
Abstract
Background:
We aimed to characterize the coagulation disturbances which may increase the risk of bleeding, thrombosis or death shortly after implantation of an extracorporeal membrane oxygenation (ECMO) or ventricular assist (VAD) device.
Methods:
Antithrombotic treatment was started in 23 VAD and 24 ECMO patients according to the hospital protocol. Additionally, conventional laboratory testing, rotational thromboelastometry (ROTEM®) and platelet function analysis (Multiplate®) were performed at predetermined intervals.
Results:
Four out of twenty-four (16.7%) of ECMO patients and 6/23 (26.1%) of VAD patients had severe bleeding after the procedure. When all the patients were analyzed together, low maximum clot firmness (MCF) in ExTEM and FibTEM analyses was associated with severe bleeding (p<0.05) and low MCF in FibTEM with 30-day mortality. Low platelet count and hematocrit levels were also associated with severe bleeding. When VAD and ECMO patients were separated into different groups, the association between ROTEM® parameters, bleeding and survival was found only in limited time points.
Four patients with VAD had cerebral ischemia indicative of thromboembolism. However, this had no significant correlation with ROTEM® or Multiplate® parameters.
Conclusion:
Hypocoagulation shown by ROTEM® was associated with bleeding complications in patients with mechanical circulatory support. In contrast, hypercoagulation did not correlate with clinical thrombosis.
Introduction
The use of extracorporeal circulatory assist devices requires effective anticoagulation due to proinflammatory and prothrombotic responses caused by blood interacting with the non-endothelial surfaces of the circuit. 1 In ECMO, additionally, the membranes of an oxygenator provide an increased non-biocompatable surface area. Therefore, anticoagulation is needed to prevent thrombosis of the cannulae, oxygenator and circuit tubing, 2 i.e. to prevent life-threatening thrombosis while excessively bleeding should be avoided. 1 On the other hand, effective anticoagulation is associated with an increased bleeding tendency.
Anticoagulation treatment is challenging as there are often underlying coagulation disorders of various reasons in these critically ill patients. Anticoagulation usually gets more and more challenging with the duration of extracorporeal circulation 3 and unidentified minor clots can cause a variety of thromboembolic events, even in patients considered adequately anticoagulated.4,5
The earliest and still the predominant test to monitor heparin anticoagulation for extracorporeal circulation devices is the activated clotting time (ACT) which measures the integrity of the intrinsic and common coagulation pathways.6–8 However, the ACT’s ability to provide adequate anticoagulation is limited because the accuracy of the test is influenced by multiple variabilities, such as coagulopathy, oral anticoagulants, hypofibrinogenemia, thrombocytopenia, platelet dysfunction or inhibition, antithrombin III (ATIII) level, hypothermia, patient age and hemodilution. 9 Also, numerous technical factors, e.g. sample size or temperature can affect the test results. 8
The activated partial thromboplastin time (aPTT) is universally recognized as a standard monitor for heparin therapy, except when high heparin dosing is required, as in cardiopulmonary bypass. However, the aPTT has also several limitations. For example, it recognizes neither fibrinolysis nor disturbance of clot formation. Due to these limitations, using ROTEM® during evaluation of coagulation status could give additional information to the use of ACT and aPTT alone.
Various easily and quickly obtainable point-of-care (POC) coagulation monitoring tests are applicable in monitoring anticoagulation during mechanical circulatory support. Whole blood viscoelastic tests, such as rotational thromboelastometry or thromboelastography, describe the entire whole blood coagulation process, including clot initiation, formation and stabilization, as well as fibrinolysis. The addition of platelet function analyses to the monitoring palette provides information about platelet function.
The objective of the current study was to characterize coagulation disturbances in combination with bleeding or thromboembolic complications using POC methods in addition to conventional laboratory hemostatic testing.
Methods
After approval of the Ethics Committee for Surgery in Helsinki University Hospital (372/E6/07), we prospectively studied consecutive patients requiring an extracorporeal circulation assist device between March 2008 and June 2012 at the Department of Cardiac Surgery in Helsinki University Hospital, Helsinki, Finland.
The indications for mechanical circulatory support were cardiac failure or severe respiratory failure (Table 1). The types of devices were ECMO (Bioconsole 560®, Medtronic, Minneapolis, Minnesota USA or Rotaflow®, MAQUET Holding B.V. & Co., Rastatt, Germany) or VAD (Berlin Heart Excor®, Berlin Heart GmbH, Berlin, Germany). The use of mechanical circulatory support was started after the decision of the multidisciplinary team of cardiologists, cardiac surgeons and anesthesiologists. Some of ECMOs were cannulated percutaneously (48% (n=11) in the ECMO group), other devices surgically centrally (22% (n=5) in the ECMO group). The cannulation procedures were performed either electively or urgently, as required. Patients were connected to ECMO by cannulas sized: v. femoralis 21-27 Fr, a. femoralis 15-21 Fr or, when centrally cannulated, aorta 20-22 Fr and vena cava 28-34 Fr. In veno-venous ECMO, Avalon® cannulas 27-31 Fr in size were used. Flow ranges in veno-arterial ECMO were 2.0-2.4 l/min/m2 and in veno-venous ECMO 1.5-2.0 l/min/m2. The duration of ECMO treatment ranged from 3 – 30 days.
Background information of the patient population.
