
Abstract
We report a unique utilization of a double-lumen, bi-caval Avalon cannula for veno-venous (VV) extracorporeal membrane oxygenation (ECMO) during placement of a total artificial heart (TAH, SynCardia, Tucson, AZ). A 22-year-old female with post-partum cardiomyopathy was rescued on veno-arterial (VA) ECMO because of cardiogenic shock. The inability to wean ECMO necessitated implantation of the TAH as a bridge to transplant. In addition, the patient continued to have respiratory failure and concomitant VV ECMO was planned with the implant. During TAH implantation, the Avalon cannula was placed percutaneously from the right internal jugular vein into the inferior vena cava (IVC) under direct vision while the right atrium was open. During VV ECMO support, adequate flows on both ECMO and TAH were maintained without adverse events. VV ECMO was discontinued, without reopening the chest, once the patient’s respiratory failure improved. However, the patient subsequently developed a profound respiratory acidosis and required VV ECMO for CO2 removal. The Avalon cannula was placed in the femoral vein to avoid accessing the internal jugular vein and risking damage to the TAH. The patient’s oxygenation eventually improved and the cannula was removed at the bedside. The patient was supported for 22 days on VV ECMO and successfully weaned from the ventilator prior to her orthotropic heart transplantation.
Introduction
Percutaneous central venous instrumentation on a patient with a total artificial heart (TAH) is challenging due to the presence of a mechanical valve in the tricuspid position. 1 Blind placement of a guide-wire for a central venous access toward the right atrium is contraindicated in the TAH due to the risk of violating the inflow valve. Under direct vision, we safely placed a double-lumen, bi-caval venous extracorporeal membrane oxygenation (ECMO) cannula (Maquet, Rastatt, Germany), using a modified Seldinger