
Abstract
We present a female patient with severe acute respiratory distress syndrome (ARDS) necessitating intubation and mechanical ventilation on the intensive care unit (ICU). High ventilatory pressures were needed because of hypoxia and severe hypercapnia with respiratory acidosis, resulting in right ventricular dysfunction with impaired haemodynamic stability. A veno-venous extracorporeal CO2 removal (ECCO2R) circuit was initiated, effectively eliminating carbon dioxide while improving oxygenation and enabling a reduction in applied ventilatory pressures. We noted a marked improvement of right ventricular function with restoration of haemodynamic stability. Within one week, the patient was weaned from both ECCO2R and mechanical ventilation. Besides providing adequate gas exchange, extracorporeal assist devices may be helpful in ameliorating right ventricular dysfunction during ARDS.
Introduction
Acute respiratory distress syndrome (ARDS) was first described in 1967. 1 There used to be a lack of a universally accepted definition, but, since 2012, ARDS has been defined by the Berlin criteria: “new or worsening respiratory symptoms developing within one week of a known clinical insult, with bilateral opacities on chest imaging, hypoxemic respiratory failure which cannot be fully explained by cardiac failure or fluid overload with a ratio of arterial oxygen tension to fraction of inspired oxygen (PaO2/FiO2) less than 300 mmHg during positive end-expiratory pressure equal to or higher than 5 cmH2O”. 2 ARDS develops in approximately 7% of patients admitted to the intensive care unit (ICU), with a mortality up to 60% in most patients requiring mechanical ventilation. 3 Usage of “lung protective ventilation” (keeping the maximum inflation pressure below 30 cmH2O and using low tidal volume ventilation of 6 to 8 ml/kg) has improved survival in patients with ARDS.4–7 However, as carbon dioxide elimination is determined by the difference in tidal and dead space volume ventilation multiplied by respiratory rate, a reduction in tidal volume can lead to hypercapnia, which may, consequently, result in respiratory acidosis. As hypercapnia and hypoxia have shown to increase right ventricular afterload while acidosis comprises ventricular function, right ventricular dysfunction is a common complication of ARDS, contributing to mortality.8,9 Furthermore, ARDS decreases lung compliance, resulting in atelectatic alveoli compressing extra-alveolar vessels with over-distension of the remaining alveoli compressing intra-alveolar vessels, both contributing to an increase in right ventricular afterload. 10 The application of the high mechanical ventilatory airway pressures needed to maintain adequate ventilation can further increase right ventricular afterload, reducing cardiac output and potentially resulting in the development of obstructive shock.
In patients with ARDS, adequate gas exchange during lung-protective ventilation can be supported on the ICU by extracorporeal lung support techniques, such as extracorporeal CO2 removal (ECCO2R) circuits, mainly facilitating carbon dioxide elimination in addition to moderate oxygenation, while extracorporeal membrane oxygenators (ECMO) provide complete oxygenation besides decarboxylation.11,12 Potentially, these devices may improve right ventricular function by enabling a reduction in applied ventilatory pressures while correcting hypoxia, hypercapnia and acidosis. However, right ventricular dysfunction could potentially be aggravated by a reduction in right ventricular preload due to the extracorporeal circulation. We report the right ventricular and haemodynamic effects after initiation of a veno-venous ECCO2R device in an ARDS patient.
Case History
A 19-year-old female without prior medical history had been admitted for treatment of a ketoacidosis triggered by new onset diabetes. On the second day, progressive dyspnoea with bilateral pulmonary infiltrates on chest X-ray developed, necessitating transfer to the ICU for endotracheal intubation and mechanical ventilation due to ARDS. All blood and urine cultures remained negative, but a few Staphylococcus aureus colonies were isolated from saliva for which intravenous flucloxacillin was started. Despite prone positioning and lung recruitment manoeuvers, mechanical ventilation with high ventilatory pressures was necessary to maintain acceptable gas exchange. With progressive pulmonary infiltrates on thoracic computed tomography (CT) scan, diuretics and steroids were given in the treatment of the ARDS, yet hypoxia, hypercapnia and acidosis worsened, with haemodynamic instability requiring vasopressors. In order to facilitate carbon dioxide removal during lung-protective ventilation, it was decided to install ECCO2R. Prior to initiation, a two-dimensional transthoracic echocardiogram was performed, ruling out severe left ventricular dysfunction while showing a severely dilated right ventricle. A single double-lumen cannula of 24 French gauge was inserted in the right femoral vein under ultrasound guidance and connected to a veno-venous (V-V) circuit and a carbon dioxide-eliminating membrane (MiniLung, Novalung, Hechingen, Germany) with a blood flow of 1.5 L/min (Figure 1). Within hours, ventilatory pressures were reduced with a decrease in tidal volume and carbon dioxide as well as an improvement in oxygenation (Table 1). Repeated echocardiography revealed a decrease in right ventricular dimensions with improved right ventricular function (Figure 2; Table 1). 13 The vasopressor dose could be reduced and stopped after 2 days. Within a week, ECCO2R was able to be discontinued, followed by endotracheal extubation. The following week, the patient was discharged from the ICU to the internal medicine ward for further recovery and treatment of her diabetes. At one-year follow-up, the patient was in good health with normal performance status.
