
Abstract
Background:
Endo-epicardial radiofrequency catheter ablation (RFCA) of ventricular tachycardia (VT) as a first-line strategy has been shown to improve outcomes. This study sought to evaluate the feasibility and validity of open-chest epicardial and transapical endocardial substrate ablation for VT with left ventricular aneurysm (LVA) applying to routine cardiac surgery.
Methods:
Porcine models of LVA with VT were developed and were divided into a study group (RFCA from the epicardium via direct-view and endocardium via transapical access) and a control group (endocardial RFCA via retrograde transaortic access). Substrate-based mapping and ablation targeting abnormal potentials were performed under thoracotomy. Outcomes, including procedural success and acute freedom from VT, were analysed.
Results:
Twenty-four of 35 (68.57%) acute myocardial infarction (AMI) pigs developed LVA with VT in a 6-week survival period and were randomly divided into a study group (n=12) and a control group (n=12). All animals in the study group successfully underwent endocardial mapping and ablation by transapical access. The scar size of the endocardium and the left ventricular chamber volume were similar in the two groups. Acute freedom from VT in the study group was remarkably superior to that in the control group (88.33% vs. 58.33%, p=0.04).
Conclusions:
Combined, direct epicardial and transapical endocardial substrate mapping and ablation appeared to be feasible and effective for treating VT with LVA under thoracotomy.
Keywords
Introduction
Left ventricular aneurysm (LVA) is a severe complication of myocardial infarction. Patients with post-infarction LVA have poor outcomes and ventricular arrhythmia is the main cause of death. 1
Surgery, including endocardectomy and cryoablation combined with ventricular aneurysmectomy and coronary artery bypass grafting (CABG), is considered as an effective treatment for post-infarction LVA and ventricular tachycardia (VT). 2 However, myocardial resection and cryoablation, as extensive procedures, may cause extra tissue damage, impairing cardiac function and increasing surgical risk. 3 Previous reports have indicated high perioperative mortality at 5-30%.4–7
Radiofrequency catheter ablation (RFCA) is a valid treatment option for scar-related VT. It is now widely recognized that endo-epicardial radiofrequency ablation of VT as a first-line strategy improves outcomes in terms of VT recurrence and repeat ablations.8,9 Despite significant advancements in catheter ablation, percutaneous epicardial access for mapping and ablation are challenging in terms of technical aspects, operative complications and the complex arrhythmia substrates.10–12 Furthermore, RFCA can only control VT and additional surgical repair of a LVA is commonly required for most patients with post-infarction LVA and VT.
Considering that RFCA has advantages, including precise ablation and less myocardial damage, endo-epicardial mapping and radiofrequency ablation of VT with LVA during off-pump CABG and LVA repair without ventriculotomy may be feasible. However, to the best of our knowledge, there is no suitable RFCA during off-pump CABG and LVA repair. For these reasons, we developed human-like models of VT with LVA and sought to evaluate the feasibility and validity of combined epicardial and transapical endocardial RFCA for VT with LVA during thoracotomy. These models can assist in the development of improved methodologies to capitalize on the major strengths associated with open surgery and catheter ablation in a pre-clinical setting.
Methods
The experimental protocol was approved by the Animal Care and Use Committee of Beijing Anzhen Hospital in affiliation with Capital Medical University (ethical approval number: 2017050X). All animals received humane care and the study was performed according to institutional guidelines.
Development of the porcine LVA model
As previously described, a minimally invasive ligation of coronary arteries via the left chest was performed in 35-45 kg pigs. 13 After an overnight fast and premedication with an intramuscular injection of 0.25 ml/kg xylazine and 0.5 mg atropine, the animals were intubated and ventilated with oxygen. General anaesthesia was maintained with inhaled 1.5-2.5% isoflurane. The heart was revealed by left thoracotomy. Using the whole length of the artery as a co-ordinate, the left anterior descending artery, the posterior descending artery and the diagonal and obtuse marginal branches were ligated totally and permanently at one-third of the distance from the apex (anatomical location by a trisection suture expanding from onset of the target artery to the apex). Continuous electrocardiogram (ECG) and haemodynamic monitoring were performed during the operation. After extubation, the pigs were observed and monitored for 1-3 hours until able to freely ambulate. After a 6-week healing period from acute myocardial infarction, the surviving pigs underwent morphologic and functional assessment of the left ventricle (LV) by left ventriculography (LVG) and transthoracic echocardiography (TTE).
LVA was diagnosed angiographically if all of the following three criteria were found: (1) protrusion of the involved segment displaying either akinetic or dyskinetic motion, (2) absence of trabeculation in the involved segment and (3) well-defined demarcation of the infarcted segment according to the Coronary Artery Surgery Study (CASS) protocol. 14
Electrophysiology study
At the end of LVG, the pigs with post-infarction LVA underwent an electrophysiological study. Before the electrophysiological study, these pigs underwent thoracotomy. The hearts were exposed by a standard procedural protocol involving median sternotomy and pericardiotomy.
Electroanatomic reconstruction of the LV
The 8F and 6F intravascular sheaths were placed in the femoral artery and vein, respectively. Then, 5,000 units of unfractionated heparin were administered via the venous sheath to maintain an activated clotting time (ACT) of 250-350 seconds. Utilizing a Carto3 system (Biosense Webster, Johnson, Diamond Bar, CA, USA) with an 8F 3.5 mm irrigated-tip catheter (Navistar-ST, Biosense Webster), a three-dimensional (3D) electroanatomic map was built.
