
Abstract
Blood transfusions could have serious consequences for patients. A reduction in the transfusion rate could be accomplished by an optimized blood management. Clear guidelines and awareness among all employees at a single institution have resulted in a reduction in transfusion rates in recent years. Identification of the group of patients who still received a blood transfusion in recent years could result in a further reduction. This study enrolled 4022 patients undergoing cardiothoracic surgery between 2008 and 2013. Patients were divided into three groups: “no blood transfusion”, “transfusion of packed red cells only” and “any other combinations of blood transfusion”. In total, 16 variables were tested for their association with the administration of homologous blood. The variables associated with blood transfusion were included in a stepwise multinomial logistic regression analysis to find the variables with the strongest association.
For the transfusion of packed red cells only and any other combinations of blood transfusion, the following predictors are found: gender, age, weight, type of surgery, reoperation, unstable angina pectoris, endocarditis, recent myocardial infarction, preoperative creatinine level, preoperative hemoglobin level and preoperative platelet count. The best predictor for the transfusion of packed red cells is preoperative hemoglobin level (4.1 to 7.8 mmol/l). For other blood products, the strongest association was found with type of surgery (aortic surgery, ventricular septal rupture and intracardiac tumour).
Keywords
Introduction
There is a strong linkage between cardiothoracic surgery and blood transfusions. Historically, 10-15% of all blood transfusions are used in cardiothoracic surgery.1–5 The main reasons are patient characteristics, hemodilution and blood loss during the procedures. Awareness of the risks and costs of blood transfusions has brought a significant reduction in the past.5,6
During cardiothoracic surgery, there is always a certain amount of hemodilution and blood loss, frequently leading to a blood transfusion. Blood transfusions are associated with serious consequences for the patient, like infections or immunological reactions. The consequences, like transfusion-related acute lung injury (TRALI), can be so dramatic that a blood transfusion does not outweigh the benefits. Therefore, the risks need to be reduced by keeping the number of blood transfusions as low as possible.5–10
Since the start of the Heart Centre at the Medical Centre Leeuwarden (MCL) in 2004, the data of all blood transfusions (except Haemocomplettan® P since 2008) have been registered (Figure 1). Clear guidelines and awareness among all employees of the Heart Centre resulted in a reduction in the transfusion rate in recent years. Awareness was created by sending transfusion rates to all participants every three months. Identification of the group of patients who still received a blood transfusion in recent years could result in a further reduction.
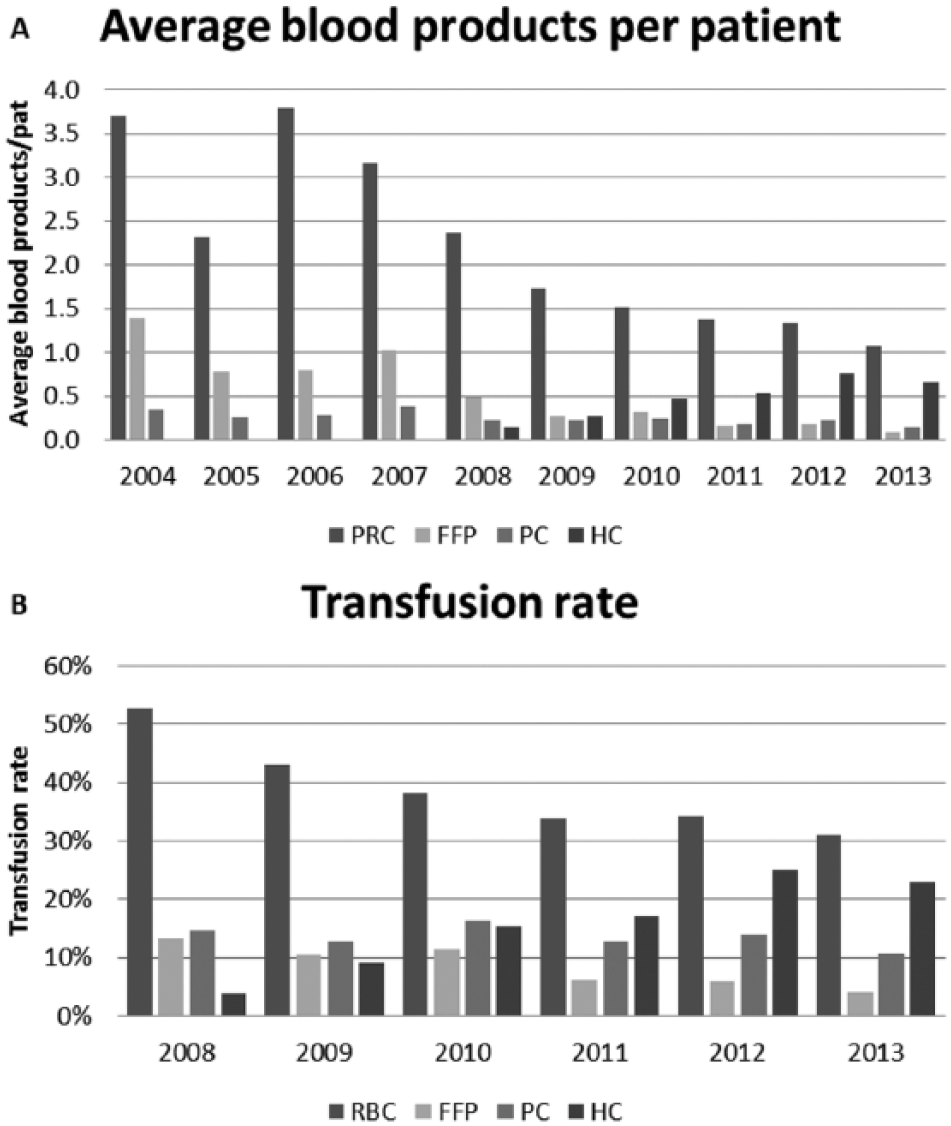
Average number of transfused blood products per patient (A) and transfusion rate (B). PRC: packed red cells; FFP: fresh frozen plasma; PC: platelet concentrate; HC: Haemocomplettan® P (since 2008).
