
Abstract
Objective:
The aim of our study was to explore long-term health-related quality of life (HRQOL) and incidence of post-traumatic stress disorder (PTSD) in extracorporeal membrane oxygenation (ECMO) survivors.
Methods:
Single-center prospective follow-up study. All patients in whom ECMO was initiated due to refractory cardiogenic shock between 2009 and 2014 were included in the study. We used Medical Outcomes Study 36-Item Short-Form Health Survey to evaluate HRQOL and IES-R questionnaire to assess incidence of PTSD.
Results:
Sixty-nine patients were treated with venoarterial (VA) ECMO during the study period. Nineteen patients survived until hospital discharge and 15 patients were alive at the study cut-off point in June 2017; mean follow-up time was 70.6 ± 10 months. The average Physical Component Summary and Mental Component Summary scores amongst long-term survivors were 46.1 ± 7 and 47.1 ± 8, respectively. PTSD was evident in 4 out of 15 participants.
Conclusions:
Despite the complex clinical course and prolonged recovery, ECMO survivors achieved satisfactory levels of both mental and physical recovery, which were comparable to the age- and pathology-adjusted population means.
Keywords
Introduction
Improvements in technology and patient management have resulted in the increasing use of extracorporeal membrane oxygenation (ECMO) as a salvage therapy in critically ill adults.1,2 Despite favorable early survival rates, long-term sequelae of ECMO survivors remains questionable. 3 Even less evidence is available regarding the clinical outcomes of patients discharged from hospital after experiencing multiple interventions: cardiac surgery, refractory cardiogenic shock and extracorporeal life support (ECLS) therapy. Whilst veno-arterial extracorporeal membrane oxygenation (VA ECMO) is a life-saving procedure, it may result in life-threatening vascular and neurologic complications or massive bleeding.4,5 Apart from numerous potential complications, postoperative outcomes may also be affected by irreversible factors, such as pre-admission co-morbidities or the patient’s age.5,6 Incorporating economic considerations into clinical decisions is ethically difficult; however, we should be aware of the costs and outcomes of advanced critical care illness treatments. Over the last few decades, it has become clear that intensive care survivors suffer devastating after-effects, known as the post-intensive care syndrome and defined as ‘new’ or ‘worsening’ impairment in physical, cognitive or mental health status arising after hospitalization for critical illness and, in some cases, persisting for years after the discharge. 7 As such, quantifying self-perceived outcomes might be beneficial in identifying those patients who are prone to developing long-term disabilities and are likely to require high utilization of healthcare services. Health-related quality of life (HRQOL) is a multi-dimensional construct which provides a more complex evaluation of post-procedural well-being. However, recent reports on long-term self-reported well-being after critical illness are conflicting. On the one hand, patients who survive critical illness experience long-term deficits in both physical and cognitive performance.8,9 On the other hand, few studies demonstrate favorable physical and social functioning in ECMO survivors in comparison to patients suffering from chronic medical conditions. 10 Conclusive evidence supporting favorable long-term outcomes of ECMO survivors is, therefore, missing. Our aims are to: 1) evaluate long-term self-reported health-related quality of life (HRQOL) and the level of post-traumatic stress disorder (PTSD) following extracorporeal membrane oxygenation (ECMO) in patients after cardiac surgery and 2) compare HRQOL of ECMO survivors with a cohort of intensive care unit survivors from the same institution, followed up after non-complicated cardiac surgery.
Methods
Our study was approved by the Vilnius Regional Bioethics Committee (Lithuania), reference number 158200-16-850-259. All patients signed the informed consent for retrospective collection of data and prospective assessment of post-procedural outcomes. Our study was conducted in a tertiary referral hospital and included adult patients who received post-cardiotomy ECMO support from 2009 to 2014. Information on patients’ demographic variables, pre-existing co-morbidities and perioperative data was collected retrospectively from medical records.
