
Abstract
Background:
This study evaluated pregnancy outcome in women with a prosthetic heart valve, especially with the oral anticoagulation therapy that must be weighed against the risk of intracardiac thrombosis.
Methods:
This multicenter, retrospective, cohort study was undertaken between January 2012 and June 2017. The principal maternal outcome variables included bleeding and thromboembolic complications, infective endocarditis, prosthetic valve thrombosis and heart failure. However, the main foetal outcome variables included miscarriage, mortality, preterm baby, warfarin embryopathy, low birthweight and the mode of delivery.
Results:
A total of 265 pregnancies in women with prosthetic heart valves were evaluated in two groups: Group I (n = 182) covers a mechanical valve, while Group II (n = 82) covers a bioprosthetic valve. The mean age of the patients was 25.2 ± 2.5 years and 24.5 ± 5.2 years in Group I and Group II, respectively. Approximately 80% of the patients had normal echocardiography findings. However, Group I (mechanical prostheses) has a higher incidence (11.54%) of thrombus formation in comparison with the bioprostheses. Hemorrhagic complications and spontaneous miscarriage were statistically significant (p⩽0.05) between the study groups. However, normal pregnancy outcome (91.57%) was significantly higher (p⩽0.05) in Group II compared to Group I (61.54%). Mean birthweight and mean APGAR score were found normal in both study groups. Only 2.75% of patients have warfarin embryopathy in Group I. Furthermore, comparison of SF-36 scores for HRQOL (Health-Related Quality of Life) before and after pregnancy were statistically insignificant among the study population.
Conclusion:
Proper antenatal care and early risk stratification are the fundamental measures to improve the maternal and foetal outcomes in a patient with a prosthetic heart valve.
Keywords
Introduction
Cardiac diseases are the primary cause of non-obstetric mortality in pregnancy and approximately 1%-4% of pregnant women suffer from concomitant heart diseases, especially mitral valve pathology. 1 At present, post-operative care and prognosis following open heart surgery have improved significantly, but women are still afraid of having babies when they have a prosthetic heart valve. 2 However, professional experience demonstrates that, if properly managed, outcomes of pregnancies after open heart surgery are encouraging. Nevertheless, there is no doubt that these women require vigilant care for their mental and physical well-being during pregnancies for having positive outcomes.2,3
Physiological changes during pregnancy include a gradual increase in cardiac output, blood volume, heart rate and myocardial oxygen consumption, all of which may cause decompensation in women with underlying cardiac disease. The haemodynamic changes of pregnancy put an extra-circulatory burden on the heart, which increases during labour and immediately following delivery. 3 Moreover, women who undergo heart valve replacement with mechanical prostheses have a lower risk of cardiac dysfunctions in comparison to those with biological prostheses. 4 During pregnancy, there are increased platelet numbers and activation of coagulation cascades, but fibrinolytic activity is decreased. These changes increase the risk of prosthetic valve thrombosis, which may necessitate emergency surgical re-intervention, with a high incidence of maternal and foetal morbidity and mortality. 5
The management of a pregnant woman with a prosthetic heart valve requires important considerations, especially with the maintenance of proper anticoagulation therapy and coagulation profile. Warfarin is considered to be a safe and effective anticoagulant for patients with prosthetic heart valves.3–5 However, treatment with warfarin poses many difficulties, specifically during the first trimester of pregnancy, due to its ability to cross the placenta, with associated foetotoxicity. 6 Furthermore, treatment with heparin during the first trimester of pregnancy reduces the risk of embryopathy, but increases maternal morbidity and mortality.5–7 The risk of thromboembolism, miscarriage and premature birth is felt to be higher in patients who have prosthetic heart valves requiring anticoagulation therapy. 7 The most common complications during pregnancies with a prosthesis are: arrhythmias, thrombosis of the prostheses, hypercoagulability, risk of thromboembolism, abortion, premature delivery, intrauterine foetal death or intrauterine growth retardation, etc.6–8 Thus, pregnancy with a prosthetic heart valve is still problematic and troublesome, but, surprisingly, most patients can tolerate the stress of normal vaginal delivery.3,8–10 This study evaluated the effects of the prosthesis on pregnancy outcome and management protocol of pregnant women, especially with anticoagulation therapy, in our country.