Material and methods
Patients
In this study, a total of 4022 patients were included. These patients underwent cardiothoracic surgery between 2008 and 2013. Three hundred and ninety patients with off-pump coronary artery bypass grafting (OPCAB) procedures were included in this study as coronary artery bypass graft (CABG). Patients who underwent transcatheter aortic valve implantation (TAVI) or a Mitra-clip procedure were excluded because these were performed in the Cath Lab.
The following preoperative data were collected: gender, age (years) height (cm) weight (kg), body mass index (kg/m2), body surface area (m2), diabetes mellitus (type I or II), unstable angina pectoris (condition: continuous intravenous administration of nitroglycerine), endocarditis, recent myocardial infarction (within 3 months), ejection fraction (%), preoperative creatinine level (mg/dl), preoperative hemoglobin level (mmol/l), preoperative platelet count (cells x 109/litre), type of surgery (isolated CABG, isolated valve surgery, combined CABG + valve surgery; other (aortic surgery; ventricular septal rupture; intracardiac tumour)) and reoperation (previous cardiothoracic surgery).
Ethics
The study was approved by our local institutional research ethics committee. The committee agreed that a formal approval was not necessary.
Clinical policy
Guidelines perioperative policy
The guidelines established in our Heart Centre for the administration of blood products ensured that a uniform policy was applied to all patients. The protocol for preoperative screening of patients, perioperative use of autologous cell salvage, perioperative monitoring and blood component therapy did not change during the study period.
The cell salvage device (Fresenius Kabi, C.A.T.S, Schelle, Belgium) was used in our clinic in 100% of the procedures pre- and post-heparinization. During extracorporeal circulation (ECC) pericardial suction was conducted. The residual volume of the cardiopulmonary bypass circuit was processed with the cell salvage device to minimize the loss of erythrocytes.
Two grams of tranexamic acid (Pfizer BV, Cyklokapron, Capelle aan den IJssel, The Netherlands) was added to our colloidal priming (1480 ml) and one gram was administered during warming. In all our procedures using ECC, the CDI500 in-line Blood Gas Analyzer (Terumo Cardiovascular Systems Corporation, CDI500, Ann Arbor, Michigan, USA) was used. Astrup, colloid osmotic pressure (COD), plasma free hemoglobin, platelet count and fibrinogen level were measured once per hour. In the case of an overload volume during ECC caused by cardioplegia or in patients with congestive heart failure or sepsis, hemofiltration could be used (no data available). Cerebral oximetry was used in the case of type-a dissection.
Guidelines perioperative and postoperative blood transfusion
The lowest accepted hematocrit during ECC was 20% for elective coronary artery bypass grafting (CABG) procedures. For valve surgery and patients over the age of 75 years, the lower limit hematocrit was 23%. In case of terminal renal insufficiency, the hematocrit was kept above 27%. Platelet concentrate was administered when the platelet count was less than 60 x 109 per litre. The minimal fibrinogen level during cardiothoracic surgery was 1.0 g/l.
Thromboelastometry (Rotem Inc., Durham, NC, USA) was used postoperatively with valve and aortic surgery, measuring the EXTEM, INTEM, FIBTEM and HEPTEM. During CABG procedures, the ROTEM was only used if the blood loss exceeded 150 ml per hour. The use of ROTEM enabled component therapy for transfusing platelet concentrate (PC), fresh frozen plasma (FFP) and Haemocomplettan® P (CSL Behring GmbH, Marburg, Germany) (HC) separately.