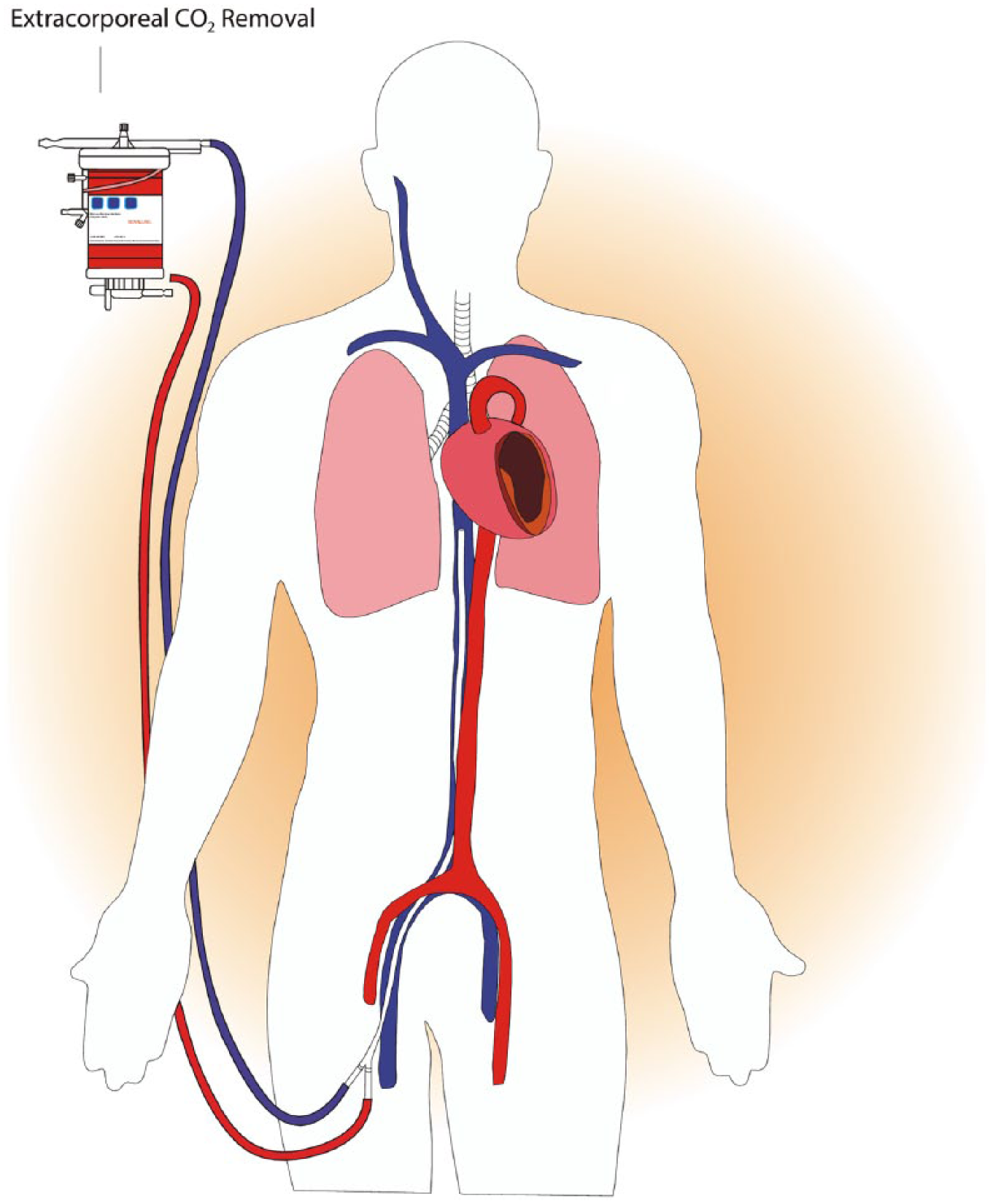
Veno-venous extracorporeal circuit using a single double-lumen cannula connected to an extracorporeal carbon dioxide-eliminating membrane (pump with additional tubing not shown). As approximately 1.5 L/min blood flows through the membrane, the ventilator has the capacity for removing more than 250 ml carbon dioxide per minute, which exceeds carbon dioxide production.