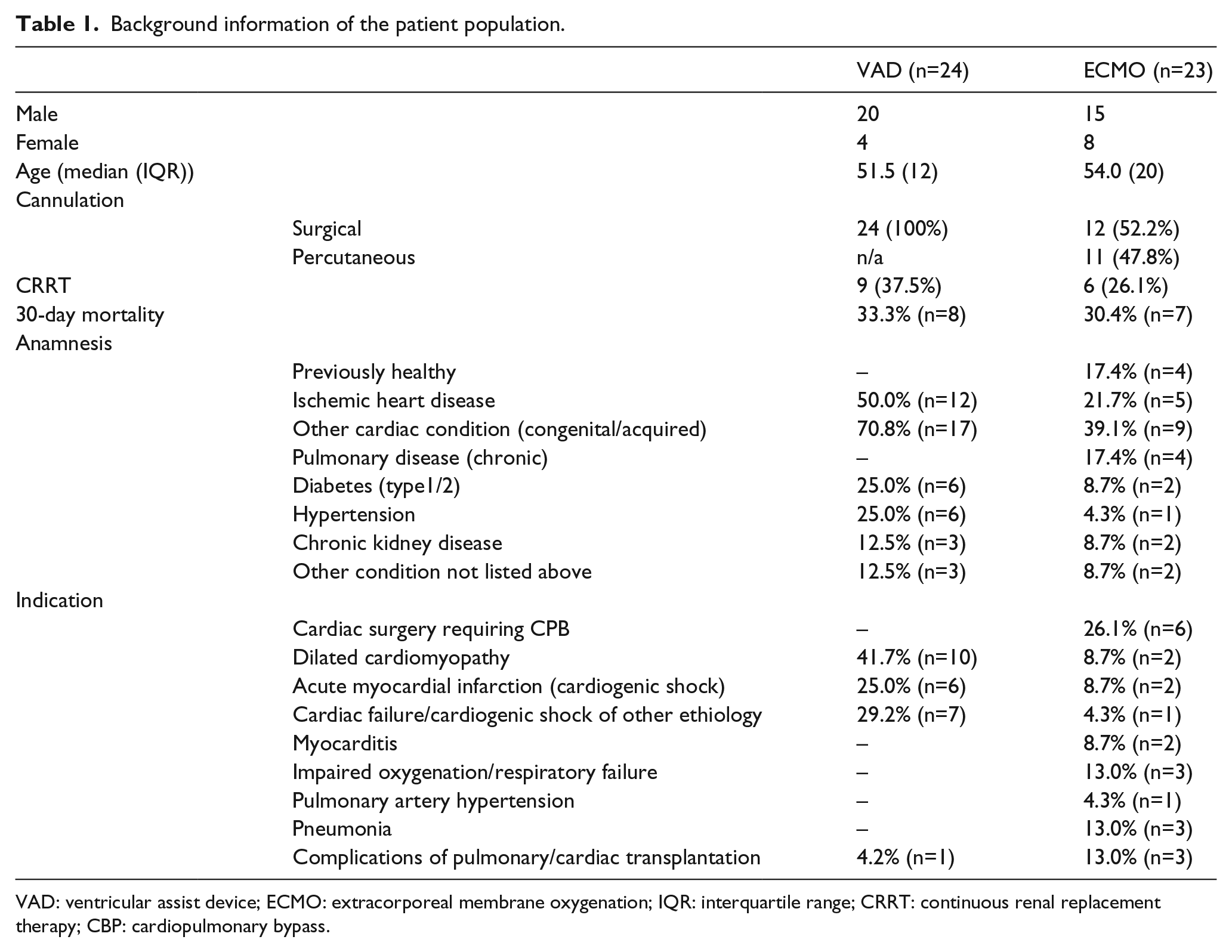
VAD: ventricular assist device; ECMO: extracorporeal membrane oxygenation; IQR: interquartile range; CRRT: continuous renal replacement therapy; CBP: cardiopulmonary bypass.
The patient’s neurological status was assessed clinically and with computed tomography scan, if necessary, during the 30-day follow-up period at the daily sedation breaks. Sedation breaks were not executed if the patient had an open sternotomy wound or central cannulation. Severe bleeding was defined as two or more liters during the 24 hours following surgery or the patient receiving more than five units of packed red blood cells (RBC) in 24 hours. 10 A thrombotic complication was defined as a venous or arterial thromboembolism leading to neurological complication or pulmonary embolism. Mortality was assessed at 30 days after the start of mechanical circulatory support.
Anticoagulation protocol
Anticoagulation was started within 24-36 hours after the initiation of extracorporeal circulatory support. If implantation/cannulation of the device was done surgically, anticoagulation was not started until postoperative bleeding had ceased. Unfractioned heparin was used as anticoagulant. Heparin was diluted in normal saline, with an heparin concentration of 100 U/mL, and administered as a continuous infusion without loading bolus, starting with 200-300 U/h. ACT and aPTT were measured before the start of the anticoagulation regimen and were then performed every 4 hours (ACT) or 6 hours (aPTT). The activity of AT III was measured daily. The heparin infusion rate was increased slowly to achieve and maintain both ACT and aPTT at the target levels. Hemoglobin (Hb) concentration was kept above 9.0-10.0 g/dL and the platelet count (PLC) above 50 x109/L or, with evidence or suspicion of bleeding, above 100 x109/L. The targets of ACT and aPTT were set according to hospital practices: if the PLC was under 100 x109/L, the target of the ACT was set to 160 – 180 sec and the aPTT to 50 – 60 sec. If the PLC was over 100 x109/L, the targets were 180 – 200 sec and 60 – 70 sec, respectively. The target AT III activity was over 50%. Pooled human plasma (Octaplas®, Octapharma AB, Stockholm, Sweden) or AT III concentrate (Atenativ®, Octapharma AB) was administered if the AT III activity decreased under 50%.
The study period was seven days after the start of the mechanical circulatory support. Blood product transfusions, urine output, postoperative bleeding and net fluid balance were registered daily with PI Client Information System (Caresuite 8.2, PICIS Inc., San Fransisco, CA, USA). Laboratory tests, including Hb (g/dL), hematocrit (Hct, %), PLC, (x 10 9/L), C-reactive protein (CRP), prothrombin time value (TT, %), international normalized ratio (INR), lactate concentration, AT III (%), anti-FXa (U/mL) and ROTEM® (ROTEM®, TEM International, Munich, Germany) (ExTEM [tissue factor activator to assess the external coagulation pathway] + FibTEM [ExTEM based assay for fibrinogen part of coagulation, platelet activity blocked with cytochalasin D] activators) were performed preoperatively (within 24 hours before device installation) and daily for seven days postoperatively. Platelet function analysis with a Multiplate®device (Multiplate®, Dynabyte Medical, Munich, Germany) using TRAPtest (Thrombin Receptor Activating Peptide-6), ADPtest (Adenosine Diphosphate) and ASPItest (to assess Aspirin®, Acetylsalicylic acid effect) activators was performed preoperatively and on postoperative days (POD) 1, 3, 5 and 7.
Statistics
The differences were analyzed with the non-parametric repeated measures analysis of variance (Kruskal-Wallis test). Correlations were tested with the Spearman test. The Mann-Whitney U-test was used for paired comparisons. Since the data were mostly not normally distributed (Kolmogorov-Smirnov test), the results are shown as medians (Interquartile range, IQR). A p-value <0.05 was considered to be statistically significant.