Postoperatively, at the intensive care unit, coagulation was corrected in the case of a bleeding patient (>150 ml/hour or persistent blood loss) or hemodynamic instability caused by blood loss. If persistent bleeding occurred, transfusion triggers were changed. A minimal hematocrit of 30% and a fibrinogen level of 1.5 g/l were accepted. If the platelet count was reduced, the lower limit of fibrinogen was 2.0 g/l. If antiplatelet therapy had recently been used or the platelet count was below 60 x 109 per litre, platelet concentrate was transfused. At the nursing ward, only packed red cells (PRC) were transfused, according to the 4-5-6 rule. Packed red cells were transfused to a patient regarding the hemoglobin level depending on the classification of the American Society of Anesthesiologists (ASA). Transfusion of packed red cells has been considered for a minimal hemoglobin level of 4 mmol/l for patients with ASA classification I; for ASA classification II and III a minimal hemoglobin level of 5 mmol/l and for ASA classification IV a minimal hemoglobin level of 6 mmol/l.
Statistics
The dependent variable in this study was “transfused or not transfused” in any quantity. A total of 4022 patients were enrolled, 1837 of them were transfused. This study distinguishes three groups of patients:
No blood transfusion (control group)
Transfusion of packed red cells only
Any other combination of blood transfusion
The variables or predictors which were used in this study have already been mentioned in section “Patients”. All of these variables were used in the statistical procedures listed below in the section (Figure 2).
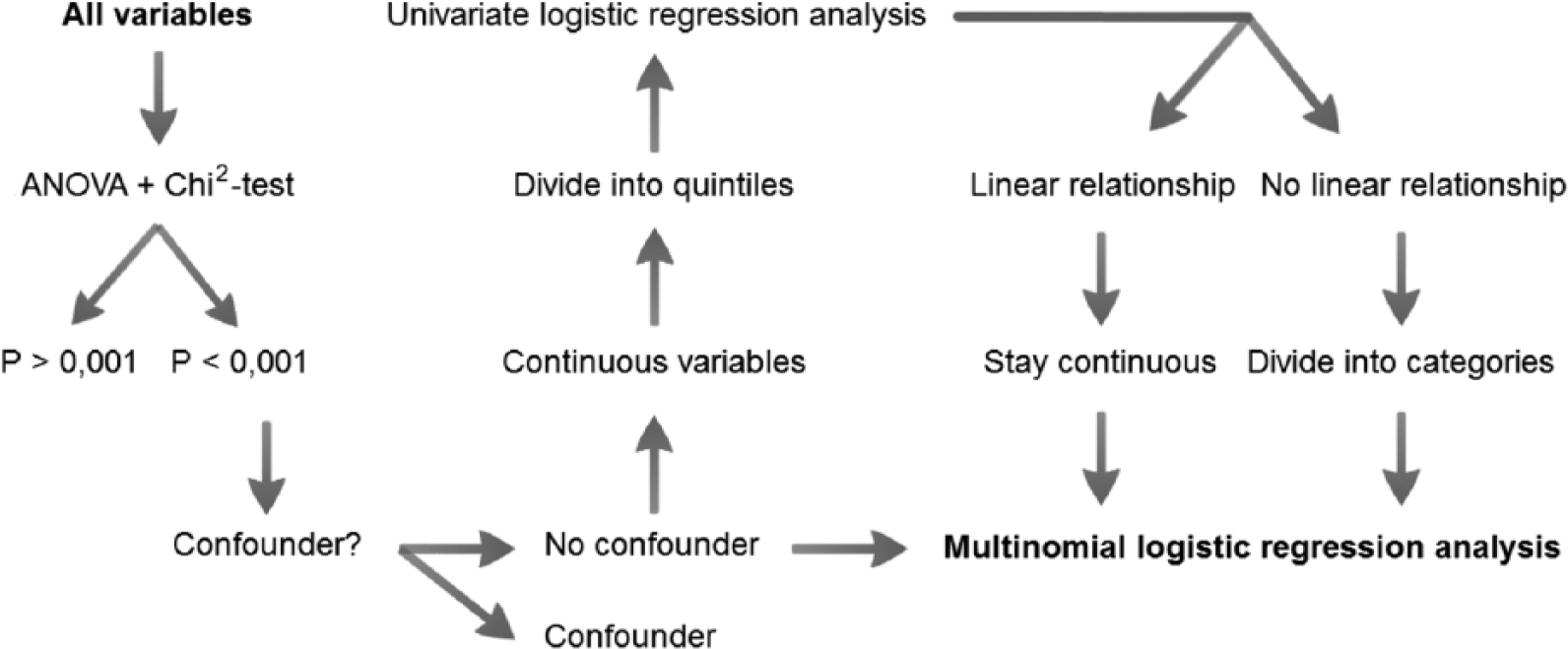
Statistical procedure.
