
Abstract
Pulsatile and non-pulsatile cardiopulmonary bypass (CPB) flows may have different impact on cerebral oxygen saturation in patients with restricted cerebral arterial blood supply. Twenty patients, ten diagnosed with carotid stenosis (CS, n = 10) and ten without known carotid disease (Controls, n = 10), were subjected to one period of pulsatile and one period of non-pulsatile flow (6-8 min each) during CPB at 32°C. Cerebral oxygen saturation was registered by near-infrared light spectroscopy (NIRS).
The mean arterial pressure (MAP) was significantly lowered by pulsatile CPB flow. The NIRS tissue oxygenation index (TOI) tended to decrease in the CS group and increase in the Controls during pulsatile flow compared with non-pulsatile; however, the changes were not statistically significant.
No significant correlations were seen between the changes in MAP and TOI across the observation periods.
In conclusion, pulsatile CPB flow caused slightly decreased mean arterial pressure while the effect on cerebral oxygenation was unclear. Pulsatile flow was not found superior to non-pulsatile flow in patients with or without carotid stenosis.
Introduction
Cerebral perfusion during cardiopulmonary bypass (CPB) may be impaired by disturbed autoregulation, arterial embolism and venous congestion.1–4 Technical circumstances, for instance, unsatisfactory positions of CPB cannulas as well as underlying medical conditions such as carotid stenosis, may contribute to or worsen cerebral hypoperfusion. The arterial flow during CPB can be delivered using pulsatile or non-pulsatile flow profiles. Pulsatile flow has been advocated and included in protocols to optimize cerebral perfusion,5–8 but there is no general consensus view regarding what mode to select a priori and the same is true regarding the decision to switch between the modes. Continuous, non-pulsatile flow has the advantage of being a well-established and technically robust method while pulsatile flow shares similarities with the natural flow from the beating heart. However, pulsatile flow is technically more demanding and the clinical benefits have been questioned.9,10 It is noteworthy that there is no sharp definition of pulsatile flow and that technical information is not always provided in the literature. A clinical situation where pulsatile flow could be of particular interest is in case of arterial stenosis where the stenotic pressure drop leaves the post-stenotic driving pressure partially dependent on the pre-stenotic pressure. However, it is unclear whether the pressure peaks during pulsatile CPB flow are more effective than non-pulsatile flow to generate optimal post-stenotic flow. Carotid stenosis is present in a fraction of the patients undergoing CPB 11 and, in similarity with other patients, the choice of which CPB flow mode to apply is not indisputable. We analyzed the impact of pulsatile and non-pulsatile flow modes on cerebral oxygenation and hemodynamics during CPB in patients with and without carotid stenosis by using near-infrared light spectroscopy (NIRS)7,12,13 and routine hemodynamic monitoring. Both flow modes were applied for each patient during aortic cross-clamping, thereby, providing an internal control for each case.
Material and methods
This is a retrospective study on openly selected patients who had been included in a quality assurance (QA) project within the department. The aim of this QA project was to evaluate the effectiveness of pulsatile and non-pulsatile flow during CPB in patients with and without known carotid stenosis.
A protocol was used to establish stabile physiological (see targets below) conditions during aortic cross-clamping, upon which the flow profile was altered once in order to identify the most appropriate profile for each patient based on clinical assessment, including hemodynamics and cerebral oxygenation. The order of the flow profiles was random. The hemodynamics and the regional NIRS were observed during the entire operation and, during the observation periods of 6-8 min per flow mode, the measurements were recorded every minute. In the retrospective analysis, groups were formed based on the presence or absence of known carotid stenosis (CS, n = 10; Controls, n = 10). (Table 1) There was no case of symptomatic carotid disease. The study was approved by the Uppsala Regional Ethical Review Board and written consent was obtained from all patients.