Changes in mechanical ventilator settings and arterial blood gas, ventricular and haemodynamic parameters before and after two hours of decarboxylation by ECCO2R.
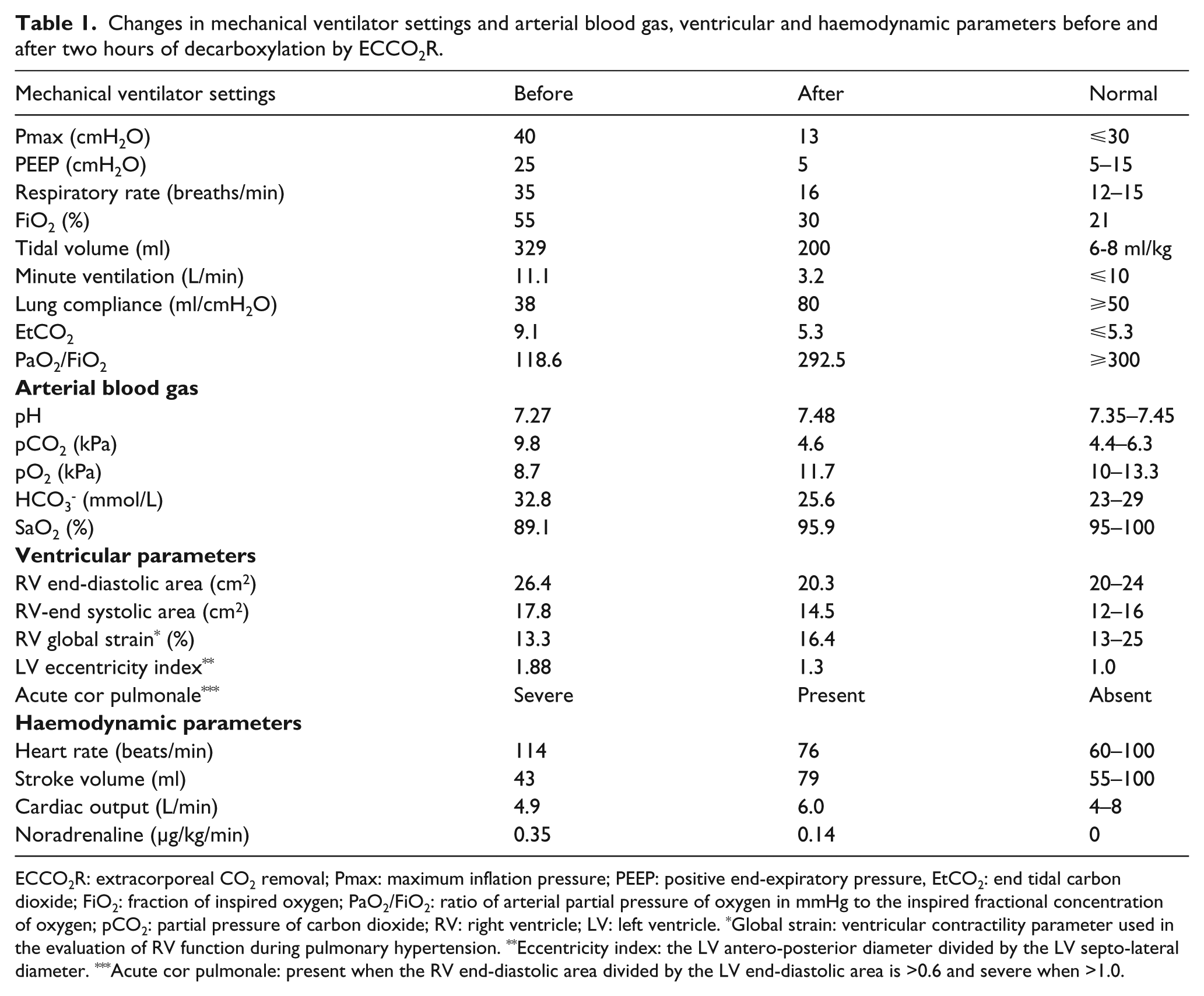
ECCO2R: extracorporeal CO2 removal; Pmax: maximum inflation pressure; PEEP: positive end-expiratory pressure, EtCO2: end tidal carbon dioxide; FiO2: fraction of inspired oxygen; PaO2/FiO2: ratio of arterial partial pressure of oxygen in mmHg to the inspired fractional concentration of oxygen; pCO2: partial pressure of carbon dioxide; RV: right ventricle; LV: left ventricle. *Global strain: ventricular contractility parameter used in the evaluation of RV function during pulmonary hypertension. **Eccentricity index: the LV antero-posterior diameter divided by the LV septo-lateral diameter. ***Acute cor pulmonale: present when the RV end-diastolic area divided by the LV end-diastolic area is >0.6 and severe when >1.0.
