
Abstract
This observational study aimed to investigate the relationship between renal injury, endothelial function and oxidative stress in claudicants undergoing maximal treadmill exercise. Twenty patients with claudication were identified in whom the urinary N-acetyl-β-D-glucosaminidase (β-NAG)/creatinine ratio, plasma oxidative state and endothelial function were tested pre- and post-maximal treadmill walking exercise. Of the 20 participants in this study, the urinary NAG/creatinine (Cr) rose from a pre-exercise level of 8.9, 6.7 to 14.3 (μmol/L/mmol Cr; median, IQR) to 12.9, 9.1 to 17.7 post exercise (p = 0.0003, Mann Whitney U test). Of the 20 participants, eight participants had a rise of the NAG/Cr ratio post exercise whereas 12 did not. Participants with a rise in the NAG/Cr ratio post exercise had a greater ability to increase endothelial reactivity (%; median, IQR; 2.56, 0.1 to 3.7) cf. (0.1, −4.8 to 0.9, p = 0.03); they also walked further (metres; median, IQR; 415, 208 to 908) cf. (170, 100 to 315, p = 0.04), had a lower pre-exercise H2O2 (median, IQR; 1.9, 1.4 to 2.3 cf. 2.7, 2.1 to 3.3; p = 0.04) and a greater rise in H2O2 post exercise (18.8, −1.5 to 129.7 cf., −7.7, −13.9 to −2.0, p = 0.04). The mechanism by which the phenotypically distinct sub-group of patients with intermittent claudication who experience a NAG/Cr rise involves complex interactions between systemic oxidative stress and endothelial function. Implications on cardiovascular risk in this group requires further investigation.
Introduction
Peripheral arterial disease is common, intermittent claudication having a prevalence of five per cent over the fifth decade of life. 1 Despite the relatively benign prognosis for the affected leg, intermittent claudication is associated with systemic atherosclerosis. 2 Compared with age-matched controls, people with intermittent claudication have a three- to six-fold increased chance of dying as a result of cardiovascular events. 3
In patients with intermittent claudication, exercise-induced tissue ischaemia causes a local response, including the accumulation of anaerobic metabolites and the synthesis of oxygen free radicals followed by reperfusion and potentially deleterious systemic manifestations. 4 It has been shown that there are increases in urinary microalbumin excretion, neutrophils and plasma thromboxane after exercise in claudicants. This low-grade ischemia-reperfusion in claudicants leads to damage of local tissues and remote organs. 5 Preliminary studies in our department have demonstrated that patients who have peripheral vascular disease develop ischaemia reperfusion injury, leading to a local and systemic inflammatory response, such as renal tubular injury. Urinary N-acetyl-β-D-glucosaminidase (β-NAG), a sensitive and specific marker of renal injury, was found to be elevated in the claudicants compared to the controls, suggesting renal tubular injury. 6
The primary aim of this study was to investigate the existence of a ‘vulnerable’ subgroup of claudicants who are more susceptible to acute kidney injury as assessed by a rise in the NAG/Cr ratio. The secondary aim was to investigate the relationship between plasma oxidative stress, endothelial function and acute kidney injury in claudicants undergoing treadmill exercise.
Methods
Potential participants were identified from the arterial database maintained at the vascular laboratory at the Hammersmith Hospital, London. All patients with intermittent claudication under surveillance were invited to participate. Patients with leg pain when at rest and/or skin ulceration were excluded. Exclusion criteria were any concomitant disease preventing treadmill exercise, e.g., due to heart disease, lung disease or musculoskeletal pain. Dialysis-dependent renal failure patients were not recruited. Patient demographics, comorbidities and medications as well as ankle-brachial pressure indices (ABPI) were recorded. UK National Research Ethics Service (NRES) approval was granted and written informed consent of the patients was obtained. The consent process was approved by the NRES committee.
A standard testing protocol was followed: ambulant patients were asked to empty the bladder before a 90-minute rest period (to avoid interference from the exercise of walking to the vascular laboratory). Following rest, urine and blood samples were collected and temporarily stored on ice in sterile standard tubes. A blood pressure cuff was placed around the participant’s upper right forearm. Flow-mediated dilation (FMD) of the participant’s right brachial artery was assessed with B mode ultrasound with the M7 portable ultrasound machine (Mindray 7, Shenzhen, China), using a 40-mm 5–10 MHz broadband linear array transducer. Longitudinal section images, approximately 2 to 3 cm above the elbow joint, were used, as previously described. 7 Briefly, the arm was positioned on an arm board attached to the examination couch. The arm was stabilised using a vacuum beanbag attached to the arm board. The blood pressure cuff was inflated to 30 mmHg above the systolic blood pressure. Inflation was maintained for a period of three minutes. Following the release of the blood pressure cuff, the brachial artery scan was repeated. The participant was then asked to walk briskly on a treadmill (10 per cent incline; 4 miles/hour) until they could not tolerate their typical claudication pain. The maximal walking distance was recorded. Further blood and urine samples were taken and temporarily stored on ice; FMD assessment was repeated on the same arm.