Methods
This multicenter, retrospective, cohort study was undertaken between January 2012 and June 2017 in the Department of Cardiac Surgery, at Bangabandhu Sheikh Mujib Medical University (BSMMU), National Institute of Cardiovascular Diseases (NICVD) and Al Helal Specialized Hospital, Bangladesh. A total of 265 pregnancies in women with prosthetic heart valves were evaluated and divided into two groups: Group I (n = 182) comprises pregnancies with a St. Jude Medical™ mechanical heart valve, while Group II (n = 83) comprises pregnancies with a St. Jude Medical™ tissue valve. Prior to commencement of this study, permission was taken from the appropriate departmental academic and technical committee (Institutional Review Board) in order to undertake the study. An informed written consent was taken from each of the patients and a standardized semi-structured data collection sheet was used to collect the necessary information of the study subject.
Moreover, an SF-36 questionnaire was obtained from all study patients and an assessment with an HRQOL questionnaire was performed before and after pregnancy, using the SF-36 score. There were 8 domains in the SF-36 questionnaire which cover the social, physical and mental life of each individual and were applied to assess the health-related quality for the study populations. These domains are Role physical, Physical functioning, Social functioning, Role emotional, Mental health, Bodily pain, Vitality and General health. For each domain, all the answers were then transformed to a scale of 0-100, where zero is worst and 100 is the best health status. Moreover, for interpreting the SF-36 questionnaire, a standardized technique was used and data was collected from authorized medical evidence before, during and after pregnancy. All data was collected during follow-up by interviewing the patient at a follow-up clinic.
Pregnant women (age ⩽35 years) with prosthetic heart valves fulfilling the selection criteria were enrolled in the study. However, pregnancy with concomitant other cardiac diseases, such as congenital heart defect, coronary artery disease, hypertension, poor LV function, renal impairment, hepatic dysfunction, diabetes and poor NYHA class ⩾3 was excluded from this study. Categorical variables are presented in the form of frequency and percentage and quantitative data is presented in the form of mean and standard deviation. The results are presented in tables. The Chi-square test was used to analyse the categorical variables, shown with cross-tabulation. Student’s t-test and the Unpaired t-test were utilised for continuous variables to test the statistical difference. P-values ⩽0.05 were considered as statistically significant.
Follow-up procedure
The details of the cardiac lesion and surgical procedure were recorded in all cases and pregnant women were treated under the joint care of obstetricians and cardiac surgeons. At the first follow-up visit, evaluation of health status was performed, especially cardiac function, then their subsequent visit schedule was arranged according to the necessity of each case. After the first visit, a follow-up schedule was planned at 3 months, 6 months, 9 months and according to the necessity of each case during pregnancy. Echocardiography, ultrasound of pregnancy profile, serology and coagulation profile were performed at the first visit and when indicated. At 18-20 week of gestation, an ultrasound scan was done for the detection of any foetal abnormalities. After 36 weeks of gestation, all pregnant women were advised for hospitalization and spontaneous normal delivery was anticipated unless there were any obstetric indications. In other cases, an elective caesarean section was done. After birth, babies were examined by pediatricians and the weight, APGAR (Appearance, Pulse, Grimace, Activity, Respiration) score and signs of any congenital anomalies were recorded on a data collection sheet.
Anticoagulation therapy
Patients taking anticoagulants should continue their treatment according to their prescription throughout their pregnancies. Heparin was administered in the first trimester (Dose: 5000 IU subcutaneously 12 hourly), thereafter oral warfarin therapy was continued until 2 weeks prior to the expected date of delivery (EDD), according to the standard dose adjusted by monitoring of the international normalization ratio (INR) level and, then, heparin started again until the commencement of delivery. The coagulation profile was monitored by measuring the activated partial thromboplastin time (aPTT) for heparin and prothrombin time (PT) with an INR for warfarin therapy at a regular interval of time. Moreover, the doses of anticoagulants were adjusted according to the type and position of the cardiac valve. Anticoagulation therapy was stopped before delivery and resumed after 6-12 hours following delivery. Other cardiac medications, such as digoxin, beta blockers or diuretics, were adjusted accordingly.
Results
This study evaluated 265 pregnancies in women with prosthetic heart valves, either mechanical or bioprosthesis. The baseline characteristics of the study population are given in the Table 1. The mean age was 25.2 ± 2.5 years in Group I and 24.5 ± 5.2 years in Group II. The majority of the patients were housewives and approximately 50% of the study patients in both Group I and Group II had completed higher secondary education. Table 2 demonstrates that only 7.14% and 7.23% of the patients were found to have atrial fibrillation in Group I and Group II, respectively. The occurrence of heart failure, endocarditis and eclampsia was statistically insignificant between the study groups. However, 39.56% of the patients had haemorrhagic complications in Group I, which is statistically significant (p⩽0.05) in contrast to Group II. In Group I, only 1 (0.55%) patient died from disseminated intravascular coagulation (DIC) followed by postpartum haemorrhagic complications. Although about 80% of the study population had normal echocardiography findings in both study groups, the mechanical prosthesis had a higher incidence (11.54%) of thrombus formation in comparison to the bioprosthesis (3.61%). Approximately, two-thirds of the study patients were followed up regularly; 70.33% and 73.50% of the study population were found in good health status in Group I and Group II, respectively.