Cardiac surgery and institution of ECMO
All cardiac surgery procedures were performed via a median sternotomy. Decisions to proceed to ECMO were made in cases of unsuccessful weaning from cardiopulmonary bypass despite maximal inotropic and intra-aortic balloon pump support (or both) and in cases of progressively worsening cardiogenic shock with a cardiac index of less than 1.5 L/min/m2. Weaning from ECMO was based on clinical and investigative evidence of cardiac function. All patients were transferred to intensive care postoperatively and discharged from the intensive care unit (ICU) when they no longer required inotropic or other organ support.
Post-procedural recovery was evaluated via postal and semi-structured telephone surveys. Health-related Quality of Life (HRQOL) was assessed using the Short-Form-Health version 2 (SF-36v2) quality of life questionnaire – a certified Lithuanian version.
The SF-36v2 consists of 8 sub-scales which cover the physical, mental and social life of each individual. They look at Physical functioning (PF); Role physical (RP); Role emotional (RE); Social functioning (SF); Bodily pain (BP); Mental health (MH); Vitality (VT) and General health (GH). The Physical Component Summary (PCS) and the Mental Component Summary (MCS) scores were calculated from SF-36v2 sub-scales to show a patient’s overall physical and mental health status. 11 Mean scores of less than 47 indicated a below-average health status and the survey has been widely used in ICU patients. All SF-36v2 data was converted and calculated using the Health Outcomes Scoring Software 4.5.1 and compared with data from the 2009 Quality Metric standard population. Mean SF 36 scores were compared with population normative values and post-cardiac surgery survivors’ data. 12
Post-traumatic stress disorder was assessed using the IES-R scale. The IES-R consists of 22 questions that cover the 3 PTSD diagnostic clusters: intrusion, avoidance and hyper-arousal. 13 Respondents used a 5-point scale to indicate their levels of distress in relation to specific events (e.g., ECMO treatment and ICU stay); scores ranged from 0 (not at all distressed) to 4 (extremely distressed). Summary scores of 33 or greater indicated a high risk of PTSD in intensive care survivors. HRQOL data in the ECMO cohort was compared with previously published data on long-term outcomes in patients who experienced elective cardiac surgery with cardiopulmonary bypass and non-operated patients with coronary artery disease in an age-matched Lithuanian population.12,14
Statistical analysis
Summary data were expressed as the number of patients and percentages; normally distributed data were reported as means and standard deviations and non-normal data were reported as medians and interquartile ranges. The Shapiro-Wilk test was used to assess the distribution of the data. The analysis of variance (ANOVA) and the independent samples t-test were used to compare means amongst the groups – p-value of <0.05 was considered statistically significant.
Results
Between 2009 and 2014, 69 salvage VA ECMO procedures were performed in 5641 consecutive cardiac surgical patients (1.2% of all operated patients). The preoperative demographics and perioperative data are shown in Table 1. Nineteen of the 69 patients survived until hospital discharge and 15 patients alive at the cut-off date of June 2017 were included in the final analysis (Figure 1). The mean follow-up of the cohort was 70.6 ± 10 months.
Baseline characteristics and perioperative data of ECMO survivors at follow-up.