Five percent of protease inhibitor cocktail (Sigma-Aldrich, Gillingham, UK) was added to the urine samples which were stored at −70°C until they could be analysed as a single batch. Urinary N-acetyl-β-D-glucosaminidase (NAG) enzyme and creatinine levels were measured using the ELISA technique and plate reader. The NAG/Cr ratio was calculated to normalize for differences in urine output volumes. Freshly collected heparinized whole blood was used for the assessment of oxidative stress and antioxidant defense capacity: the ‘point-of-care’ free oxygen radicals test (FORT) and the free oxygen radicals defense test (FORD; FORM®, CR 2000, Parma, Callegari, Italy). 8
Data was analysed using Microsoft Excel (2010 edition) and SPSS (version 20). Data was expressed as median; interquartile range as was not normally distributed and non-parametric tests were used for significance testing; significance was taken at the five percent level. Formal sample size calculation was not performed and this study was conducted as a pilot from which further studies could be designed.
Results
Demographic data
Twenty participants agreed to participate in this study. Their characteristics are summarised in Table 1. Further details of individual participants are included in Table 2.
Demographic data for total cohort and participants who had a rise versus no rise in NAG/Creatinine ratio post exercise. Except for the maximum walking distance, there were no significant differences between those who had a rise versus no rise.