technique in the operating room prior to implantation of the right-sided device to avoid violation of the tricuspid valve of the TAH. ECMO flow was successfully maintained without complicating the output of the TAH during the perioperative period. The patient was successfully supported while the pulmonary dysfunction recovered prior to orthotropic heart transplantation.
Case Report
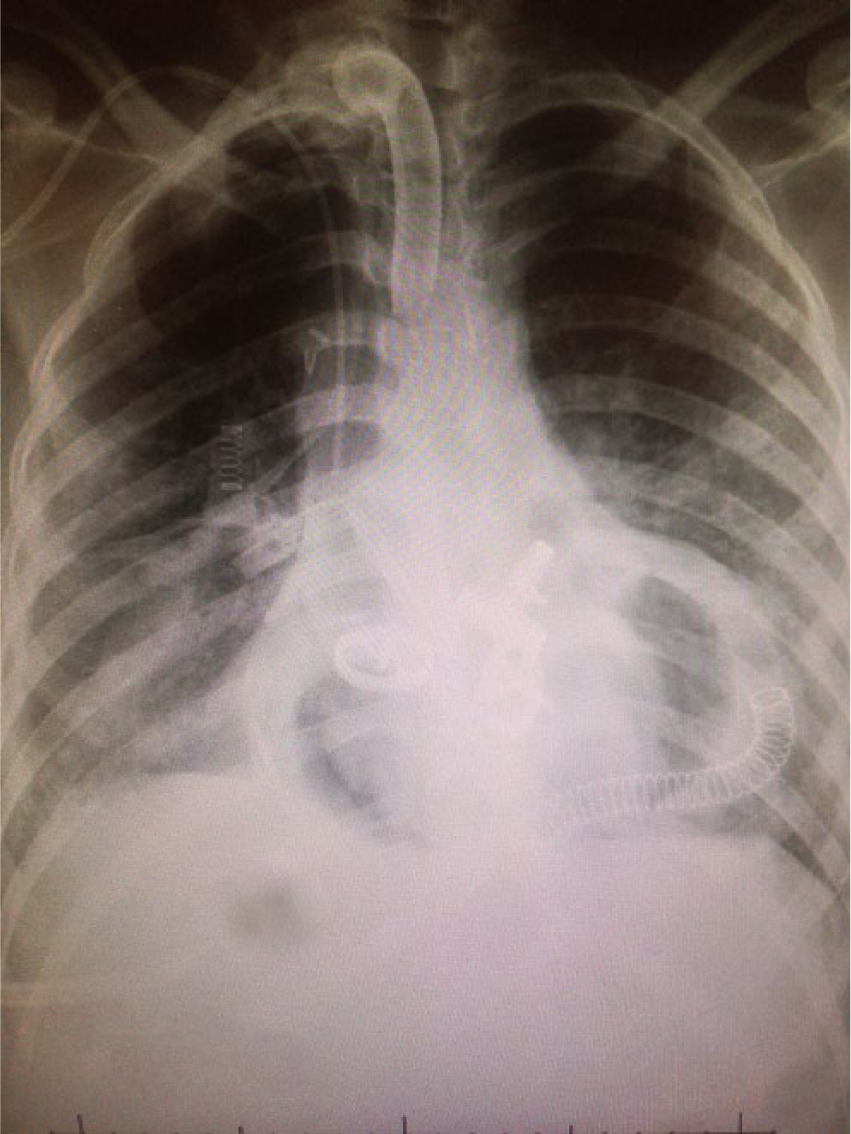
The patient was a 22-year-old female of small body habitus (body surface area of 1.5 m2) without any past medical history who developed congestive heart failure 2 weeks after an uncomplicated pregnancy and vaginal delivery. Echocardiography showed severe biventricular dysfunction with an ejection fraction of 10%. The patient rapidly decompensated into cardiogenic shock despite maximal medical management and was placed on VA ECMO for salvage as a bridge to decision (Figure 1). Despite ECMO support, the patient developed liver and kidney failure, which were supported with molecular absorbent recirculation system (MARS) and continuous venovenous hemodialysis (CVVHD), respectively. The patient’s fluid balance was managed with ultrafiltration. The patient failed multiple attempts at weaning off VA ECMO and was evaluated for TAH as a bridge to cardiac transplantation. Multiple modalities of lung protective mechanical ventilation were utilized, as well as prone position to optimize the patient’s respiratory status, prior to TAH implant. However, her lung compliance was poor and profound respiratory failure was expected after discontinuation of cardiopulmonary bypass following TAH implantation. We decided to prepare for VV ECMO during the implantation of the TAH to avoid the problems associated with catheter placement after the TAH was already in place.
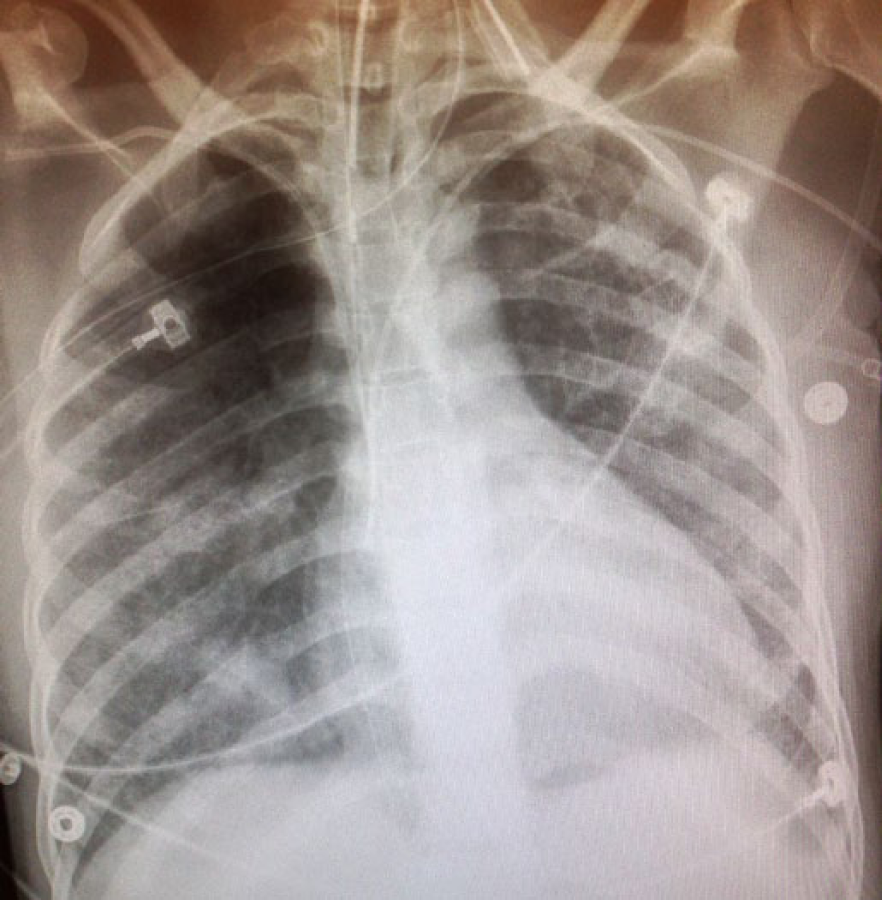
Chest x-ray of the patient prior to the total artificial heart shows the venous cannula in the right atrium while on VA ECMO.