During sinus rhythm, endocardial mapping of the LV was performed with bipolar electrograms filtered at 10-400 Hz and displayed at a sweep speed of 100 mm/s. The validated bipolar cut-off values of <0.5 mV (dense scar), 0.5-1.5 mV (border zone) and >1.5 mV (normal tissue) were used for mapping. 15 Using a fill threshold of <10 mm, sufficient mapping density was achieved, allowing accurate electroanatomic reconstruction.
VT induction
Programmed electrical stimulation (PES) was performed after electroanatomic reconstruction of the LV. A 6F quadripole catheter (Bard EP, Lowell, MA, USA) was placed in the right ventricular (RV) apex or the right ventricular outflow tract (RVOT) to allow recording and pacing.
PES was performed from the RV apex first. The stimulation protocol included electrical stimulation using a 10-mA current strength and 2 ms pulse width or burst pacing at a basic cycle length of 400-500 ms with up to 3 extra stimuli until down to a refractory period, with or without intravenous isoproterenol (up to 5 ug/min). 16 Sustained VT was defined as tachycardia lasting more than 30 s or requiring cardioversion due to haemodynamic deterioration. 17 If the RV apex stimulation failed to induce VT, the same protocol was repeated from the RVOT. If the VT was haemodynamically not tolerated, it was terminated by pacing or electrical cardioversion.
The models with VT were randomly divided into a study group and a control group. In the study group, the animals underwent combined epicardial and transapical endocardial VT ablation. In the control group, the animals only received endocardial VT ablation by a retrograde transaortic approach.
VT radiofrequency ablation
In the study group, transapical access was built by puncturing the core of the apical LVA. A traction line was sutured in a horizontal mattress fashion at the core of the LVA. Then, an 8F sheath was located in the left ventricle via puncturing between the two horizontal mattress sutures of the traction line. Endocardial mapping and ablation were performed. Then, epicardial mapping and ablation under direct vision were implemented.
In the control group, the endocardial mapping and ablation were performed with a retrograde transaortic approach via femoral access alone.
During sinus rhythm, mapping was performed from the LV endocardium or ventricular epicardium. More mapping points were captured at areas of the LVA, particularly focusing on the border zone of the LVA. Maps were considered complete when the entire chamber of interest was completely mapped. The mapping points were recorded and analysed. The regions including abnormal electrograms (EGMs) that were fractionated and/or had delayed or isolated components are likely responsible for arrhythmogenic substrate. 15 The ablative targets of VT were determined by fractionated electrograms, 18 isolated potentials19,20 and late potentials. 21
In both groups, radiofrequency ablation under sinus rhythm was performed using a 3.5-mm irrigated-tip catheter. The radiofrequency energy was 50 W with a temperature limit of 40°, lasting at least 60 s until abnormal potentials disappeared. The radiofrequency parameters in the epicardium were the same as in the endocardium.
VT induction after ablation
At the end of ablation for abnormal potentials, PES was performed again with the same protocols and sites following the above method to test the inducibility of any VTs. The acute ablation success in both groups was defined by the non-inducibility of any sustained monomorphic VTs before and after the administration of isoproterenol (up to 5 µg/min).
Statistical analysis
All data were analysed using SAS version 9.4 statistical software (SAS Institute Inc., Cary, NC, USA). Continuous variables are presented as the mean ± standard deviation (SD) and categorical data are expressed as the percentage. Student’s t-test was used to address non-paired samples for the comparison of normally distributed parameters and the Wilcoxon test for the comparison of non-parametric variables. The qualitative variables were compared by using the Chi-squared test. Any difference with a p-value <0.05 was considered statistically significant.
Results
LVA models
Thirty-five of the 36 swine (97.22%) underwent the AMI procedure and one animal was lost during anaesthesia induction. One swine developed refractory ventricular fibrillation 10 minutes after coronary ligation despite defibrillation and antiarrhythmic drug therapy. During the AMI healing period, two swine died suddenly 10 days and 35 days after the AMI procedure without preceding signs or symptoms of heart failure. One swine suffered from a stroke, with symptoms of limb paralysis. The swine was subsequently euthanized and a mural thrombosis of the LVA was found at autopsy. The remaining 31 (88.57%) animals spent the survival period of 6 weeks without complications. All survivors had severe cardiac dysfunction compared with baseline (left ventricular ejection fraction (LVEF) 34.52 ± 5.09% vs. 63.32 ± 5.60% p<0.05) and distinct post-infarction LVA was demonstrated by LVG in 28 of 31 (90.32%) animals (Figures 1 and 2).