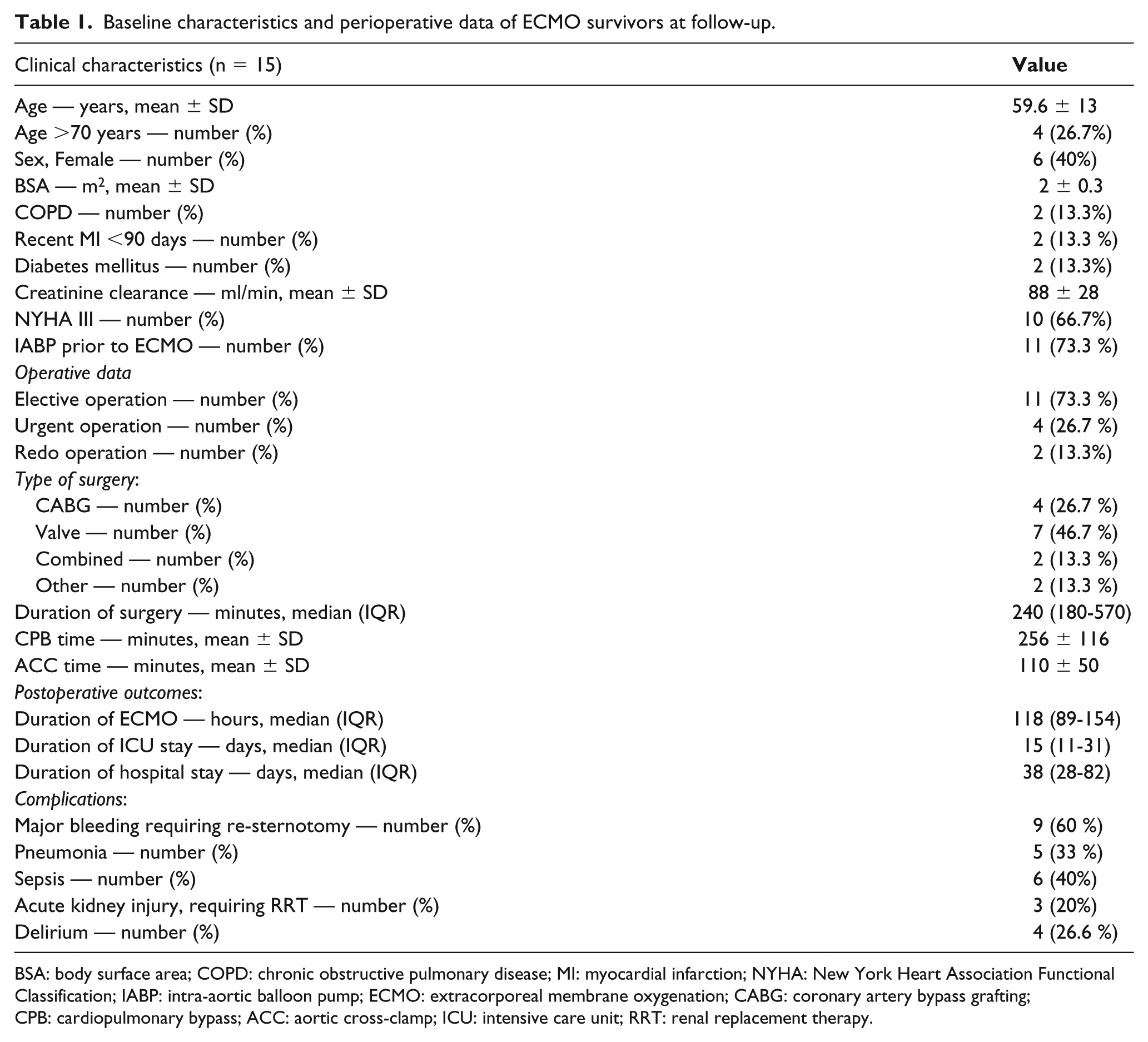
BSA: body surface area; COPD: chronic obstructive pulmonary disease; MI: myocardial infarction; NYHA: New York Heart Association Functional Classification; IABP: intra-aortic balloon pump; ECMO: extracorporeal membrane oxygenation; CABG: coronary artery bypass grafting; CPB: cardiopulmonary bypass; ACC: aortic cross-clamp; ICU: intensive care unit; RRT: renal replacement therapy.
