
Abstract
Background:
Current blood pumps used for cardiopulmonary bypass generally fall into two different pump design categories; non-occlusive centrifugal pumps and occlusive, positive-displacement roller pumps. The amount of foreign surface area of extracorporeal circuits correlates with post-operative morbidity due to systemic inflammation, leading to a push for technology that reduces the amount of foreign surfaces. Current roller pumps are bulky and the tubing forms an arc in the pumping chamber (raceway), positioning the inlet 360 degrees from the outlet, making it very difficult to place the pump closer to the patient and to efficiently reduce tubing length. These challenges put existing roller pumps at a disadvantage for use in a compact cardiopulmonary bypass circuit. Centrifugal blood pumps are easier to incorporate into miniature circuit designs. However, the prime volumes of current centrifugal pump designs are large, especially for pediatric extracorporeal circuits where the prime volumes are too great to be of clinical value.
Method:
We describe a preliminary report on a novel, occlusive, linear, single-helix, positive-displacement blood pump which allows for decreased prime volume and surface area of the extracorporeal circuit. This new experimental pump design was used to perfuse a 6 kilogram piglet with a pediatric cardiopulmonary bypass circuit for two hours of continuous use. Blood samples were obtained every thirty minutes and assayed for plasma free hemolysis generation.
Conclusions:
The results from this initial experiment showed low plasma free hemoglobin generation and encourages the authors to further develop this concept.
Introduction
Extracorporeal systems used for open heart surgery utilize components that interface directly with human blood. This interaction subjects patients to an increased risk of morbidity and mortality. 1 The amount of foreign surface area of these extracorporeal circuits correlates with post-operative morbidity due to systemic inflammation. This systemic inflammatory response syndrome (SIRS) has led to a push for technology that reduces the amount of foreign surfaces in an extracorporeal circuit. Decreasing the length of plastic tubing used in a cardiopulmonary bypass (CPB) system decreases the amount of foreign material, thus, reducing inflammation.2,3 Roller pumps are considered the standard for pump design for perfusion although centrifugal pumps are gaining popularity, especially within the adult population. 4 Current roller pumps require the tubing to form an arc in the raceway, positioning the inlet 360 degrees from the outlet, making it very difficult to place the pump close to a patient, efficiently reducing tubing length. Remote mounted roller pumps have been described as a method of reducing tubing lengths for pediatric patients. 5 However, when attempting to mimic this circuit design, the authors found too much congestion and confusion of the CPB circuit to make it a realistic solution. These challenges put existing roller pumps at a disadvantage for use in a compact CPB circuit. Centrifugal blood pumps are easier to incorporate into miniature circuit designs, but the prime volumes of current centrifugal pump designs are large, especially for pediatric extracorporeal circuits. The prime volumes in these circuits are too great to be of clinical value. Additionally, centrifugal pumps are only effective as an arterial pump within the CPB circuit, which accounts for only one pump (of several) in a typical CPB circuit. The remaining pumps are used in ancillary positions, i.e. cardioplegia pump and suction pumps. Centrifugal pumps are not useful in these ancillary positions because they must remain fluid-filled at all times and cardioplegia pumps typically use very low flows. Centrifugal pumps do not perform optimally at very low flows.
Efforts have been made to minimize perfusion circuits by reducing the size of the various CPB devices and by reducing tubing diameter and length, but the current pump designs still require a relatively large prime volume and surface area. This fact has identified a need for a pump that is better suited for miniaturized circuits. The novel linear pump can be described as a single helix with ball bearings that can be optimally occluded (Figures 1 & 2). As the cam turns, the ball bearings occlude the tubing and positively displace the volume of fluid within the pump’s raceway. The purpose of our design and development efforts have focused on this need, designing a novel pumping system for use in cardiopulmonary bypass which, due to its linear design, enables clinicians to significantly decrease tubing lengths (Figures 3 & 4). To address the obvious question of hemolysis generation (Figure 5) from this pump design, the following experiment was undertaken.

Rendering of single-helix cam.
