
Abstract
The correct selection and placement of a single-site Avalon® Elite Dual Lumen Cannula for veno-venous extracorporeal membrane oxygenation (ECMO) in children weighing less than 20 kg is dependent on both the mechanical characteristics of the catheter, including length and diameter, as well as the unique vascular anatomic considerations of the patient. This manuscript describes the development of a clinical strategy, over a four-year period from 2012-2016, for cannula selection to reduce the risk of migration and malposition in 20 critically ill children weighing less than 20 kg who presented for veno-venous ECMO.
Introduction
Veno-venous extracorporeal membrane oxygenation (VV ECMO) has been used to support more than 13,000 neonates and children with respiratory failure since 1989, with nearly 2,500 reported cases in the last 5 years alone.1,2 Extracorporeal membrane oxygenation (ECMO) cannulas are commonly selected based solely on a target flow rate as described by pressure drop versus flow curves supplied by the cannula manufacturer. Dual-lumen, single-catheter cannulation is the preferred modality for VV ECMO support in pediatric patients when compared with dual-site cannulation. 3 The Avalon Elite Dual Lumen Cannula (Maquet, Rastatt, Germany) is one dual-lumen cannula option and the cannula of choice at our center, though its use in pediatric patients is controversial. 4 Precise placement of the cannula is required to optimize the efficacy of VV ECMO support by maximizing oxygenated blood flow across the tricuspid valve and to ensure adequacy of venous drainage. Ideal placement of the cannula may be challenging due to the cannula length and variability in vessel anatomy in small children, specifically in the inferior vena cava (IVC).
Cannulation techniques, complications and the use of this cannula have been described in the literature, but anatomical considerations are not well documented.3,5–8 Some centers have abandoned the use of this cannula due to serious complications related to placement and migration. 9 The aim of this manuscript is to describe a single institution experience and insertion technique with this cannula, with specific attention to placement of the catheter tip in the IVC in children weighing less than 20 kg.
Cannulation technique
Measurements
