
Abstract
Gaseous microemboli (GME) generated during cardiopulmonary bypass (CPB) can present a significant risk to patient outcomes, specifically if they are delivered to the cerebral vasculature. A number of GME sources have been identified, leading to improved clinical practice and equipment design to ameliorate the presence and intensity of GME during CPB. Recently, a number of new venous reservoir/oxygenator systems have entered the market, including the Sorin Inspire6 and Inspire8, the Terumo FX15 and FX25 and the Maquet Quadrox-i. The goal of the current study was to evaluate the GME-handling capacity of these contemporary venous reservoirs, oxygenators and complete systems, as well as our currently used Sorin Synthesis, using the EDAC system. The venous reservoir of the Quadrox-i was the most effective in removing all sizes of GME and total GME load, while the Synthesis was the least effective. The FX15 and FX25 were least effective removing small GME, while the FX15 and Quadrox-i were the least effective at removing medium GME. The Quadrox-i was least effective at removing large GME. In terms of complete venous reservoir/oxygenator systems, the Synthesis permitted the greatest amount of GME to pass, while the other systems appeared largely equivalent.
Introduction
During cardiopulmonary bypass (CPB), gaseous and particulate emboli represent a major risk to cardiac surgery patients. In terms of gaseous emboli, advances in modern cardiopulmonary bypass equipment and practice have limited the incidence of fatal gross air embolism during cardiac surgery. However, CPB is known to generate gaseous microemboli (GME) which can present a significant risk to patient outcomes. These emboli may partially obstruct end-organ blood flow, resulting in regional ischemia. If they are delivered to the brain, GME may cause post-operative cognitive dysfunction, ranging from transient to permanent defects. 1
A number of potential sources of GME during CPB have been identified. These include increased blood viscosity (hypothermic), increased number of extracorporeal circuit (ECC) connections, cardiotomy suction, aortic cannula type and placement, sampling and injection ports, use of vacuum-assisted venous drainage, use of high blood flow rates and high temperature gradient and properties of the oxygenator and filters (reviewed in 2,3).
Clinically, the detection of GME has been largelyconducted using transcranial Doppler which can only detect bubbles greater than 40 µM. The majority of GME during CPB are less than 40 µM.4,5 More recently, other GME detection systems have been employed clinically in the operating room that can detect smaller GME, including the emboli detection and classification quantifier (EDAC) system (Luna Innovations, Roanoke, VA, USA). An important question that has remained largely unanswered, however, is the critical GME load that will skew defects. A recent in vivo study attempted to identify an association between the intensity of GME load during CPB, neurocognitive testing and clinical outcomes. Dognanci et al. demonstrated a significant decrease in three of four neurocognitive tests at one week post-op in patients who were observed to receive greater than 500 GME during CPB compared to patients who received less than 250 GME during CPB. However, there were no differences one month post-op. 1
While the acceptable level of GME during CPB remains unanswered, manufacturers of CPB equipment have recognized the importance of reducing GME. Subsequently, advancements in CPB equipment design, specifically the venous reservoir, oxygenator and arterial filters, have been shown to provide significant improvements in GME removal.3,6 For example, a recent, in vivo study evaluated the efficacy of using a 20 µM arterial filter instead of the commonly utilized 40 µM arterial filter in emboli reduction. While the 20 µM arterial filter was superior at removing emboli greater than 30 µM, the overall emboli count was not found to be significantly reduced. 7 This contradiction may be due to the fact that smaller GME are more common during CPB and are skewing the counts. Unfortunately, total embolic load was not reported, as this may have strengthened the evidence for using a smaller arterial filter during CPB.
The first opportunity to eliminate GME entering the circuit is at the venous reservoir. Many studies evaluating past venous reservoirs have demonstrated significant differences in air handling.8,9 These have underscored the impact of blood flows 9 and operating volumes on GME transmission, reporting that air handling is compromised with higher blood flows and lower operating volumes.8,9 The latter is of particular interest as the trend in venous reservoir design is reduced minimal operating volumes in order to achieve reduced patient hemodilution. Any GME that are not eliminated by the venous reservoir must now be eliminated by the oxygenator and arterial filter.
In the past couple of years, a number of new venous reservoirs/oxygenators with integrated arterial filters have entered the market. In addition to other performance indicators, companies present their products as possessing optimal GME handling capacity.