The potential predicting variables were tested with SPSS (SPSS 22 Inc., Chicago, IL, USA) for their association with the dependent variable. The ANOVA test was used for continuous variables and the Chi2-test for categorical variables. Due to the large number of patients, it was assumed that a variable with a p-value of <0.001 was associated with the transfusion of a blood product.
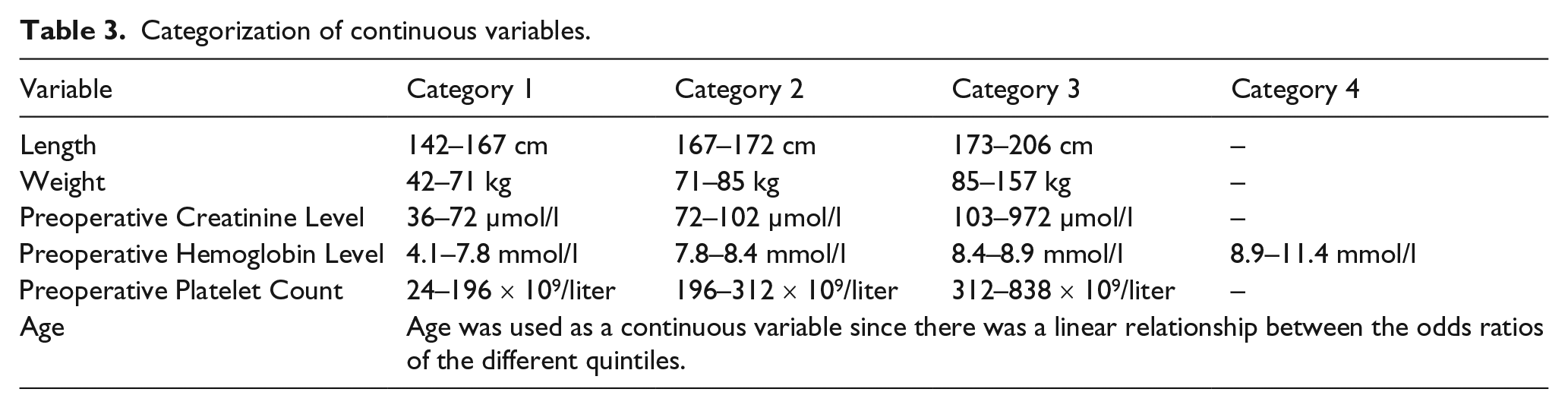
The necessity for categorization of the continuous variables was investigated with univariate logistic regression analysis. For this analysis, the variables were grouped into quintiles (a set of five equal parts sorted from low to high). Similar odds ratios were merged. The variable remained continuous in the case of a linear relationship between the odd ratios of the quintiles.
In a stepwise, multinomial, logistic regression analysis, the variables were, one by one, excluded from the final model if the p-value was >0.05. The final model contained the variables that formed an independent predictive factor for the transfusion of packed red cells or other blood products. The final model was tested with the Hosmer-Lemeshow goodness of fit test. A non-significant result meant the model fits the data.
Results
Differentiation transfusion groups
Patients were differentiated into three groups: Group A (n = 2185) was the control group in this study and consisted of patients who did not receive any blood transfusion. Group B (n = 841) included patients transfused with packed red cells only. Group C (n = 996) included patients transfused with any other combination of blood transfusions. This differentiation is shown in Table 1. The overall transfusion rate of packed red cells was 38.0% (packed red cells only 20.9% and packed red cells plus others 17.1%).
Differentiation transfusion groups.