Results
Forty-seven patients were enrolled in this study. Overall, forty-five patients (23 treated with ECMO, 24 with VAD; of which 16 LVAD and 8 BiVAD) were analyzed. Two patients were first treated (2 and 7 days respectively) with veno-arterial ECMO before a VAD was implanted. The total duration of treatment for each patient in the VAD group was more than 7 days; in the ECMO group 14 patients were treated for more than 7 days, 1 for 6 days, 4 for 5 days, 3 for 4 days and 1 for 3 days. The median age was 54.0 (IQR 20) in the ECMO group and 51.5 (IQR 12.2) in the VAD group. Descriptive statistics of all patients are presented in Table 1.
Indications for extracorporeal circulatory support were acute cardiac failure (n=42) or respiratory failure (n=5). One patient had ECMO installed after drowning. Five ECMOs were veno-venous and eighteen veno-arterial. The results of the conventional coagulation tests and CRP during the study period are shown in Table 2.
Median conventional laboratory test values during the study period.
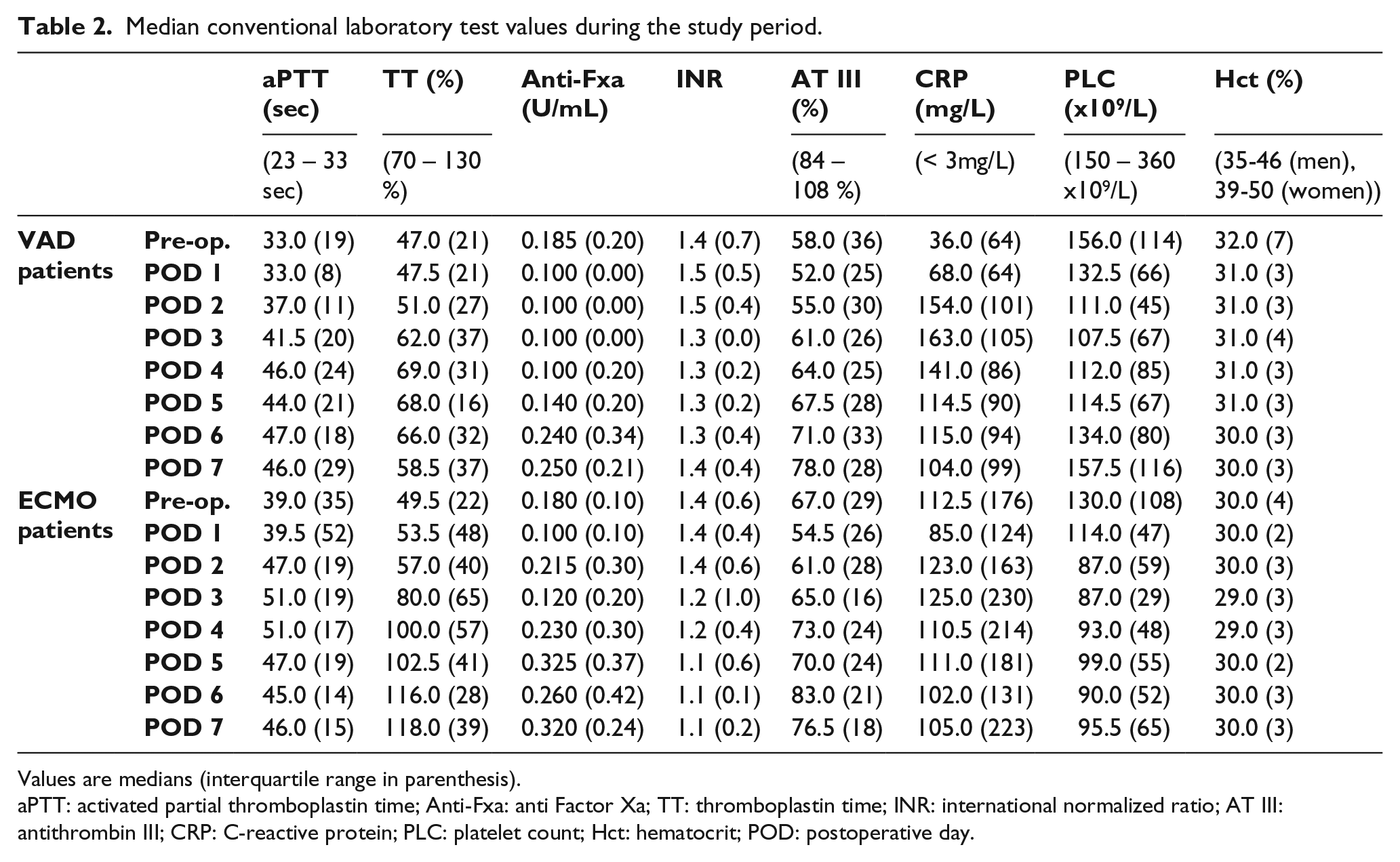
Values are medians (interquartile range in parenthesis).
aPTT: activated partial thromboplastin time; Anti-Fxa: anti Factor Xa; TT: thromboplastin time; INR: international normalized ratio; AT III: antithrombin III; CRP: C-reactive protein; PLC: platelet count; Hct: hematocrit; POD: postoperative day.
Twelve patients, four in the VAD group (16.7%) and six in the ECMO group (26.1%), had severe bleeding postoperatively, either from cannulae insertion sites or from postoperative chest tube drains. When all the patients were analyzed together, the median ExTEM MCF (63.0 mm (IQR 8 mm) vs. 52.0 mm (IQR 27 mm), p=0.032) and FibTEM MCF (26.0 mm (IQR 17 mm) vs. 11.0 mm (IQR 14 mm), p=0.011) were preoperatively significantly higher in patients without severe postoperative bleeding than in those patients with severe bleeding. ExTEM MCF on POD 1 (51.5 mm (IQR 9 mm) vs. 61.0 mm (9 mm), p=0.018) and on PODs 6 (53.0 mm (IQR 9 mm) vs. 64.5 mm (12 mm), p=0.011) and 7 (57.5 mm (IQR 11 mm) vs. 67 mm (11 mm), p=0.011) were significantly lower in the patients with severe postoperative bleeding than in those without bleeding. On the other hand, FibTEM MCF showed significant difference only on POD 1 (9.5 mm (IQR 9 mm) vs. 19.0 mm (13 mm), p=0.024).