The goal of the current study was to evaluate the GME removal capacity of these venous reservoirs/oxygenators with our current system as part of a best-model determination initiative to identify the ideal product to protect our patients from GME exposure.
Methods
EDAC: To quantify and determine sizes of GME, the emboli detection and classification quantifier (EDAC) system (Luna Innovations) was used. EDAC is one of the two available clinical microbubble-counting devices currently available. An analyzer attached to a cuvette permits quantification of total embolic load, total embolic counts and counts of different size emboli (10 µM to greater than 100 µM). With this device, multiple detectors (channels) can be used to collect GME data simultaneously at multiple sites within a CPB circuit.
For this research, the EDAC system at the Terumo Plant in Elkton, ML was used. Being cognizant of the perception of company interference, the researchers and Terumo lawyers agreed to a legal letter of understanding that the researchers alone would operate the evaluation system, run the analysis software and analyze the data without interference by Terumo representatives. Furthermore, that the data collected was the property of the researchers since the goal of this evaluation was publication. Following training on the EDAC system, the Terumo representatives left the evaluation area.
Oxygenators: Oxygenators evaluated included the Sorin Synthesis, the Sorin Inspire6, the Sorin Inspire8, (Sorin Group Canada Inc., Markham, ON) the Terumo FX15, the Terumo FX25 (Terumo Medical Corporation, Burlington, ON) and the Maquet Quadrox-I (Maquet Cardiopulmonary AG, Hirrlingen, Germany), along with the associated venous reservoirs. The order of the oxygenators was randomized prior to evaluation. The oxygenators were flushed with CO2 (3 liters per minute for 5 minutes) prior to priming with normal saline and de-airing as per the individual product’s Instructions for Use. The saline was then replaced with fresh bovine blood, which was warmed to 36 ± 1oC.
GME Evaluation Circuit: Refer to Figure 1. The evaluation circuit consisted of a bucket containing 15 liters of fresh bovine blood (Hct 30 ± 3, pH 7.1 ± 0.1, base excess 0 ± 1). This bucket was connected to the venous reservoir via 3/8” internal diameter tubing. Prior to connection with the venous reservoir, a 3/8” Luer-lock connecter was inserted. A 3-way stopcock was attached to ¼” tubing which was placed in a roller pump set at a flow rate of 100 ml/min and was connected to this connector such that room air could be introduced into the circuit prior to the venous reservoir. The orientation of the venous line was parallel to the floor and remained consistent for all tests. From the venous reservoir, the tubing went through a roller pump raceway of a Terumo System-1 heart-lung machine and into the oxygenator being evaluated. A line of 3/8” internal diameter tubing from the arterial outlet of the oxygenator returned to the bucket.