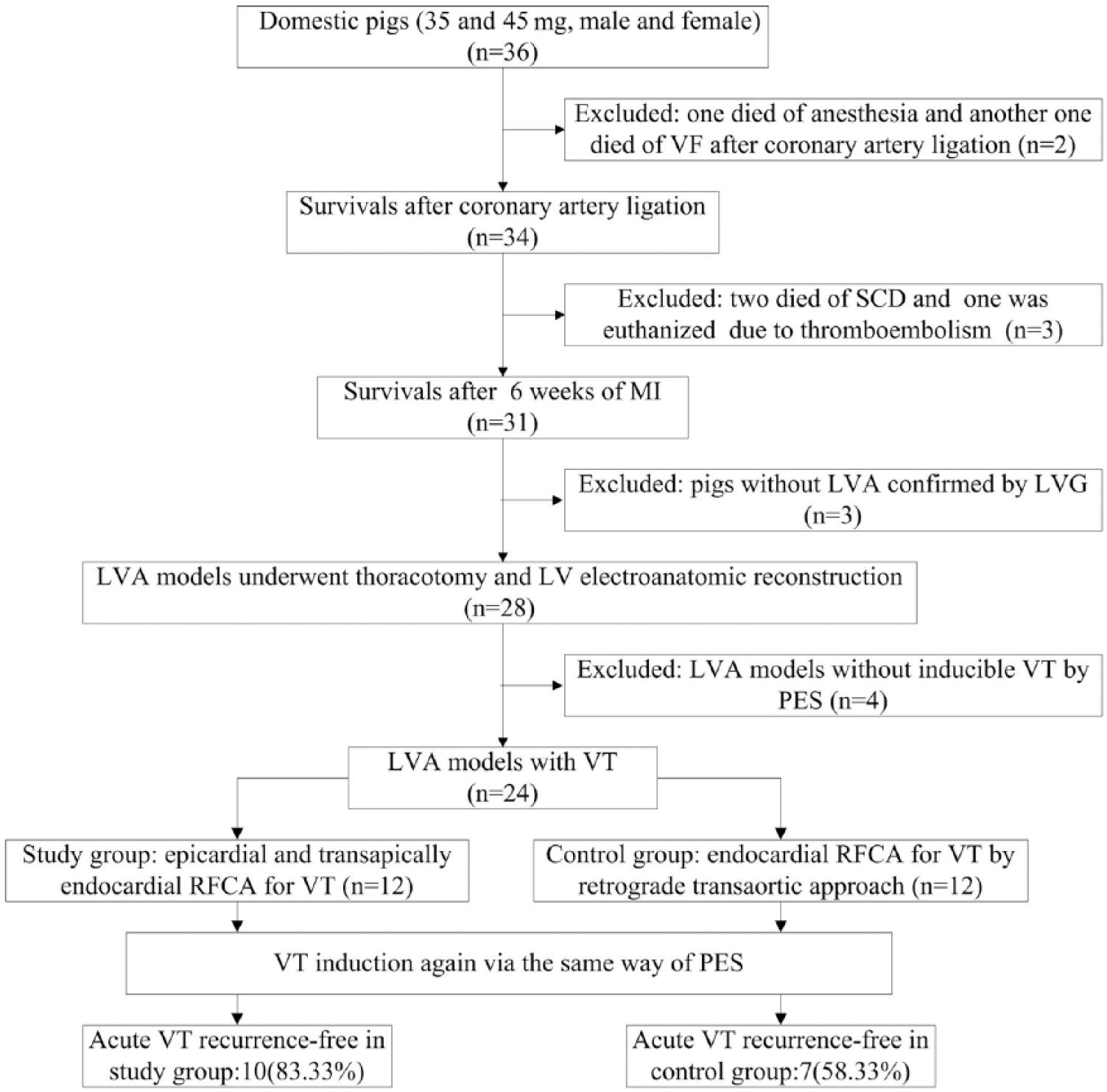
The flow diagram showing the study design and outcomes. SCD: sudden cardiac death; LV: left ventricle; LVA: left ventricular aneurysm; LVG: left ventriculography; MI: myocardial infarction; PES: programmed electrical stimulation; RFCA: radiofrequency catheter ablation; VT: ventricular tachycardia.
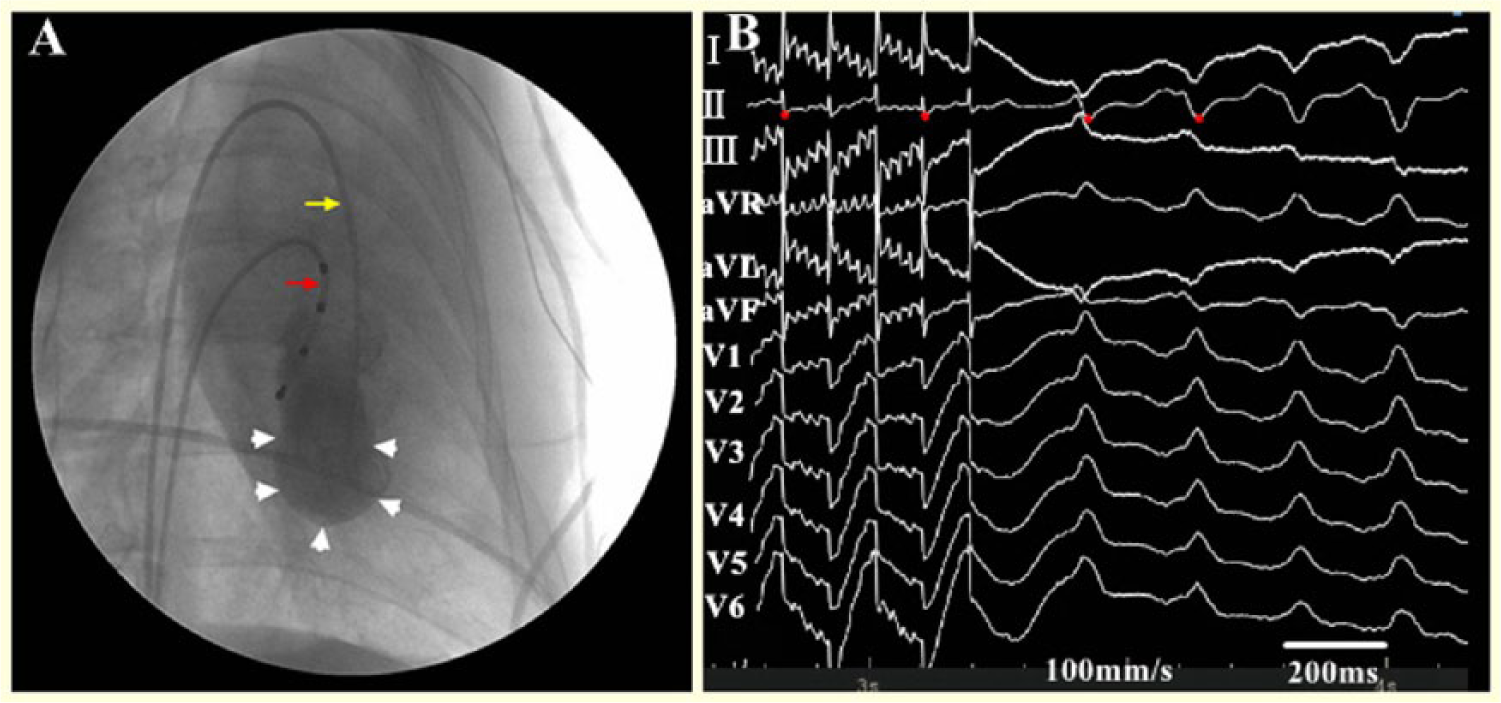
Left ventriculography and VT induction after 6-8 weeks of AMI. A: Ventricular aneurysm was indicated in the apex of the left ventricle (white arrows); a 6F quadripole catheter for stimulation was located at the right ventricle (red arrow); a 6F pigtail catheter was located at the left ventricle (yellow arrow). B: The sustained monomorphic VT was initiated by stimulating at the right ventricular outflow tract. VT: ventricular tachycardia.
Characteristics of VT in models with LVA
Sustained monomorphic VT was induced in 24/28 (85.71%) pigs with PES from the apex of the RV or RVOT (Figure 2). One to three (median 2) extra stimuli were required for induction. A total of 53 VTs were induced (2.21 ± 0.88; range 1-4) with 311 ± 74.9 ms VT cycle length. The left bundle branch block type pattern was seen in 37 (69.8%) and the right bundle branch block type pattern was seen in only 16 (30.2%). The mean duration was 150 ± 72 s (range 40-300 s) prior to VT termination. Only eight (13.2%) VTs were haemodynamically tolerated without inotropic support (intravenous administration of 0.5 mg epinephrine after electrical cardioversion). Finally, twenty-four animals with LVA and VT were randomly divided into the experimental group (n=12) and the control group (n=12) for VT mapping and ablation.
