
Abstract
Objectives:
The real mechanism for the development of the later stages of chronic venous insufficiency still remains unclear. Venous hypervolemia and microvascular ischemia have been reported to be the consequences of venous insufficiency. The aim of this study was to investigate the effects of induced venous hypovolemia by dorsiflexion exercise in patients with venous leg ulcers.
Methods:
Thirty-six participants, all of whom had an ankle brachial pressure index between 0.8 and 1.2 mmHg, were chosen for this study. The participants were divided into two groups: Group A, a non-exercise group and Group B which performed regular exercise in the form of dorsiflexion. The basic assessment, including the history and examination, ankle-brachial pressure index (ABPI), Duplex scan and tcPO2 measurements, was performed on two occasions at the beginning of the trial and after three months.
Results:
The tcPO2 level was low in the beginning in all the subjects, but the picture was different at the end of the trial. There was a significant increase in the tcPO2 level (p<0.001) in the patients who performed exercise while there was no difference in the measurements (p>0.05) in the non-exercise group.
Conclusions:
Induced venous hypovolemia through regular evacuation of the peripheral venous system improved tissue oxygenation at skin level. Venous hypervolemia may be the main contributing factor for the development of venous hypoxia and microvascular ischemia.
Introduction
Chronic venous insufficiency (CVI) is a common clinical problem that affects millions of patients throughout the world. CVI often indicates the more advanced form of venous disorders, namely, venous leg ulcer (VLU). Venous insufficiency occurs as a result of a defect in the venous system, mostly due to damage in the venous valves or an obstruction of the veins. Venous insufficiency leads to venous hypertension, edema, venous hypervolemia, lipodermatosclerosis and, eventually, venous ulcer. 1
It is estimated that the prevalence of VLU is as high as 1%–2%. 2 CVI causes a severe socio-economic burden on both individuals and the healthcare system. The cost of the treatment of CVI is substantial; however, it constitutes 1% of the total annual health budget in Western countries.3,4
Although VLU is one of the most common challenging clinical problems recognised since Hippocrates’ era, there is still no clear understanding of the pathophysiology mechanism, especially in the end stages of the disease.5,6 Since a few theories have been discussed, but no universal agreement has been achieved, we might be able to call it the iceberg of CVI (Figure 1). Lack of understanding of the CVI mechanisms has played a major role in the absence of effective treatment. It is interesting to know that the “gold-standard” treatment is a compression therapy that has been in use since 3000 BC.7,8
The iceberg of venous insufficiency
Researchers have mentioned the development of venous hypervolemia and microvascular ischemia as a consequence of venous insufficiency.9,10 Others reported the effect of exercise on venous insufficiency problems, such as post-thrombotic syndrome. 11
Hypothesis
In CVI, there is a continuous retrograde venous pressure that leads to the dilatation of capillaries and accumulation of venous blood in the microcirculation at the skin level.
The accumulation of venous blood results in venous hypervolemia and peripheral edema. This phenomenon disturbs the normal regular smooth exchange process between venous blood and arterial blood at the capillary level. Accumulated venous blood has a low level of oxygen and the stagnation of deoxygenated venous blood at the skin level could lead to “venous hypoxia and ischemia” (Figure 2).