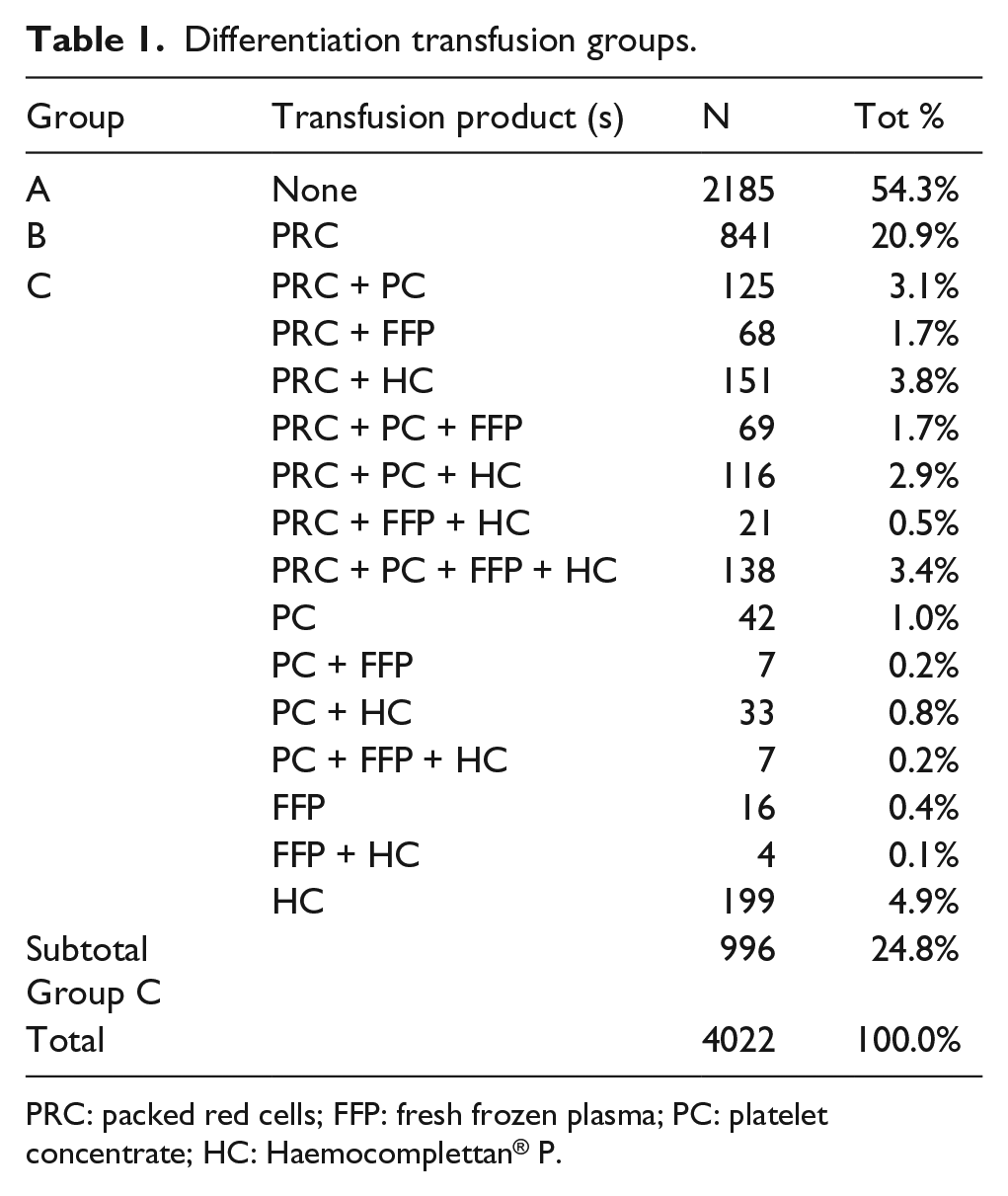
PRC: packed red cells; FFP: fresh frozen plasma; PC: platelet concentrate; HC: Haemocomplettan® P.
Demographic, medical and surgery-related data
The demographic, surgical-related and medical data of the patients are shown in Table 2. The calculated average or percentage is shown per group. Association between gender and the administration of a blood product (Group A vs. Group B or Group C) was tested with the Chi2-test and was significant.
Demographic data, surgery-related data and medical data.
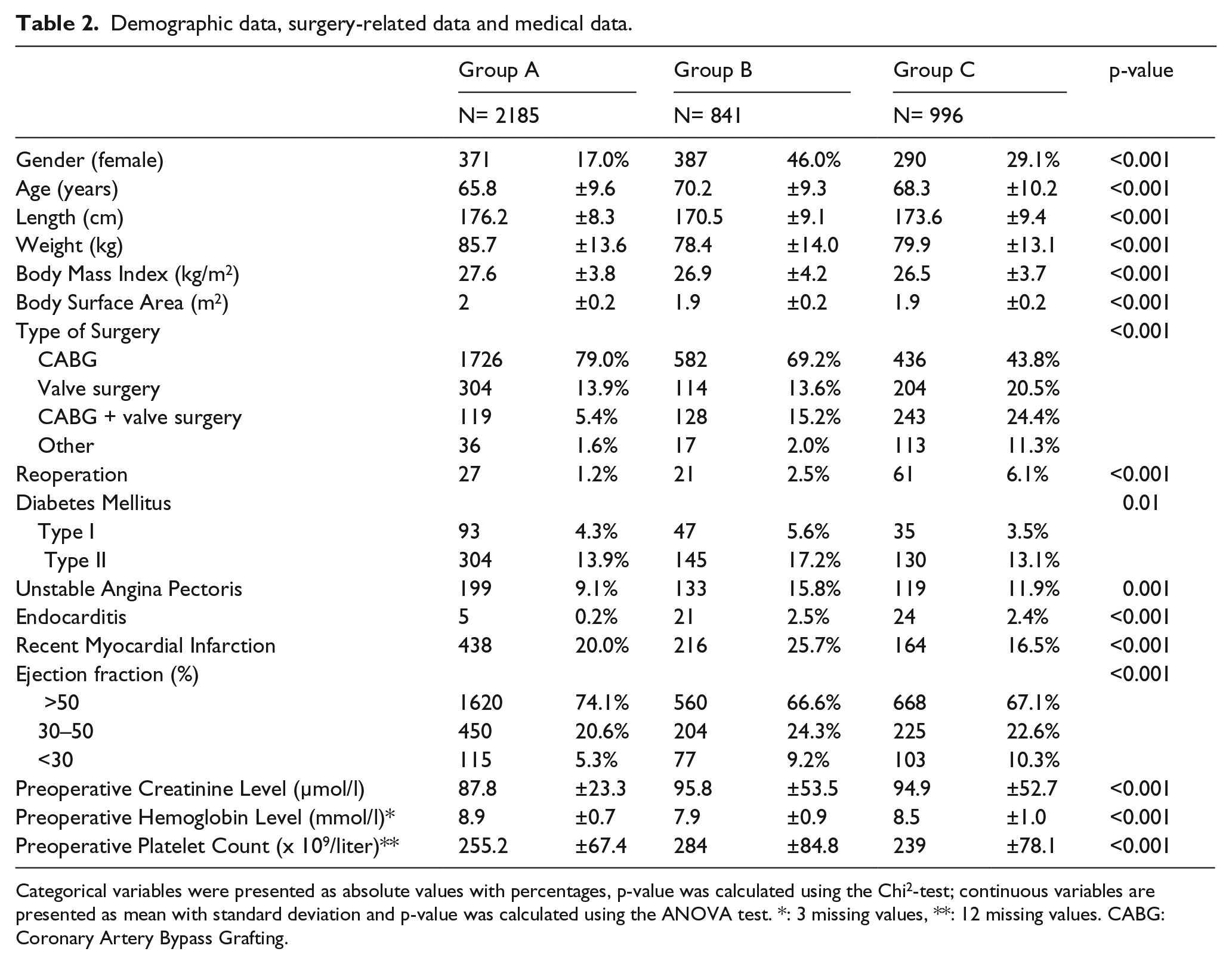
Categorical variables were presented as absolute values with percentages, p-value was calculated using the Chi2-test; continuous variables are presented as mean with standard deviation and p-value was calculated using the ANOVA test. *: 3 missing values, **: 12 missing values. CABG: Coronary Artery Bypass Grafting.
All significant variables (p<0.001) were included in the multinomial logistic regression analysis. Therefore, only diabetes mellitus was not included.
Confounders were excluded before multinomial logistic regression analysis. Therefore, height and weight are included, but the confounding variables body mass index (BMI) and body surface area (BSA) were not.
Categorization continuous variables
The continuous variables were divided into quintiles and assessed with univariate logistic regression analysis. Group A (no blood transfusion) was used as the reference category. Similar odds ratios were merged. The results are shown in Table 3.
Categorization of continuous variables.
Multinomial logistic regression analysis
The results of the multinomial logistic regression analysis included all variables which had an independent association with the transfusion of a blood product. In a stepwise procedure, the variables ejection fraction and length were excluded from the final model (Figure 3). The model was tested not significant (p=0.672) with the Hosmer-Lemeshow goodness of fit test.