A VV ECMO cannulation technique that includes vascular measurements was developed at our center after several patients less than 20 kg developed cannula malposition requiring intervention. Cannulation is performed in the catheterization laboratory by interventional cardiologists under fluoroscopic guidance. Cannulas are selected based on both patient weight and anatomical measurements. X-ray and, if necessary, trans-thoracic echocardiography (TTE) are used to measure the distance from the superior vena cava (SVC)/right atrial junction (RAJ) to the most proximal hepatic vein take-off (A), the SVC/RAJ to the mid tricuspid valve (B) and the mid tricuspid valve to the most proximal hepatic vein take-of (C) (Figure 1). Cannulas are selected by comparing the patient’s weight and anatomical measurements to manufacturer-supplied pressure versus flow curves for the cannula. A measurement table created by measuring distances on each size of the Avalon cannula (Table 1) is used to ensure both adequate flow and optimal cannula length to minimize the risk of cannula malposition. 10
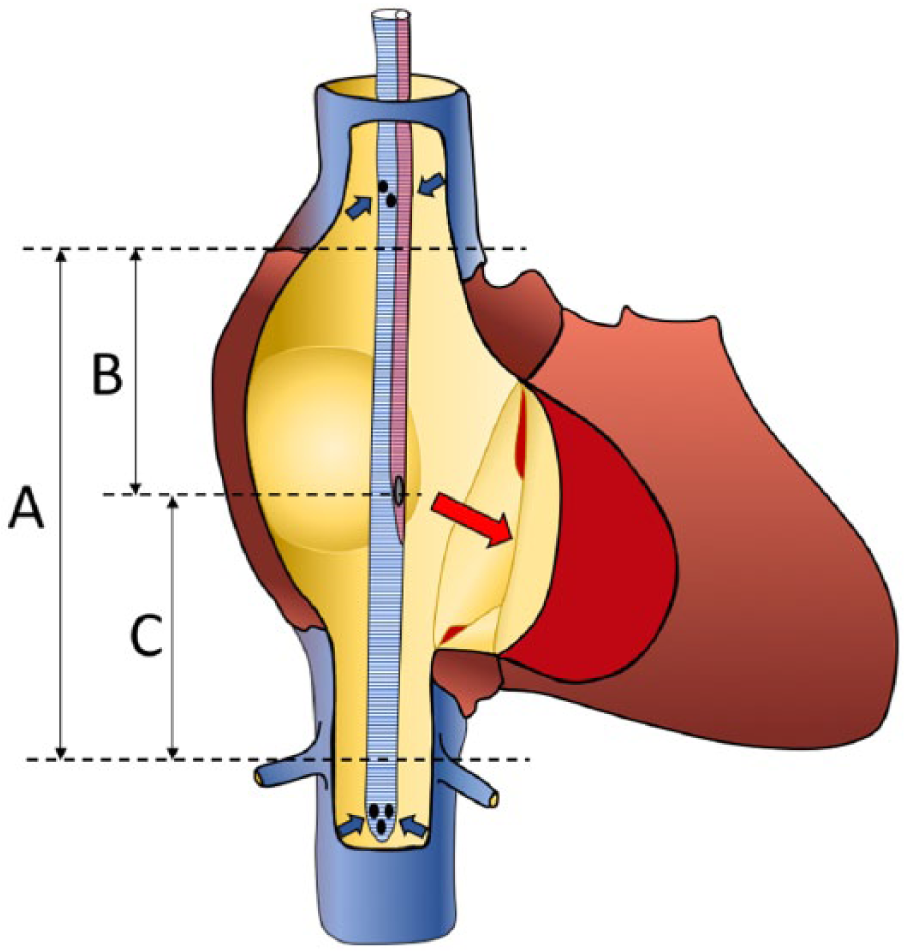
Anatomic Measurements for Cannula Insertion.
Avalon cannula measurement chart.
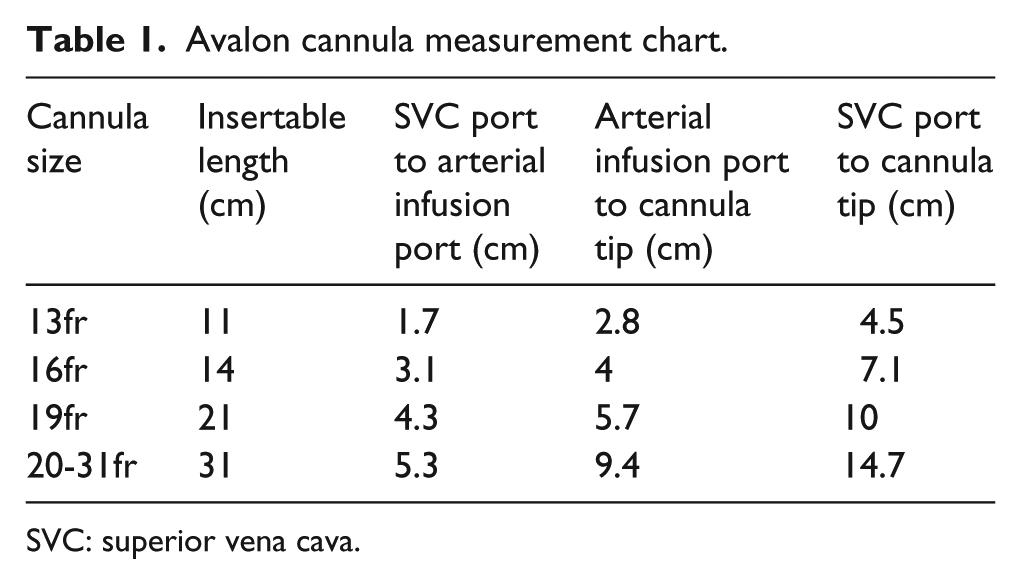
SVC: superior vena cava.
Insertion
Vascular access is obtained via the right internal jugular vein using a modified Seldinger technique. A guidewire is passed across the RAJ into the IVC through the access catheter. Fluoroscopy is used to verify the position of the guidewire and ensure the wire is not looped within the right ventricle. The patient is then heparinized with 50 international units/kg of heparin. The jugular vein is serially dilated, using vascular dilators, up to the size of the cannula. The cannula is inserted into the jugular vein and positioned across the RAJ with the distal tip of the cannula in the IVC distal to the hepatic veins using fluoroscopic guidance to verify position. The patient is then connected to the ECMO circuit and ECMO flow is initiated. Once ECMO flow is established, precise placement of the cannula is confirmed or adjusted using TTE to ensure the arterial flow is projected towards the tricuspid valve and the distal cannula tip remains unchanged relative to the hepatic veins. The cannula is secured by suturing to the skin of the patient to minimize the risk of cannula migration.