Mapping and ablation of VT
All models of VT with LVA underwent 3D electroanatomic mapping based on bipolar voltage (BV) criteria during thoracotomy (Figures 3 and 4). The endocardial and epicardial EGMs were recorded from 319.42 ± 45.59 (range, 252-392) and 358.42 ± 52.04 (range, 287-456), respectively, distinct points per animal in the experimental group. Only endocardial EGMs were recorded in the control group, with 277.5 ± 39.49 (range, 291-385) distinct points. Abnormal potentials for ablation were tagged onto the endocardial and/or epicardial surface of the LVA in all animals. The area of the scar, as defined by a BV<1.5 mV, was 28.85 ± 4.36 cm2 (range, 23.5-33.5 cm2) on the endocardial surface and 24.26 ± 4.64 cm2 (range, 18.90-31.70 cm2) on the epicardial surface in the experimental group. At the end of ablation, VT was stimulated again with the same PES. Acute freedom from VT was 58.33% in endocardial ablation alone and 83.33% in the combined endo-epicardial ablation, p<0.05. In the study group, 2 of the 12 animals had inducible VTs after ablation, but the VTs were slower, with stable hemodynamics. However, in the control group, among five animals with inducible VTs after ablation, four had rapid VT inducible two extra stimuli. These inducible VTs of both groups did not match the PES protocol, cycle length or morphology of the VTs before ablation. The detailed data on echocardiography, VT induction, mapping and ablation in the two groups are displayed in Table 1.