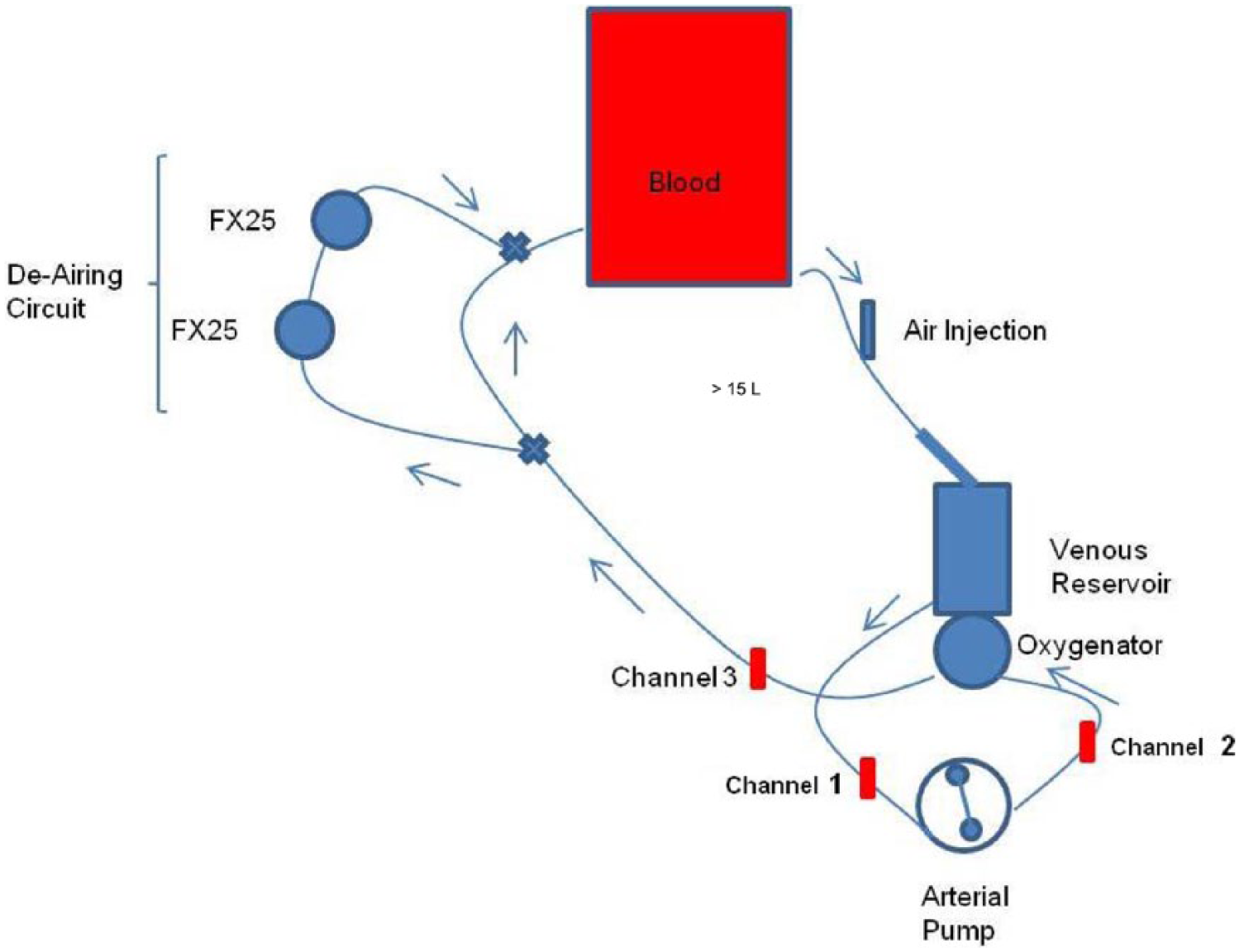
Three EDAC unit bubble sensors were placed in the circuit: Channel 1 in the tubing coming out of the venous reservoir, Channel 2 in the tubing coming out of the roller pump and Channel 3 in the tubing coming out of the oxygenator. This permitted monitoring of GME leaving the venous reservoir (Channel 1), leaving the roller pump (Channel 2) and leaving the oxygenator (Channel 3). From these, the efficacy of GME removal by the venous reservoir, the oxygenator and the entire system could be evaluated.
The roller pump occlusion was checked after the blood was warmed to 36 ± 1oC. After the pump speed was set to 4 liters per minute, a variable-resistance clamp was applied to the arterial outlet of the oxygenator distal to the Channel 3 sensor and adjusted to set the outlet pressure to 200 mmHg. Prior to the introduction of room air, purge/re-circulation lines were closed (or left open as per each product’s Instructions for Use) and the sampling manifold was left open. Further, GME activity in all three channels was at or below 10 counts per 6 second intervals to establish a low baseline. The volume in the venous reservoir was then brought to the minimum operating level as described in each product’s Instruction for Use. The air introduction system consisted of ¼” tubing attached to the pre-venous reservoir stopcock being placed in the raceway of a roller pump set to 100 ml/min. To introduce air into the circuit, the stopcock was opened to the circuit.
Air Introduction: One researcher operated the EDAC system while the other was responsible for maintaining the minimal venous reservoir, as recommended by the manufacturer, and introducing air. Using the minimal venous reservoir level recommended by the manufacturer was hypothesized to provide a significant GME-handling challenge for these products as past work indicated that GME handling was reduced at lower reservoir levels.8,9 To establish a baseline, the EDAC system was initiated 30 seconds prior to the introduction of room air. At the end of this time, the stopcock was opened to introduce air into the system. Air was introduced at a rate of 100 ml/minute for one minute. GME data were continuously collected by all three EDAC channels over this time in 6 second intervals. Following data collection, the de-airing circuit was opened such that tandem Terumo FX25 oxygenators could accelerate air removal and return to baseline (<10 GME/6 seconds). A new circuit was used for each oxygenator evaluation.
