
Abstract
We developed a novel open cardiopulmonary bypass (CPB) system, a drainage flow servo-controlled CPB system (DS-CPB), in which rotational speed of the main roller pump is servo-controlled to generate the same amount of flow as the systemic venous drainage. It was designed to safely decrease the priming volume while maintaining a constant reservoir level, even during fluctuations of the drainage flow. We report a successful use of a novel DS-CPB system in an elderly Jehovah’s Witness patient with dehydration who underwent mitral valve replacement.
Case Report
The patient provided written consent for the scientific use of her data.
An 86-year-old, 42-kg, 148-cm Jehovah’s Witness woman who had a 40-year history of mitral regurgitation was referred to our hospital for an exacerbation of heart failure. The patient wished the mitral valve replacement (MVR) to be without blood transfusion.
Her comorbidities included recurring heart failure, anemia, atrial fibrillation and renal dysfunction. The preoperative assessments were as follows; hemoglobin (Hb) concentration 10.1 g/dL, brain natriuretic peptide (BNP) 188 pg/ml, estimated glomerular filtration rate 34.6 ml/min/1.73m3 and international normalized ratio 1.47. A decision was made to wait until the Hb level rose to at least 12 g/dL before proceeding with the MVR.
After stabilization of the heart failure, the patient was discharged from the hospital on erythropoietin (EPO) and iron therapy to correct her anemia. After 5 weeks, the patient was readmitted with an Hb of 15.3 g/dL (Figure 1), a body weight of 37.9 kg and a BNP of 61 pg/ml and scheduled for MVR.
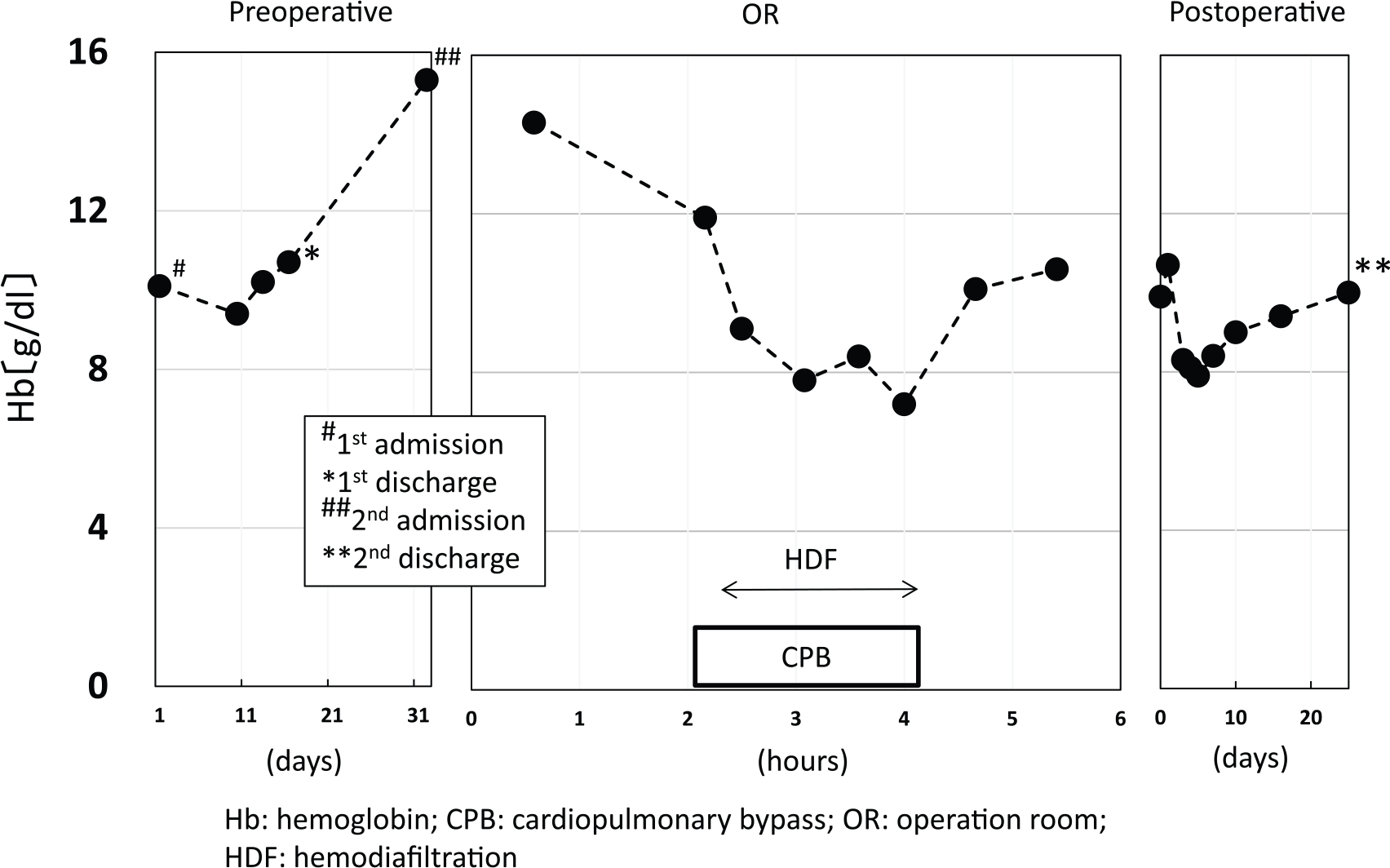
Course of the hemoglobin level.