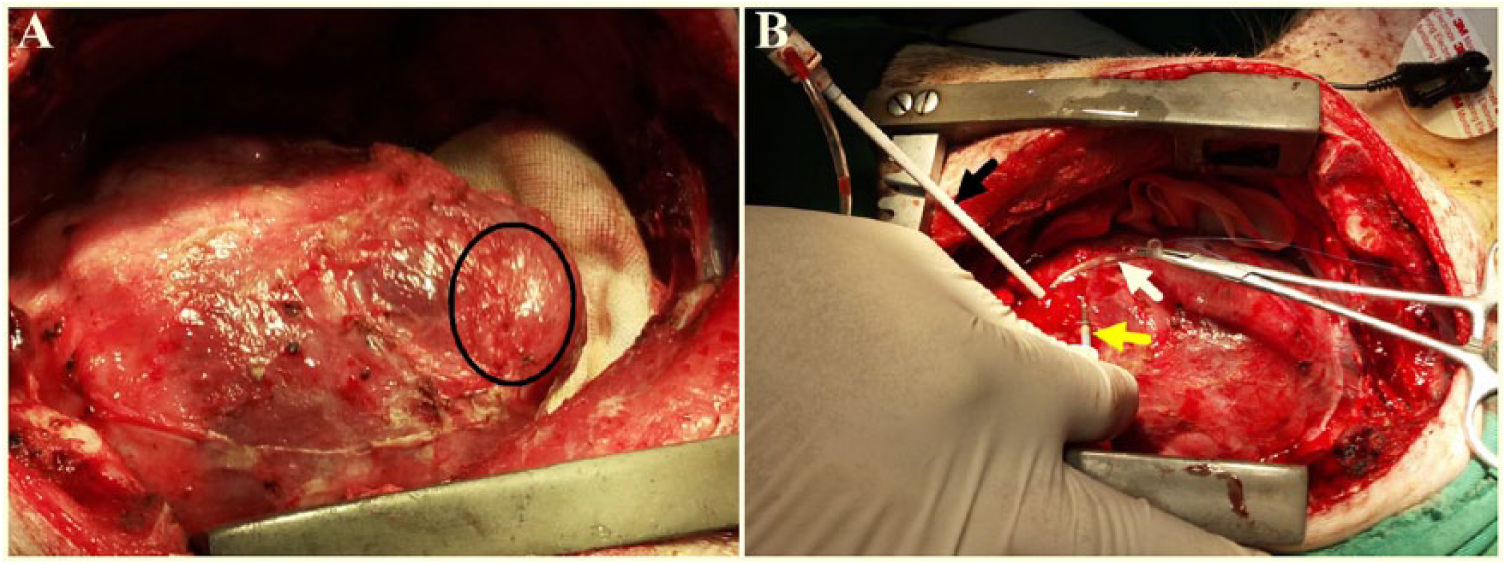
Location of LVA and catheter access during thoracotomy. A: the LVA with distinct margins was located at the apex of the LV (black circle). B: an 8F sheath was placed in the LV by puncturing the core of the LVA (black arrow); haemostasis and sheath fixation were performed by a traction line (white arrow); the yellow arrow indicates an 8F 3.5-mm irrigated-tip catheter. LV: left ventricle; LVA: left ventricular aneurysm.
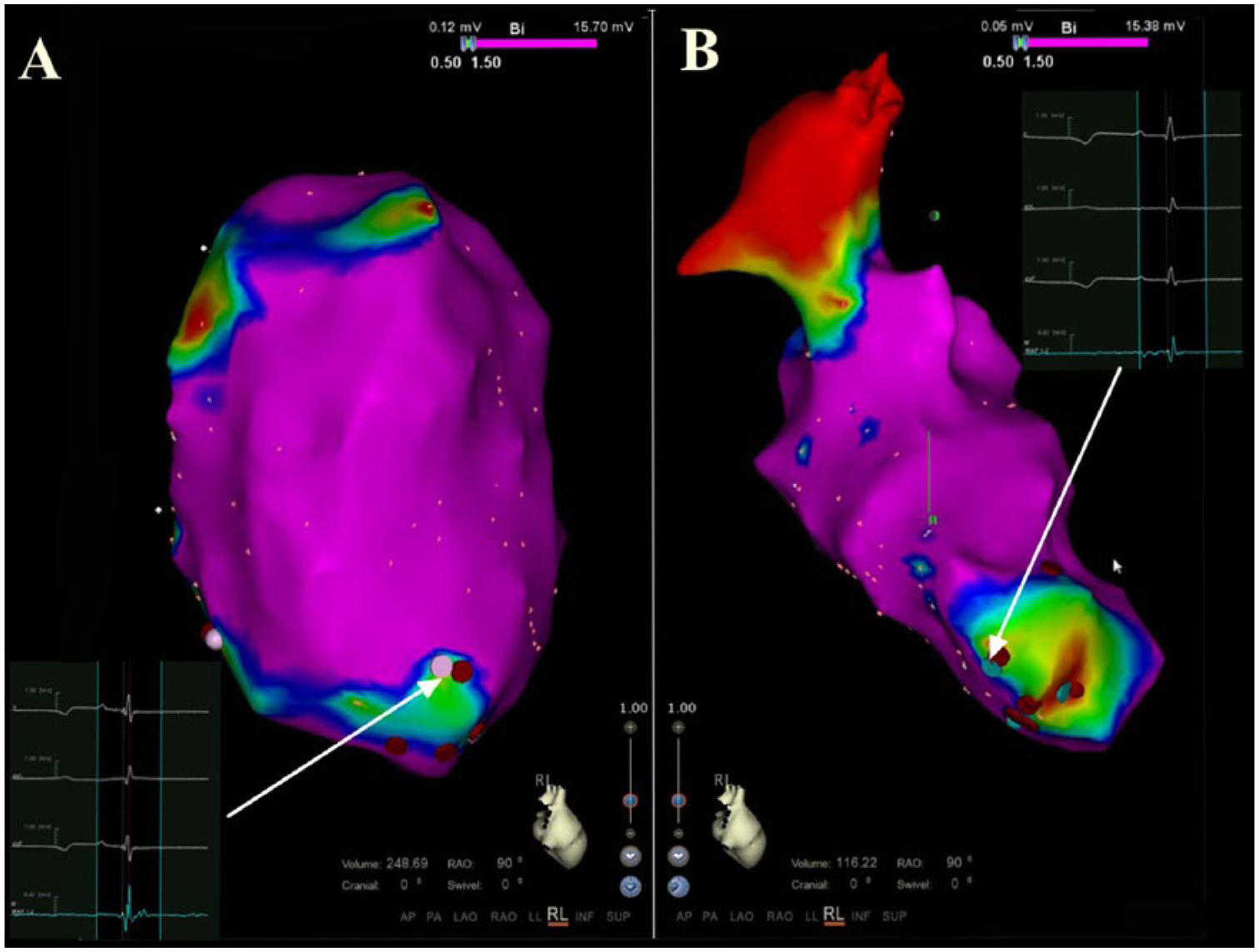
Endo-epicardial mapping and ablation of LVA-related VT in a porcine model. In Figure 4A, the low voltage area (BV<1.5 mV) was identified by epicardial mapping; regions containing abnormal potentials were captured and ablations tagged with coloured dots (white arrow); regions with abnormal potentials were ablated and tagged with red dots. In Figure 4B, the low voltage area (BV<1.5 mV) of the endocardium was identified by transapical mapping; coloured dots indicate abnormal potentials and targets of ablation (white arrow). BV: bipolar voltage; LVA: left ventricular aneurysm; VT: ventricular tachycardia.
