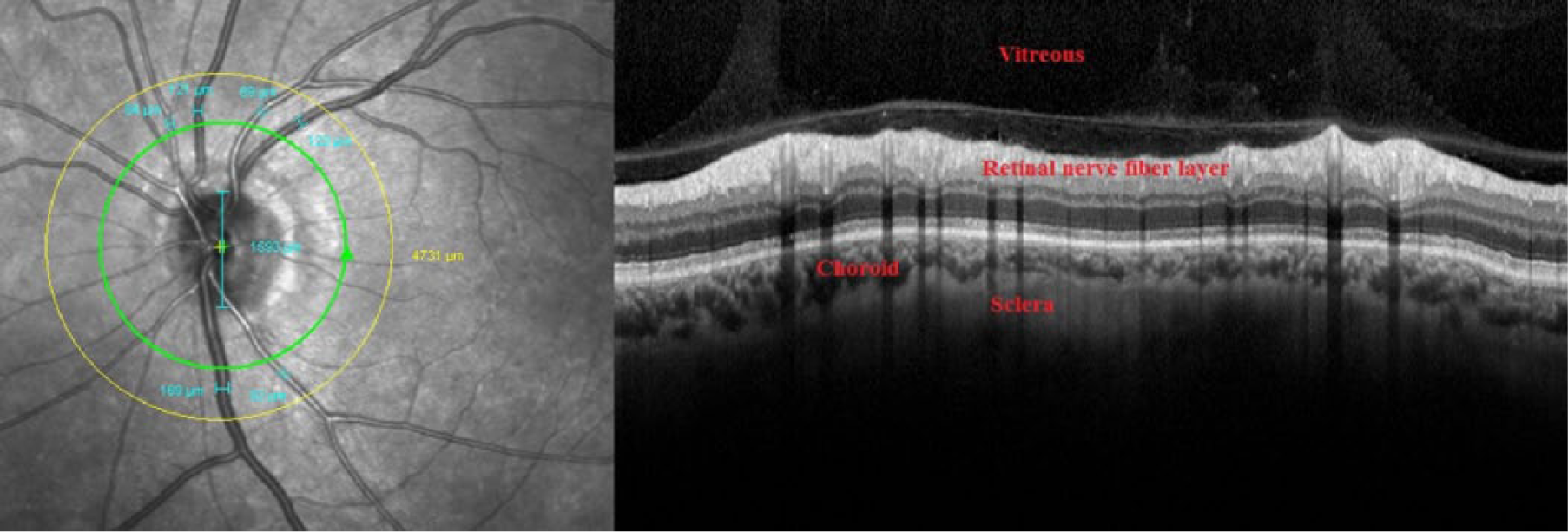
Technique for retinal vessel caliber measurements and related images of posterior pole ocular structures are shown.
The OPA and IOP measurements were done with the Pascal dynamic contour tonometer (Pascal DCT, Swiss Microtechnology AG, Port, Switzerland). This is a slit-lamp biomicroscopy mounted, self-calibrating, 7-mm tip diameter and 1.2-mm pressure sensor diameter device. Three DCT measurements were taken in order to have one good quality measurement. Only quality 1 and 2 measurements were taken into consideration.
Statistical Analysis
For statistical analysis, SPSS 17.0 software for Windows (SPSS Inc., Chicago, IL, USA) was used to analyze the outcomes. ‘P’ values lower than 0.05 were considered to be statistically significant. The Mann-Whitney U test was used for comparison of RVC, OPA, peripapillary RNFL and macular thickness measurements between the study group and the control group. Pearson correlation analysis was used to examine the relationship between retinal arteriole caliber, OPA and the time interval between CABG surgery and the ocular examinations.
Results
Some of the demographic and clinical properties of the patients are shown in Table 1. The mean time interval between CABG surgery and eye examinations was 6.6 ± 5.3 (range: 1-20) years in the study group. Figure 2 is the scatter plot graphic showing the correlation of OPA and the time interval between CABG surgery and ocular examinations (p=0.35, r=−0.19). Figure 3 is the scatter plot graphic showing the correlation of retinal arteriolar caliber and the time interval between CABG surgery and ocular examinations (p=0.99, r=0.001).
Some of the demographic and clinical characteristics of the participants are shown.