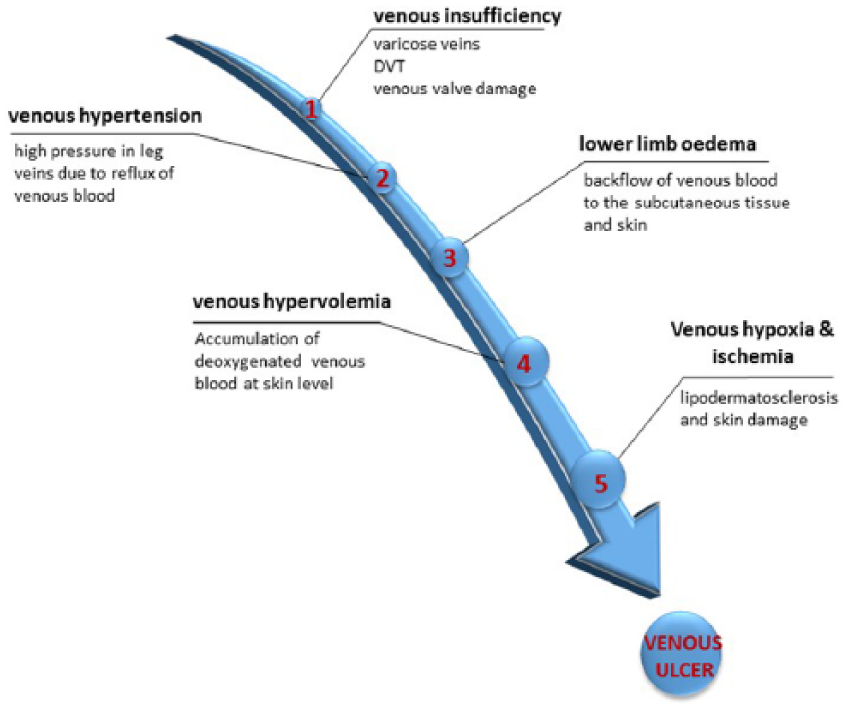
Chronic venous insufficiency process.
Regular exercise may help to overcome venous hypoxia because the pumping action of the calf muscle results in continuous evacuation of the deoxygenated venous blood, replacing it with oxygenated blood (Figure 3).
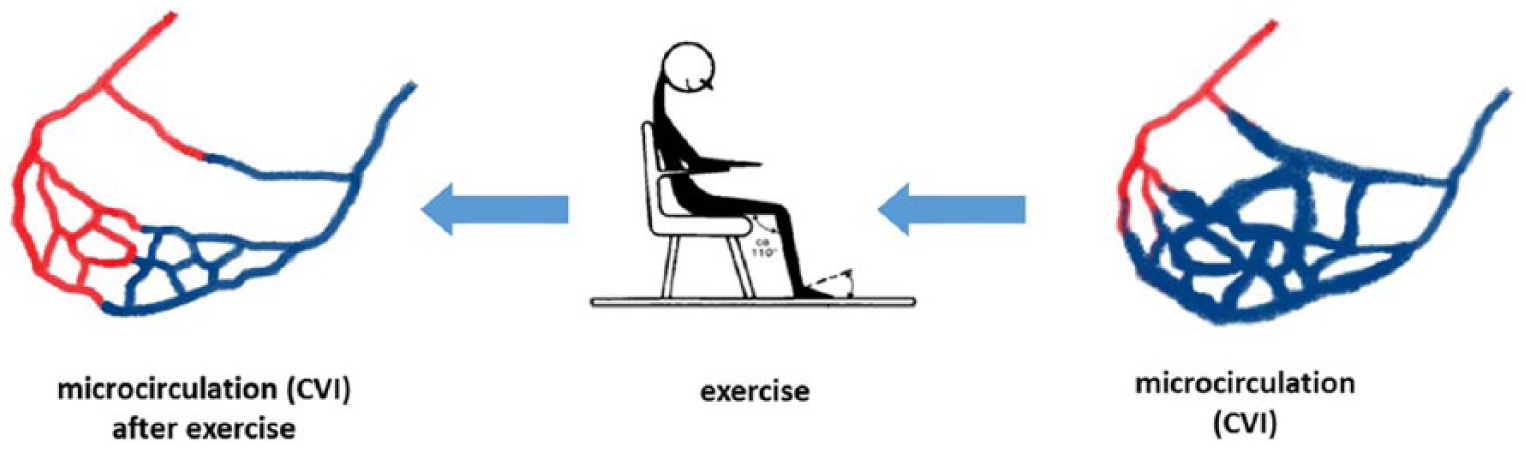
The effect of exercise on venous hypervolemia.