Study methods
A retrospective review of 20 patients weighing less than 20 kg cannulated with an Avalon cannula for VV ECMO between January 2012 and December 2016 was conducted. Institutional Review Board approval was obtained. Data, including age, weight, height, cannula size and cannula malposition complications were collected from EPIC© (Epic Systems Corporation, Verona, WI). Measurement data were collected by retrospective review of the TTEs performed near the time of ECMO cannulation (Table 2). Statistical analyses were performed in Prism (version 7; GraphPad Software, La Jolla, CA, USA). All values are reported as means with standard deviation or median with corresponding inter-quantile range as dictated by the distribution of the considered variable. The analysis of variances in echocardiographic measurements were compared using Bartlett’s test.
Retrospective review of patients weighing less than 20 kg cannulated with an Avalon cannula for VV ECMO over a four-year period.
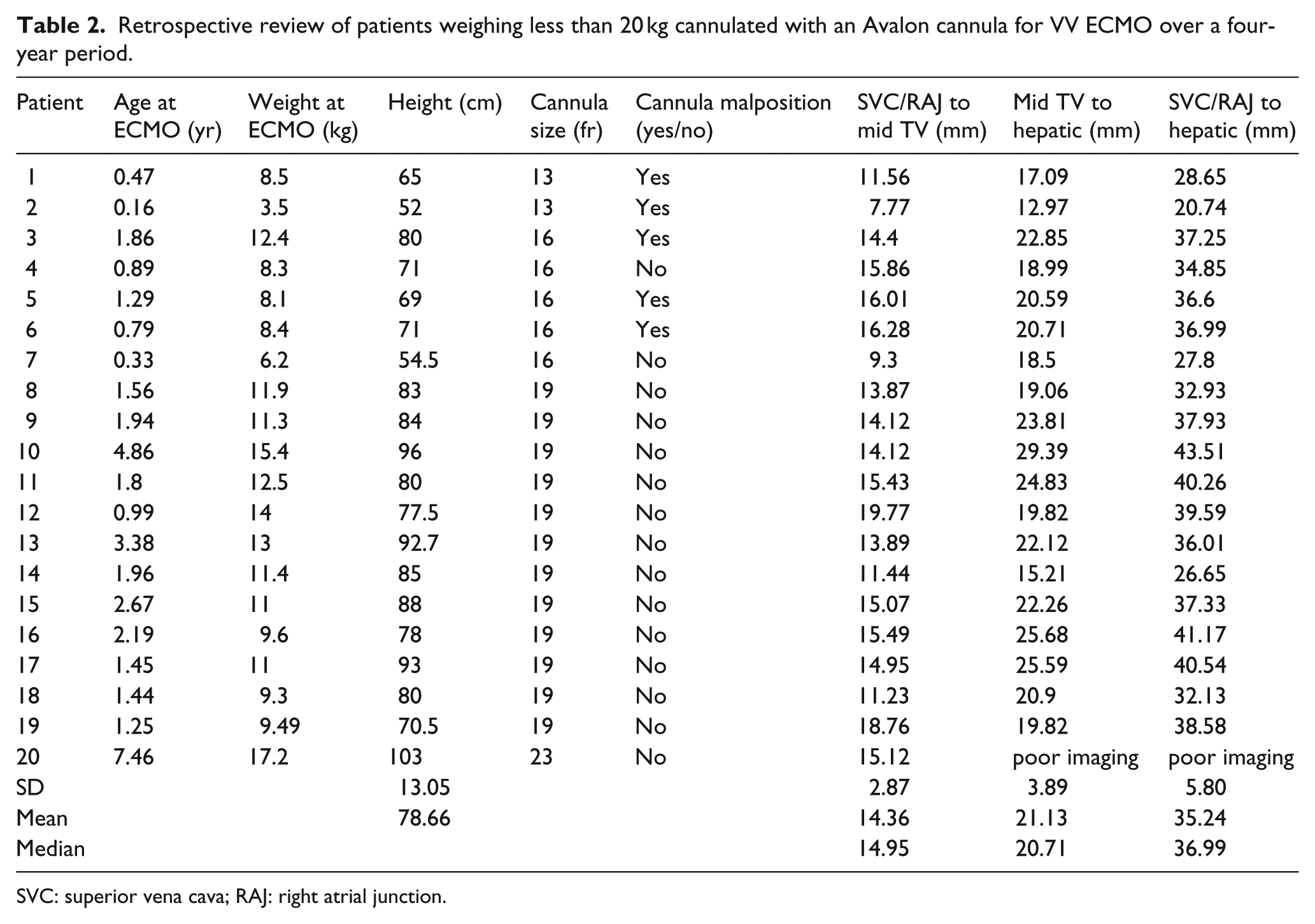
SVC: superior vena cava; RAJ: right atrial junction.
