
Abstract
Cardiac rupture (CR) is one of the most serious and life-threatening complications of blunt chest trauma (BCT) usually associated with high mortality. Moreover, its diagnosis and treatment strategies may be extremely challenging for clinicians due to various anatomical localisations of the tear. Whereas most injuries fall under the category of right atrial ruptures, left ventricular lesions represent a rare type of this injury, with greater mortality, particularly in cases of multi-chamber injuries. However, not only cardiac chamber or great vessel ruptures may occur as a result of BCT; a growing number of reports also describe BCT-induced isolated coronary artery injuries, including ruptures. Whereas CR requires immediate surgical treatment, less invasive interventional techniques, such as stent placement and closure with fibrin glue or coils, can be the treatment of choice in selected cases of hemodynamically less relevant coronary artery ruptures. In this report, we present a rare case of a ventricular rupture following BCT, with the tear localized in the right ventricular wall and an occult connection to the left ventricle without ventricular septum injury. Also, another contemporaneous emergency in our department that had to be managed at the same time resulted in challenging the decision-making process. As such an emergency constellation is difficult to manage, this report may help clinicians in difficult situations in terms of diagnosis and choosing the right treatment strategy.
Introduction
After the first successful repair of a cardiac rupture (CR) in 1955, several cases of blunt chest trauma (BCT) complicated by cardiac injuries were reported. 1 CR is one of the most serious complications of BCT, with substantial mortality that may even increase due to delayed diagnosis. 2 Being diagnosed in 7-12% of all thoracic trauma cases, this condition can be associated with extremely high mortality, depending on the trauma mechanisms and the extent of the rupture. 3 In this report, we describe a rare case of a BCT with a complex biventricular rupture, with a single tear localized in the right ventricular wall with an occult connection to the left ventricle.
Description
A 76-year-old male cyclist suffered a collision with a lorry, resulting in multiple long bone fractures of the upper and lower extremities without involvement of the pelvis, a subdural hematoma and a BCT with multiple rib fractures bilaterally without signs of an unstable thorax. The patient was immediately transported to our high-volume regional referral centre. During the initial body check, the patient had a slight tachycardia of 105 bpm, an adequate respiratory rate of 18 and an arterial blood pressure of 105/65 mmHg. No significant skin lesions or hematoma were noted. Neurologically, the patient was confused, but awake and oriented (Glasgow Coma Scale 13). As the patient was hemodynamically stable and transportable and no significant abdominal injury was suspected, no focussed assessment sonography for trauma (FAST) was performed and a computed tomography (CT) scan was immediately requested. On the CT scan, there were no signs of an active bleed, whereas a notable, but hemodynamically not compromising, pericardial effusion of approximately 2 cm was detected. After a while, the patient required an increasing amount of norepinephrine, gradually rising up to 0.8 μg/kg/min and rapid volume substitution while his central venous pressure (CVP) was permanently increasing and urine output was worsening. Having a strong clinical suspicion of an onset pericardial tamponade, the patient was intubated and an emergent transthoracic echocardiography was performed, showing a hemodynamically relevant pericardial effusion (5 cm in size). After draining 1 L of light red blood using a lock pericardiocentesis set, the size of the pericardial effusion significantly decreased and the amount of norepinephrine support could be reduced to the minimum. Nonetheless, the intrapericardial catheter persisted draining, while both visually and according to the blood gas analysis of several samples from the catheter, it was not absolutely clear as to whether the blood was arterial or venous. There was a suspicion of a potential dissection and a rupture of the left anterior descending (LAD) artery that could be treated interventionally. On the other hand, as the blood was not purely arterial, any other venous or multiple lesions of the heart could not be excluded at that time. Also, as the patient’s hemodynamics were under control after pericardiocentesis, a “wait and see” strategy with clotting factor substitution was also discussed. However, facing the problem of an ongoing blood loss under stable conditions, the decision was made in favour of the less invasive coronary angiography in order to exclude potential LAD rupture or dissection. Heart catheterisation (Figure 1) showed normal coronary arteries. However, an unusual small accumulation of contrast agent was seen in the anterior wall of the left ventricle, adjacent to the interventricular septum, presenting a left ventricular lesion (Figure 2), whereas there were no signs of interventricular septum injury.
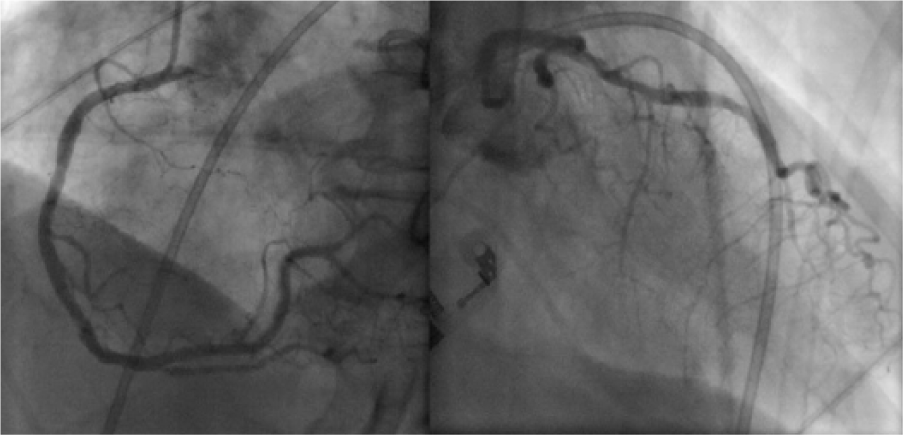
No signs of significant stenosis, dissection or rupture in any coronary arteries.