Data Analysis: Collected data was immediately saved and imported into Microsoft Excel®. Data were binned into three categories of GME based on size: small (10-49 µM), medium (50 – 99 µM) and large GME (>100 µM). For all three channels, the 30-second baseline values (total embolic load, total embolic count and counts of differently sized emboli) were subtracted from those collected during air introduction to account for any potential variation in the GME baseline. The data are presented as mean ± standard deviation.
Given the limited time permitted to conduct the current evaluation, each venous reservoir/oxygenator combination could only be subjected to two air-handling trials. As such, the data presented could not be subjected to rigorous statistical analysis. Instead, this evaluation of GME handling by venous reservoir, oxygenator and complete system are more qualitative in nature.
To evaluate the venous reservoirs, data collected by Channel 1 were used. These data included quantification of GME of each size category (small, medium and large), as well as total embolic load. Total embolic load was calculated by the EDAC software in cubic centimeters of air. To evaluate the oxygenators, data collected by Channel 2 and Channel 3 were used. For this, percentage removal by the oxygenators was calculated as: {1- (Channel 3/Channel 2) X 100}. GME removal was calculated for each size of GME. To evaluate the complete system (venous reservoir and oxygenator), data collected by Channel 3 were used. For this, total embolic load values were analyzed.
Results
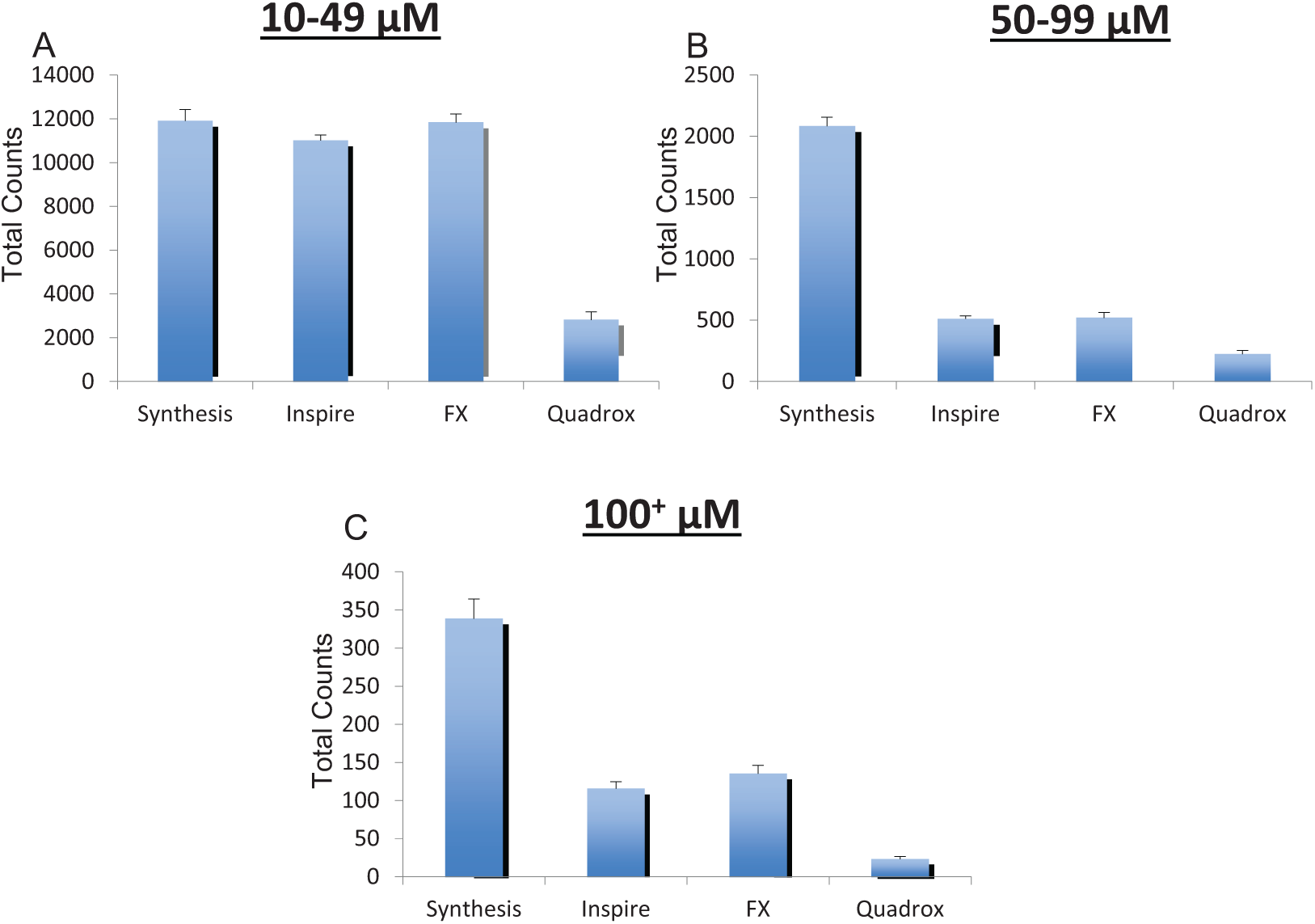
Venous reservoir: When air was introduced into the venous inlet of the CPB circuit (100 ml over one minute), the efficacy of the venous reservoirs at removing the air was evaluated using data from Channel 1(immediately distal to the reservoir). Data collected from this sensor permitted quantification of small (10-49 µM), medium (50-99 µM) and large (>100 µM) GME as well as the overall embolic load that passed through the reservoir. The venous reservoirs of the Synthesis, Inspire and FX oxygenators demonstrated comparable capability at removing small GME, while the Quadrox-i was the most efficient (Figure 2A). The venous reservoir of the Synthesis was noticeably the least effective at removing medium GME, while the Inspire and FX appeared equally efficient. The Quadrox-i appeared the most efficient (Figure 2B). The venous reservoir of the Synthesis was markedly the least effective at removing large GME, while the Inspire and FX were equally efficient. The Quadrox-i was the most efficient (Figure 2C.)
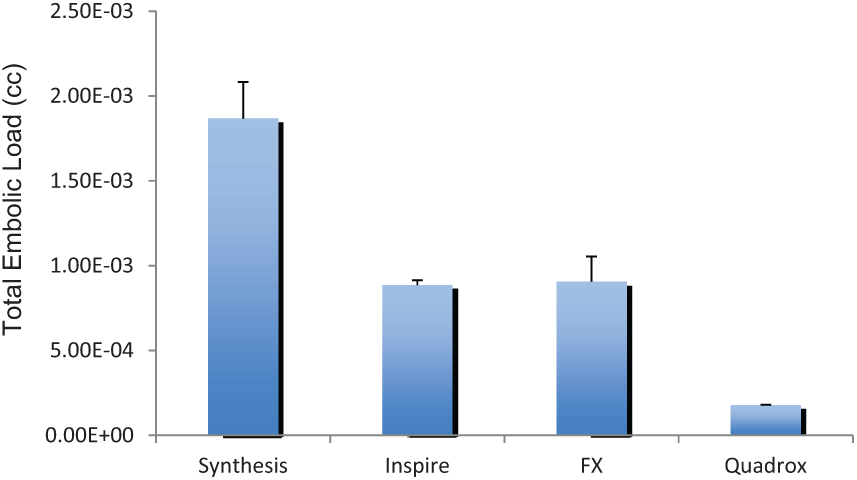
The venous reservoir handling of total embolic load was next examined (Figure 3). The venous reservoir of the Synthesis permitted the greatest total embolic load to exit. The venous reservoirs of the Inspire and FX oxygenators were comparable at reducing total embolic load. The venous reservoir of the Quadrox-i was noticeably the most efficient.