Materials and Methods
A randomised, prospective, pilot study lasted for a period of three months and was performed in a teaching hospital where 36 participants with VLU were recruited out of the 62 who were approached. Inclusion criteria: any patient with a venous leg ulcer who was willing to participate in the study and able to do the exercise has been included. Local ethics committee approval was obtained from the South West - Cornwall & Plymouth National Research Ethics Service (11/SW/0307).
The 26 patients were excluded either because they were not fit for the study or they were not interested. According to the statistician’s advice, since this was a pilot study, the sample size calculation was not required.
The method of randomization was by computer-generated random numbers sealed in envelopes by a member not allied to the research team. Participants were comparable at the baseline in terms of age, sex and body mass index (Table 1).
Participant characteristics.
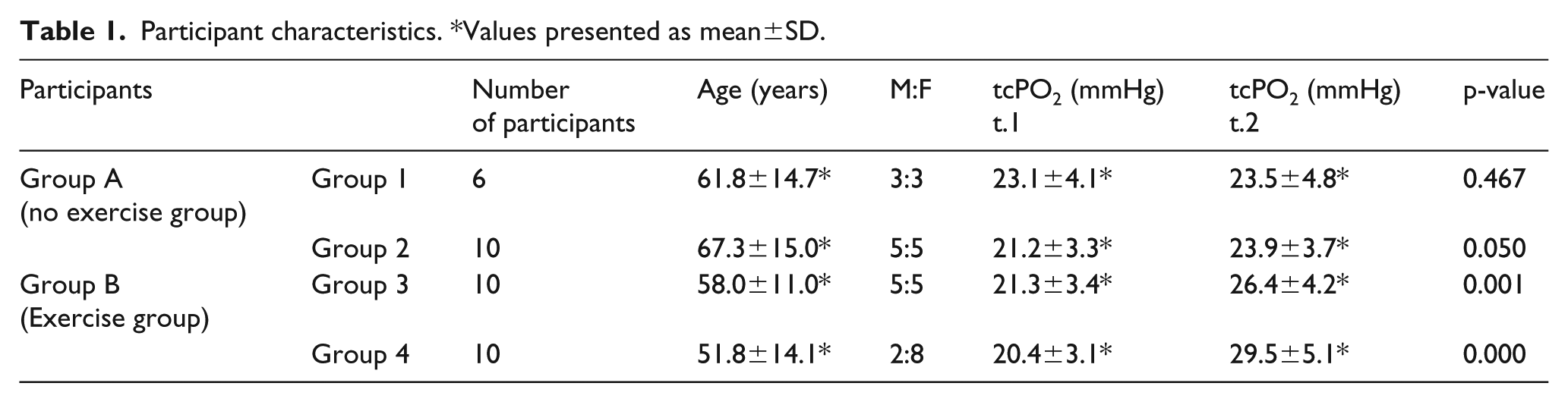
Values presented as mean±SD.
The participants were divided into two main groups (Figure 4); the first group (Group A) was the non-exercise group (n = 16), while the second group (Group B) included 20 subjects who performed the exercise. Each of the two main groups was further divided into two groups according to the treatment they received. Group 1 received no treatment (control group), Group 2 received compression therapy, Group 3 received no treatment but performed the exercise and Group 4 performed the exercise and also received compression therapy.