Under general anesthesia and with sterile technique, a 16G single-lumen intravenous catheter was placed in the right internal jugular vein and it was prepped into the field to be accessed intraoperatively. Following median sternotomy, the patient was placed on cardiopulmonary bypass, using a superior vena cava (SVC) cannula and the pre-existing femoral venous cannula that was used for VA ECMO. The heart was excised in the standard fashion. The left and right atrial, pulmonary and aortic graft connectors were sewn into place, the left TAH ventricle was inserted. Under direct vision, a guide-wire was passed through the previously placed 16G intravenous catheter, while maintaining full flow on cardiopulmonary bypass from the femoral cannula. Using a modified Seldinger technique, a 23-French double-lumen, bi-caval Avalon cannula was inserted and the tip was placed in the inferior vena cava. The Avalon cannula outflow was positioned in the mid-body of the right atrium, directed to the TAH inflow (tricuspid) valve. In order to prevent migration of the cannula across the TAH inflow valve, the cannula was fixed loosely with a monofilament suture to the lateral wall of the right atrium, away from the right atrial connector so it would not inadvertently migrate across the inflow valve, but was capable of being pulled out when VV ECMO support was no longer required. After the Avalon cannula was positioned, the right TAH ventricle was connected and the patient was weaned from cardiopulmonary bypass while VV ECMO was initiated (Figure 2).
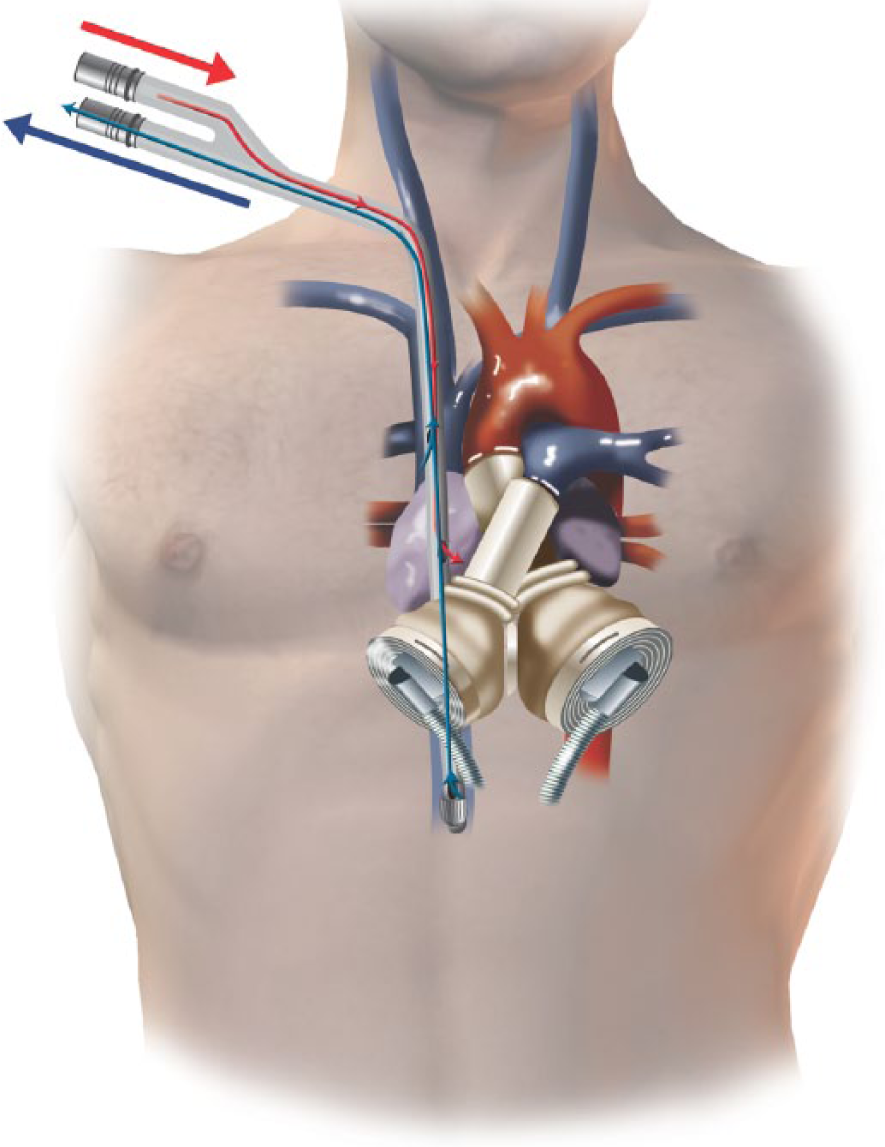
Illustration of the Avalon cannula placement with the total artificial heart.