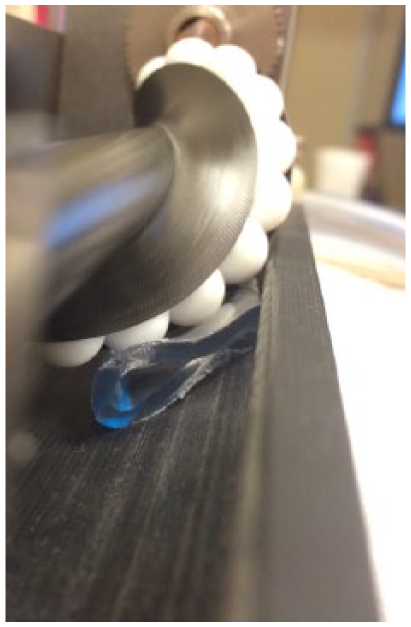
Photo of single-helix cam interacting with tubing in pump raceway.
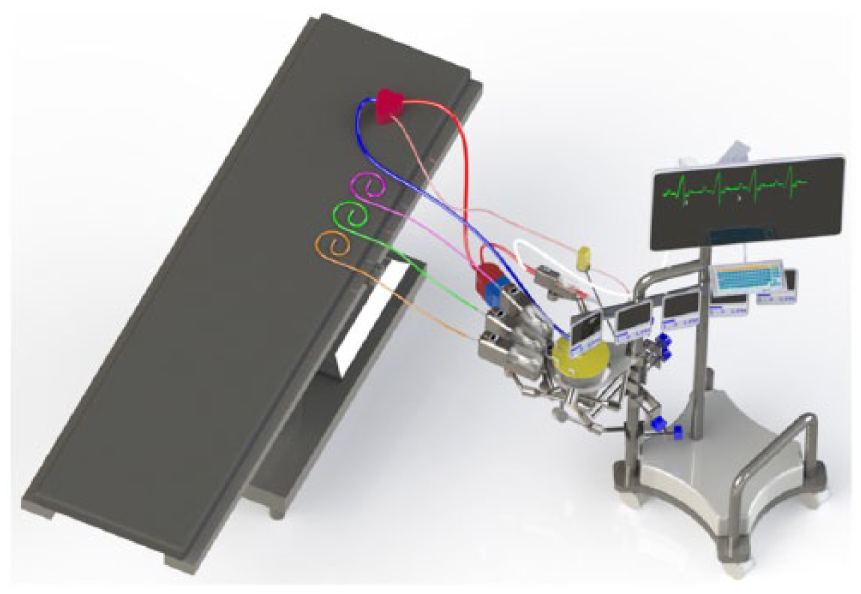
Rendering of CPB circuit utilizing linear pumps.
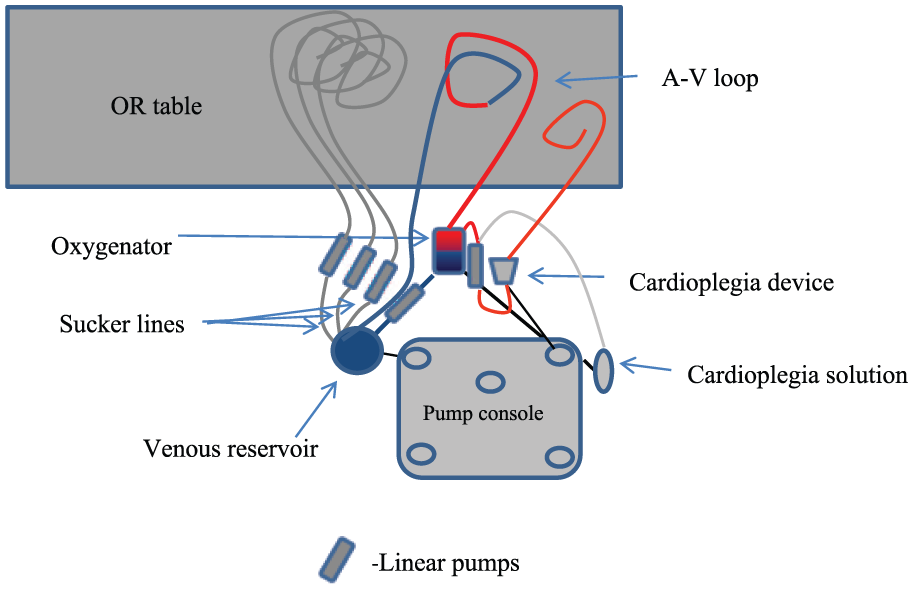
Diagram of CPB circuit utilizing linear pumps.