Experimental data in the two groups.
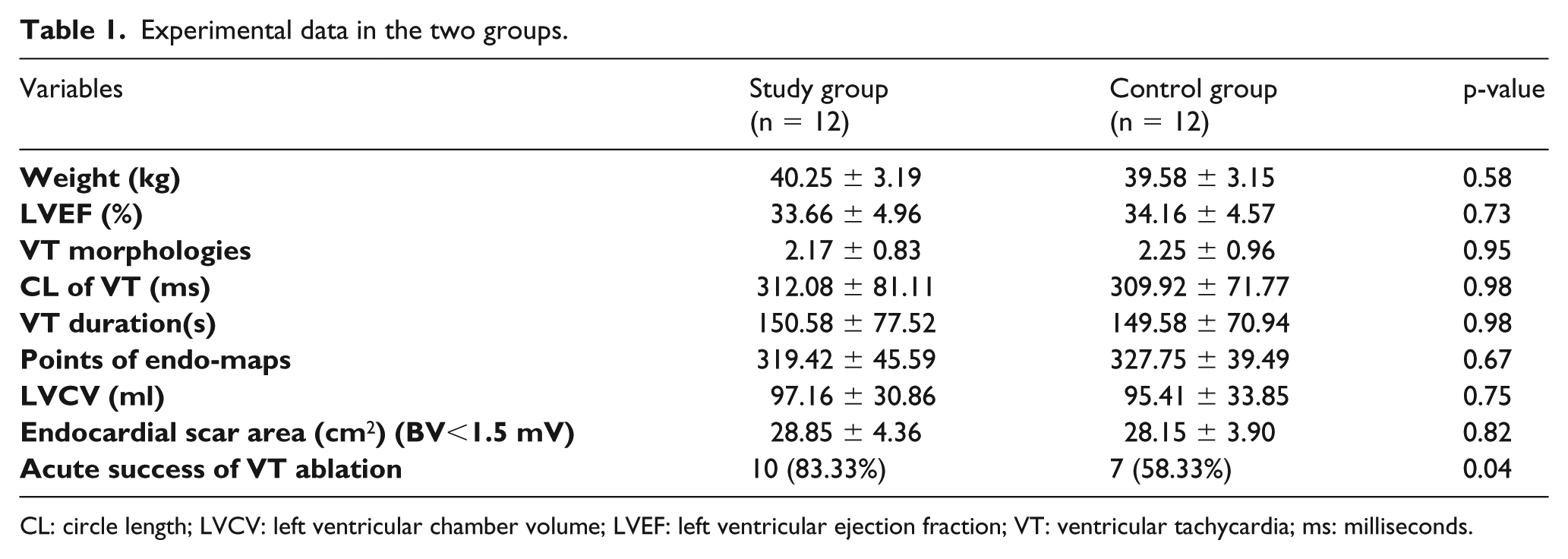
CL: circle length; LVCV: left ventricular chamber volume; LVEF: left ventricular ejection fraction; VT: ventricular tachycardia; ms: milliseconds.
Correlation of the endocardial BV maps via transapical access versus transfemoral access
Endocardial substrate mapping was performed smoothly via transapical access or transfemoral access due to the relatively regular shape of the LVA. Differences were not found in terms of the number of captured points or size of scars defined as a BV<1.5 mV (Figure 5).