The baseline hematocrit (Hct) level after anesthetic induction was 42%, hence, autologous normovolemic hemodilution was performed with a target post-hemodilution Hct of 25%. Despite volume replacement with 6% hydroxyethyl starch (1000 ml) and the administration of titrated norepinephrine, only 400 ml of blood was removed due to hemodynamic instability. The blood was kept in continuity with the patient. The final Hct level was 34%.
We started hemofiltration soon after the initiation of CPB since the initial electrolytes demonstrated a high potassium level of 7.5 mmol/L. The aim of hemofiltration is to gradually dilute potassium levels to the lower limit of normal by removing plasma water while replacing it with dialysate (potassium level 2 mmol/L). Hemofiltration was continued throughout CPB. The total fluid extraction during CPB was 4,200 ml and her urine output was 2,000 ml. The patient received a total of approximately 8,000 ml of crystalloid during CPB, consisting of 6,000 ml of dialysate and 2,000 ml of Ringer’s solution.
The procedure consisted of a MVR, a tricuspid annuloplasty and a left atrial appendage closure, requiring 87 minutes of aortic cross-clamping and 119 minutes of CPB, reaching a temperature of 28°C, with the lowest hematocrit value being 23%.
The total blood loss was approximately 500 ml. Serum lactate level at the end of the procedure was 1.5 mmol/L. The patient was extubated on postoperative day (POD) 1. A nadir Hb of 7.9 g/dL was recorded on POD 4. Although the postoperative course was uneventful, the patient was discharged on POD 25 since she felt anxious about returning home, wishing a longer hospital stay and more aggressive rehabilitation.
CPB system
The circuit components were deployed on a HAS II heart-lung machine (Senko Medical Instrument Mfg., Tokyo, Japan). The open CPB circuit consisted of a roller pump, a membrane oxygenator (Terumo Capiox FX15, Terumo Cardiovascular Systems Co., Tokyo, Japan) and a hard-shell reservoir with a minimum recommended reservoir level of 70 ml (Terumo CX-RR30, Terumo Cardiovascular Systems Co.). An ultrasonic flow probe was placed on the venous line of the CPB circuit and the main pump was servo-controlled to produce the same amount of flow as the systemic venous drainage. The DS-CPB has an alarm system to warn when the flow is reduced to 10% below the target flow.
The circuit was primed with 850 ml Ringer’s bicarbonate solution, 300 ml of 20% mannitol and 5,000 IU of porcine heparin. The pump flow was set at 2.4 L/m2/min and moderate hypothermia of 28 °C was employed. Although interruption of the venous return due to the collapse of a large vein occurred frequently during CPB, arterial flow was reduced instantly by the DS-CPB system (Figure 2), maintaining a reservoir level of 100 ml throughout the CPB course.