Demographic variable of study population (N = 265).
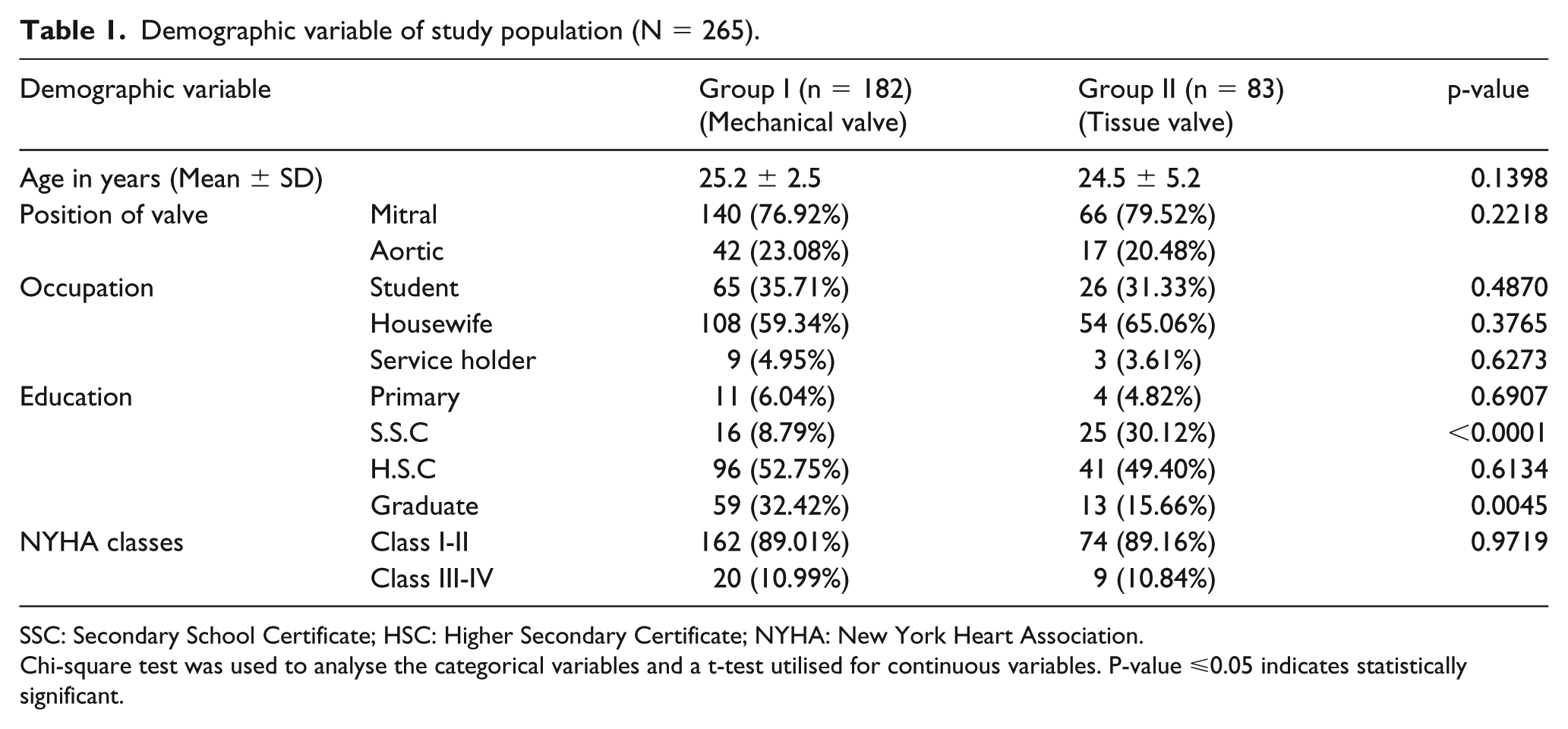
SSC: Secondary School Certificate; HSC: Higher Secondary Certificate; NYHA: New York Heart Association.
Chi-square test was used to analyse the categorical variables and a t-test utilised for continuous variables. P-value ⩽0.05 indicates statistically significant.
Maternal complications related to prosthesis during pregnancy.