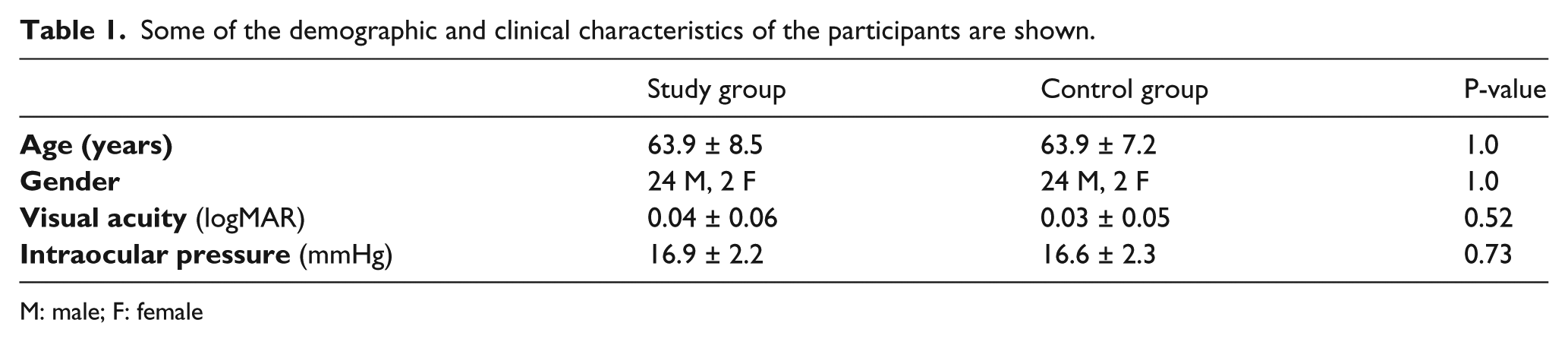
M: male; F: female
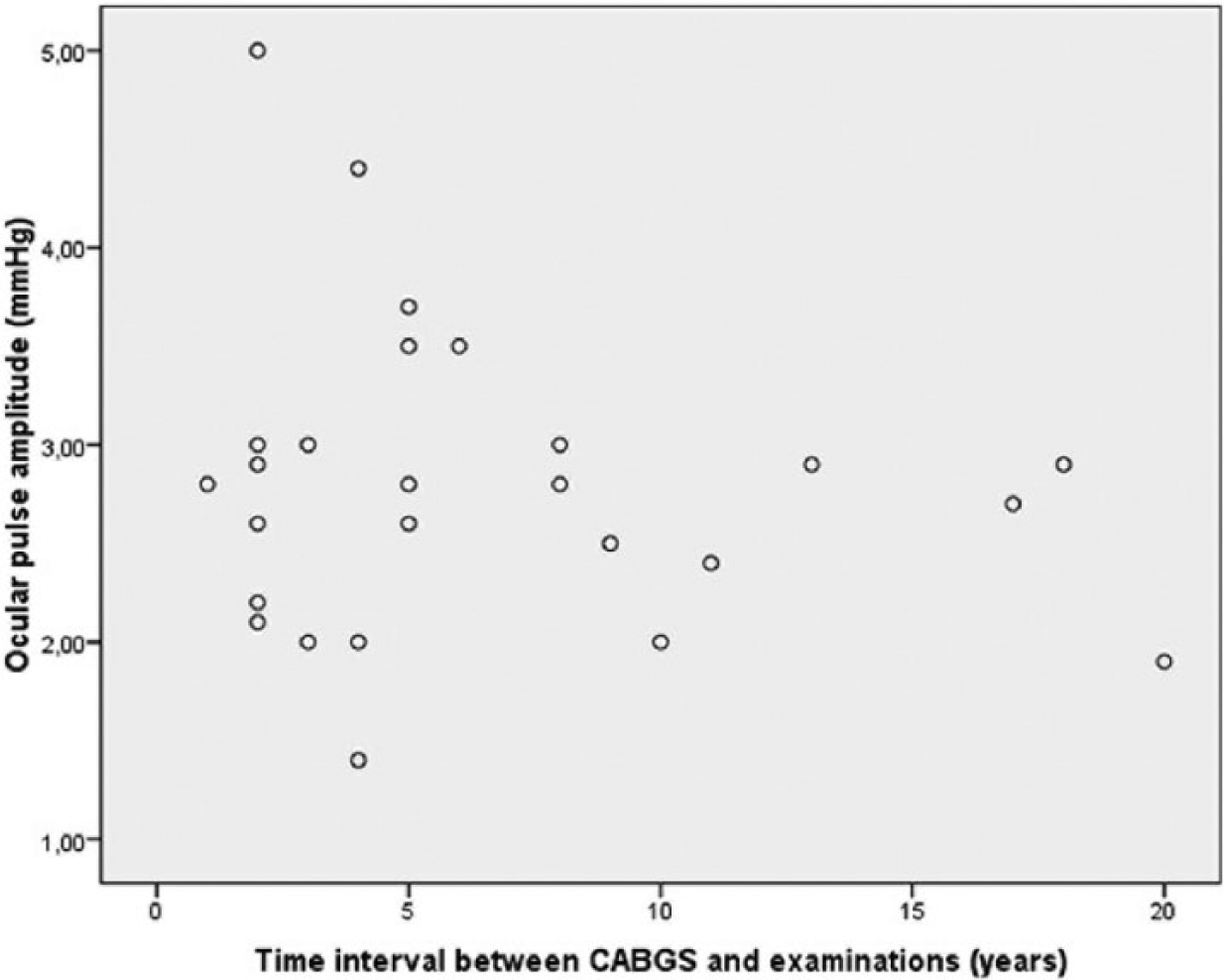
The scatter plot graphic showing the correlation of ocular pulse amplitude and the time interval between CABG surgery and ocular examinations.