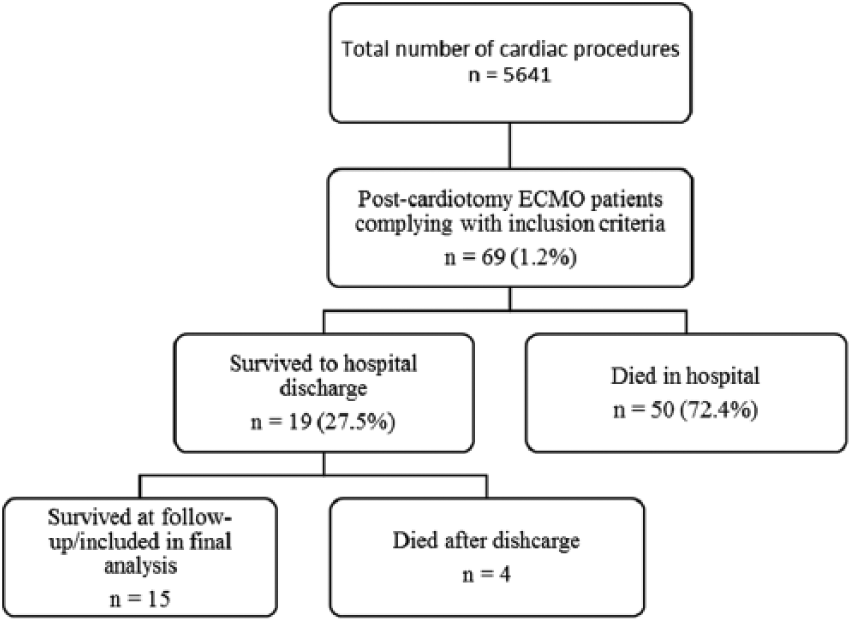
Flowchart of patients included in the study. ECMO - extracorporeal membrane oxygenation.
Of the 15 study patients, ten were classified as New York Heart Association (NYHA) functional class III/IV. The mean left ventricular ejection fraction for the study group was 48.9 ± 9. Surgical procedures were distributed as follows: coronary artery bypass grafting (CABG) four, valve seven, combined valve and CABG two, one patient underwent pulmonary artery thrombectomy and one received ECMO therapy after a heart transplant. Fourteen patients had a perioperative intra-aortic balloon pump (IABP) inserted as an attempt to wean from cardiopulmonary bypass (CPB) and were then initiated on VA ECMO. The median duration of ECMO was 118 (89-154) hours. Major hemorrhage, followed by re-sternotomy, developed in nine patients. Distribution of other postoperative complications are presented in Table 1. IES-R summary scores indicative of PTSD were evident in four participants.
Health Survey
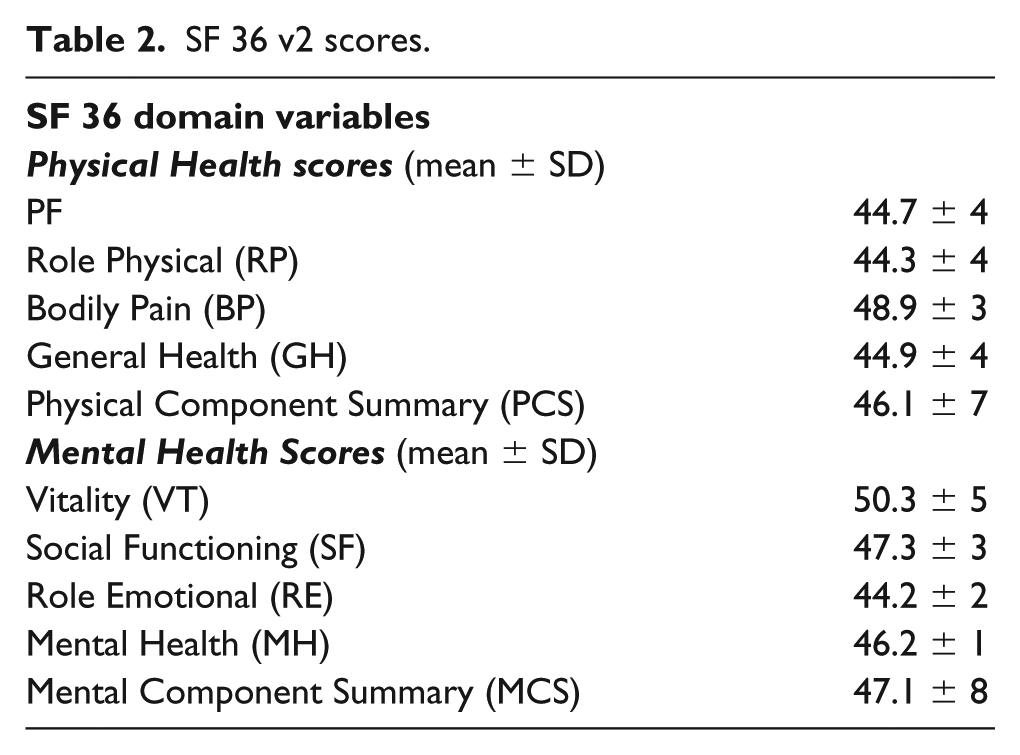
Mean values of SF-36 physical component scores and the sub-scales for physical function, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health domains are presented in Table 2.