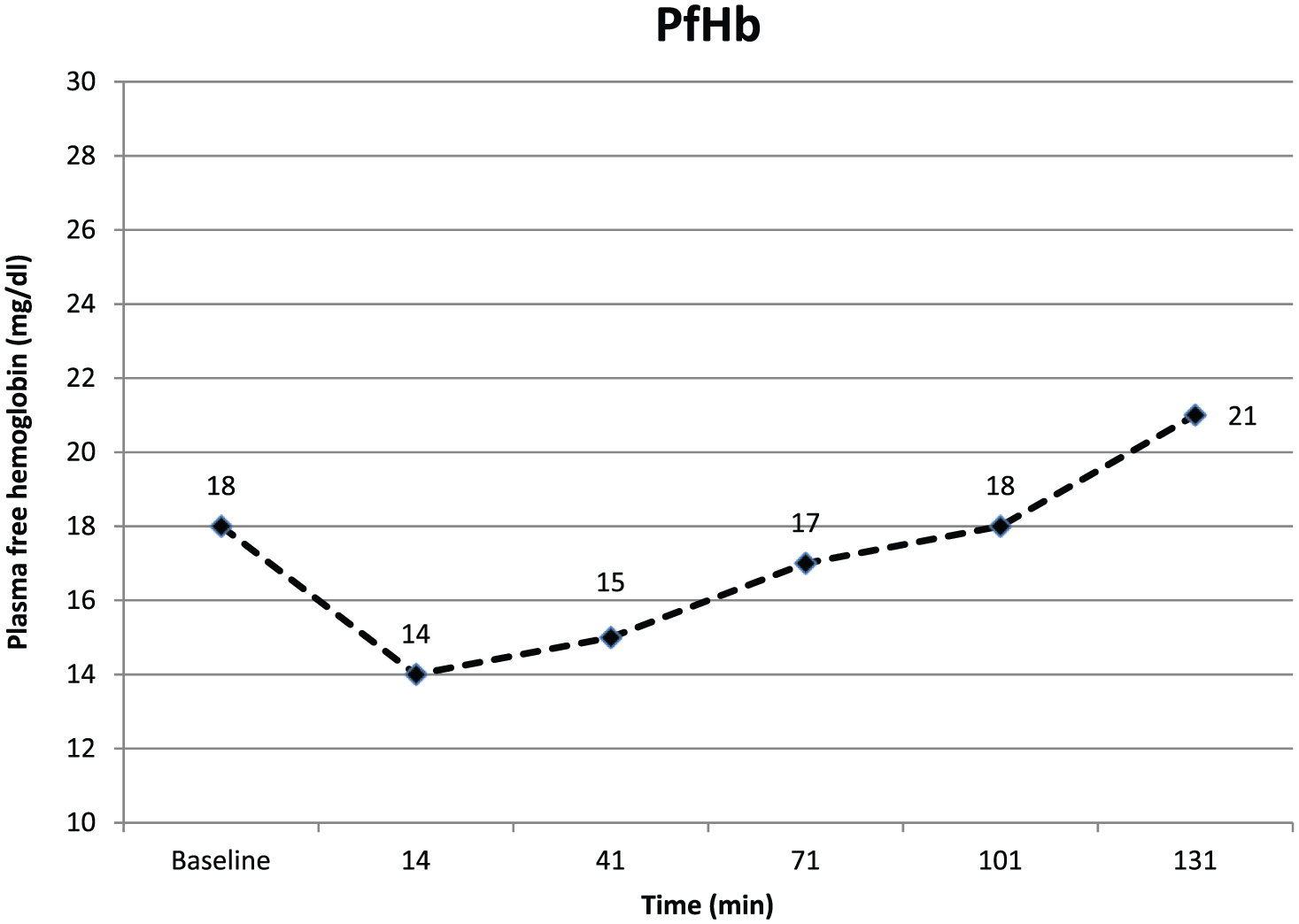
Plasma free hemoglobin data points at 14 mins through 101 mins occurred at a flow of 0.8 LPM and 368 RPM. Flow was then increased to 1.0 LPM at 537 RPM from 101 mins through 131 mins.