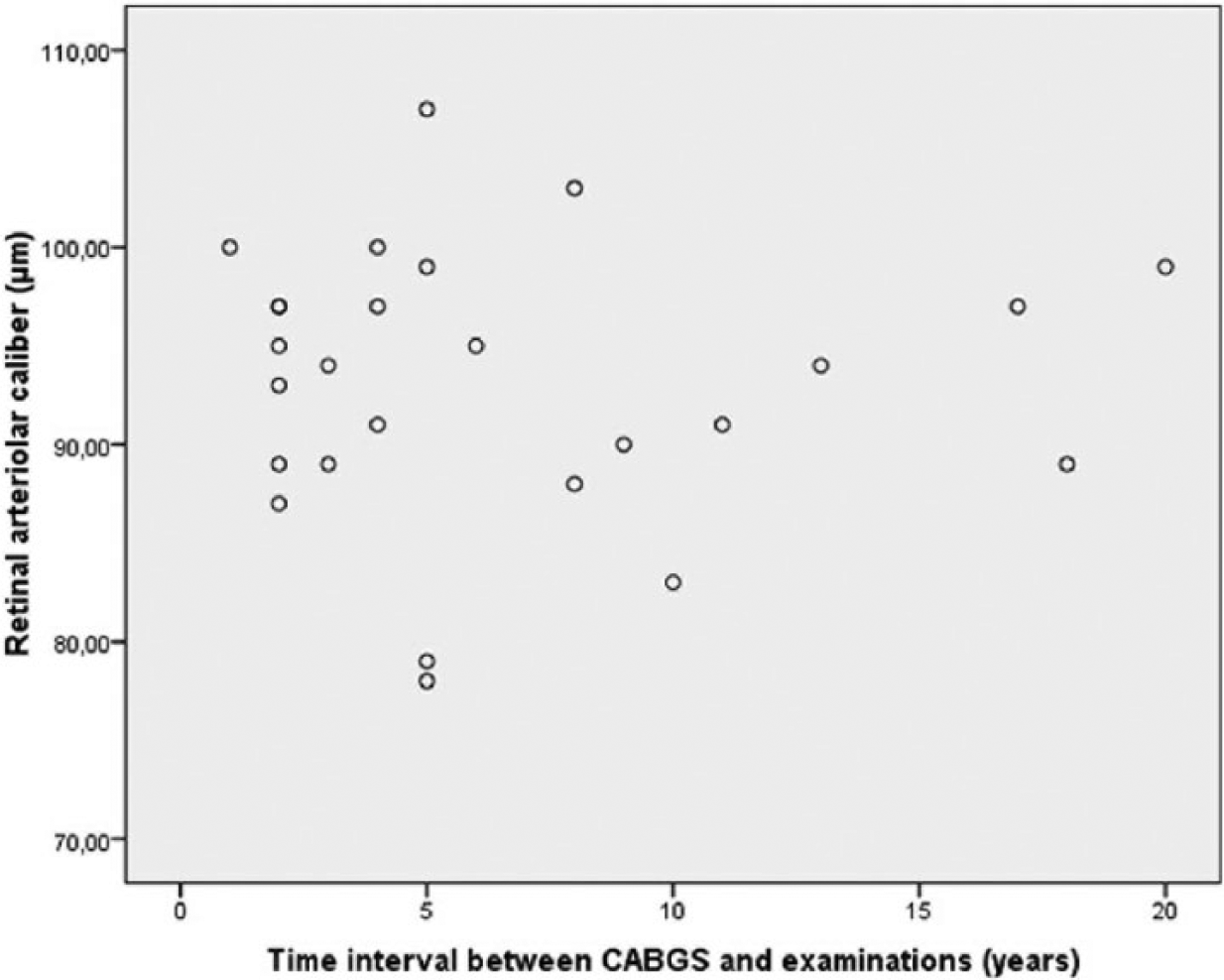
The scatter plot graphic showing the correlation of retinal arteriolar caliber and the time interval between CABG surgery and ocular examinations.