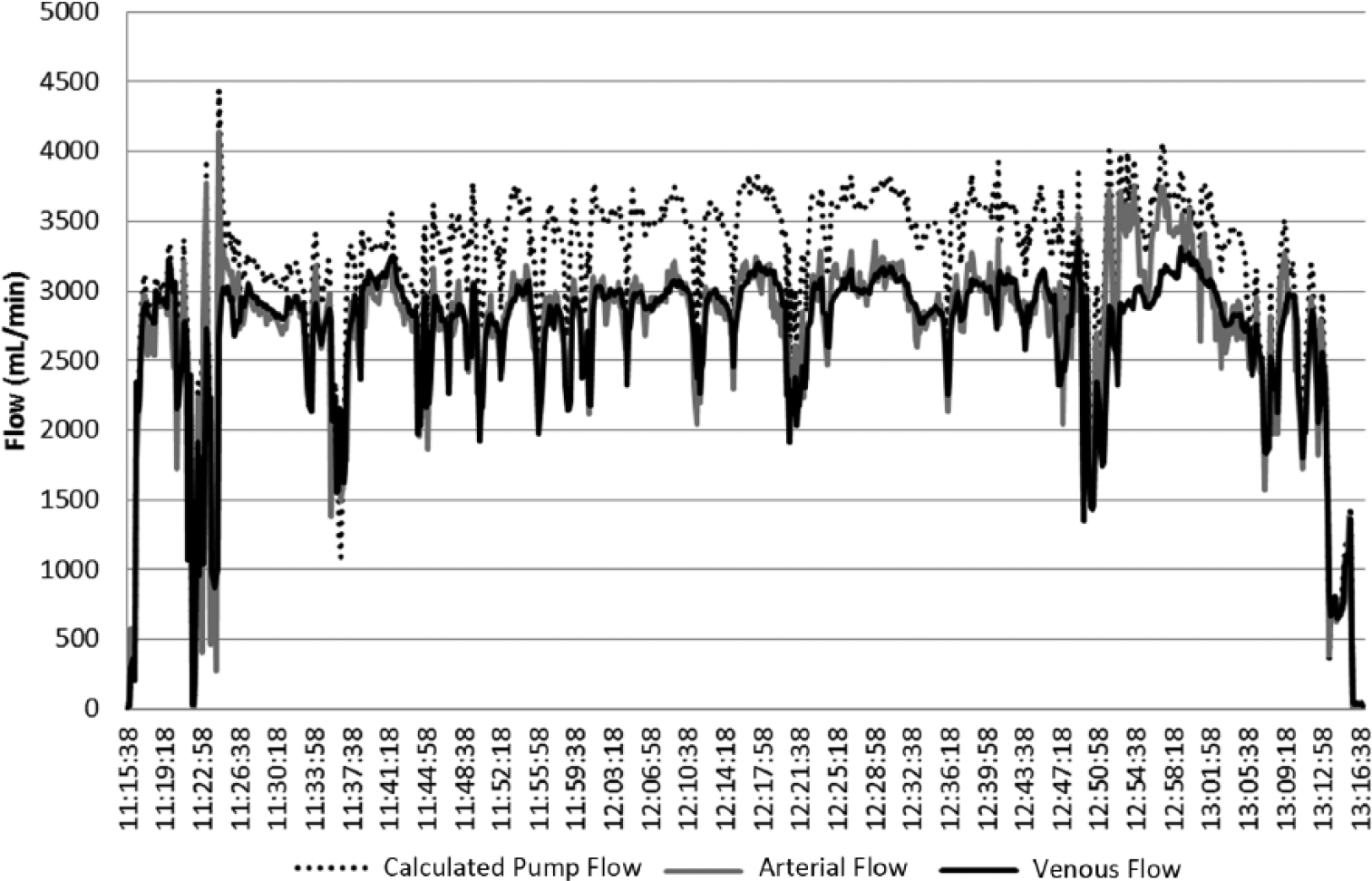
Changes in calculated pump flow and arterial and venous flow during CPB.
Discussion
Our patient was an elderly Jehovah’s Witness woman with anemia, heart failure, renal dysfunction and dehydration. In this case, the pump flow was difficult to maintain due to recurring interruptions of the systemic venous drainage as a result of dehydration.
Preoperative EPO therapy is an important strategy in the management of Jehovah’s Witness patients undergoing cardiac surgery.1,2 One study showed that EPO therapy increased the mean Hb concentration by 1.2 g/dL preoperatively, 3 while our patient showed a rather greater increase in the Hb level (5.2 g/dL). Since a concurrent weight loss of 5.9 kg was observed with the administration of diuretics and strict fluid restriction, we concluded that the increase in Hb was partly due to hemoconcentration.
When the venous return is compromised, the following steps are usually taken in our hospital:
Decrease pump flow immediately;
Notify surgeon and check malposition or air lock in the venous cannulas;
Check blood loss to the cardiotomy suction or to any undetected area;
Confirm the administration of vasodilators by an anesthesia provider;
Give fluid boluses.
DS-CPB allows the perfusionist to skip the first step and use ample time to investigate the underlying causes. In conventional CPB, a rapid fall of venous drainage may lead to a pump stop to avoid massive air embolism, while this system allows the reservoir level to remain constant and prevents the pump from being stopped.
Since we conducted hemofiltration to treat renal dysfunction, a reduction in the hemodilution with the use of the DS-CPB system could not be demonstrated. However, our case suggested that this system could allow the perfusionist to run CPB safely with the minimum reservoir level, even in the dehydrated patient.
Conclusion
We report the successful use of a novel DS-CPB system in an elderly Jehovah’s Witness patient with dehydration who underwent a mitral valve replacement. The system can improve safety and feasibility of CPB management by adjusting the arterial pump flow according to the systemic venous drainage.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.