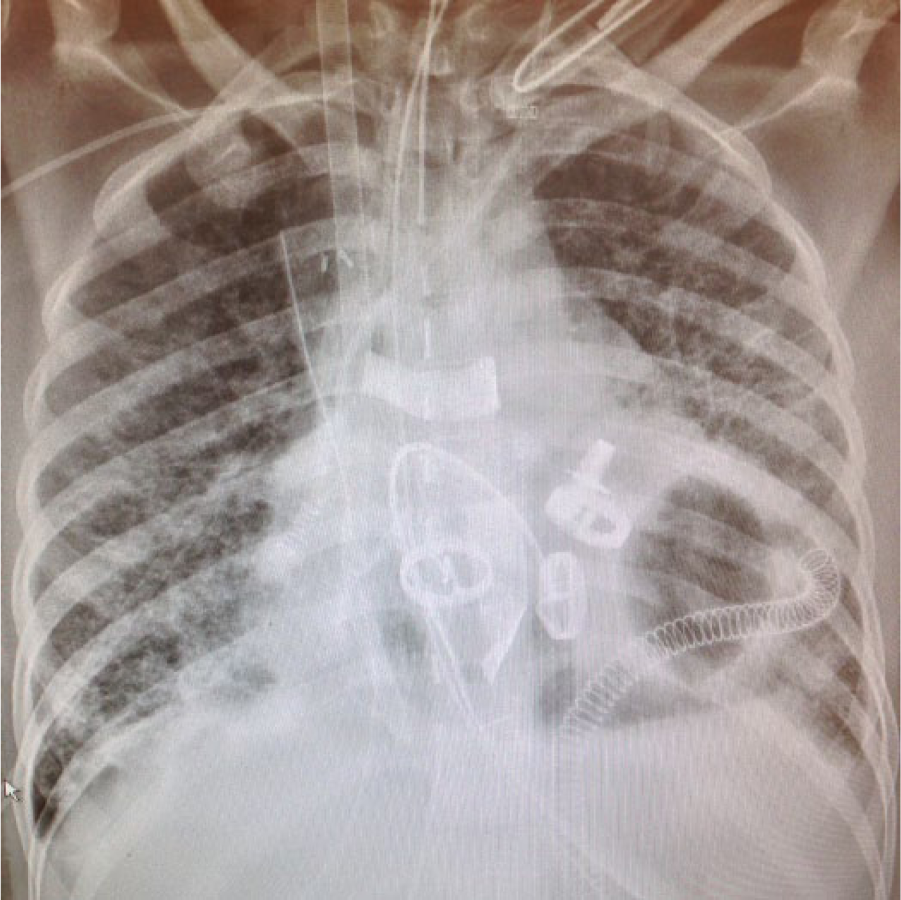
Post-operatively the patient developed severe hypoxic respiratory failure that was supported adequately on 3 L/min of VV ECMO flow (Figure 3). The TAH functioned adequately with 3.6 L/min (cardiac index = 2.4 L/min/m2) output. The beat rate initially was set at 90 beats per min to maintain ventricle filling of 50 ml and the rate was gradually increased as fluid resuscitation was accomplished.

Chest x-ray immediately after total artificial heart placement showing severe pulmonary edema. The Avalon dual-lumen cannula is located in the right atrium for VV-ECMO oxygen support.