FibTEM MCF on POD 6 was significantly higher in recovered patients than in non-survivals (25.0 mm (IQR 15 mm) vs. 19 mm (7 mm), p=0.024) (Figure 1). This was also seen in VAD patients (p=0.016) when analyzed separately, but not in ECMO patients. ExTEM MCF had a tendency to differ between survivals and non-survivals: in the survival group, it did not change during the observation time and stayed on the preoperative level, p>0.05. In the non-survivals, ExTEM MCF had a trend of decreasing compared to recovered patients, although the finding was not statistically significant (Figure 2). The platelet count was significantly lower in patients with severe postoperative bleeding. This was displayed preoperatively (119 x 109/L (IQR 105 x 109/L) vs. 153 x 109/L (111 x 109/L), p=0.024) and on PODs 5 (61 x 109/L (48 x 10 9/L) vs. 110.5 x 109/L (61 x 109/L), p=0.012), 6 (78 x 109/L (59 x 109/L) vs. 132 x 109/L (86 x 109/L), p=0.009) and 7 (95.5 x 109/L (62 x 109/L) vs. 146 x 109/L (102 x 109/L), p=0.017). The hematocrit was significantly lower on PODs 5 and 6 in patients with severe bleeding. Neither the thromboplastin time nor the aPTT were associated with bleeding in this patient population.
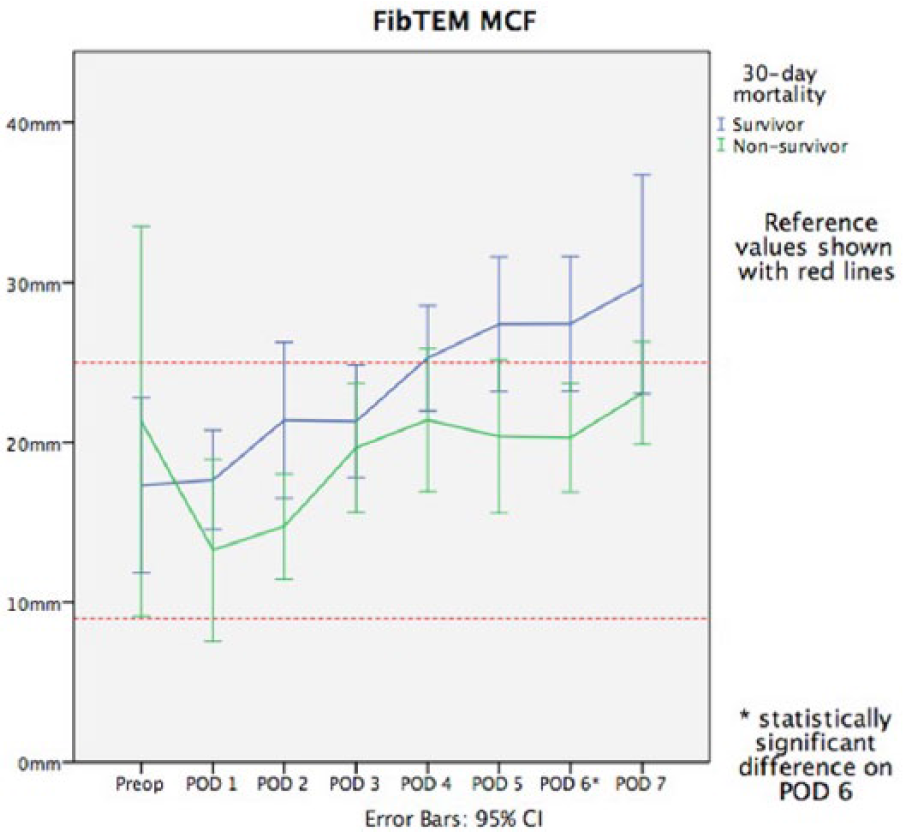
Median maximum clot firmness in FibTEM.
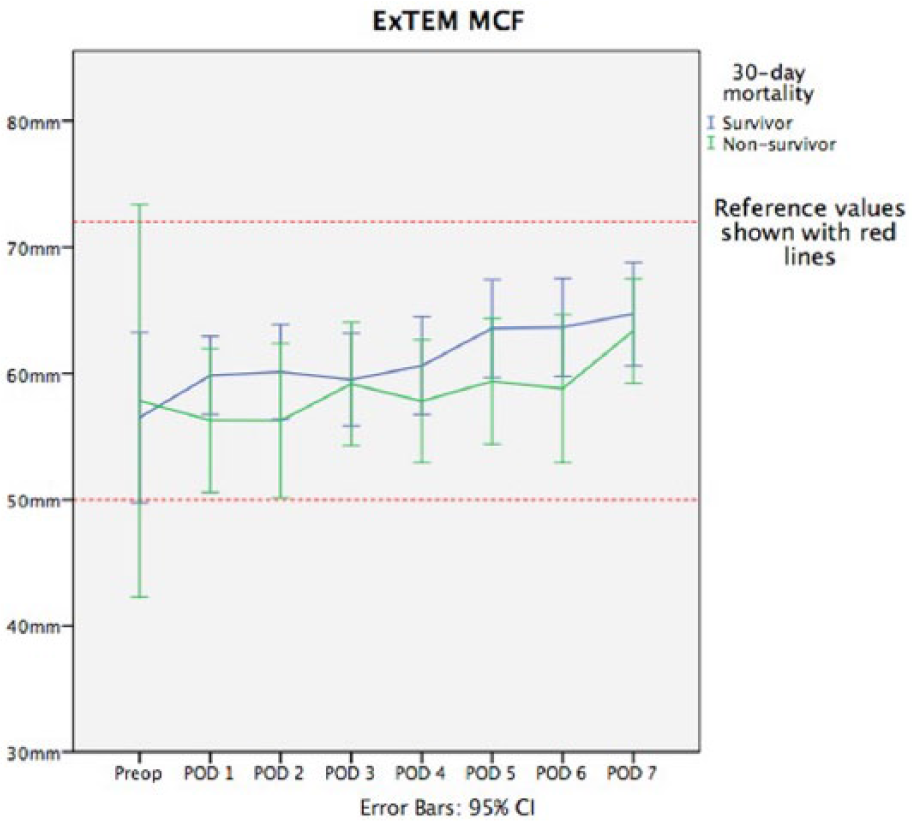
Median maximum clot firmness in ExTEM.