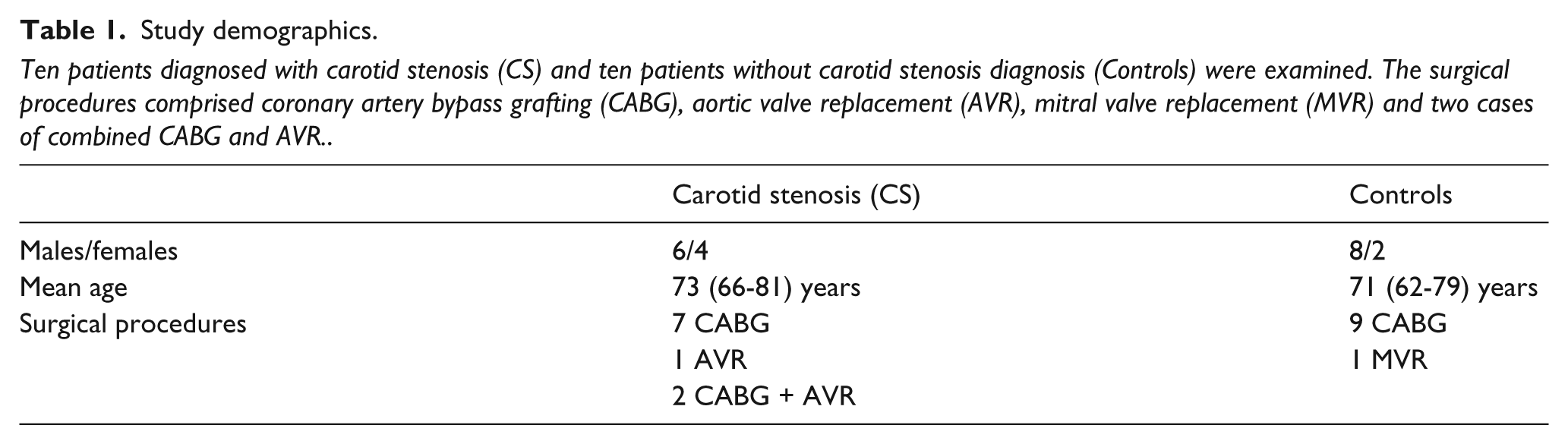
Study demographics.
Ten patients diagnosed with carotid stenosis (CS) and ten patients without carotid stenosis diagnosis (Controls) were examined. The surgical procedures comprised coronary artery bypass grafting (CABG), aortic valve replacement (AVR), mitral valve replacement (MVR) and two cases of combined CABG and AVR.
CPB was carried out by the same perfusionist in all cases (TT) with a Stöckert SIII roller-pump heart-lung machine (Sorin Group GmbH, Munich, Germany), standard Jostra polyvinyl chloride tubing, a Jostra Quadrox oxygenator and a Jostra hard-shell venous reservoir. All Jostra equipment was manufactured by Maquet GmbH & Co. KG, Rastatt, Germany. Cerebral oxygenation was monitored using NIRS (NIRO-200 TOI, Hamamatsu Photonics Deutschland GmbH, Herrsching, Germany) by which the proportions of oxygenated and de-oxygenated haemoglobin are presented as a Tissue Oxygenation Index (TOI). The measurement represents regional cortical vessels, predominantly veins.13–16 Arterial blood pressure was measured in the left radial artery. The physiological targets were PO2 13–17 kPa, PCO2 4.5–5.5 kPa and hematocrit >22 %; the nasopharyngeal temperature was 32°C during the cross-clamp period. The perfusion index was 2.4 liters/min/m2 and the pulse flow settings were: frequency 70/min, pulse width 40% and base flow 30%.
Data and statistics
All data are expressed as means ± SD. A paired t-test was used for within-group comparisons and an unpaired t-test was used for between-group analysis. Correlation analyses were carried out with the Pearson test for parametric data. An alpha-level of 0.05 was considered significant. Two data points relating to relative changes of TOI were excluded from the CS group after applying Grubbs’ test for outliers; one in the pulsatile subgroup and one in the non-pulsatile subgroup. All calculations were conducted with GraphPad Prism 6.02 (GraphPad Software Inc., San Diego, CA).
Results
The TOI recordings were generally symmetrical for all patients and, for all analyses, the means of the right and left side values were used.
MAP was significantly lower during pulsatile (P) compared with non-pulsatile flow (NP) (P: 71.1 ± 5.5, NP: 75.5 ± 7.7 mmHg, p=0.025, all patients). In the CS group, no significant MAP differences were seen between pulsatile and non-pulsatile flow (P: 72.2 ± 4.8, NP: 76.5 ± 9.8 mmHg, p=NS). However, in the Controls, the MAP was significantly lower during pulsatile compared with non-pulsatile flow (P: 70.1 ± 6.2, NP: 74.5 ± 5.3 mmHg, p=0.038). (Figure 1) The magnitude of change in MAP response to flow mode did not differ between the CS and Control groups.