NAG: N-acetyl-β-D-glucosaminidase ABPI: ankle-brachial pressure index; IQR: interquartile range; BMI: body mass index.
Demographic data of patients with no rise in NAG/Creatinine ratio post exercise.
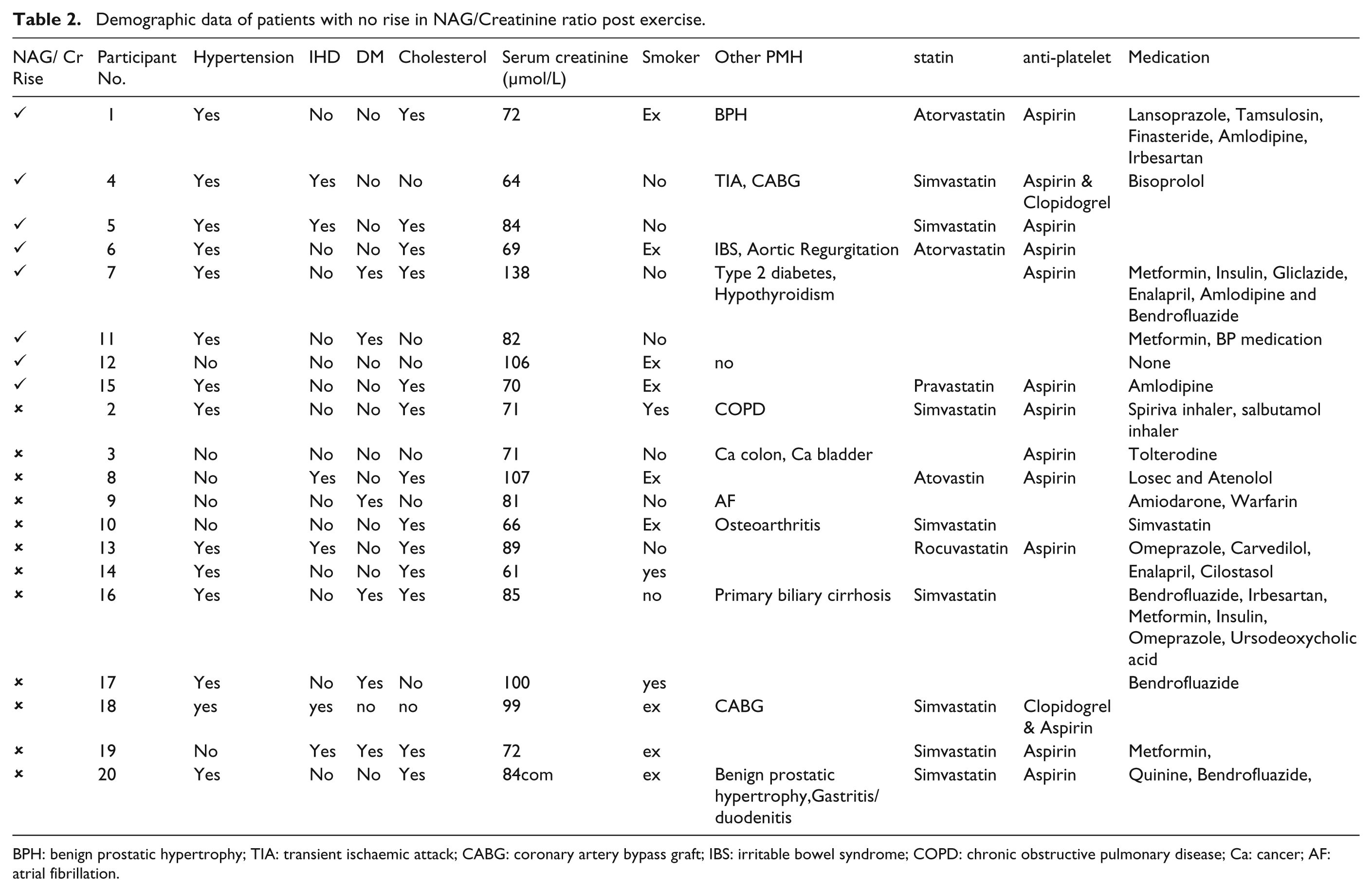
BPH: benign prostatic hypertrophy; TIA: transient ischaemic attack; CABG: coronary artery bypass graft; IBS: irritable bowel syndrome; COPD: chronic obstructive pulmonary disease; Ca: cancer; AF: atrial fibrillation.
Urinary NAG/Creatinine ratio in claudicants pre and post exercise
The urinary NAG/Cr rose from a pre-exercise level of 8.94, 6.73 to 14.27 (μmol/L/mmol Cr; median, IQR) to 12.90, 9.07 to 17.72 post exercise (p = 0.0003, Mann Whitney U test; Figure 1). There was a positive correlation between the percentage change in FMD post exercise and percentage change NAG/Cr ratio post exercise, R = 0.56 (p = 0.02; Spearman’s rank correlation). There was a similar positive correlation between percentage change in H2O2 post exercise with the percentage change in NAG/Cr ratio post exercise, R =0.51 (p = 0.04; Spearman’s rank correlation). However, there was a negative correlation between the percentage change post exercise of NAG/Cr with the pre-exercise H2O2, Rs = −0.47 (p = 0.04; Spearman’s rank correlation; Figure 1).
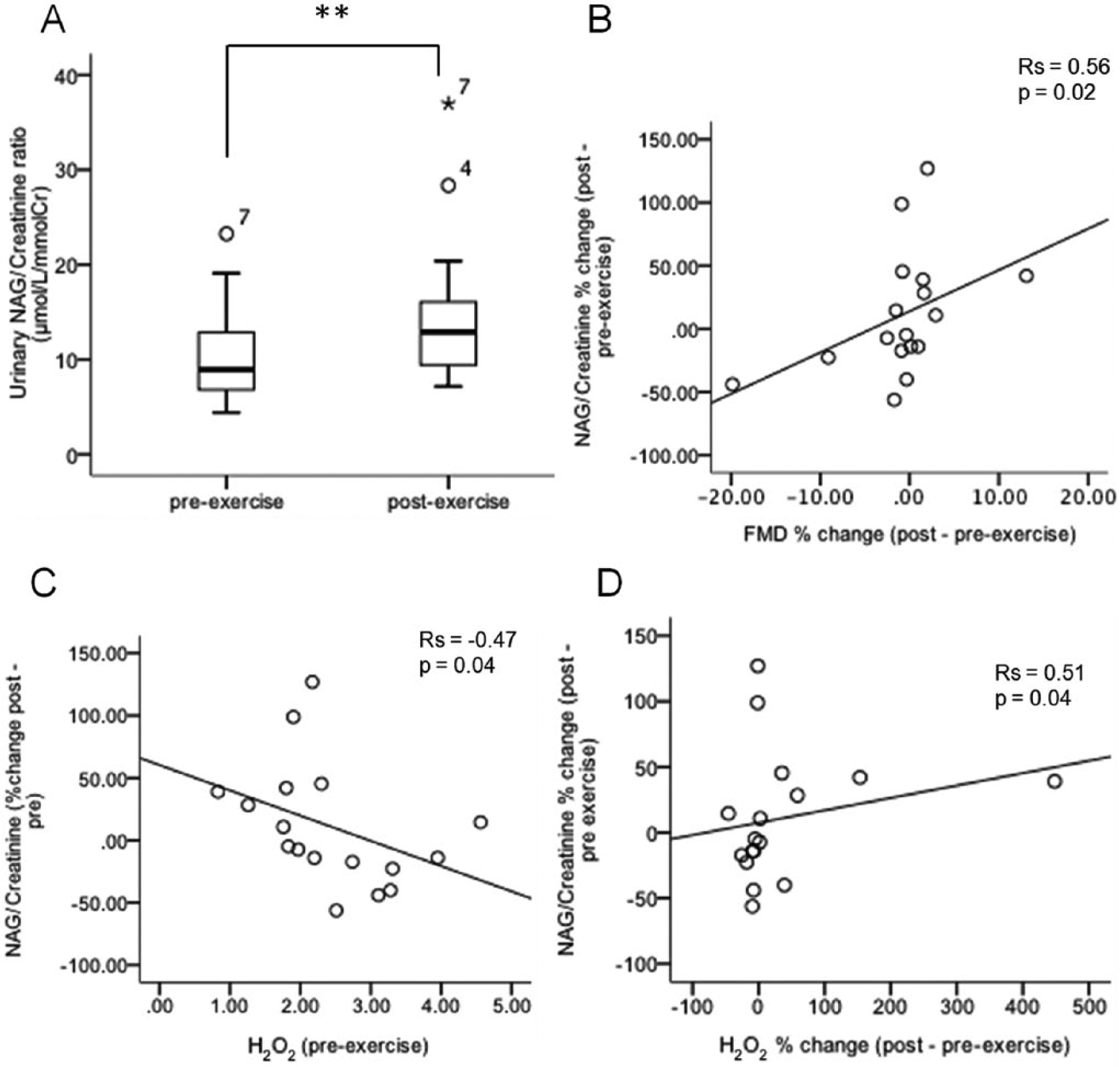