Analysis of separated groups
In the VAD group, there were no significant findings in ExTEM MCF and FibTEM MCF preoperatively in patients with bleeding or thrombotic complications. On POD 6, both ExTEM and FibTEM MCF were significantly lower in patients with bleeding complications (p=0.043 and p=0.014, respectively) (Table 3). FibTEM MCF on POD 6 was significantly higher in recovered patients (26 mm vs. 20 mm, p=0.016). In the ECMO group, there were no thrombotic complications. In the ECMO patients, ExTEM MCF was significantly lower on POD 1 (p=0.045) and FibTEM MCF was already preoperatively significantly lower (p=0.019) in patients with bleeding complications (Table 3). There was no correlation between survival and ExTEM or FibTEM MCF in either of the study groups when analyzed separately. The median ExTEM and FibTEM MCF values in both groups are presented in Table 4. The platelet counts on POD 5 (86.5 x 109/L (37 x 109/L) vs. 121 x 109/L (63 x 109/L), p=0.020) and 6 (88.5 x 109/L (53 x 109/L) vs. 149.5 x 109/L (66 x 109/L), p=0.044) were significantly lower in VAD patients with severe bleeding. The PLC was also significantly lower in ECMO patients with severe bleeding on PODs 5 (51 x 109/L (50 x 109/L) vs. 100 x 109/L (30 x 109/L), p=0.041) and 6 (54 x 109/L (74 x 109/L) vs. 107 x 109/L (50 x 109/L), p=0.037). The aPTT on POD 3 was significantly lower in patients with bleeding (40 sec vs. 41.5 sec, p=0.012).
Median ExTEM and FibTEM MCF in VAD and ECMO groups. Patients with bleeding complications are shown separately.
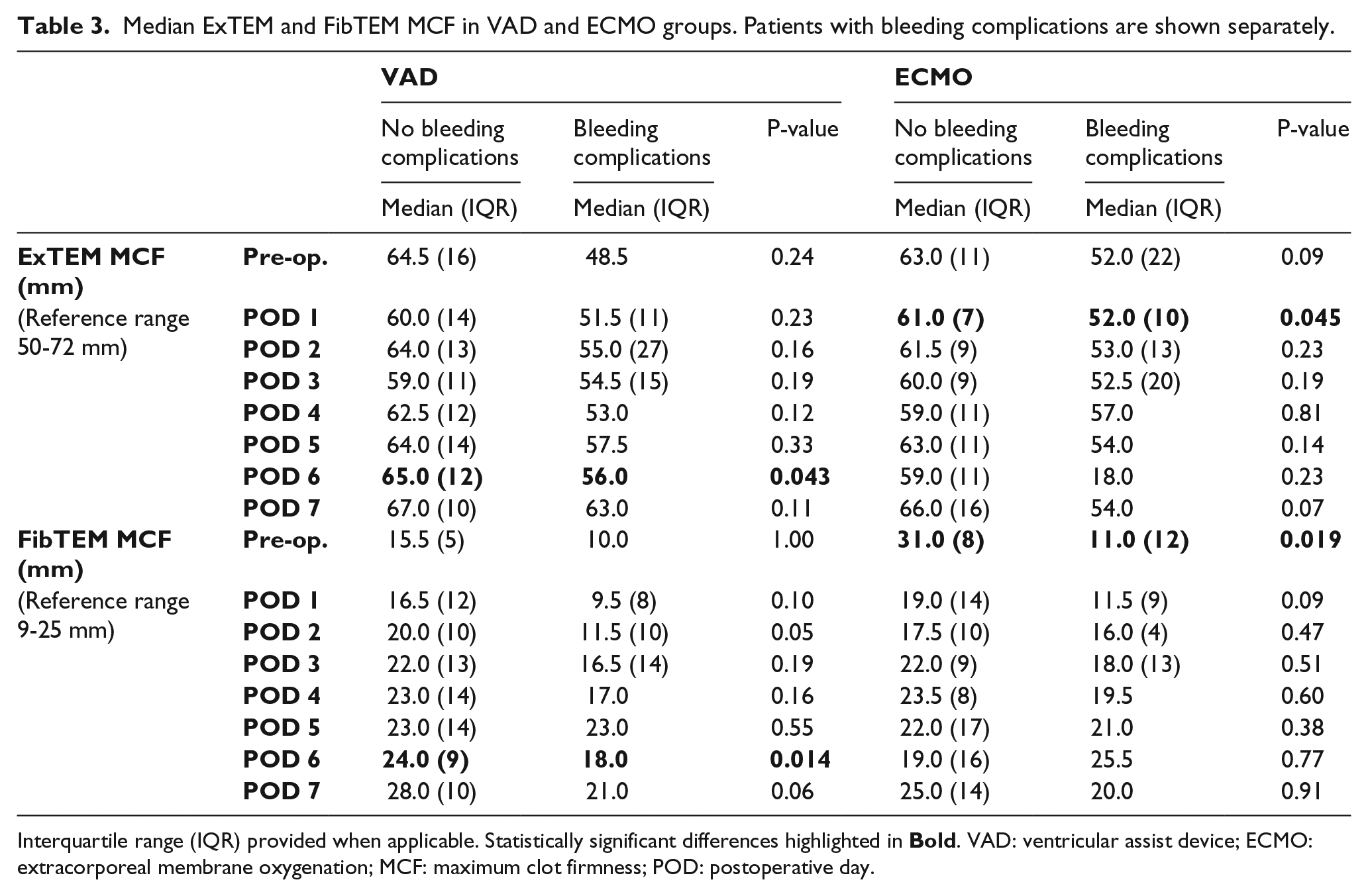
Interquartile range (IQR) provided when applicable. Statistically significant differences highlighted in
Median ExTEM and FibTEM in VAD and ECMO groups.