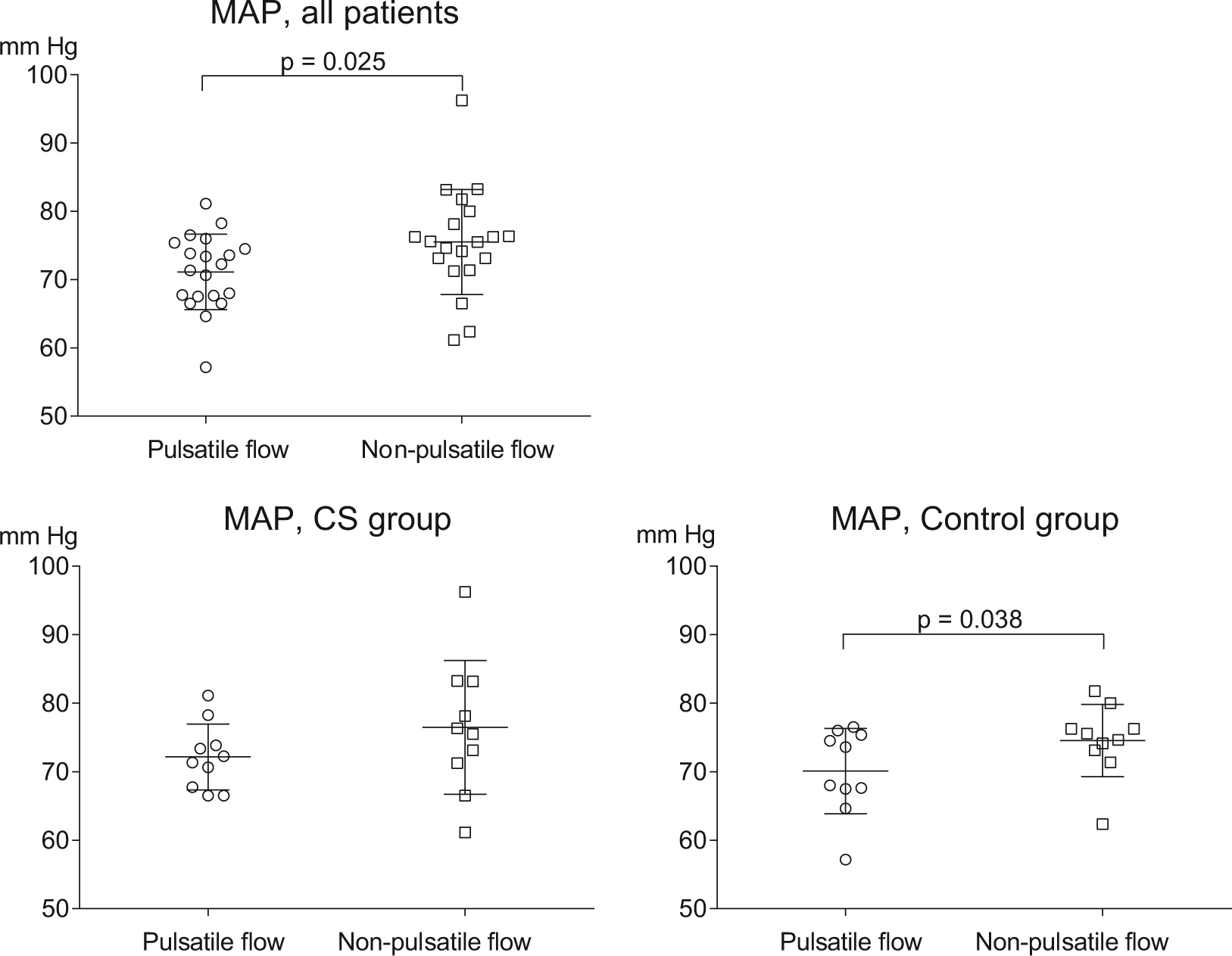
Mean arterial pressure (MAP) during pulsatile and non-pulsatile cardiopulmonary bypass flow in patients with (CS) and without (Controls) carotid stenosis. MAP was lower during pulsatile than non-pulsatile flow (p=0.025, all patients), a phenomenon present in both sub-groups, but statistically significant only in the Controls (p=0.038).