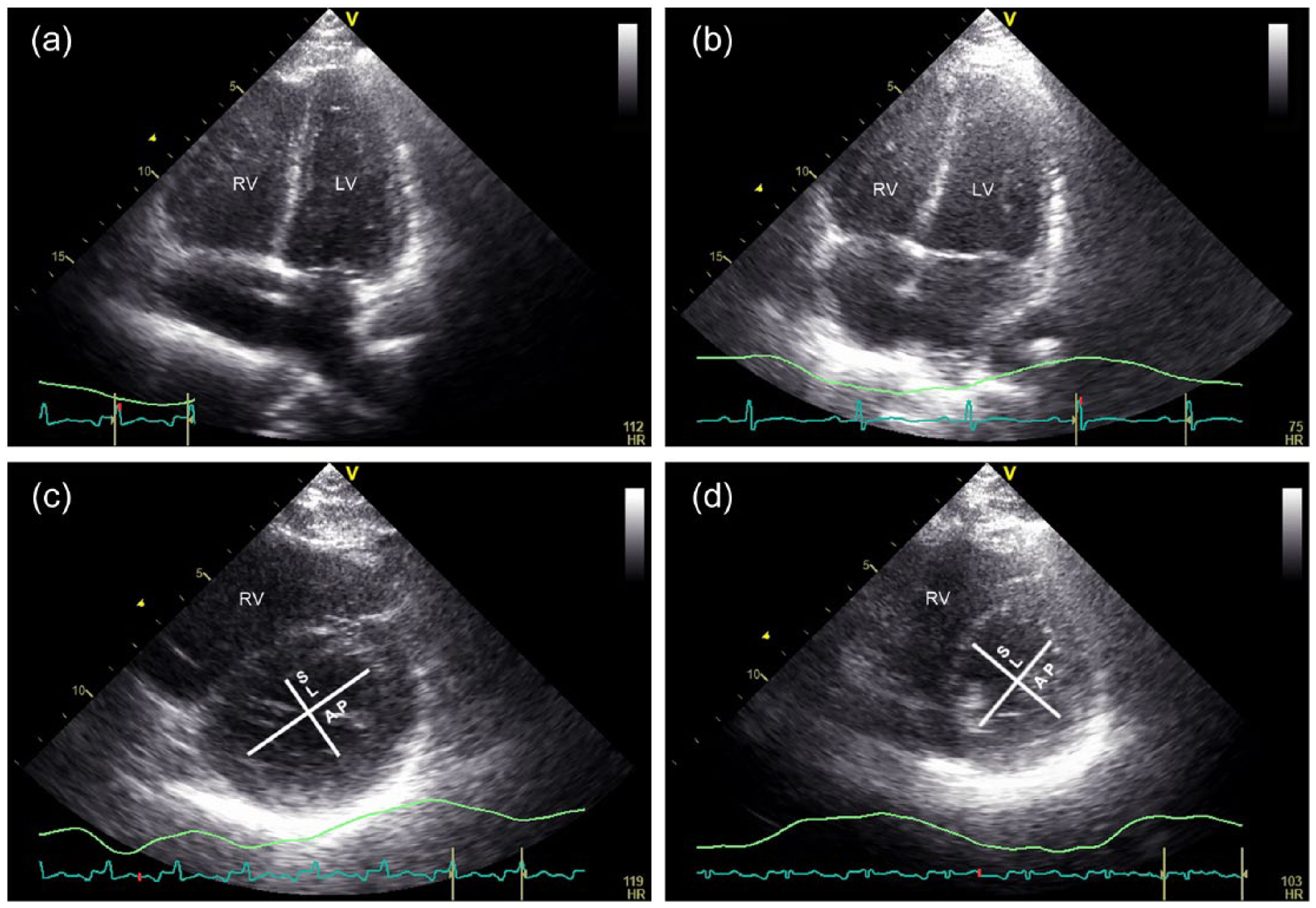
Ventricular dimensions before and 2 hours after implementation of extracorporeal CO2 removal (ECCO2R). Initially, the right ventricular end-diastolic area exceeded the left ventricular end-diastolic area, corresponding with a severe acute cor pulmonale (a), which diminished after ECCO2R (b). In comparison, the left ventricular eccentricity index, determined by the antero-posterior (AP) diameter divided by the septo-lateral (SL) diameter, was initially increased, demonstrated by a D-shaped left ventricle (c). After ECCO2R, the left ventricular eccentricity index nearly normalised, with a return to its round shape indicating a decrease in right ventricular afterload (d).