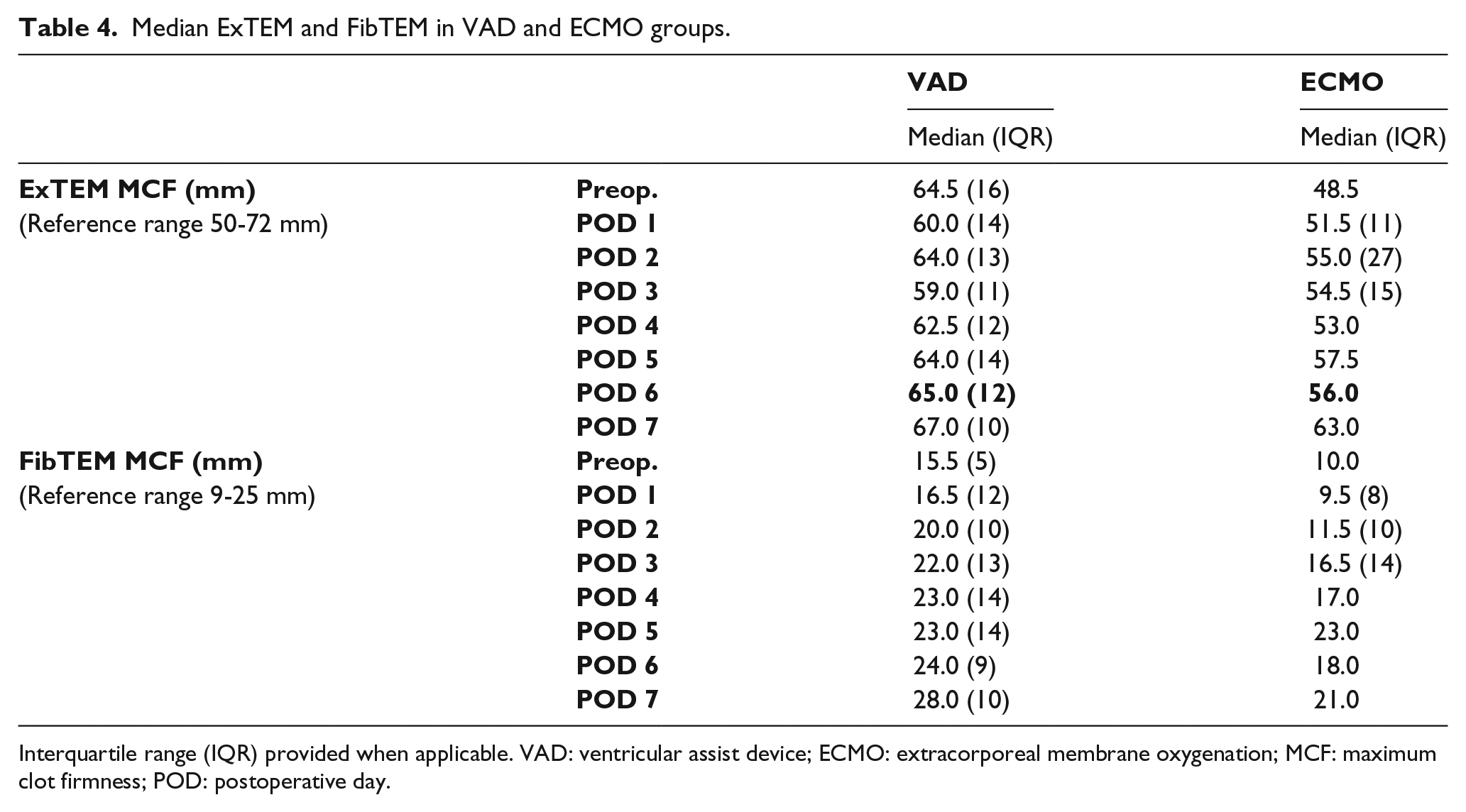
Interquartile range (IQR) provided when applicable. VAD: ventricular assist device; ECMO: extracorporeal membrane oxygenation; MCF: maximum clot firmness; POD: postoperative day.
Multiplate® analyses did not show any significant correlation with bleeding, thrombosis or survival in either group. Values are presented in Table 5. Fluid balance did not show any significant correlation with ROTEM® parameters.
Median Multiplate® values in VAD and ECMO groups.
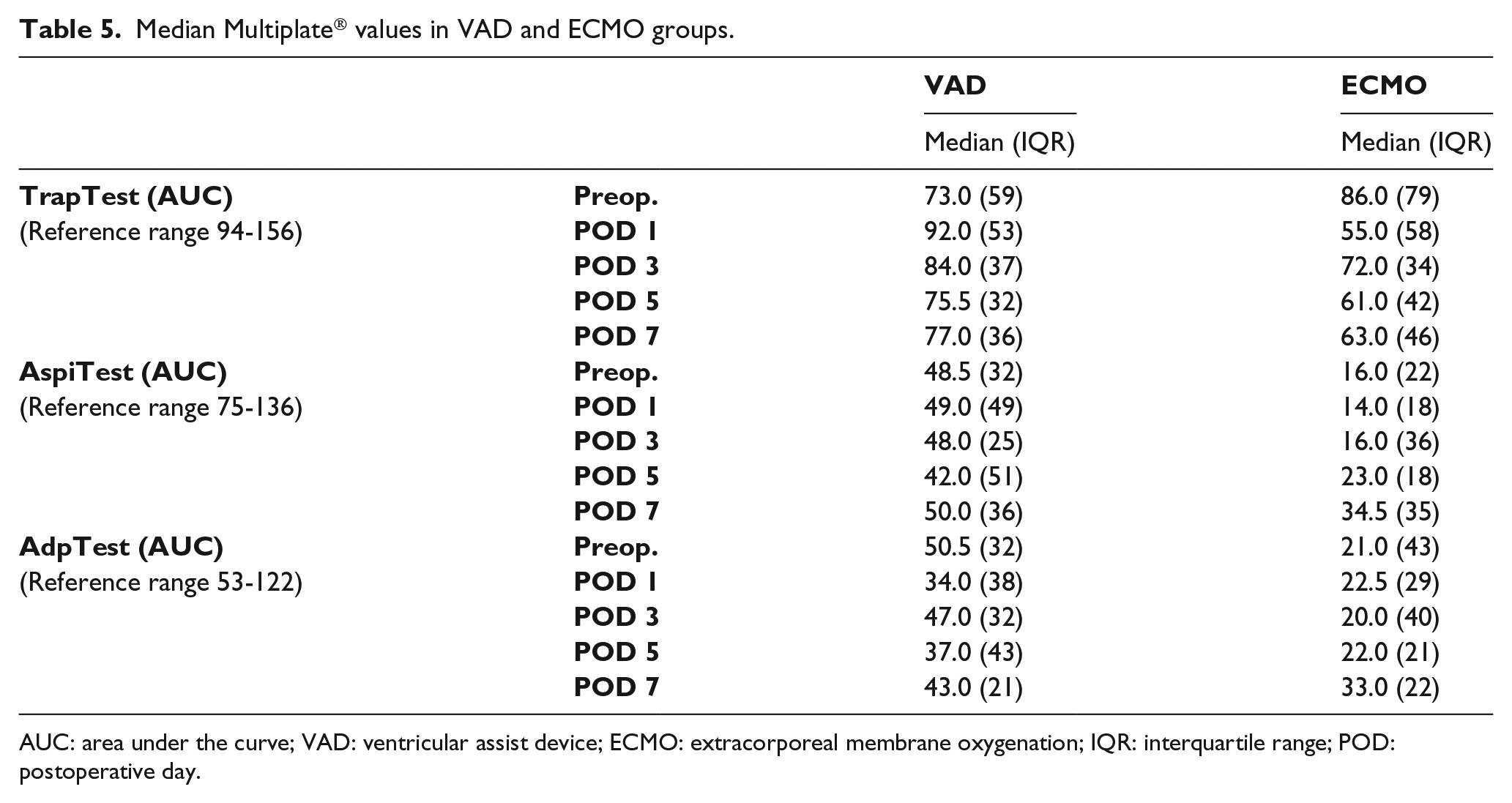
AUC: area under the curve; VAD: ventricular assist device; ECMO: extracorporeal membrane oxygenation; IQR: interquartile range; POD: postoperative day.