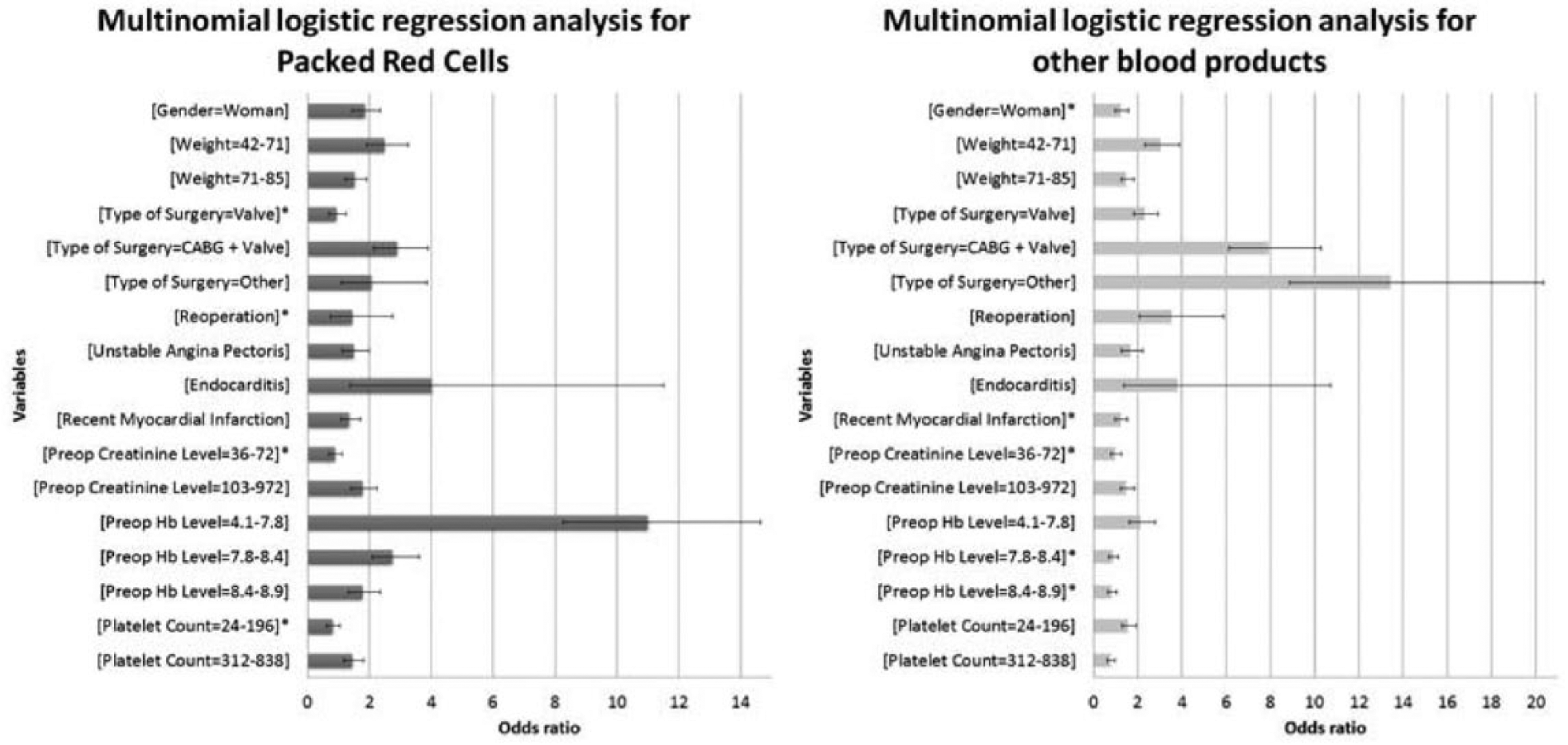
Multinomial logistic regression analysis. Reference group is A (no blood transfusion). Reference categories are: gender = male, weight (kg) = 85–157, type of surgery = CABG, preoperative creatinine level (mg/dl) = 72–102, preoperative hemoglobin level (mmol/l) = 8.9 to 11.4, preoperative platelet count (x 109/l) = 196–312, reference category for the variables re-operation, unstable angina pectoris, endocarditis and recent myocardial infarction are patients who do not meet these variables. *: not significant.
In Group B (transfusion of packed red cells only), the variable preoperative hemoglobin level (4.1 to 7.8 mmol/l) had the highest odds ratio. Categories type of surgery (valve), reoperation, preoperative creatinine level (36–72 mg/dl) and preoperative platelet count (24–196 × 109/litre) were not significant.
The highest association with other blood products (Group C) was found with type of surgery (other). Categories gender (female), recent myocardial infarction, preoperative creatinine level (36–72 mg/dl) and preoperative hemoglobin level (7.8–8.4 mmol/l and 8.4 to 8.9 mmol/l) were not significant for other blood products.
The odds ratio for age as a continuous variable for transfusion of packed red cells was 1.018 and for other blood products was 1.013.
Discussion
In the review article by Khanna et al., 11 62 studies were compared. In these studies, different variables were associated with blood transfusions. Of these studies, 32 were related to cardiac surgery. In, respectively, 20 and 15 of these articles, an association was found with age and gender. This could be explained by the transfusion triggers which were often higher in elderly patients. In addition, elderly patients and women often have a smaller body size and, thus, the effect of hemodilution is stronger. The degree of hemodilution appears to have an important influence on the number of blood transfusions. The association between the transfusion of a blood product with the preoperative hemoglobin level, in combination with body size (length / weight / body mass index / body surface area), has been identified many times before.11–22
The limitation of many of these studies is that they do not distinguish between different transfusion products. The studies which investigated an association with the transfusion of packed red cells did not isolate this group. So, the group of patients who were transfused included patients with a large number of blood transfusions or a combination of different blood products. Magovern et al. 19 divided patients into groups by the number of blood transfusions. As a result, patients with a high number of transfusions and a combination of different blood products were divided into another group. A low amount of blood transfusions could still have a variety of reasons. In our study, it proved beneficial to isolate patients receiving packed red cells only. It revealed that the administration of packed red cells in this group was caused mainly by one reason: hemodilution in combination with a low pre-operative hemoglobin. To avoid the transfusion of packed red cells in this specific group of patients, they could be treated to preoperatively increased hemoglobin levels. In addition, a significant, but weaker correlation was found with the variables age, gender, weight, type of surgery, reoperation, unstable angina pectoris, endocarditis, recent myocardial infarction, preoperative creatinine level and preoperative platelet count.