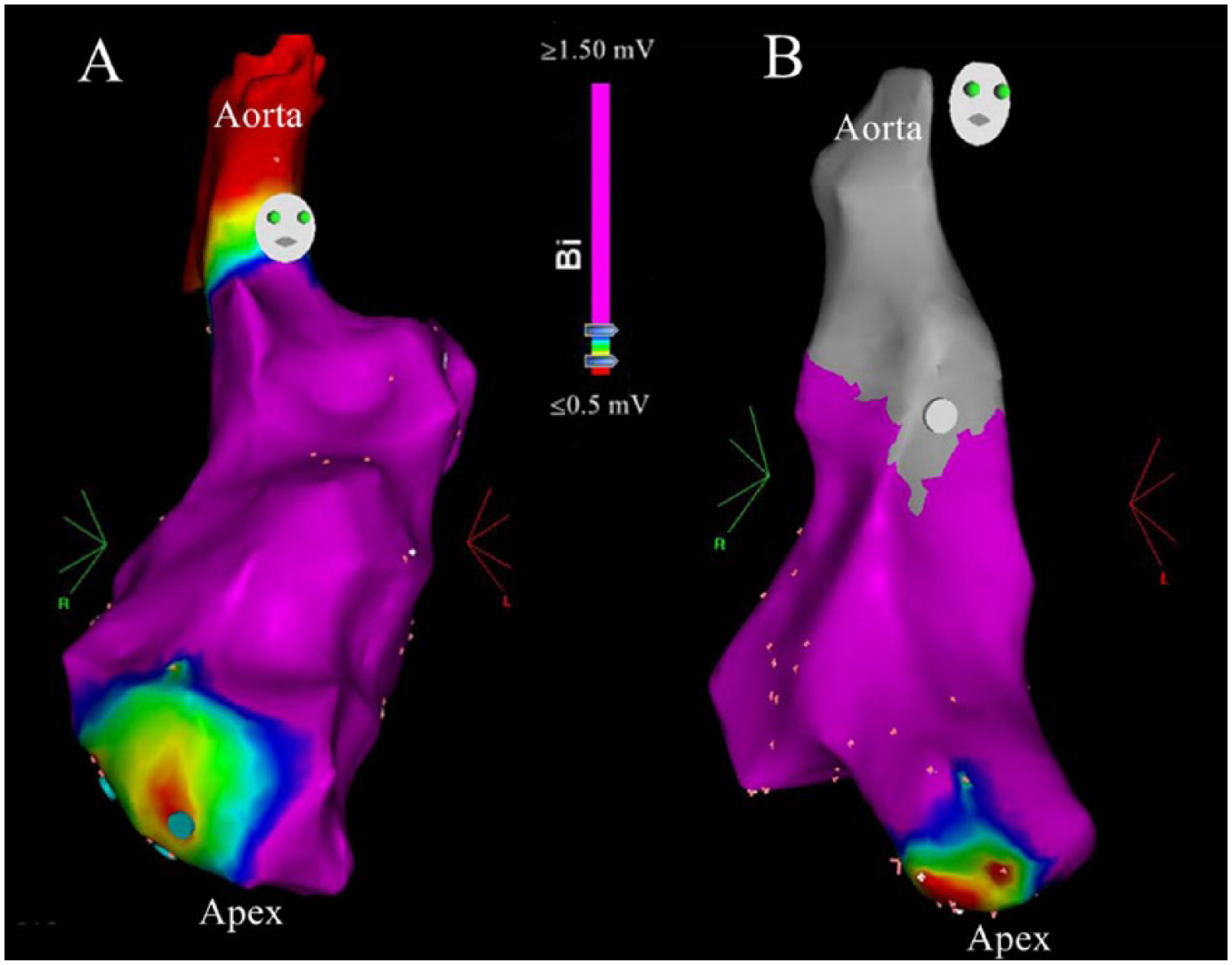
Endocardial substrate mapping of the LVA model via a transapical approach (A) and a transfemoral approach (B). Both approaches identified scars with BV criteria in which the red region indicates dense scars (BV⩽0.5 mV), the purple region indicates normal myocardium (BV⩾1.5 mV) and the colour range between red and purple indicates the border zones of scars (BV>0.5 mV and <1.5 mV). BV: bipolar voltage.
Discussion
The major findings of this study include: (1) the transapical access approach can be feasible for rendering a realistic 3D electroanatomic reconstruction of the endocardium of the LV and is comparable with traditional transvascular catheter mapping; (2) the endo-epicardial substrate mapping based on BV criteria under sinus rhythm can reliably localize the dense scar and border zone of the LVA; and (3) the substrate-guided endo-epicardial ablation during thoracotomy can be achieved easily for VT with LVA without scrupling the coronary artery or producing phrenic nerve injury.
VT is an adverse factor and causes more than 40% of sudden deaths in patients with LVA. 1 The relationship between VT and LVA after myocardial infarction (MI) has been noted since the 1930s. 22 In our study, VT was induced in the majority of pigs with LVA. The VTs were more frequently of the left bundle branch block type pattern. The reason may be the relatively rightward position of the porcine heart with standard ECG lead recordings. Remodelled LVAs after MI provide substrate for VT. Remodelling of the LVA that mainly involves the border zone of the LVA results in heterogeneous myocardial islands consisting of viable myocardial fibrosis and necrotic tissue in a staggered arrangement between dense scar and normal tissue. The structural remodelling provides a perfect milieu for forming the arrhythmogenic substrate. This arrhythmogenic substrate is characterized by slow conduction zones due to the conduction block corresponding with viable fibres embedded between areas of fibrosis.23,24 Furthermore, clinical data25,26 have provided convincing evidence that this arrhythmogenic substrate within the border zone of the scar is most likely three-dimensional, including endo-, mid- and epi-cardial myocardium.