The mortality rate at 30 days was 30.4% in the ECMO group and 37.5% in the VAD group. In both groups, slightly more negative fluid balance was associated with better survival, but this finding was not statistically significant except in the ECMO group on POD 3 (-583 ml (IQR 1073 ml) vs. +630 ml (IQR 1161 ml), p=0.033). Median net fluid balance in survivors and non-survivors is presented in Figures 3 and 4. Six patients (26.1%) in the ECMO group and nine patients (37.5%) in the VAD group needed continuous renal replacement therapy during the study period. Additionally, decreased amount of platelets on POD 4 and 5 in the VAD group correlated positively with mortality.
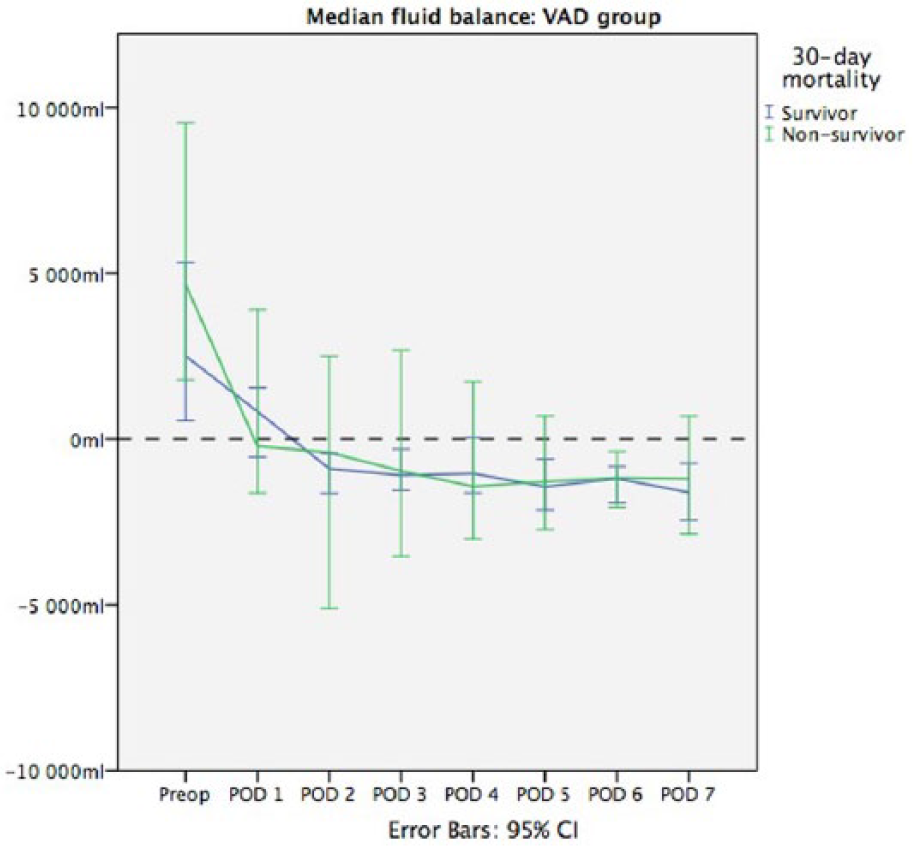
Median fluid balance in the VAD group.
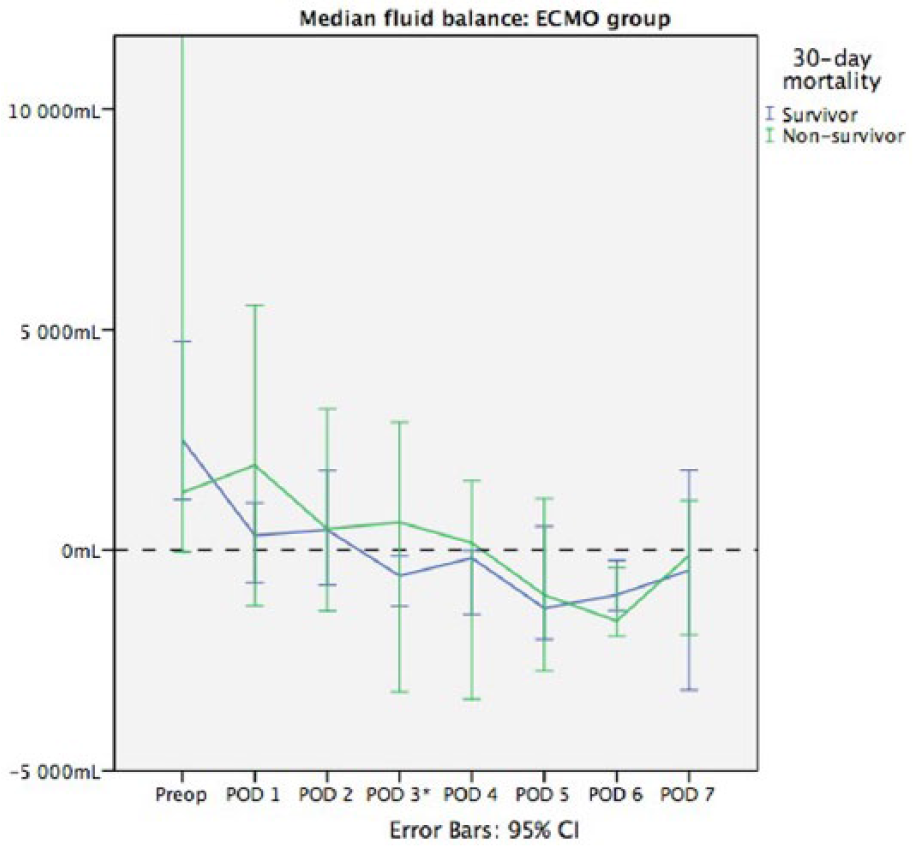
Median fluid balance in the ECMO group. ECMO: extracorporeal membrane oxygenator; CI: confidence interval; POD: postoperative day. * statistically significant (p=0.033).