A) Box plot demonstrating urinary NAG/Cr ratio pre and post exercise. Scatter graphs of: B) percentage change in endothelial function (FMD) post exercise versus percentage change in NAG/Cr ratio post exercise; C) pre-exercise oxidative stress versus change in NAG/Cr ratio post exercise; D) Scatter graph of percentage change in oxidative stress post exercise versus percentage change in NAG/Cr ratio post exercise. **, p<0.01).
Characteristics of claudicants with NAG/Cr rise versus no rise on exercise
The claudicant cohort was segregated into those with any rise in NAG/Cr ratio post exercise (n=8) versus those who did not (n=12) (Figure 2). It was found the group who had a rise in the NAG/Cr ratio had a greater ability to increase FMD (%; median, IQR; 2.56, 0.13 to 3.7) than those without a rise (0.09, −4.82 to 0.91, p=0.03, Mann Whitney U test). Similarly, the group with a rise in the NAG/Cr ratio post exercise were able to walk further (metres; median, IQR; 415, 208 to 908) compared to those without a rise (170, 100 to 315, p = 0.04, Mann Whitney U test). Also, the group with a rise in the NAG/Cr ratio post exercise had a significantly lower pre-exercise H2O2 (median, IQR; 1.85, 1.39 to 2.27 cf. 2.74, 2.09 to 3.30; p = 0.04, Mann Whitney U test) as well as a significantly greater rise in H2O2 post exercise (18.75, −1.53 to 129.70 cf., −7.72, −13.85 to −1.97, p=0.04, Mann Whitney U test). Demographics, ABPI, use of ‘Best Medical Therapy’ (in the form of an antiplatelet agent and statin), blood pressure, history of diabetes or ischaemic heart disease or serum creatinine do not distinguish the group with a rise in NAG/Cr ratio post exercise from those with no rise (Table I).