SF 36 v2 scores.
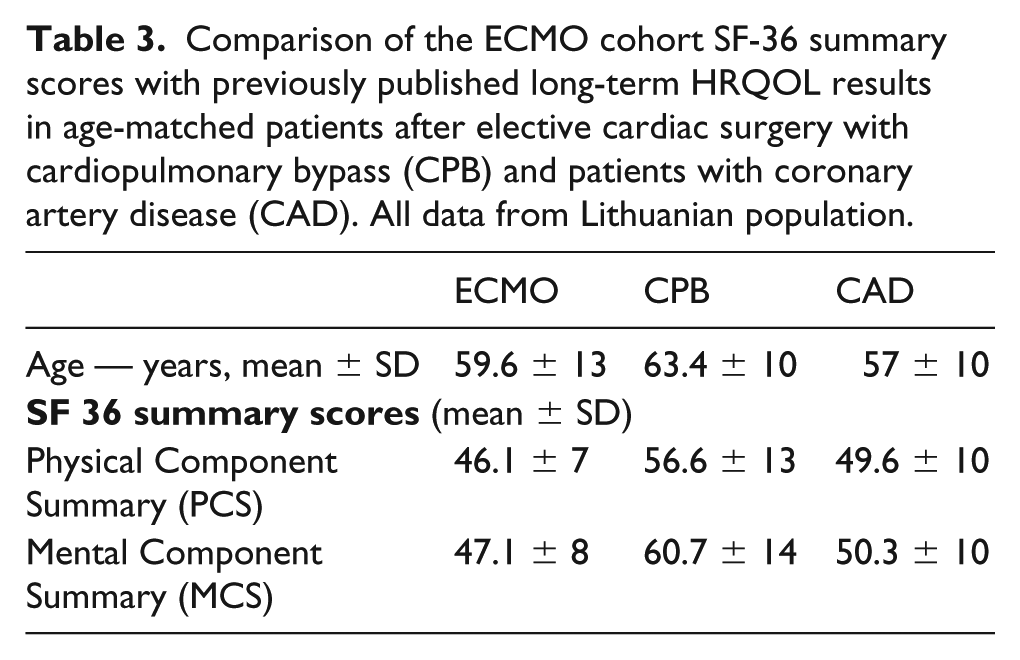
We have also compared HRQOL data in this ECMO cohort with long-term outcomes in patients after elective cardiac surgery with cardiopulmonary bypass (CPB, n=210) and non-operated patients with coronary artery disease (CAD, n=1072) in an age-matched Lithuanian population (p<0.05 for age in the ECMO group compared to the CPB and CAD groups) (Table 3). There was no difference between ECMO survivors and patients with CAD (p>0.05 for both PCS and MCS scores). Patients following elective cardiac surgery had better HRQOL than ECMO and CAD cohorts (p<0.01 for both PCS and MCS).