Results
Between January 2012 and December 2016, 20 patients, mean ± standard deviation (1.9 ± 1.7 years) weighing less than 20 kg (10.6 ± 3.15 kg) with height (78.6 ± 13.0 cm), were supported with VV ECMO. Distribution of the individual echocardiographic measurements with variance analysis is depicted in Figure 2. There was minimal inter-patient variability in the SVC/RAJ to mid tricuspid valve distance (14.36 ± 2.87 mm). There was greater anatomical inter-patient variability in the distance from the mid tricuspid valve to the most proximal hepatic vein take-off in children under 20 kg (21.1 ± 3.9 mm). The greatest inter-patient variability existed in the SVC/RAJ to hepatic vein take-off (35.24 ± 5.8 mm). One patient was excluded from the analysis of variances for sub-optimal imaging window. There was a significant difference between variances for the aforementioned measurements with Bartlett’s test, p=0.017. Notably, one patient had no image of the first hepatic vessel captured during TTE.
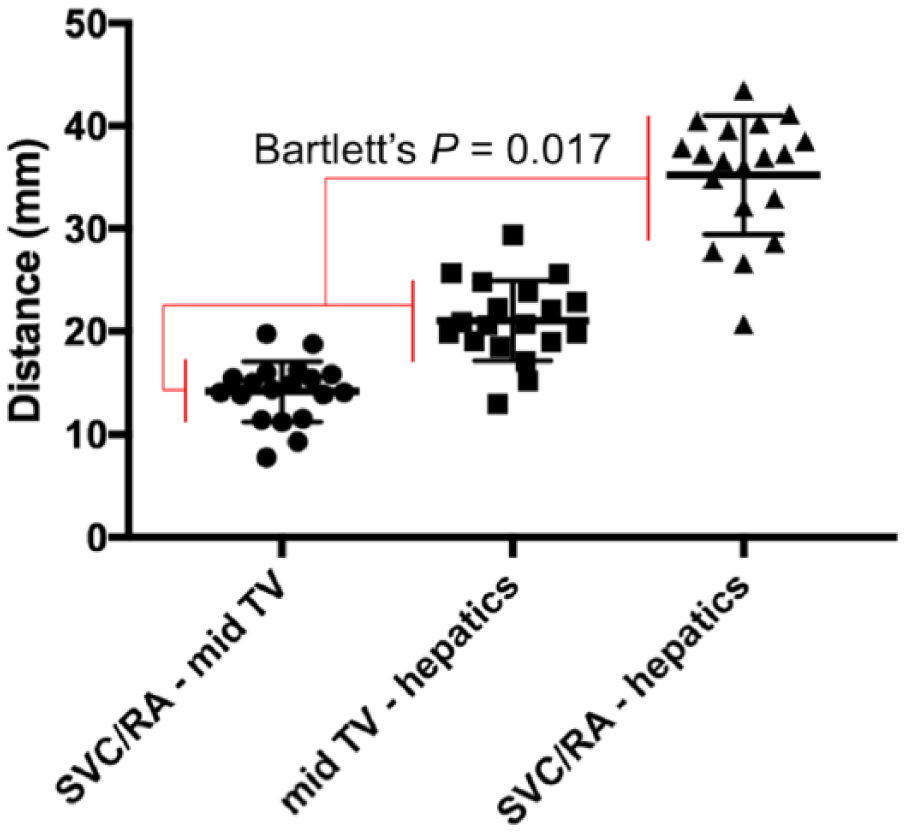
Echocardiographic Measurement Analysis of Variance.