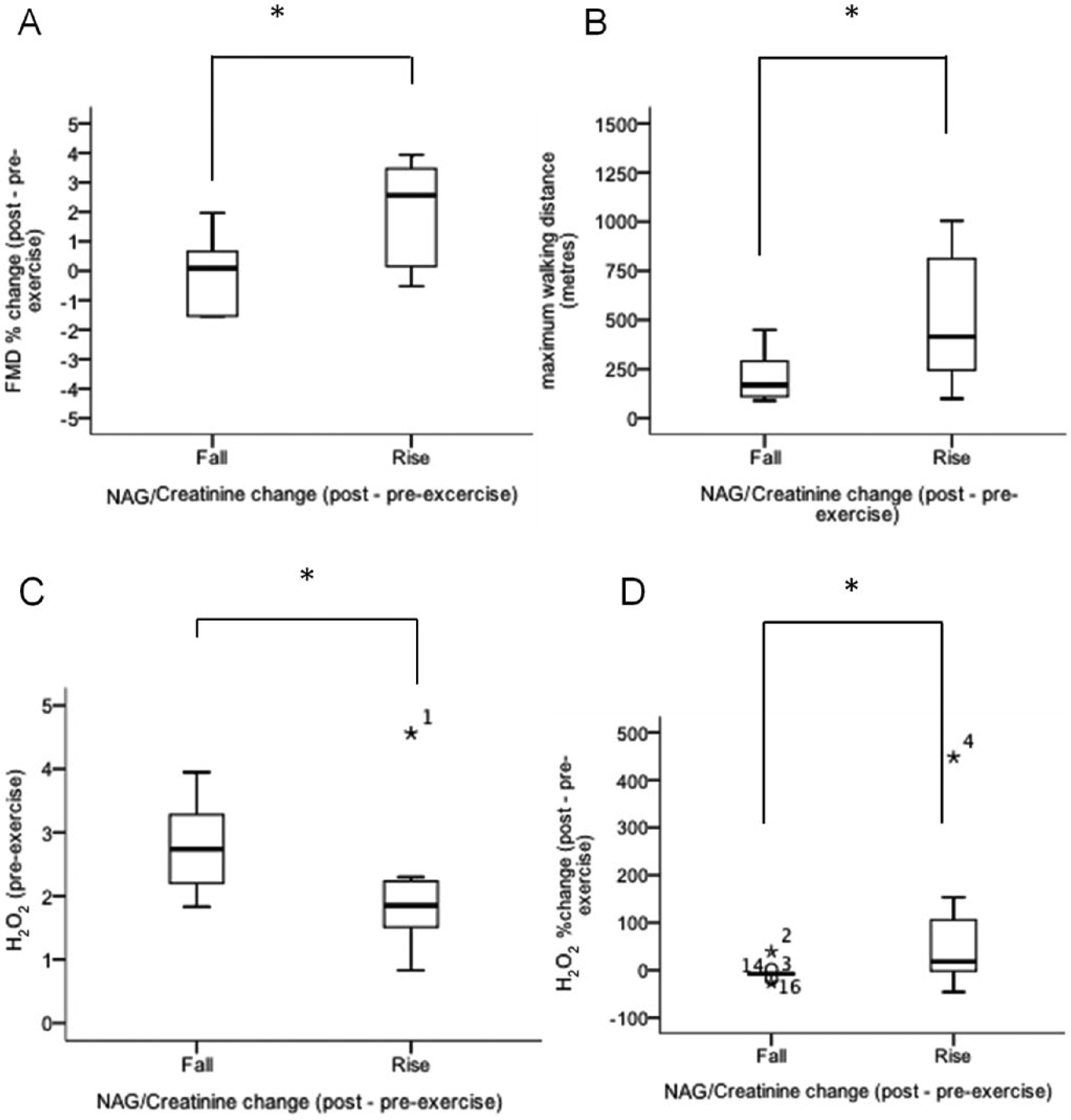
Box plots demonstrating: A) percentage change in endothelial function (FMD); B) walking distance (The scale has been adjusted to omit outliers, but all data have been used in the calculations); C) pre-exercise H2O2 mmol/L; D) percentage change in H2O2 – in patients experiencing a rise vs no rise in NAG/Creatinine post exercise; *, p<0.05).
Discussion
These findings support the hypothesis that there may be a phenotypically distinct subgroup of claudicants who suffer kidney injury on exercise. Here, the basal oxidative stress levels are lower than claudicants without such a pattern of acute kidney injury. Also, these claudicants have a longer walking distance and a higher post-exercise increase in oxidative stress and macro-vascular endothelial function.