The initial strategies of RFCA for VT involve identifying and ablating the critical isthmus of re-entrant circuits, using activation and entrainment mapping during VT.27,28 However, VT is characterized by non-inducibility, multiple morphology and haemodynamic instability in the majority of patients with LVA, limiting this approach.29,30 In addition, LVA often contains a large scar with impaired left ventricular function, further restricting utilization of this approach. In recent years, substrate-based mapping and ablation for VT after MI during sinus rhythm has been developed and the substrate-based approach in sinus rhythm was not inferior to mapping during VT for long-term VT ablation success. 31
Substrate-based mapping and ablation takes its origin from surgical VT therapy experience with endocardial scar resection. 32 In addition, the CARTO system can create a 3D BV map and characterize the electroanatomic substrate in more detail. This substrate mapping approach can be performed during normal sinus rhythm and reliably identify abnormal EGMs corresponding with VT substrate.33,34 This approach allows RFCA for VT with LVA irrespective of its inducibility, morphologies or haemodynamic tolerability.
RFCA has been proven to be superior to medical therapy for scar-related VT.35,36 However, VT recurrence after VT ablation remains high and the long-term success rates were only 55-60%.37–39 The complex anatomic structure of arrhythmogenic substrate and a limited endocardial ablation might be potential causes of poor prognosis. Considering the 3D nature of the arrhythmogenic substrate of LVA, the depth of ablative burns is an important factor for adequately modifying substrate of LVA. Therefore, an endo-epicardial ablation strategy is still required for VT with LVA.
Our study indicated that combined endo-epicardial RFCA was superior to endocardial RFCA in terms of improving acute ablation success (83.33% vs. 58.33%) and our previous study has also indicated that transmural linear ablation extending from the dense scar of LVA to the normal myocardium and across the border zone of LVA by bipolar radiofrequency device (AtriCure, Mason, OH, USA) could control VT with LVA 40 and both ablative strategies (endo-epicardial RFCA in this study versus transmural linear ablation in our previous study) gained similar acute ablation success rates (83.33% vs. 84.62%). Although endocardial catheter ablation via transvascular access is advocated as the first-line approach because of its minimally invasive nature, for VT with post-infarction LVA, the transapical ablative approach has its advantages and benefits. The benefits of this transapical access include: (1) shorter manipulation distance that is non-indispensable for fluoroscopic imaging, (2) less disturbance from mitral valve leaflets and papillary muscles and (3) contribution of detailed mapping at the border zone because the LVA is a paradoxical sac with distinct margins. The transapical technique is relatively simple to learn.
In addition, epicardial mapping and ablation under direct vision are easier to manipulate than a sub-xyphoid puncture approach. The region of LVA is distinguishable after heart exposure. It is important to note that poor catheter-tissue contact has a remarkable effect on the BV value. 41 Catheter-tissue contact is not assured by sub-xyphoid access, whereas visual epicardial mapping can be guaranteed with good catheter-tissue contact. Before epicardial ablation, coronary angiography and phrenic nerve capture are needless. The area of interest can be precise ablation irrespective of coronary artery and phrenic nerve damage.
In addition to VT ablation, CABG and LVA repair are necessary for most patients with post-infarction LVA, which not only relieves ischemia, but also restores left ventricular shape. 17 However, traditional CABG and LV aneurysmectomy with cardiopulmonary bypass can cause severe myocardial injury. Off-pump CABG and LVA repair without ventriculotomy are less invasive procedures with good outcomes. 42
Therefore, combined epicardial and transapical endocardial RFCA during off-pump CABG and LVA repair may be a promising method for post-infarction LVA with VT. On the one hand, RFCA aims at a VT substrate rather than the whole scar, reducing additional myocardial injury. On the other hand, this hybrid approach can accomplish multiple goals, including VT substrate modification, myocardial revascularization and LVA repair, with no need for stepwise intervention.
Limitations
At present, left anterior descending coronary artery balloon occlusion 16 as a closed-chest infarction procedure has been become mainstream and been proven effective for developing the AMI model. However, this model is a classic ischemia-reperfusion model that does not guarantee transmural MI. Transmural MI is the prerequisite to LVA. In this report, the AMI model was built by a minimally invasive permanent ligation of the coronary arteries, which insured transmural MI contributing to LVA formation. Although open chest procedures can cause surgical adhesions to a certain degree, the minimally lateral incision and only 6 weeks of healing had little effect on subsequent thoracotomy and epicardial mapping and ablation.
Furthermore, LVA was only located at the apex of the LV. Transapical endocardial mapping and ablation VT with LVA at other locations may be different. Such a simplified mapping and ablation may not be applicable to patchy scars with irregular shapes or scars resulting from non-transmural MI or non-ischaemic myocardiopathy. Since previous studies indicated endo-epicardial RFCA with improved transmural lesion, 9 the microscopic examination to observe transmural lesions was not conducted. Long-term efficacy of this combined ablation technique by follow-up should be verified in further studies.
Conclusion
These data showed that combined epicardial and transapical endocardial substrate-based mapping and ablation were feasible under thoracotomy. This experimental protocol appeared to provide enlightenment for future clinical studies incorporating endo-epicardial RFCA and off-pump CABG and LVA repair to treat patients with post-infarction LVA and VT.
Footnotes
Acknowledgements
The authors acknowledge Rong Bai for proof reading.
Author contributions
C.G. designed the study and revised the article. B.L., C.L., L.W., J.W., Y.H. carried out the study, including developing the model and the electropyhsiological study. C.L. and L.W. collected and analysed the data. B.L.wrote the article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China [Grant No. 81370436]