Discussion
For patients with refractory respiratory failure, ECMO may be lifesaving. VV ECMO, previously undertaken via dual-site cannulation of the internal jugular and femoral veins, has been supplanted by modern dual-lumen catheters. When using these catheters, positioning of the oxygenated flow jet across the tricuspid valve is critical to success of VV ECMO support. 11 Though successfully and broadly adopted, use of an Avalon cannula in VV ECMO comes with some intrinsic challenges. In order to maximize ECMO pump efficiency and minimize the potential for recirculation, the outflow jet is precisely placed in relation to the tricuspid valve. When the outflow is accurately positioned in relation to the tricuspid valve, the distal tip of the cannula may be sub-optimally positioned. In this cohort, it was found that the distal tip may reside near the junction of the IVC and the right atrium or near the hepatic veins, depending on the variable vessel anatomy of individual patients. Malposition of the cannula may lead to serious complications. Currently, there are several reports describing life-threatening complications, including atrial perforation leading to pericardial tamponade or erosion of the atriocaval wall, occurring both at the time of placement and in subsequent days.6,12,13 A 2015 study by Speggiorin and colleagues included 79 neonates undergoing VV ECMO with the Avalon cannula where five serious events occurred requiring sternotomy, leading that study center to abandon the Avalon dual-lumen cannula in favor of VA ECMO. 6 Johnson and colleagues changed their practice by placing the cannula more distally into the IVC to decrease the risk of displacement into the atrium. 5 At least one group has recommended design modifications to the cannula, supported by the experience presented in this retrospective review, suggesting that lengthening the inferior pole of the cannula may reduce rates of cannula malposition and right atrial perforation. 14 The two most common cannula sizes in this cohort were the 16 and 19 Fr. The 19 Fr cannula is approximately 30% longer in all relevant measurements when compared with the 16 Fr, including insertable length (21 and 14 cm), SVC to arterial infusion port (4.3 and 3.1 cm), arterial infusion port to cannula tip (5.7 and 4 cm) and SVC port to cannula tip (10 and 7.1 cm) (Table 1). In patients greater than 20 kg, a cannula size of 20-31 Fr is usually selected. In these longer cannulas, the SVC port to cannula distal tip distance is 14.7 cm or approximately 50% longer than the 19 Fr cannula. Therefore, in bigger patients, distal tip hepatic vein cannula migration or malposition does not occur as frequently as it does in patients weighing less than 20 kg.
During the study period, no serious complications, including perforation or vascular erosion with the use of the Avalon cannula, were reported. However, prior to adding routine measurement of right atrial anatomy to the cannula selection criteria, cannula malposition was common. The most common type of cannula malposition was the migration of the distal cannula tip into an hepatic vein, which occurred in a quarter of the patients early on in the series. Hepatic vein malposition limited venous return to the ECMO circuit and resulted in sub-optimal ECMO support, requiring intervention and repositioning. Imaging studies during insertion of veno-venous ECMO cannulas have been previously recommended in adults. 15 Since implementing the anatomical mapping strategy prior to cannula selection in 2013, as described in this manuscript, there has been no hepatic vein cannula malposition when using the optimal Avalon cannula in children less than 20 kg.
Conclusion
The Avalon cannula is a viable clinical option for VV ECMO support in patients under 20 kg. Patient vessel anatomy should be considered in addition to patient weight when selecting an Avalon cannula for VV ECMO support. Imaging studies are recommended to measure the distances from the SVC/RAJ to the mid tricuspid valve and the mid tricuspid valve to the most proximal hepatic vein take-off prior to cannula selection. Larger cannulas than would be required based on patient weight alone are sometimes necessary to ensure the distal tip is positioned well into the IVC and below the take-off of the hepatic veins. Future studies are needed to describe the anatomical variability between the tricuspid valve and the most proximal hepatic vein take-off in patients weighing less than 20 kg.
Limitations to our study include those typical for single-center, retrospective reviews. Due to the nature of the review, results may not be generalizable to other institutions. Imaging data were collected retrospectively and measured in fractions of millimeters, which may be inaccurate. An image of the first hepatic vessel was not captured for one patient in our review.