Discussion
The V-V ECCO2R circuit can provide effective carbon dioxide elimination, yet only modest improvement in oxygenation when using a single double-lumen cannula limiting blood flow. At merely 1.5 L/min blood flow, more than 250 ml carbon dioxide per minute can be removed by the membrane, exceeding normal carbon dioxide production and forming the basis for low-flow decarboxylating extracorporeal devices. When oxygenation is required as well, two venous cannulae for V-V ECMO are necessary to attain a sufficiently high blood flow as oxygen diffuses 20-times slower than carbon dioxide. 14 Veno-venous extracorporeal circuits have become more durable and biocompatible in recent years and are now increasingly used as an adjunct to conventional mechanical ventilation to enable lung-protective ventilation on the ICU.
Important additional benefits of ECCO2R may include improvement in right ventricular function. Under normal circumstances, the pressure rise in the right ventricle quickly exceeds the low pressure in the pulmonary artery, which largely determines right ventricular afterload. However, the right ventricle is quite sensitive for elevations in afterload, with a small increase resulting in a decrease in right ventricular output, with a subsequent increase in right ventricular end-systolic volume. The interventricular septum, subsequently, can move towards the left ventricle during systole, which can be objectified by the determination of the so-called eccentricity index (Figure 2c), causing a decrease in left ventricular preload. The reduction in cardiac output can lead, eventually, to the development of obstructive shock. If venous return remains unchanged on top of the already increased right ventricular end-systolic volume, right ventricular end-diastolic volume will increase as well. When the right ventricular end-diastolic area is more than 60% of the left ventricular end-diastolic area, acute cor pulmonale is present, which has been demonstrated to increase mortality in ARDS. 9 When the right ventricular end-diastolic area even supersedes the left ventricle, severe acute cor pulmonale is present, as was the case in our patient (Figure 2a).
Prior to initiating V-V ECCO2R, echocardiography should be performed to exclude severe left ventricular dysfunction that might require a veno-arterial extracorporeal system for circulatory support. In our patient, with respiratory failure resulting in severe hypercapnia, ECCO2R could be used in the absence of overt left ventricular dysfunction and severe hypoxemia. The presence of pulmonary hypertension was thought to be a contraindication as well, but pulmonary artery pressure has shown to decrease following treatment with V-V extracorporeal devices, mainly ascribed to a reduction in hypoxic and hypercapnic pulmonary vasoconstriction.14,15 To our knowledge, the effect of ECCO2R on right ventricular parameters has not been specifically studied before. We observed a marked decrease in right ventricular dimensions with improved right ventricular function as a result of achieving normocapnia in combination with the reduction in ventilatory pressures. The subsequent observed increase in stroke volume and cardiac output implies that a possible decrease in right ventricular preload was not a major factor, probably since the V-V ECCO2R circuit returns blood in the venous system with only 250 ml blood in the extracorporeal circuit.
In conclusion, treatment with ECCO2R resulted in improved haemodynamic and right ventricular parameters and enabled lung-protective ventilation in our patient with severe ARDS. Since right ventricular dysfunction is a major determinant of the outcome in ARDS, mortality will remain high as restrictions in mechanical ventilatory pressures and tidal volumes, frequently, are not attained on ICUs in the real world. 16 The use of ECCO2R is a promising tool in ARDS to facilitate lung-protective ventilation while maintaining adequate gas exchange, ameliorating right ventricular dysfunction.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.