
Abstract
Venovenous extracorporeal membrane oxygenation (ECMO) is used for patients with severe, potentially reversible, respiratory failure unresponsive to conventional management. It is relatively contraindicated in patients with traumatic brain injury (TBI) due to bleeding complications and use of anticoagulation. We report two cases of TBI patients treated with ECMO.
Keywords
Introduction
Traumatic brain injury (TBI) is a relative contraindication for extracorporeal membrane oxygenation (ECMO) due to bleeding complications and anticoagulation required for the ECMO circuit.1,2 However, bleeding complications, including intracranial hemorrhage and anticoagulation requirements may be reduced with modern circuits. We report the successful use of venovenous ECMO using our low-dose anticoagulation protocol in two TBI patients with severe acute respiratory distress syndrome (ARDS).
Cases
Patient 1
The first patient was an 18-year-old man admitted after being struck by a vehicle. His initial Glasgow Coma Scale score (GCS) was 14, but he became combative and required endotracheal intubation. His Injury Severity Score (ISS) was 27. A head computed tomography (CT) scan revealed a right parieto-occipital epidural hematoma, right frontal subarachnoid hemorrhage and hemorrhagic contusions (Figure 1A). An external ventricular drain and bolt were placed; due to his well-controlled intracranial pressure (ICP), neurosurgical intervention was not required. On hospital day 4, he developed pneumonia and severe ARDS, with nadir partial pressure of arterial oxygen (PaO2) to fraction of inspired oxygen (FiO2) ratio of 42. Lung protective ventilation was attempted; however, hypercapnea led to an ICP crisis and the progressive hypoxemia resulted in decreased brain tissue oxygen (PbO2). Our center’s ECMO team was consulted and the patient was cannulated with a 31 French Avalon Elite™ bicaval dual-lumen cannula (Maquet, Rastatt, Germany) which was our standard for ECMO transport at that time. A heparin infusion was titrated according to our standard low-dose anticoagulation protocol; activated partial thromboplastin time (aPTT) target for patients receiving ECMO is 40-60 seconds. The median aPTT was 47 seconds for the ECMO run. Once on ECMO, his cerebral perfusion pressure, ICP, PbO2, PaO2 and PaCO2 were maintained within acceptable ranges. His neurologic exam improved and he was following commands by ECMO day 11, decannulated on ECMO day 13 and extubated 6 days later. He made a complete neurologic recovery
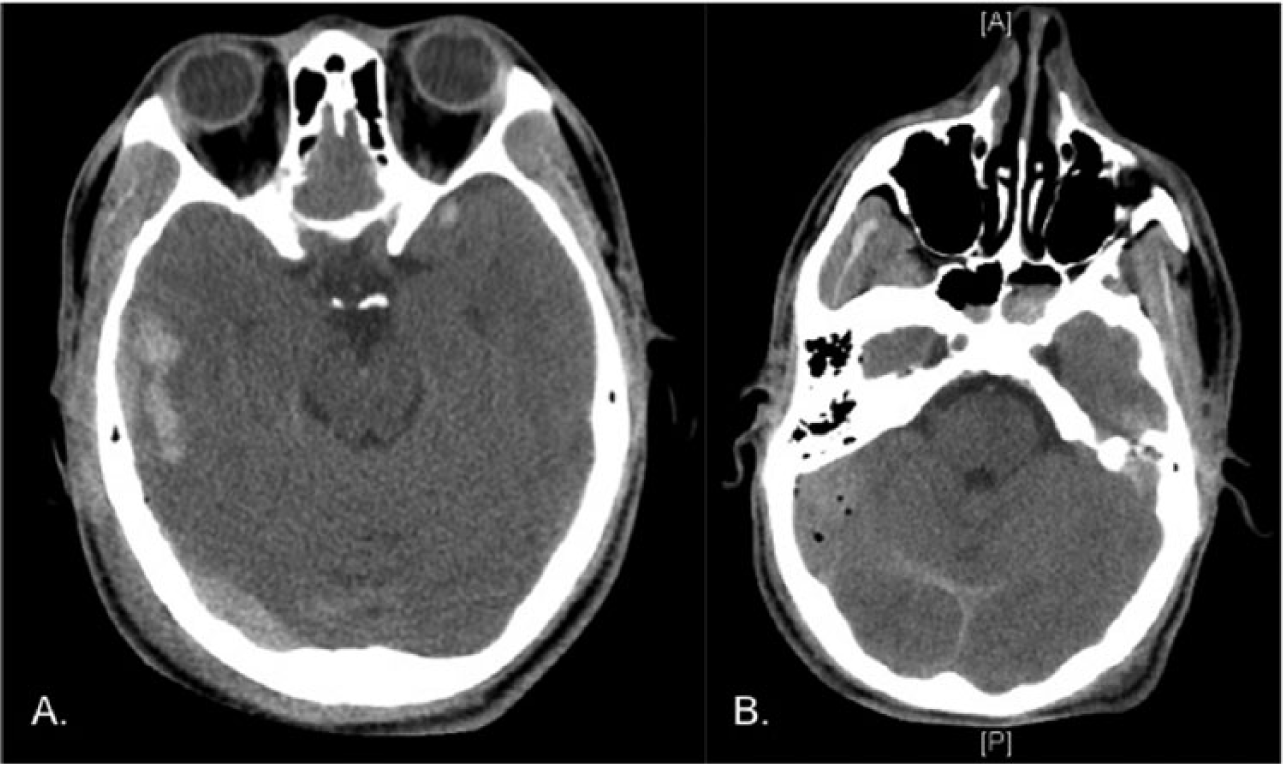
A) Patient 1 CT head; B) Patient 2 CT head.
Patient 2