Pulsatile CPB flow did not increase cerebral oxygenation
The relative change in the TOI from the start to the end of each period was calculated for each individual and observation and plotted for all subgroups. Minor variations in TOI were seen in all subgroups (CS; P: - 0.2 ± 2.8, NP: 0.5 ± 2.0 %, p=NS, and Controls; P: 0.1 ± 3.3, NP: - 0.7 ± 2.5 %, p=NS), but there were no statistically significant differences between patient groups or flow modes. (Figure 2)
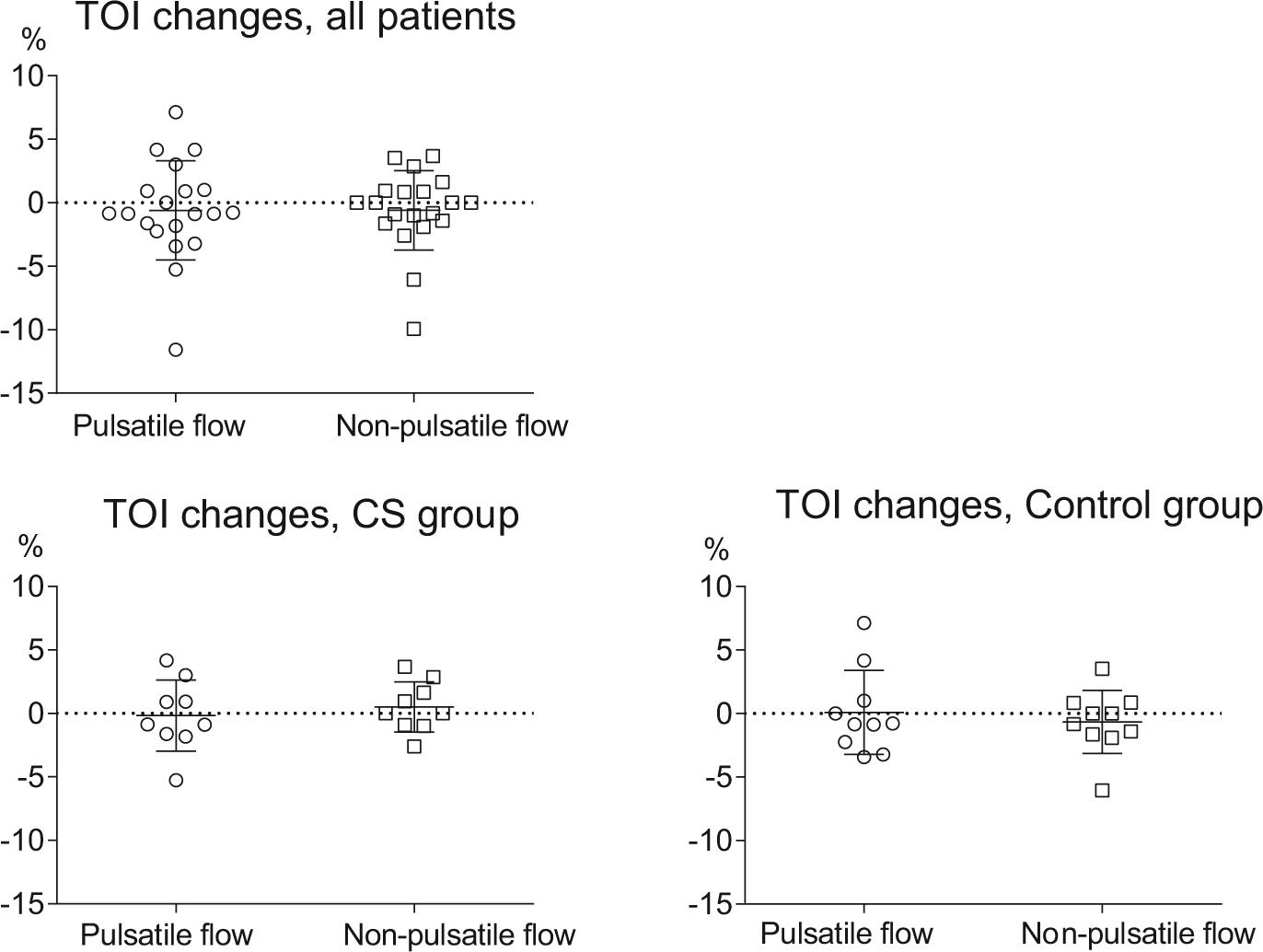
Relative changes in cortical tissue oxygenation index (TOI) during pulsatile and non-pulsatile cardiopulmonary bypass flow in patients with (CS) and without (Controls) carotid stenosis. The TOI changes were subtle in all groups and without statistical significance. Two data points were excluded from the CS group after applying Grubbs’ test for outliers; one in the pulsatile subgroup and one in the non-pulsatile subgroup.