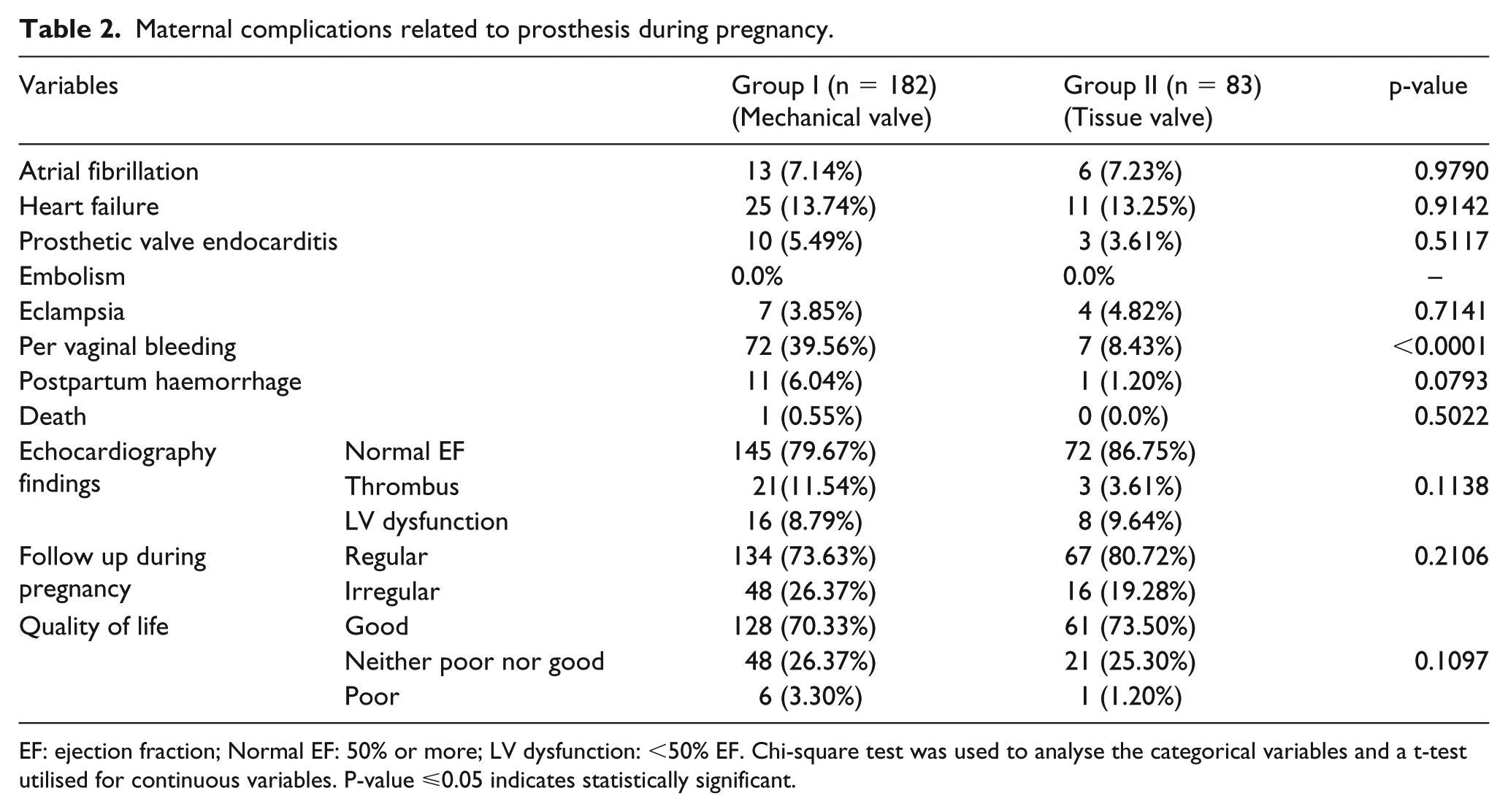
EF: ejection fraction; Normal EF: 50% or more; LV dysfunction: <50% EF. Chi-square test was used to analyse the categorical variables and a t-test utilised for continuous variables. P-value ⩽0.05 indicates statistically significant.
In the first trimester of pregnancy, 35.16% and 6.02% patients had a spontaneous miscarriage in Group I, and Group II, respectively, which is statistically significant (p⩽0.05) between the two groups (Table 3). Normal pregnancy outcome was significantly higher in Group II (91.57%) in comparison to the Group I (61.54%), which was statistically significant (p⩽0.05) between the study groups. Only 2.75% pregnancy had warfarin embryopathy in the mechanical prosthetic group. Mean birth weight was found to be 2.5 ± 0.25 kg and 2.75 ± 0.25 kg in Group I and Group II, respectively. The mean APGAR score was 8.5 ± 0.75 and 8.7 ± 0.50 in Group I and Group II, respectively. A total of 91.76% and 93.98% of cases had caesarean section surgery done in Group I and Group II, respectively. Furthermore, the blood transfusion rate was statistically significant (p⩽0.05) among the study groups. Table 3 illustrates other pregnancy outcomes of the study population.