Initial ECMO and ventilator FiO2 were 1.0. CVVHD was reinstituted to optimize her fluid status. Pulmonary edema completely resolved within 10 days (Figure 4). The ventilator and ECMO FiO2 requirements were both gradually weaned down to 0.5 (Figure 5). There were no significant alterations in TAH flow during this time. After 12 days of support on VV ECMO, the patient underwent an uneventful removal of the Avalon cannula without reopening the mediastinum. Immediately following discontinuation of VV ECMO, the patient developed a severe respiratory acidosis secondary to poor pulmonary compliance in the presence of adequate oxygenation. To rescue the patient in the intensive care unit (ICU), a 19-French Avalon cannula was inserted into the femoral vein for the purpose of CO2 removal. Because of the risk of disruption of the TAH inflow valve and the need for CO2 removal, but not oxygenation, the right jugular vein approach was abandoned and femoral cannulation was our procedure of choice.
Chest x-ray prior to VV ECMO removal shows improved pulmonary edema.
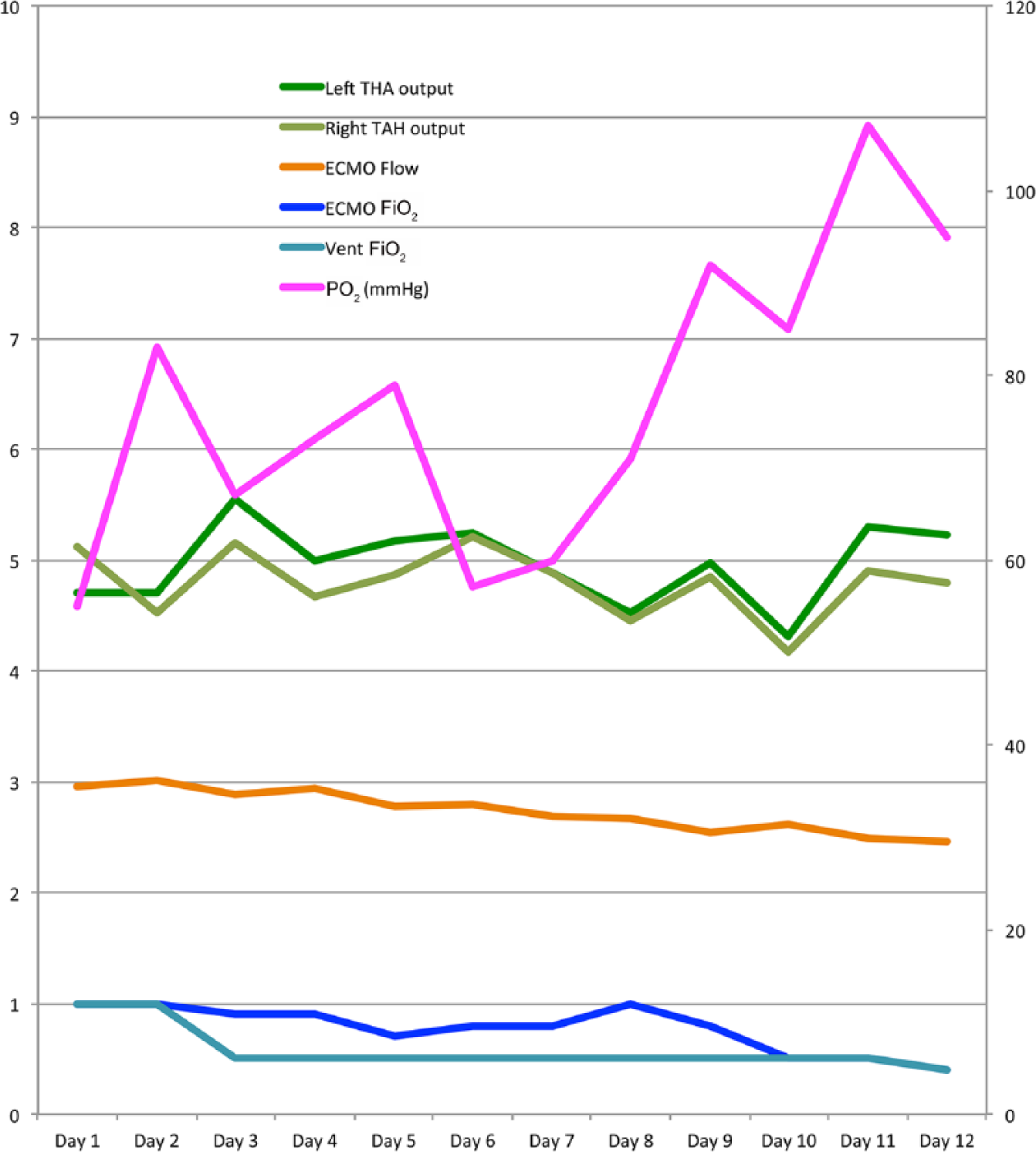
PaO2 and FiO2 relation over the course of the VV ECMO. FiO2 from both VV ECMO and ventilator were decreased to 50% as the systemic oxygenation improved.