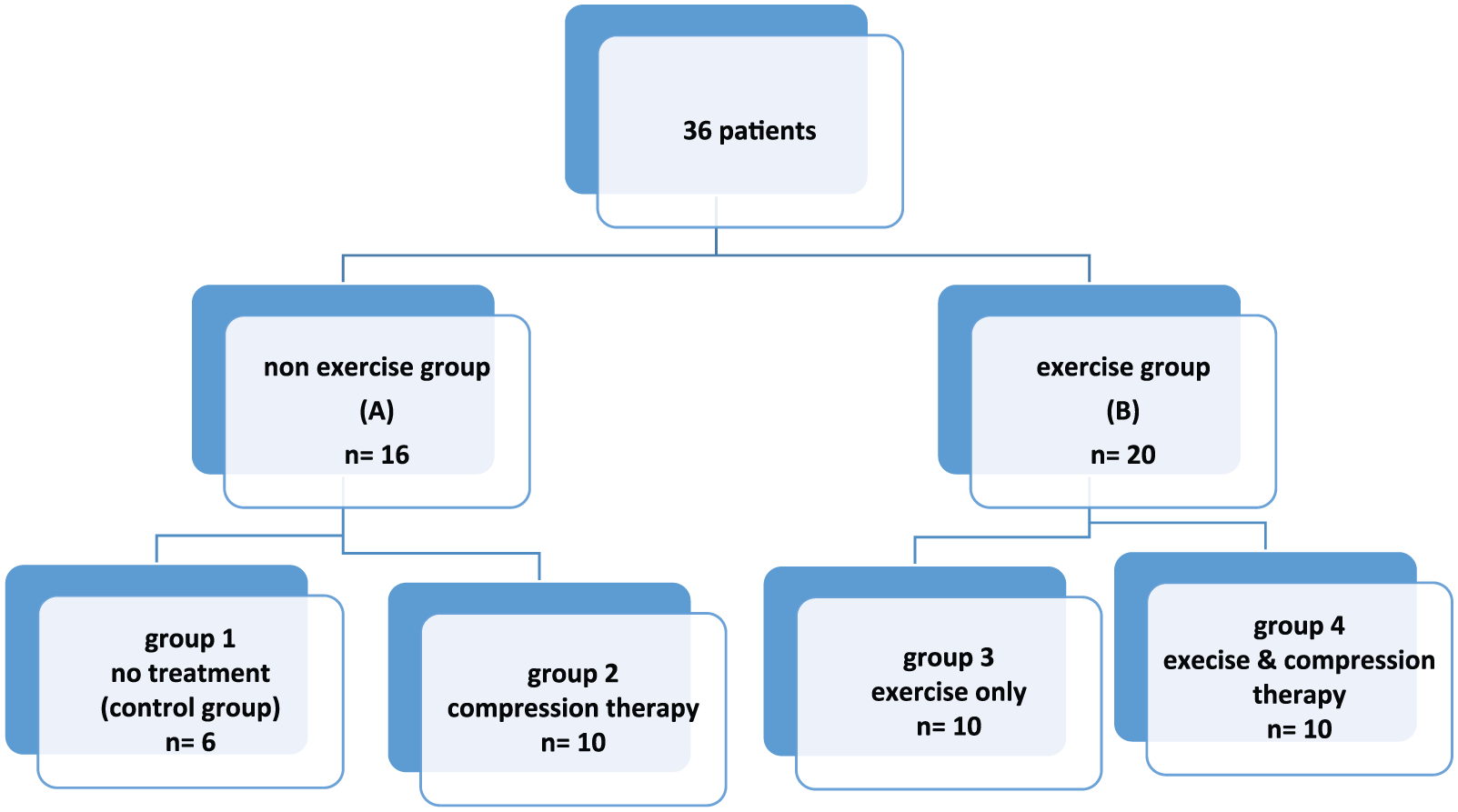
Groups of patients
All the participants had an ankle-brachial pressure index measured (ABPI was 0.94 ± 0.08). The exclusion criteria included peripheral arterial disease (PVD), (ABPI<0.8), signs of cellulitis or infections, use of corticosteroid, non-venous ulcers and patients who were unable to perform the exercise due to either mental or physical reasons.