Four patients with VAD (16.7%) and no patients with ECMO had neurological complications (for this study, defined as intracranial hemorrhage or ischemia). Two of them had a transient ischemic attack and two had a stroke. Both patients with a stroke died. There was no significant correlation between ROTEM® or Multiplate® parameters and neurological complications.
Discussion
In this study, we showed that low ExTEM and FibTEM maximum clot firmness in ROTEM® analysis was associated with a bleeding tendency in patients treated with extracorporeal circulatory support. Bleeding complications are often encountered during extracorporeal circulation and they are a major cause of morbidity and mortality. Surgical site bleeding is reported in 6-32% of cases 11 and intracranial hemorrhage, the most devastating and potentially life-threatening complication, occurs in up to 3-19% of patients.12,13 In our study group, severe bleeding was observed in 21% of the patients, but none died from this complication. There were no intracranial bleeding complications; central nervous system complications were limited to ischemic events.
In conventional laboratory tests, such as ACT and aPTT, we saw, preoperatively, signs of underlying clotting disorders. This relates mostly to the severe and chronic illness from which the patients are suffering, as well as previous surgery with blood and coagulation factor loss and transfusions. Liver congestion due to heart failure often leads to the underproduction of coagulation factors and chronic illness, itself, together with repeated laboratory testing can drive the patients to anemia. Also, in the postoperative state, there is usually some hypocoagulation present due to the acute consumption of coagulation factors caused by the surgery. Extracorporeal circulation associates strongly with acquired coagulation deficiencies, such as factor XIII deficiency, von Willebrand syndrome and thrombocytopenia, as early as during the first week of treatment. 14 The low platelet count predictably was associated with bleeding complications. The crucial role of platelets for postoperative bleeding, especially after cardiac surgery, has been demonstrated previously.15,16 In this study, we were unable to show any significant association between Multiplate® parameters and outcome results. This most probably has to do with the relatively small number of patients, as platelet function analysis has previously been shown to correlate with bleeding tendency in cardiac surgery. 17
MCF in ExTEM and FibTEM was associated with 30-day survival in ECMO and VAD patients. This was seen very early in the 7-day study period. In survivors, MCF in ExTEM remained almost unchanged while MCF in FibTEM was significantly higher in the last days of the study period. As many extracorporeal life support patients die from multi-organ failure, the problems with coagulation factor production, possibly associated with decreased liver function, can be seen in viscoelastic blood analysis in the early phase, although, when the VAD and ECMO groups were analyzed separately, the statistical significance of this finding diminished. This has to do with the fact that the number of patients in this study was limited and not enough to demonstrate statistical difference. Thirty-day mortality in our study groups (30% in the ECMO group and 38% in the VAD group) was relatively low compared to previous studies, indicating in-hospital mortality rates between 24-90%. 18 As recognized in numerous previous studies,19–21 negative fluid balance correlated with better survival; in our study, we could demonstrate only a tendency for this. About 30% of all our patients needed renal replacement therapy during extracorporeal life support, which is less than in previous reports. 22 Despite extracorporeal ultrafiltration, some patients were still unable to maintain negative fluid balance, leading to complications and even death. The dilution of coagulation factors in patients with a positive fluid balance could expose patients to bleeding. Non-survivors also seem to be unable to recover from thrombocytopenia caused by bone marrow suppression and by the use of extracorporeal circulation. 23
Generally speaking, ROTEM® analyses could have an effect on guiding the treatment choices in these patients, e.g. when choosing transfusions of blood products versus coagulation factor concentrates. The reduction of blood product use in VAD patients when using POC hemostasis monitoring was shown in a retrospective analysis by Sun et al. 24 In our institution, this method is still not fully established, but has proven to be an effective additional tool, especially in complex major surgery. Getting the blood analysis results promptly and bedside is a present-day method of testing coagulation in both the intensive care unit and the operating room. Whole blood viscoelastic tests also reflect the coagulation status in a way that no conventional laboratory test is able to do; it shows clot propagation, formation, and stabilization dynamically; additionally, it demonstrates the presence of fibrinolysis better than any laboratory analysis, e.g. fibrinogen d-dimer is always elevated in this patient group as an acute phase protein. Previous studies showed that whole blood analysis provides more accurate information of the coagulation process in vivo.25,26
There are several limitations in our study. First, the patient number is limited due to scarcity of critically ill patients requiring extracorporeal circulatory support. Analyzing VAD and ECMO patients together has its limitations due to some crucial differences between the systems but, in our opinion, is, in part, justified based on numerous similarities of the two systems: the patients’ blood moves continuously through tubes with non-biocompatible surfaces. Secondly, there are numerous confounding factors that have to be considered when generalizing the results: surgical bleeding versus bleeding caused by deficiency in coagulation factors cannot be compared, especially when considering thromboelastometry.
Whether the additional information provided by these POC tests could actually assist with the decision-making in anticoagulation and transfusion therapy in ECMO and VAD patients has to be studied in a randomized, prospective arrangement.
Footnotes
Acknowledgements
The authors are grateful to Anna-Maria Koivusalo, M.D., Ph.D., (Division of Intensive Care Medicine, Department of Anaesthesiology, Intensive Care and Pain Medicine, University of Helsinki, Helsinki University Hospital) and laboratory technician Mailis Himberg (HUSLAB, Helsinki University Hospital) for technical support.
Declaration of Conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Schramko has received congress-related travel reimbursement from TEM International GmBH.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partially funded by a Government Grant for Healthcare Research in Finland.