Using the ROTEM has been associated with a reduction in the number of blood transfusions. 23 Increasing the fibrinogen level at the end of cardiothoracic surgery may contribute to correcting the coagulation. Fibrinogen is the first clotting factor that will be critical with hemodilution and blood loss. An observational study of Blome et al. 24 demonstrated less blood loss postoperatively in patients with a higher fibrinogen level compared with a lower level (2.7 vs. 2.3 g/l).24–28 An increased fibrinogen level could also compensate for a reduced platelet count.29,30 Since using ROTEM in our heart centre, the administration of Haemocomplettan® P has raised significantly. It is possible that some patients received Haemocomplettan® P according to ROTEM results, but unjustified by the clinical situation. On the other hand, correcting the coagulation by Haemocomplettan® P could be the reason for a further reduction of fresh frozen plasma or platelet concentrate in recent years (Figure 1). It is also known that the fibrinogen level does not always correlate with the FIBTEM assay in thromboelastometry (ROTEM). 31
The group “other blood products” could be divided again into smaller groups (Table 1). Transfusion of all blood products (PRC + PC + FFP + HC) and Haemocomplettan® P have a large share in this group. Transfusion of all blood products in one patient has a different cause than the transfusion of Haemocomplettan® P only. A major bleeding or coagulopathy could be the cause of transfusion of all four products. Haemocomplettan® P was often administered, based on ROTEM results or a low fibrinogen level. Haemocomplettan® P administration might, therefore, be caused by hemodilution. The type of surgery had a major impact on the number of blood transfusions in Group C. Liu et al., Alghamdi et al. and Ranucci et al. have also shown that the type of surgery was associated with the transfusion of a blood product.20–22
As an obliged item, validation of the model of multinomial logistic regression analysis was carried out. After validation, the model can be used for predicting which patient is at high risk for a blood transfusion. This patient should be, if possible, treated preoperatively. Ranucci et al. have developed and validated such a model to predict which patients are at high risk for a blood transfusion. Unfortunately, no distinction was made between the various blood products in that study. 20
In our Heart Centre, we already used intraoperative autotransfusion, hemofiltration and antifibrinolytics. Retrograde autologous priming (RAP) could be an addition for our blood management. RAP appears to increase the nadir hematocrit in cardiac patients in general, but there is no solid evidence for a reduction in blood transfusions. Furthermore, it might not be effective for smaller patients, while transfusion of packed red cells actually is more likely in these patients. 7 The preoperative treatment of a reduced hemoglobin level could, in theory, lead to a reduction in blood transfusions,7,32 particularly for patients who are administered exclusively with packed red cells. Preoperative hemoglobin level had the strongest association with the transfusion of packed red cells (Figure 3). The possibilities to increase the hemoglobin level preoperatively are preoperative autologous donation (PAD), iron supplementation and erythropoietin (EPO) administration. PAD is a technique that is not suited for our patient population. Too low hemoglobin level and age above 70 years are exclusion factors of this method in our hospital.7,33,34 Oral iron supplementation has side-effects, possibly leading to non-compliance with drug treatment.7,32,35 Patients treated with intravenous iron supplementation will be clinical. So, the administration of EPO in the preoperative period seems to be effectively, financially and logistically the best method of treatment. This could lead to a further reduction of blood transfusions in our hospital.
Conclusion
For the transfusion of packed red cells alone, any other blood product or a combination with packed red cells, the following predictors were found:
gender;
age;
weight;
type of surgery;
reoperation;
unstable angina pectoris;
endocarditis;
recent myocardial infarction;
preoperative creatinine level;
preoperative hemoglobin level;
preoperative platelet count.
The best predictor for the transfusion of packed red cells was hemoglobin level (4.1 to 7.8 mmol/l). Selective, preoperative treatment to increase the hemoglobin level might reduce transfusions of packed red cells. For other blood products, the strongest association was found with type of surgery (aortic surgery, ventricular septal rupture and intracardiac tumour).
Footnotes
Acknowledgements
The authors greatly appreciate the valuable help of J.S.E Haenen, M. Spiegelenberg, A. Wolthuis, R. Andela and N.J.G.M. Veeger.
This manuscript was presented as a poster during the AmSECT Quality and Outcomes 2015 in San Antonio, TX, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.