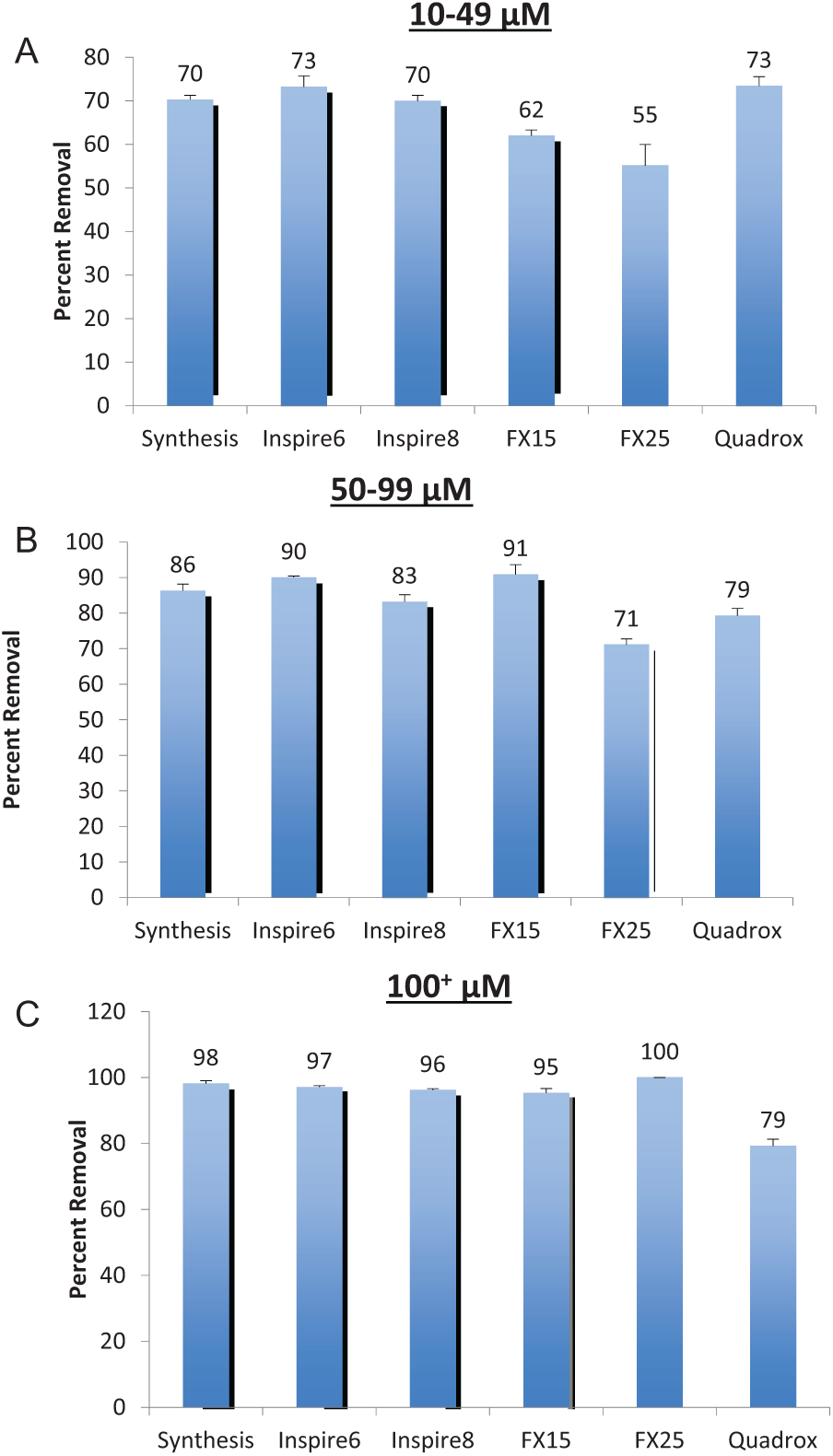
Oxygenator: The efficacy of the oxygenators at removing small, medium and large GME was evaluated using data collected from Channel 2 and Channel 3 and calculating the percentage of GME removal. The Sorin oxygenators and the Quadrox-i were most effective at removing small GME (Figure 4A), removing between 70% and 73%. The FX15 and FX25 were least effective, removing 62% and 55% of small GME, respectively. All the oxygenators were more effective at removing medium-sized GME (Figure 4B). The Inspire 6 and FX15 were the most effective, removing 90% and 91%, respectively. The FX25 was the least effective, removing 71% of medium-sized GME. Large GME were the most effectively removed by the oxygenators, in general. Most oxygenators removed over 90% of large GME, with the FX25 appearing the most effective, removing 100% (Figure 4C). The Quadrox-i was least effective, removing 79% of large GME.