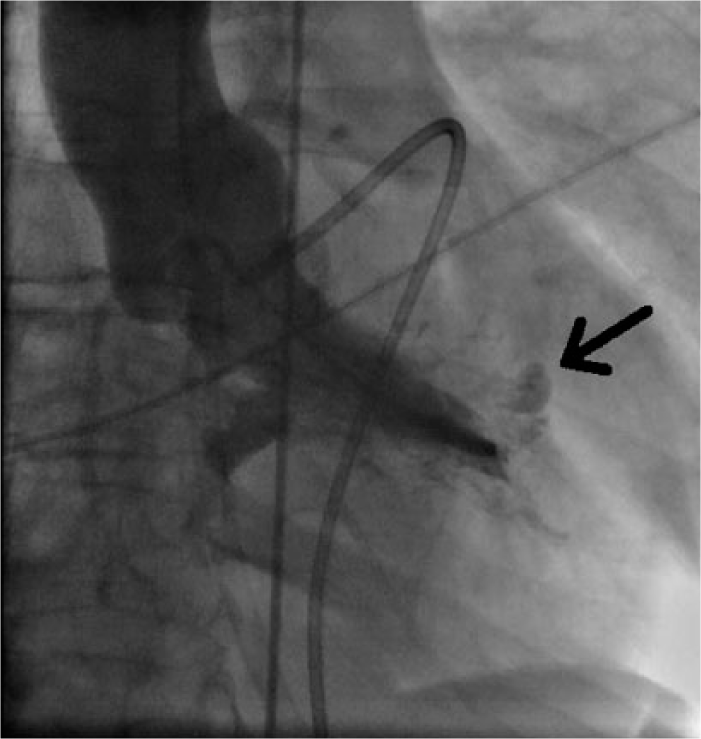
An unusual small accumulation of contrast agent in the anterior wall of the left ventricle.
At the same time, another patient suffered a severe myocardial infarction and subsequent therapy refractory to cardiac arrest, requiring immediate placement on cardiopulmonary bypass under cardiopulmonary resuscitation and subsequent coronary artery bypass grafting. This logistical incident did not allow the cardiothoracic team on call to take the trauma patient to the operating theatre and it was decided to bridge his surgery with conservative treatment on the intensive care unit (ICU). The patient’s coagulation status was deranged, with an international normalized ratio (INR) of 1.5 and a platelet count of 50,000. Apart from platelets (Plt), fresh frozen plasma (FFP) and red blood cells (RBCs), no other clotting factors were given as the bleeding situation was under control and the patient remained hemodynamically stable. A total of 12 units of RBCs, 4 units of FFPs and 2 pools of platelets were transfused, with close monitoring of the hemoglobin and hematocrit levels in order to prevent dilution. As the patient remained hemodynamically stable with sufficient cardiac output, satisfactory pump function and no need for inotropic support, no mechanical support as a bridging strategy was considered. After finishing another emergent surgery, the patient was taken to the operating room where a 0.5 cm lesion was detected in the anterior wall of the right ventricle adjacent to the LAD. The blood was not completely desaturated, representing a mixture of arterial and venous blood. The lesion was successfully closed using two separate pledgeted Prolene sutures. After one day of stabilisation, the patient was transferred to the orthopaedic department for further treatment of his bone fractures. The second patient also survived the emergency surgery and was discharged from hospital.
Comment
Our experience confirms that the decision-making process in a “heart team” in terms of the treatment sequence in difficult cases can be crucial, whereas several strategies might be the right choice. Nevertheless, the diagnosis of cardiac injuries in cases of BCT can be difficult and time consuming as it might be hidden by other symptoms, such as post-traumatic systemic inflammatory response syndrome, multiple organ injury and bleeding with hemodynamic instability. 4 On account of the ambiguous diagnostic results in the present case, our team was facing a clinical dilemma in terms of first choice treatment strategy.
Initially, the decision was made in favour of a less invasive procedure, with the option of interventional treatment of a potential coronary lesion. However, no lesion was detected. This angiography ensured the completeness of the diagnostics excluding other coronary injuries potentially requiring additional coronary artery bypass grafting and providing the reason for the mixed blood consistence in the pericardial space.
Another important problem is to make a decision in terms of the appropriate bridging strategy. In our case, the patient remained hemodynamically stable with good pump function while being transfused. Otherwise, apart from inotropic support, extracorporeal life support as a bridge to definitive treatment may be an option for temporary stabilization, even in local hospitals. Cannulation can be performed by mobile extracorporeal life support (ECLS) teams before transport to the center.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.