Materials and Methods
Two 6 kg standard piglets were prepared for inclusion into this experiment: one was sacrificed as a blood donor and the second piglet was used as the experimental patient. The study was approved by the Institutional Animal Care and Use Committee (no. 107715(08)1D). The animals used for this study received humane care in compliance with the “Guide for the Care and Use of Laboratory Animals”. 6 After three days of acclimatization and a fasting period of 10 hours, two female infant pigs were pre-medicated with ketamine/acepromazine (30–35/1.1 mg/kg IM), atropine (0.05 mg/kg) and buprenorphine (0.05 mg/kg). The donor pig was administered 3000 IU of heparin (Fresenius Kabi USA, Lake Zurich, IL, USA) through the ear vein, then the right jugular vein was catheterized and blood drawn for donation. The pig used as the experimental subject was then intubated and anesthesia continued with 2 −2.5% isoflurane in 99% oxygen, under mechanical ventilation. An 18 gauge butterfly catheter was placed percutaneously into the auricular vein for drug and fluid administration. Rectal temperature was maintained at 37°C during the procedure. Open surgical access for femoral artery placement of the first catheter (22 gauge for blood pressure monitoring, blood gas analysis and blood sampling) and bolus administration of 300 IU/kg of heparin administered prior to initiation of CPB was achieved. An infusion of dopamine (3.0 µg/kg/min prn) was administered for hemodynamic support. An 8 French (Fr.) arterial cannula was inserted into the carotid artery (BioMedicus, Medtronic Inc., Minneapolis, MN, USA) and a 12 Fr. jugular venous cannula (BioMedicus, Medtronic, Inc.) was placed for CPB access; the circuit was then completed. The CPB circuit consisted of a Maquet Quadrox-i Neonatal oxygenator with the VHK 11000 integral open venous reservoir (Maquet Cardiovascular, LLC, Wayne, NJ, USA), 3/8 x 3/32 inch tubing (LivaNova PLC, London, UK) in the linear raceway and ¼ x 3/32 inch tubing completing the A/V loop. This configuration was the entire circuit; no suction nor cardioplegia circuits were included in the test circuit design. The CPB circuit was initially primed with approximately 200 ml of PlasmaLyte A (Baxter Healthcare Corp. Deerfield, IL, USA) with 1,000 units of heparin, 50 mg calcium chloride (Hopira Inc., Lake Forest, IL, USA) and 20 mEq sodium bicarbonate (Hopira Inc.). Once the whole blood (Hct = 26%) from the donor animal was obtained, the circuit was blood primed. This resulted in an Hct of 19% in the test animal’s circuit. Electrolyte, blood gas and hematocrit values were periodically assayed using the i-STAT Handheld system (Abbott Point of Care, Princeton, NJ, USA) and kept within normal ranges for the animal. Gravity venous drainage was utilized for the entire experiment and the arterial line pressure was monitored and kept below 200 mmHg. The new linear pump was tested for slightly over 2 hours while the pigs were maintained under anesthesia, with constant blood pressure and heart monitoring. Flow was initiated at 0.8 LPM at an RPM of 368 and at the 101-minute point the pump flow rate was increased to 1.0 LPM, with a corresponding RPM of 537. The experiment was ended after a total of 131 minutes of bypass. The pump flow rate was increased at the 101-minute point to ‘stress’ the experimental situation in an attempt to better understand the pump’s effect on the animal in a more extreme environment. Blood samples were collected into 0.105M sodium citrate tubes every half hour, with the first draw after premedication. These samples were used for activated clotting time (ACT) (Abbott Point of Care) and hemolysis testing. The ACT was maintained above 500 seconds during the entire procedure. To assess hemolysis, free plasma hemoglobin (pfHb) was quantified (Figure 5). To do so, the first 60 µl of whole blood was removed from each blood sample at each time point and analyzed with a Hemavet® (HV950FS, Drew Scientific Inc., Oxford, CT, USA) to obtain a complete blood count. Subsequently, the blood sample was centrifuged for a period of 10 minutes at 2000 x g to obtain platelet poor plasma. PfHb levels were measured using the hemoglobin assay kit (MAK115-1KT, Sigma-Aldrich Corp., St. Louis, MO, USA), following the manufacturer’s instructions. Results were obtained by measuring absorbance using a UV/visible spectrophotometer (Synergy 2, BioTek, Winooski, VT, USA) at 400 nm. An index of hemolysis (IH) was, thereby, calculated which relates the plasma free to the total hemoglobin:
Wherein Hct is the hematocrit [%], Hb is the total hemoglobin [mg/100 mL] and pfHb is the plasma free hemoglobin [mg/100 mL]. 7
At the end of the testing period and still under anesthesia, the animals were euthanized by an overdose of pentobarbital (2 mL IC).