The second patient was a 20-year-old man admitted after being ejected from a truck. His initial GCS was 3. Injuries included hemotympanum and left chest ecchymosis with an ISS of 33. A head CT demonstrated bilateral subdural hematomas, subarachnoid hemorrhage, bilateral temporal and frontal contusions and cerebral edema (Figure 1B). He was intubated and bilateral external ventricular drains were placed. On hospital day 4, after several stable head CTs, the patient developed severe ARDS, with a nadir PaO2:FiO2 ratio of 30, despite optimized ventilator management and inhaled nitric oxide. The patient was cannulated with a 31 French Avalon Elite™ bicaval dual-lumen cannula by our ECMO team and transported to our institution where he was paralyzed, cooled to 33oC in an attempt to reduce cerebral metabolic demand and supported with ECMO. The median aPTT from the heparin infusion was 51 seconds while on ECMO. He was decannulated on ECMO day 6 and made a complete neurologic recovery.
Discussion
The incidence of ARDS in patients with isolated TBI is 20-30% and is an independent predictor of poor outcomes. 3 The management of TBI includes minimizing ICP by targeting PaCO2 between 30-35 mmHg and avoiding hypoxemia. However, lung protective ventilation in ARDS may result in hypercapnea and methods to improve oxygenation, such as high PEEP, may decrease cerebral perfusion pressure.
ECMO can improve control of PaCO2 and PaO2 in patients with cerebral and pulmonary insults when optimized ventilator management is inadequate. However, TBI is a relative contraindication to ECMO, given the need for anticoagulation, bleeding complications and circuit-related thrombocytopenia. Several case series report the successful use of ECMO in TBI patients, both with and without systemic anticoagulation.2,4–6 We typically see 10 pure TBI cases and 70 subdural hemorrhages from falls yearly in our neuro-ICU. In our experience, we used our standard heparinization at the initial cannulation with a 2000U IV heparin bolus and maintained a low aPTT target throughout the ECMO run. We have demonstrated safety and efficacy of using a heparinized ECMO circuit to support TBI patients with ARDS. The risks of severe hypoxemia and elevated ICP must be weighed against the risk of intracerebral hemorrhage in a coordinated discussion between critical care, ECMO and neurology teams.
Footnotes
Declaration of Conflicting Interest
Dr. Bacchetta has consulted for Maquet Inc., a non-remuneration agreement.
Dr. Brodie reports receiving research support from Maquet Cardiovascular, including travel expenses for research meetings, as well as anticipated support for upcoming studies and compensation paid to Columbia University for research consulting. He receives no direct compensation from Maquet. He is a member of the Medical Advisory Board for ALung Technologies. Compensation is paid to Columbia University; he receives no direct compensation from ALung Technologies. Dr. Brodie anticipates joining the Medical Advisory Board of Gambro with compensation to be paid exclusively to Columbia University.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.