The PeriFlux System 5000 (Perimed AB, Järfälla, Sweden) was used to measure the tcPO2 level. All the measurements were taken before 10 a.m. to avoid the effect of standing or working for long hours and, particularly, to avoid the effect of oedema. The measurements were taken in a controlled room temperature within the range of 22±1°C. The patients were asked to lie in a supine position and were supported from both sides to keep them as comfortable as possible in order to decrease the effect of movement on the recording.
Immediately after calibration, the area around the ulcer where the probe had to be applied was prepared by stripping the skin 10–15 times with adhesive tape to remove the excessive cells, which resulted in an improved oxygen diffusion that helped in standardizing the measurements. All the ulcers were clean with no inflammation, slough or necrosis at the time of measurements. According to the manufacturer’s protocol, the probe was applied on the gaiter area within 2 cm from the edge of the ulcer.
The exercise performed by the exercise group (Group B) was composed of 10 dorsiflexion movements per hour throughout the day while the participant was awake. The patients performed the exercise in sitting and supine positions. The researcher of the study decided that there was no need for resistance during exercise as it might cause injury to the Achilles’ tendon as most of the VLU patients were elderly. All the participants were provided with a log book and received a phone call every week from the investigator.
Compression bandages were used for the compression therapy; the pressure measurements and time of change of the bandages took place under the care of a specialist nurse and according to the venous ulcer clinic protocols.
The study lasted for three months. All patients had full history and clinical examination; in addition, they had diagnostic studies, including ABPI and Duplex ultrasound scan. Transcutaneous oxygen level (tcPO2) measurements were taken on 2 occasions: once at the beginning of the study (t1) and repeated at the end of the study (t2).
Statistics
The methodology used was Linear Mixed Models for repeated measures, adjusting for group, gender and age. Bonferroni correction was used for comparisons between the groups. Gender was not a significant outcome measure. The difference between before and after varies across the groups (Table 1), (Figure 5) and (Figure 6). A p-value of less than 0.05 was accepted as statistically significant.
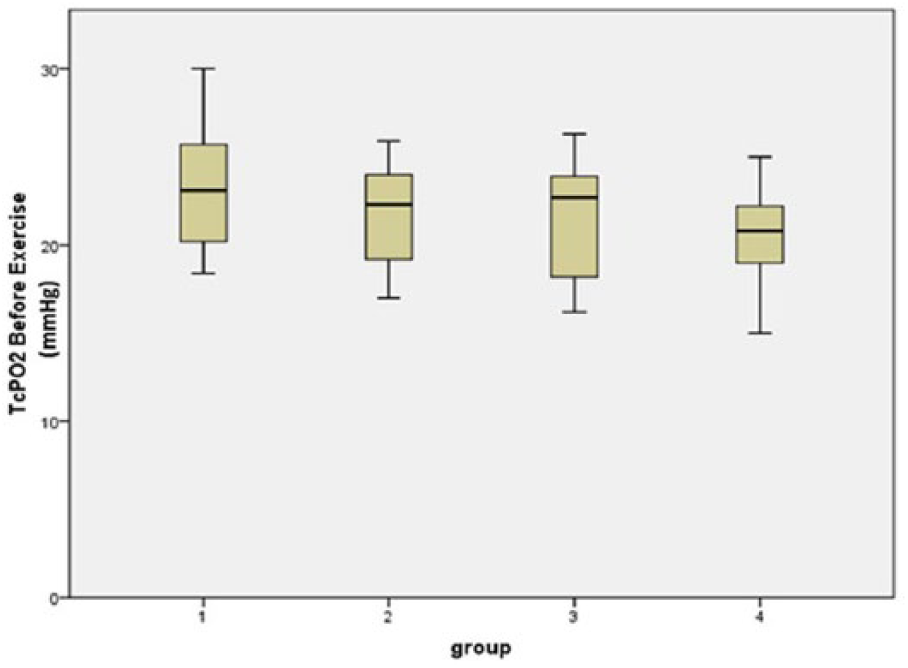
Measurements of tcPO2 at the beginning of the study.