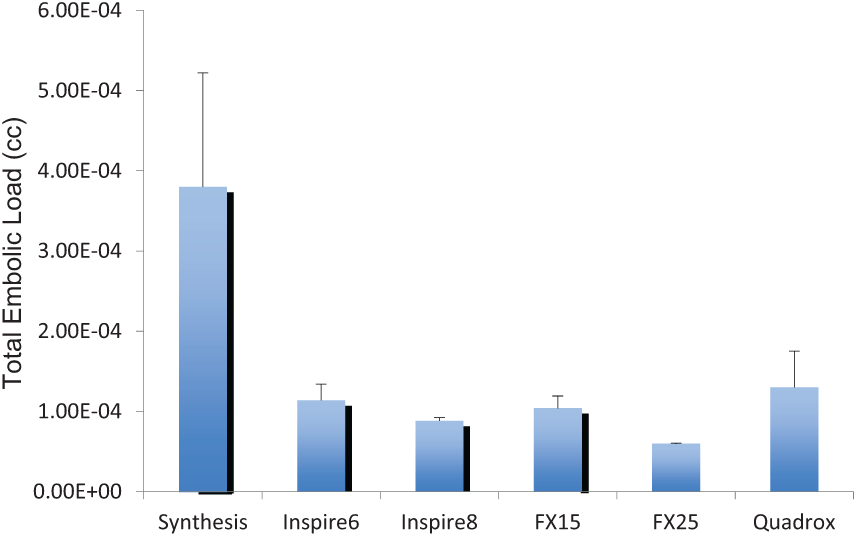
Complete system: The final component of the current GME evaluation was the assessment of total embolic load handling by each venous reservoir/oxygenator system using data from Channel 3 (Figure 5). The Synthesis venous reservoir/oxygenator system permitted the largest total embolic load to pass through to the outlet of the oxygenator. The other venous reservoir/oxygenator systems were largely equivalent at reducing total embolic load.
Discussion
As part of new oxygenator development, both Sorin and Maquet have re-designed their respective venous reservoirs. While the previous Maquet Quadrox venous reservoir was not part of the study and cannot be commented on, the Sorin has clearly made significant improvements over the Synthesis venous reservoir. The Inspire venous reservoirs, while comparable to the FX venous reservoirs were markedly more efficient in managing GME than the Synthesis. However, the Quadrox-i venous reservoir demonstrated superior GME handling. While the structural design of this venous reservoir may be responsible for this outcome, it is important to note that it is the only one that has Anti-Foam C in the venous inlet line. All the other new products have Anti-Foam C in the sucker/vent inlet systems and at various volumes in the reservoir itself (e.g. Inspire has Anti-Foam C that contacts the blood at a reservoir level above 1800 mL). An earlier anti-foam agent, Anti-Foam A, fell out of favor in cardiac surgery as it was found to transfer into the blood and micro-embolize. 10 Subsequently, autopsies of CPB patients detected the presence of Anti-Foam A in capillary beds and hypothesized it to be a contributing factor in patient morbidity and/or mortality. While Anti-Foam C is FDA-approved, the authors could not find literature for its safe use for CPB equipment.
In general, all the oxygenators were better at handling larger GME in comparison to small GME. The Quadrox-I, interestingly, did not have the same marked improvement in removing GME of increasing size as the other oxygenators and was the worst at removing large GME. Since larger GME may be more likely to have detrimental effects on patient outcomes, this is an important finding. This weakness is, however, offset by the efficiency of the Quadrox-i venous reservoir at removing GME prior to entry into the oxygenator. This makes the Quadrox-i system an interesting scenario: a highly efficient venous reservoir coupled with a relatively inefficient oxygenator. As observed in the overall embolic load of the complete system, the two individual components neutralized each other and are comparable to the Inspire and FX systems. Improvements to the Quadrox-i oxygenator air handling could greatly improve overall air handling by this system.
The data on GME removal by complete venous reservoir/oxygenator systems may be the most crucial as it reflects the total embolic load the patient would be subjected to in the event of air introduction into the venous line. Not surprisingly, the oldest system evaluated, the Synthesis system, was observed to permit the greatest embolic load to pass out the arterial side of the oxygenator. Sorin’s Inspire product line has much improved the air-handling capacity and likely reflects advancements in product design. Other complete systems are largely equivalent
By evaluating individual components, as well as the complete system, this study presents perfusion departments with an intriguing option: coupling the most efficient venous reservoir with the most efficient oxygenator to provide optimal patient protection against GME. Provided that Anti-Foam C is not detrimental to patients, the Quadrox-i would be the optimal choice for a venous reservoir. The choice of oxygenator would require consideration into which GME size is of greatest importance with small GME best removed by the Inspire or Quadrox-i oxygenators, medium GME best removed by the Inspire 6 or FX15 and large bubbles best removed by the Sorin or Terumo oxygenators.