The patient required an additional 10 days of ECMO support for CO2 removal while pulmonary compliance and gas exchange improved (Figure 5). The catheter was removed at the bedside on day 22 post-TAH. The patient’s condition stabilized and she underwent tracheostomy. The patient was cycled on and off the tracheostomy collar. After 96 days of TAH support, the patient tolerated no ventilator support and she was listed 1A for orthotropic heart transplantation. After 103 days of TAH support, she underwent orthotropic heart transplantation (Figure 6).
Chest x-ray prior to the heart transplant.
Discussion
Respiratory failure is a common concomitant morbidity in the patient with cardiogenic shock. Post-cardiotomy acute pulmonary edema is often observed in the patient who has undergone open-heart surgery with poor myocardial protection or the patient with poor cardiac function. However, the cardiac function after TAH placement, theoretically, should be normal, as long as the TAH is functioning appropriately. The mechanism of the acute pulmonary edema in our patient is most likely related to pre-implantation pulmonary injury, as well as poor pulmonary compliance and capillary leak related to fluid overload.
Profound respiratory failure despite optimal ventilator support could be an indication for either VV or VA ECMO. 2 Acute pulmonary edema related to poor cardiac function is best treated with VA ECMO since VV ECMO does not unload the heart and provide systemic perfusion. Currently, the Avalon cannula is predominantly chosen for VV ECMO in our institution. The Avalon inflow is designed to be located in the superior and inferior vena cavae and the outflow faces the tricuspid valve to minimize shunting. The oxygenated blood from the outflow orifice should travel from the right ventricle to the pulmonary circulation, then to the left ventricle and eject to the systemic circulation. In the setting of TAH implantation, since the TAH maintains bi-ventricular function, VV ECMO should be theoretically functional. In our case, VV ECMO did not adversely affect flow on the TAH because the preload to the right atrium was not reduced by the Avalon cannula itself.
Previously, Anderson described a patient who underwent TAH placement, requiring VA ECMO to manage the patient’s subsequent respiratory failure. 3 They placed VA ECMO centrally between the aorta and right atrium. During ECMO support, VA ECMO flow and TAH flow were carefully adjusted, based on the mixed venous saturation, to balance the systemic circulation. VA ECMO flow was noted between 2.5 and 4.5 L/min and TAH flow was between 1.5 and 2.0 L/min. Although there was no complication observed during their 16 hours of VA ECMO support, longer periods of VA ECMO-TAH support may lead to flow competition and possible TAH thrombosis. In a report by Spiliopoulos, 4 VV ECMO is initiated in a patient with TAH support who developed acute respiratory distress syndrome (ARDS). They placed an Avalon cannula via the right internal jugular vein, using transesophageal echocardiography (TEE) guidance. The authors stated that the placement of the Avalon cannula in this TAH patient was difficult despite TEE guidance and there was a significant risk of inflow valve violation and TAH damage.
In the patient with severe hypercapneic respiratory failure, femoral cannulation with a double-lumen cannula may provide adequate gas exchange. We expected femoral cannulation would result in significant shunting in the IVC, which would not provide oxygenation. In our case, CO2 removal alone was our goal and this was achieved with this approach. Additionally, femoral cannulation for an additional ECMO run was preferred to avoid the risk of violation of the TAH inflow valve. To the authors knowledge, there are no documented cases of using VV ECMO for CO2 removal, only via the femoral vein approach.
Conclusion
Pulmonary support with VV ECMO following implantation of the TAH can be safe and effective. In our case, the double-lumen, bi-caval cannula flow was stable and did not interfere with the TAH filling. VV ECMO was able to provide appropriate oxygenation while the TAH provided adequate systemic perfusion. We believe that using single cannula VV ECMO is the best option for ECMO in a patient with TAH flow. The surgically directed Avalon cannula placement during the TAH implantation minimized the risk of TAH inflow valve damage. For CO2 removal only, femoral cannulation using a single, double-lumen cannula is a safe option.
Footnotes
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.