Results
A baseline blood sample was obtained from the animal at the start of extracorporeal perfusion; the baseline pfHb was 18 mg/dl. The initial sample was obtained after 14 minutes of CPB showing a pfHb of 14mg/dl, 41 minutes after initiation of bypass the pfHb rose to 15 mg/dl, at the 71 minute mark, the pfHb was 17 mg/dl and after 101 minutes of CPB the pfHb was 18 mg/dl. At this point the pump flow rate was increased to 1.0 LPM with a corresponding RPM of 537and, after a total of 131 minutes of CPB, the pfHb was 21 mg/dl (Figure 5).
Discussion
Patients undergoing cardiac surgery with CPB are at risk of major organ system sequelae due to numerous physiologic insults between blood and the artificial surfaces and conditions resulting from CPB circuitry. Some of these insults include hemodilution, hypothermia, exposure to foreign materials, non-pulsatile flow and non-physiologic shear stresses. 8 Significant strides have been made to ameliorate the sequelae of CPB via circuit surface modification, 9 pharmacologic intervention 10 and various new techniques. It is now understood that, in infants undergoing low to moderate complexity cardiac surgery, the contribution of inflammatory mediator production to post-operative morbidity is relatively limited. 11 Much work has gone into decreasing the surface area and prime volumes of CPB circuits. Neonatal oxygenators, hemofilters and cardioplegia devices may have reached the limits of miniaturization. Tubing lengths and diameters have likewise approached terminal limits given current technology. However, pump designs stagnated years ago with the roller pump followed by centrifugal pump designs. Mr. Collin Green hit the nail precisely on the head when he stated, “Admittedly, there are machines today where the arterial pump can be re-positioned closer to the table and sometimes higher, but, to the best of my knowledge, sucker and cardioplegia pumps tend to stay on the machine base.” 12 Mr. Green closed out his thoughts by stating, “So, I ask you all why aren’t more machines produced and used with multi-positional pumps? Why does industry continue building conventional machines with 3/4/5 in a row modular pumps on a base? Why do today’s perfusionists continue to accept this configuration?”
The baseline plasma free hemoglobin value in this study was noticeably higher than the first assay result on CPB (Figure 5). It was noted that the baseline hematocrit (17%) was markedly less than expected and was, initially, confusing. The decreased Hct led to the unexpected need to sacrifice a second piglet for use as a blood donor. Marini et al. reported that a similar phenomenon has been observed when using isoflurane on ferrets. 13 Temporary reductions in Hct, Hb, red blood cell counts, white cell counts and plasma protein levels were observed with a partial recovery after 45 minutes. This resulted in a test animal circuit Hct of 19% despite the use of donor blood. The authors are curious if this isoflurane effect was the reason for the elevated baseline pfHb and are preparing to study this phenomenon.
In conclusion, this new device design occludes tubing as it rotates, to positively displace a volume of blood along its contact length, generating a pressure differential and subsequent flow. The linear design of the pump allows for elimination of approximately 6.1 meters (20 linear feet) of plastic tubing from the extracorporeal circuit. Our current neonatal CPB circuit, used clinically, has a total of 0.22 M2 of surface area; that amount of surface area can be cut by approximately 53% by utilizing this new design. The linear design allows for tubing to come off the operating table and go directly to the venous/cardiotomy reservoir via remotely mounted linear pumps, with minimal redundant tubing traversing over to base-mounted roller pumps for cardioplegia and sucker pump utilization. Additionally, the linear design is less congested and allows for a less confusing tubing route than the remotely mounted roller pumps currently used. This hemolysis data suggests that this new pump design may be acceptable for use in extracorporeal circulation. Further studies are in place to validate this assumption.
Limitations of the study are that it is a single, preliminary experience with the novel pump design on a piglet. This fact prohibits the ability to examine any statistical data. The manuscript is describing an encouraging first experience utilizing the new design in a biological setting.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lawson, Eilers and Jaggers declare that they are listed as inventors for this device on the patent number PCT/US2016/018091. Osorio Lujan and Bortot declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or non-profit sectors.