The mean OPA value was 2.79 ± 0.78 mmHg in the study group and the mean OPA value was 2.63 ± 0.87 mmHg in the control group (p=0.40). The mean retinal arteriolar caliber was 93.1 ± 6.9 µm in the study group and 95.3 ± 6.6 µm in the control group (p=0.42). The mean retinal venular caliber was 123.8 ± 11.0 µm in the study group and 123.2 ± 9.1 µm in the control group (p=0.92).
The mean macular thickness was 268.2 ± 24.2 µm in the study group and 266.2 ± 22.3 µm in the control group (p=0.87). The mean peripapillary RNFL thickness was 99.7 ± 9.1 µm in the study group and 102.2 ± 10.7 µm in the control group (p=0.36). Figure 4 shows the box plot graphic of both groups for peripapillary RNFL and macular thickness parameters. Segmental peripapillary RNFL thickness (inferior, superior, nasal and temporal) measurements are shown in Table 2. There were no significant differences between the groups in regard to quadrantal peripapillary RNFL thickness values (p>0.05).
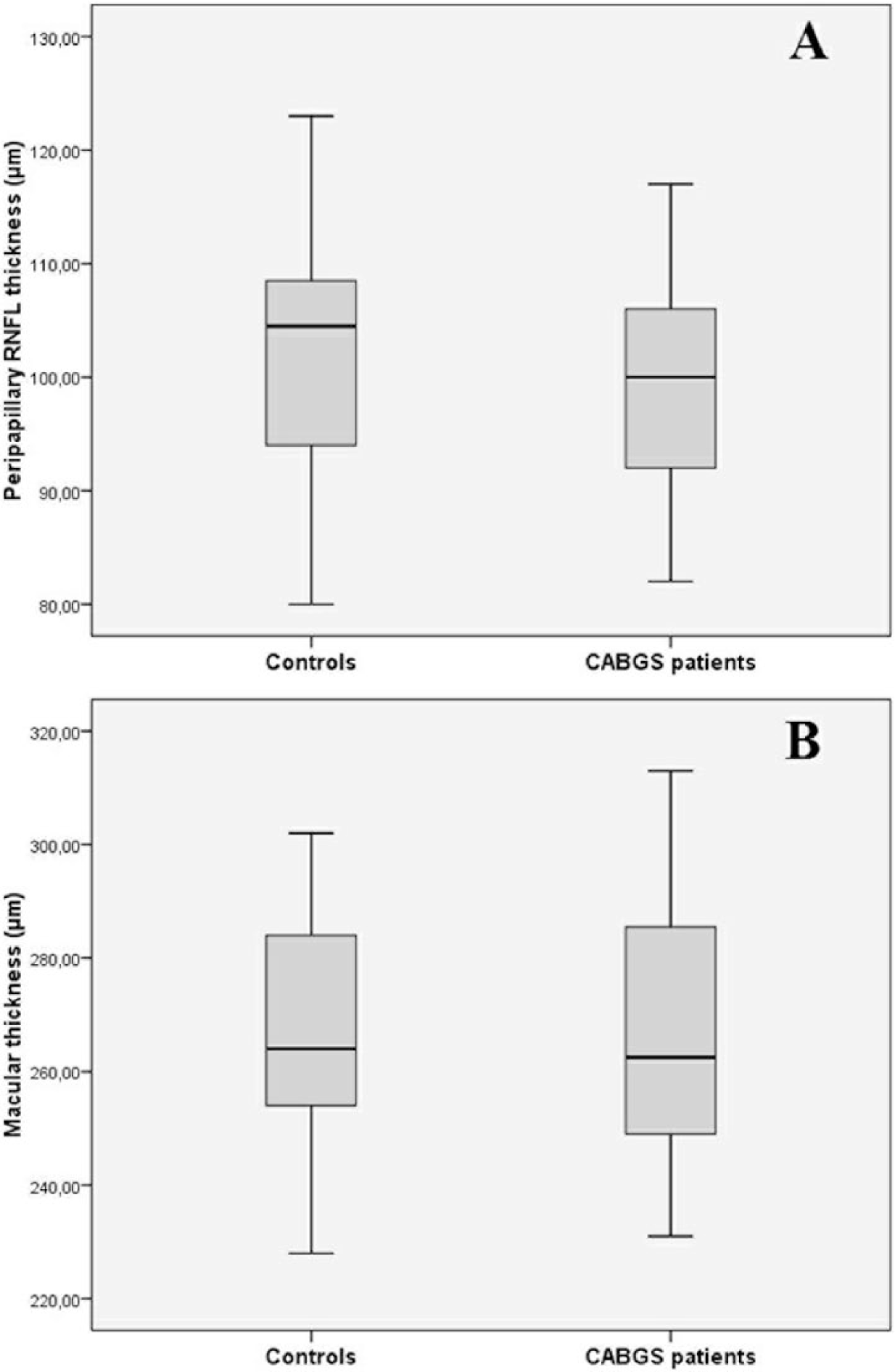
The box plot graphic of both groups for peripapillary RNFL (A) and macular thickness (B) parameters.
Segmental peripapillary RNFL thickness (inferior, superior, nasal and temporal) measurements are shown.

Discussion
Our results show that CABG surgery does not damage retinal structures and functions in the long-term follow-up. Among other non-ocular surgeries, cardiac surgery possesses a higher risk of visual impairment and ocular dysfunction.5-7 Most of the previous reports related to ocular problems after cardiac surgery focused on the individual patients who had visual loss due to ischemic optic neuropathy.4,8 But, in this study, rather than obtaining data about the diseased eyes from the patient records, we compared various ocular parameters related to perfusion between CABG surgery patients and healthy controls.
The OPA is accepted as the difference between systolic and diastolic values of the pulsatile IOP and it gives us an estimation of the global ocular and choroidal blood flow corresponding with the heart pulse as a function of time. 9 Various factors, such as carotid artery stenosis and glaucoma, decrease OPA.10,11 However, diabetes mellitus and systemic blood pressure do not affect OPA.12,13 In this study, no difference was found in terms of OPA between the CABG surgery patients and the controls. This result might be interpreted as there is not much difference between a normal and an operated heart in pumping blood to the choroid. The IOP could rise during CABG surgery,14,15 and this transient increase in IOP might affect ocular perfusion and cause damage to the optic nerve. Additionally, we found that CABG surgery does not affect IOP in the long term.