Previous studies have reported that patients with peripheral vascular disease have an elevation in serum markers of oxidative stress, which can be improved with the administration of antioxidants 9 and a decrease in the activity of plasma glutathione peroxidase compared to the controls. 10 In a murine model, it has been shown that tissues with higher levels of catalase (lung and vena cava c.f. aorta and myocardium) and, hence, low levels of H2O2 had an attenuated up-regulation of endothelial nitric oxide synthase (eNOS) in response to exercise. The dissimilarities were abolished by the administration of a catalase inhibitor. 11 Furthermore, in another murine model, mice transfected with a gene to overexpress catalase in vascular tissue demonstrated no ability to up-regulate eNOS expression in response to exercise compared to wild type. 12 This study reports that a lower level of resting oxidative stress is associated with exercise-induced kidney injury as measured by a rise in the urinary NAG/Cr ratio, suggesting a potential protective function of basal oxidative stress.
Previously, reports suggest that resting brachial artery FMD in claudicants is lower than in controls (5.1% vs 11.7%) and maximal treadmill exercise causes a decrease in FMD in claudicants. 13 The brachial artery response to sublingual nitroglycerine was similar, indicating the effect was mediated by the endothelium rather than smooth muscle dysfunction. 14 Others have also reported a significant decrease in the percentage FMD of claudicants following maximal treadmill exercise (–1.5 ± 1; mean ± SD). 15 Tisi et al. have demonstrated an increase in the albumin/creatinine ratio following exercise in claudicants, but not controls following maximal exercise. 16 Additionally, a case control study reports that free radical scavenging capacity is lower in claudicants compared to controls. 10 However, endothelial dysfunction has been reported to exist in young hypertensive and non-hypertensive men, suggesting that there may be phenotypic variation in the population rather than dysfunction being simply a consequence of oxidative stress. 17 This study reports that both percentage change in oxidative stress and FMD post exercise are associated with an increased NAG/Cr ratio.
In a study comparing 20 patients with intermittent claudication stable for at least six months and 20 healthy controls, although claudicants had a higher level of plasma CRP and NAG/Cr ratio than controls, exercise did not significantly increase either parameter. 18 The seeming discrepancy in the findings may be a function of the potential ‘long-term survivor status’ of the claudicants recruited. Their chronic nature may represent an adaptation or a selection bias resulting from long-term survival.
A possible overarching mechanism arises where a low resting oxidative stress relates to an attenuated ability to respond to the increased oxidative burden associated with maximal exercise. This ability may normally be facilitated by NOS up-regulation. 12 An increasing production of reactive oxygen species leads to the oxidation of BH4 to BH3⋅ radicals.19,20 Low BH4 bioavailability uncouples eNOS, thereby, reducing eNOS function and augmenting eNOS superoxide production. 21 Others have reported that hydrogen peroxide increases the expression and activity of eNOS in endothelial cells and that increased eNOS activity is thought to be an acute cellular adaptation to an increase in oxidant stress. 22 This may also support the theory that ‘vulnerable’ claudicants fail to upregulate some anti-oxidant defense mechanism by lack of basal hydrogen peroxide release.
Although it is beyond the scope of this study to formally investigate, there is a similar prevalence of antiplatelet agent and statin usage in claudicants who suffered a NAG/Creatinine ratio rise compared to those without a rise. It has been shown that, in a rat model, statin administration reduced the degree of renal ischaemia reperfusion injury following renal artery clipping. 23 However, it has been demonstrated that the administration of either lipo- or hydrophilic statins does not modulate the effect of ischaemia reperfusion injury on brachial artery FMD in healthy volunteers. 24 Of additional note, a reduction in infarct size may well be associated with short-term use and these protective effects may be lost in chronic use. 25
According to Suvorava and Kojda, repeated short-terms bouts of oxidative stress may cause the up-regulation of anti-oxidant protein expression in the vascular wall, eventually increasing its antioxidant capacity. 26 A case control study compared pro-inflammatory cytokine levels in patients with moderate and severe intermittent claudication to healthy controls before and after exercise. This study demonstrated a rise in cytokine levels post exercise in all groups; most in the severe group and some in the moderate group exhibited a continued rise in cytokine levels in the resting period. 27 This finding may support the notion that certain individuals may not be able to cope with increased oxidative stress and these people may be prone to worsening of atherosclerotic lesions. The previous dogma of treating claudication in five words “stop smoking and keep walking” 28 may not be the best management for all claudicants. Although caution should be taken in drawing firm conclusions from the data presented in this small pilot study, further work may be warranted to provide security to these findings and elucidate the existence of a ‘vulnerable’ cohort of claudicants.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.