Mean arterial pressure and cerebral oxygenation changes
The changes in MAP and the TOI across each observation period were calculated and tested for correlation. No correlation between MAP and TOI changes was found between pulsatile and non-pulsatile flow, between CS and Controls or within any of the subgroups. (Figure 3)
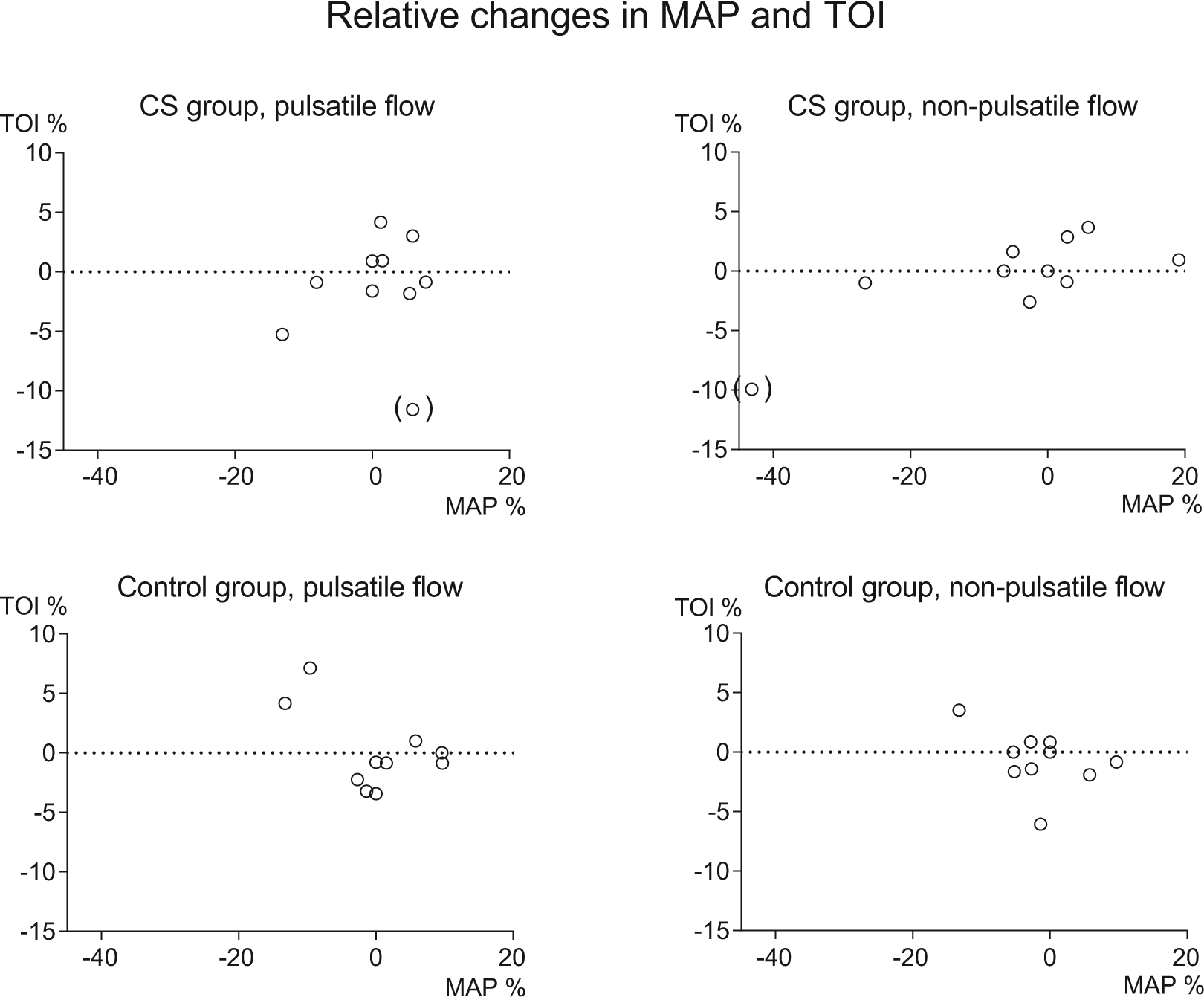
Relative changes in cortical tissue oxygenation index (TOI) and mean arterial pressure (MAP) during pulsatile and non-pulsatile cardiopulmonary bypass flow in patients with (CS) and without (Controls) carotid stenosis. No correlation between the parameters with either flow mode was shown in either subgroup. Two data points (in brackets) were excluded from the CS group after applying Grubbs’ test for outliers; one in the pulsatile subgroup and one in the non-pulsatile subgroup.