Comparison of the ECMO cohort SF-36 summary scores with previously published long-term HRQOL results in age-matched patients after elective cardiac surgery with cardiopulmonary bypass (CPB) and patients with coronary artery disease (CAD). All data from Lithuanian population.
Discussion
ECMO is expensive and one of the most invasive of treatments, with a relatively high percentage of serious and well-recognized complications. The undertaking of such a treatment should be based on a very clear assessment of risks and benefits and with a clear understanding of the potential outcomes. While there is a significant pool of evidence on survival and short-term outcomes, data on long-term outcomes after extracorporeal life support remains contradictory.3,15 In our research group, the out-of-hospital discharge rate was 27.5%, which is comparable to other studies that demonstrate out-of-hospital discharge rates ranging from 24-54% in postcardiotomy ECMO patients.4,15,16 Our long-term survival rate of 21.7% is also similar to other authors’ findings.16,17 One of the largest postcardiotomy ECMO cohorts of 517 patients, published by Rastan and colleagues, demonstrates that only 13.7% of postcardiotomy ECMO patients survive five years after hospital discharge. 17 Such low survival rates raise the question of who is the best candidate for extracorporeal life support. It also shows that any medical interventions should be patient-centered and, therefore, long-term health-related quality of life should become one of the leading factors in our decision making. However, defining quality of life is challenging and subjective – any perceptions of well-being include a consideration of both basic human needs and life satisfaction more generally. Health-related quality of life assessments cover physical, mental and social aspects of health (as set out by the World Health Organization), yet opinion on QOL is personal and what an observer might consider a dismal level of QOL may be acceptable to the individual.
ECMO is inevitably accompanied by prolonged ICU and hospital stay, associated complications, slow recovery and, as recent studies suggest, an impact on long-term mental health. ECMO survivors not only experience clinical risk factors for adverse health outcomes similar to the risk factors of other ICU patients, but also have some unique risk factors for adverse health outcomes and delayed recovery. Comparisons with long-term acute respiratory distress syndrome (ARDS) survivors revealed that those who were supported by ECMO for refractory hypoxemia had similar physical health, but decreased mental health, general health, vitality and social function compared to other ARDS survivors. 3 However, our cohort data demonstrates that ECMO survivors have comparable HRQOL to patients with coronary artery disease and those following major cardiac surgery. SF-36 scores in our study were marginally lower than short- and mid-term outcomes reported by Wang and colleagues. 15 Interpretation of this difference is complicated by different follow-up periods and the fact that the mean age in our cohort was ten years older. The multi-center ENCOURAGE trial in France analyzed long-term outcomes in 69 rescue VA ECMO patients. 6 PCS and MCS scores in our study were very close to those published (46 v 50 and 47 v 50, respectively), suggesting that long-term outcomes are ECMO-specific and less influenced by geographical or healthcare system factors.
Incidence of post-traumatic stress disorder in our study was relatively high at 28.5%. However, a recent systematic review by Ratzer and colleagues demonstrated PTSD incidence in the general ICU population to be up to 52%, with a mean point prevalence of 19.7% for questionnaire-based studies. 18 Although controversial, there is some evidence that ICU length of stay, duration of ventilation and disease severity may contribute to a higher incidence of PTSD. It would be speculative to apply this evidence directly to the ECMO population, but many of the same risk factors are common in both groups.
Limitations of the study
A major limitation of this study is the small number of patients included. Procedural data was reviewed retrospectively and the follow-up periods for quality of life assessments were variable. Due to the complex nature of telephone interviews, we were unable to acquire additional information on possible confounding factors contributing to a decrease in self-perceived quality of life, especially considering the long follow-up intervals. Further prospective research is needed to clarify whether a complicated postoperative course determines long-term self-perceived quality of life.
Conclusion
Despite the complex clinical course and prolonged recovery, ECMO survivors achieved satisfactory levels of both mental and physical recovery, which were comparable to the age- and pathology-adjusted population means.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.