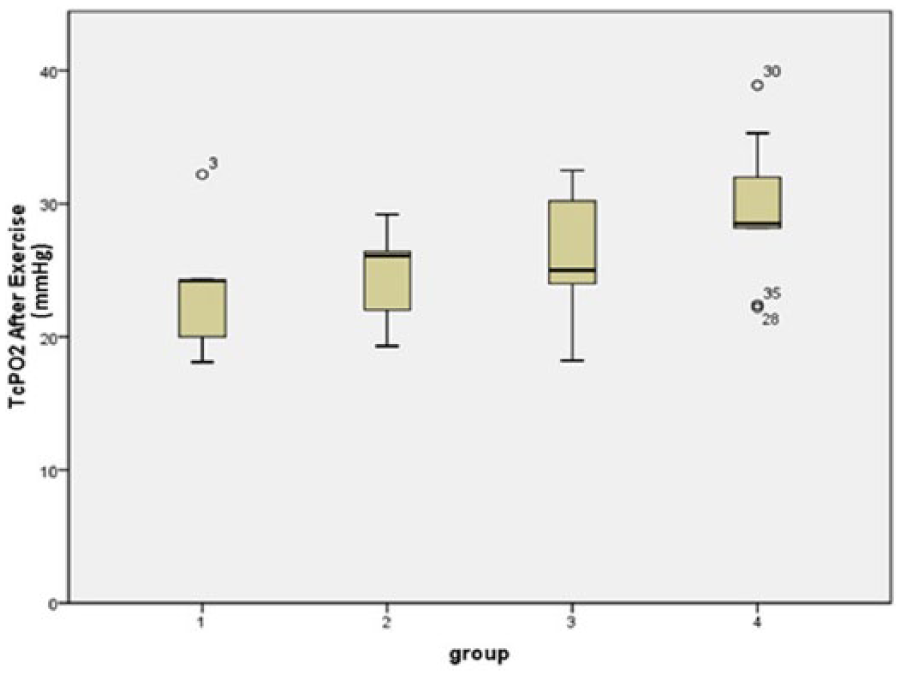
Measurements of tcPO2 at the end of the study.
Results
The tcPO2 level of all the 36 patients was low at the beginning of the study (Table 1), but the picture was completely different at the end of the trial. There was a significant increase in the transcutaneous oxygen level in the participants of Group B (Group 3 and Group 4) who performed dorsiflexion exercise; however, there was no difference or very little in the measurements between the beginning and the end of the study in the patients of Group A (Group 1 and Group 2) (Table 1), (Figure 5), (Figure 6).
Only Groups 3 and 4 showed a significant increase, with a p-value =0.001 and <0.001, respectively. Before exercise, there is no significant difference between the groups. However, after exercise, Group 4 was significantly higher than Groups 1, 2 and 3 and Group 3 was higher than Groups 1 and 2.
Discussion
Even though VLU is one of the most complicated of clinical problems, scientists and researchers do not have a clear idea about the pathophysiology. 12 We know that venous hypertension leads to peripheral edema and venous hypervolemia, which eventually results in venous ulcer.13,14 Despite the identification of the primary hemodynamic factors that lead to CVI, there is no clear understanding of the end stages mechanism.15,16 The lack of clear understanding of CVI pathophysiology has been reflected in different aspects of venous diseases, such as management.