In the present study, the macular thicknesses of the CABG surgery patients and control subjects were very similar. This result might indicate that CABG surgery does not affect the macula. It is already known that visual disturbance is usually related to the optic nerve rather than the macula after CABG surgery.7,16 We found that peripapillary RNFL was slightly thinner in CABG surgery patients, although the difference was not statistically significant. Normally, the neuro-retinal rim is thickest
Alterations in RVC are related to a high risk for cardiovascular problems and are predictive of coronary heart disease.17,18 Narrower retinal arteriolar caliber and wider retinal venular caliber are associated with the increased risk of coronary heart disease. 19 In the present study, although the difference was not statistically significant between the groups, the retinal arterioles were narrower and the venules were wider in the CABG surgery patients. The time interval between the heart operations and the ocular examinations was not associated with retinal arteriolar caliber.
Our study has several limitations. First, the number of participants was relatively low, but it is not usual to find coronary heart disease patients without any associated systemic and ocular abnormalities. It would be nice if we had pre-operation ocular measurements in the study group. Lastly, fundus fluorescein angiography might give additional data about retina-choroidal blood flow in CABG surgery patients. All of our patients had undergone on-pump CABG surgery, but lesser complications have been reported when performing off-pump cardiac surgery techniques instead of on-pump techniques. 20
The impact of heart surgery on eyes has been investigated for nearly 40 years. In this study, we tried to reveal some new points about the ocular effects of CABG surgery in the long term. As a result, by the help of OCT and DCT instruments, we found that OPA, IOP, RVC, peripapillary RNFL and macular thickness were similar in the CABG surgery patients and controls. In conclusion, CABG surgery does not affect retinal thickness, retinal vessels or pulsatile ocular blood flow in long-term follow-up.
Footnotes
Declaration of conflicting interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.