Discussion
The first main finding in this study was that pulsatile flow during aortic cross-clamping did not enhance cerebral oxygen saturation compared with non-pulsatile flow. The response in cerebral oxygenation varied between flow modes within the subgroups, although the differences were subtle and the clinical significance uncertain. In a study similar to ours, but not including CS patients, Grubhofer et al. also examined pulsatile and non-pulsatile CPB flow with cerebral NIRS, without being able to draw conclusions on superiority for either of the two flow modes. 10 Our second main finding was that MAP decreased during pulsatile mode compared with non-pulsatile, a phenomenon that has been described by Nakamura et al. for clinically relevant CPB flow levels. 17 Similarly, increased MAP has been previously reported by Mandelbaum et al. and Giron et al. during non-pulsatile CPB flow.18,19
Murkin et al. have presented the beneficial impact of pulsatile CPB flow on the incidence of myocardial infarction, major complications and death20,21 and more recent papers also demonstrate advantageous effects, such as increased overall cerebral blood flow and cerebral oxygen saturation levels, along with reduced vascular resistance and less plasma free haemoglobin.22,23 In a review of 159 papers on pulsatile blood flow, Ji et al. reported no evidence of adverse effects of pulsatile flow, but several papers described the positive effects on various parameters, such as hormone release, lung function, inflammatory response and perfusion of vital organs. 5 However, other authors have demonstrated negative effects10,24 or conflicting findings. 25 The literature on cerebral blood flow autoregulation in patients with carotid stenosis is sparse, but suggests that the degree of stenosis and impaired post-stenotic cerebral blood flow autoregulation due to exhausted vaso-reactivity increases the risk for cerebral damage.2,26 Contemporary CPB equipment usually offers a choice between pulsatile and non-pulsatile blood flow. The default preference varies and it is uncontroversial to switch between the two modes when attempting to optimize organ perfusion. In the case of arterial stenosis, it appears logical to maintain a higher blood pressure to compensate for the pressure drop across the stenosis. This, in turn, could provide a rationale to apply pulsatile flow in order to benefit from the pressure peaks exclusive to that mode. On the other hand, Piskin et al. describe that increased flow velocity generates post-stenotic turbulence with vortex formations and non-linear relationships between post-stenotic pressure, flow velocity, wall shear stress and flow distribution. 27 Furthermore, when the pressure peaks are generated by variations in the roller pump speed, a rapid cyclic reduction of pump speed follows, with a subsequent moment of negative pressure in the oxygenator. This might lead to the formation of gaseous CPB tubing emboli due to cavitation and, possibly, to excessive gas transfer across the porous oxygenator membrane. 28 Additionally, cavitation causes hemolysis and increased release of free oxygen radicals.29–31 Mulholland et al. have demonstrated a linearly increasing rate of change in plasma free hemoglobin beyond a negative pressure threshold of approximately -120 mmHg, with exposure to the venous reservoir air interface as a superimposing factor. 32 Other investigators suggest that negative blood pressures are of minor importance to hemolysis compared with other factors during CPB. 33 Yet, it seems reasonable, as far as possible, to avoid exposing the blood to excessive negative pressures during pulsatile flow. To that end, we optimized the CPB pulse settings to maximize the pulse amplitude within acceptable negative pressure limits. Nevertheless, the MAP in the present study was found to be lower during pulsatile flow than during non-pulsatile flow. This is in line with the described findings of Nakamura et al. 17 and indicates that, technically, the pulse mode characteristics could be adjusted to ensure a favorable MAP level by, for example, reducing the pulse-cycle base flow or narrowing the pulse width. However, empirically, such alterations have very limited impact on common perfusion parameters. With the present pulse-wave settings, peak blood flows are close to the maximum oxygenator flows recommended by the manufacturers while, during the nadir tubing pressure phase, they maintain a good margin to the hemolysis-creating negative pressure levels reported by Mulholland et al. 32 There are some important limitations to our study. The design was open and non-randomized, the degree of stenotic vessel disease was not closely penetrated, the observation time was brief and the power of the study did not allow multifactorial analysis. Thus, the findings are not possible to translate into CPB patients in general. However, the study sheds doubt over the possibility to improve cerebral oxygenation by pulsatile flow generated by variable roller-pump speed, regardless of the presence of carotid stenosis.
Conclusion
Pulsatile flow was associated with slightly decreased arterial pressure. The effect on cerebral oxygenation was uncertain. Pulsatile flow could not be shown superior to non-pulsatile flow in patients with or without carotid stenosis.
Footnotes
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.