Up to this day, the mainstay treatment for CVI is compression therapy, a therapy that has been used since 3000 years BC. Some people may argue that it is an effective treatment, which it is, otherwise it would not have continued for 5000 years. The key question here though is about the percentage of people who benefit from compression therapy, which, in fact, is low. Researchers have reported several shortcomings of this therapy, such as substantial non-compliance, inefficacy and non-usability; 17 the percentage of non-compliance is very high, up to approximately 80%. 18 The same applies to surgical treatment where the healing rate is only 58.9% and the recurrence rate is 48.9%. 19
As we have seen above, there is a need for an effective treatment for CVI patients. The best way to achieve this goal is to understand the mechanisms of the development of CVI and VLU. There are several theories discussed on the development of venous microangiopathy, but further work is needed as these postulated mechanisms have been criticized and have not gained the research community’s agreement. 20
Franzeck et al. reported that microangiopathy in the initial stages of CVI is characterised by dilatation of the capillaries as a result of continuous retrograde venous pressure; it eventually becomes very dilated and tortuous under the effect of retrograde venous hypertension. 9 The findings were supported by Steins et al. who mentioned that there is a “constant state of venous hypervolemia” in patients with CVI through the propagation of venous blood into the cutaneous capillaries. 10
We proposed that the back pressure due to venous hypertension initiates venous hypervolemia and leads to the accumulation of deoxygenated venous blood in the cutaneous capillaries as this diminishes the space for the arterial oxygenated blood and might be the explanation for low tcPO2 in the venous ulcer area. There was some controversy about the presence of low tcPO2 in patients with CVI among a few researchers; however, researchers now agree on a low tcPO2 in the VLU area.10,21,22
While we have agreed that the majority of cutaneous capillaries are filled with deoxygenated venous blood rather than oxygenated blood, the question that arises is whether the deoxygenated hypervolemia causes ischemia and, eventually, VLU. Logically, when there is a lack of O2 in the blood bathing the skin, the end result will be hypoxemia, cell damage and ischemia of the skin. Therefore, we might call it “venous hypoxia”, which then leads to a venous ulcer or, at least, recognize this as a factor that contributes to the “multifactorial microvascular ischemia” mentioned by Franzeck et al. 9 We should emphasise that this explanation does not exclude the other factors participating in the development of venous ulcers, such as the inflammatory process, although it might be the main and the crucial factor. It is important to mention here that researchers tend to think about complicated explanations for difficult problems like CVI and venous ulcer. On the other hand, we argue that simple solutions could be the answer.
We believe venous ischemia is a different type of ischemia, unlike arterial ischemia where there is a lack of blood supply. In venous ischemia, there is no problem with blood supply, but there is a lack of oxygen within the blood. Our hypothesis gained support when, in our study, we found an improvement in the tcPO2 level in the venous area after regular exercise for three months. The explanation for this is that the accumulated deoxygenated blood was drained under the effect of exercise and was replaced by freshly oxygenated blood. Researchers reported that the venous pressure in the lower calf veins was reduced during exercise. Stegall found that the dorsiflexion exercise of the feet causes a drop in the superficial venous pressure from 90 mmHg to less than 10 mmHg. 23 Other studies have reported the role of exercise in venous ulcer.24-26 However, the majority of these studies focused on the effect of exercise on improving calf muscle function, but no study has reported the effect of exercise on improving oxygenation at skin level.
We propose that exercise initiates the movement of stagnant venous blood underneath the skin into the deep venous system. The venous blood is replaced by fresh fully oxygenated blood which explains the high tcPO2 at the end of the study.
Limitations of the study include the small sample size. The recruitment of such patients is difficult and time-consuming if it takes place in only one centre and, hence, a multicenter study is highly recommended. The exercise performance is highly patient dependent, so compliance needs effort to keep patients adhering to the study protocol.
Conclusions
Our hypothesis suggests that the real mechanism behind developing CVI and a venous ulcer may be the hypervolemia of deoxygenated venous blood that leads to “venous hypoxia” and ischemia and, eventually, venous ulcer. Exercise induces hypovolemia in the ulcer area and leads to the delivery of oxygenated blood. We cannot exclude the role of other factors, such as inflammatory factors, in the development of CVI; however, their role may be minimal.
Footnotes
Acknowledgements
Dr Fabiana Gordon, Statistics Department, Imperial College London was responsible for the statistical advice for the study and conducted the majority of the statistical analyses.
Presented at The Controversies and Updates in Vascular Surgery Conference, Paris, France, 2016.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.