A recent study evaluating the clinical characteristics of the FX25 and the Synthesis raised an interesting notion: a relationship between GME and extracorporeal circuit coating. Onorati et al. demonstrated evidence for the Synthesis having a reduced inflammatory response, improved coagulation protein conservation and increased serum proteins compared to the FX25 in a small sample of patients undergoing elective isolated aortic valve replacements. 11 The authors hypothesized that the effect may be due to differences in GME load, which may be, in part, due to differences in the coatings used by each company. In the current study, all oxygenators were coated as per company protocol (Sorin: Mimesys phosphorylcholine® coating, Terumo: Xcoating®, Maquet: SOFTLINE® coating), however, the tubing used for the circuit was uncoated. This permitted isolation of the venous reservoir/oxygenator sets, with reduced influence of the tubing coatings. A more thorough examination may have included comparing completely uncoated systems (tubing, venous reservoir/oxygenator) to fully coated systems. However, time did not permit this. The data in the current evaluation, in contrast to Onorati et al., demonstrate the Synthesis to be inferior at handling GME to the FX25 and all the other systems evaluated. The implication of this finding is that the hypothesis from Onorati et al. that increased GME production from the FX25 compared to the Synthesis being responsible for differences in clinical outcome may not be correct, unless coating the entire circuit makes a significant difference. This is unlikely, however, as the largest surface area in the circuit will be in the oxygenator and the integrated arterial filter. Furthermore, as the current evaluation was an in vitro study with uniform testing conditions, confounding factors that would be present in a small in vivo assessment could be minimized.
One mechanism which has led to a reduction in both total volume and the size of GME has been the presence of an open arterial filter purge line. With the newer generation of oxygenators, arterial filters are no longer separate components, but, instead, are integrated into the oxygenator system. However, integrated arterial filters still contain a purge line. A consequence of this purge line is the diversion of a potentially large volume of blood away from the patient. 12 Both the Inspire and Quadrox-i have arterial filter purge lines that are to be kept open during CPB, in addition to the arterial manifold line. For example, according to the Instructions for Use for the Inspire8, there is “spontaneous flow of purge/recirculation line @ 150 mmHg arterial line pressure and 6 l/min main pump blood flow is approx. 620 ml/min with both purge lines open, 420 ml/min with pre-filter purge line open and 420 ml/min with post-filter purge line open.” 13 In contrast, the arterial filter purge line in the FX oxygenators are to be kept closed following de-airing, meaning that less blood will be diverted from the patient. The use of a flow-probe downstream of the oxygenator can negate the apparent reduction in patient flow if the Inspire or Quadrox-i systems are used. Regardless, it is important that the perfusionist is aware of this large volume of diverted flow to provide the best patient care.
Recently, two new GME quantifiers were developed for clinical use during cardiac surgery. While the current study utilized EDAC to classify and quantify GME, the Gampt BC200 (GAMPT mbH, Merseburg, Germany) is also available. A recent study evaluated the accuracy of both devices against backlight shadowgraphy and optical counting (industrial reference techniques). 14 While both can be used in the clinical setting for the measurement of GME, each has important limitations. On average, the EDAC tends to underestimate bubble size while the Gampt BC200 tends to overestimate bubble size. Further, at low blood flow (3 liters per minute), the Gampt BC200 misses twice as many GME as the EDAC. At high blood flow (6 liters per minute), both miss the same percentage of GME.
Limitations: The first limitation of this in vitro evaluation is that each system was evaluated only twice due to time limitations at the Terumo facility. This made it difficult to perform rigorous statistical evaluation. Instead, the study is more qualitative in nature.
The effects of multiple variables on handling GME could not be evaluated. For instance, only a single blood flow rate, blood temperature and back pressure were used. In comparison, Matthas et al. evaluated GME handling of four pediatric oxygenators at different flows and temperatures and with shunts opened or closed. 12
Footnotes
Presented at the 36th Annual Seminar of The American Academy of Cardiovascular Perfusion, San Antonio, Texas 5-8 Feb 2015.
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.