Pregnancy outcome of study population.
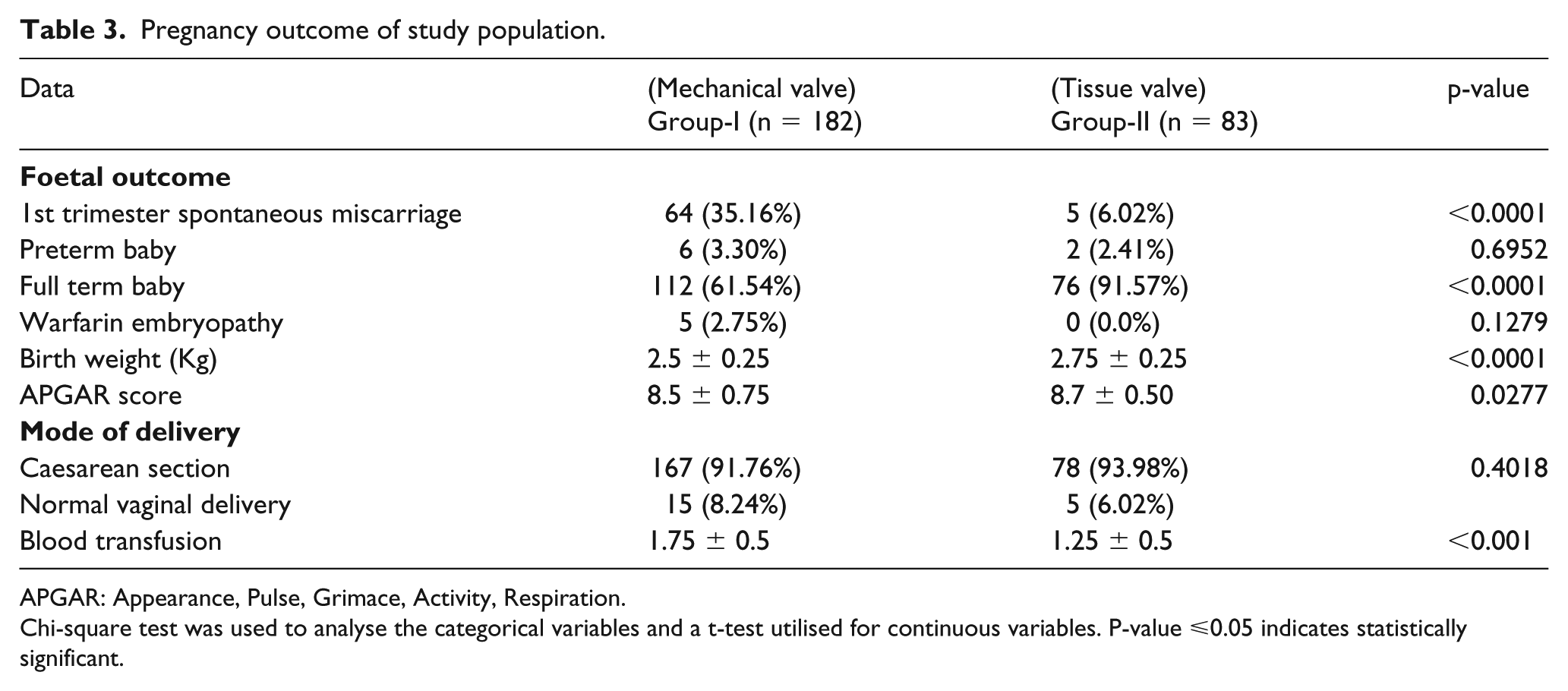
APGAR: Appearance, Pulse, Grimace, Activity, Respiration.
Chi-square test was used to analyse the categorical variables and a t-test utilised for continuous variables. P-value ⩽0.05 indicates statistically significant.
Table 4 shows that the SF-36 scores for HRQOL before pregnancy were statistically insignificant between the study groups; however, SF-36 scores were relatively higher in the tissue valve group. This study also observed SF-36 score differences of HRQOL domains among the study population before and after pregnancy (Table 5). Nonetheless, there was no statistically significant difference among SF-36 sub-scores for HRQOL assessment between the study groups. Comparison of SF-36 sub-score before and after pregnancy between the two study groups is presented in Table 5.
SF-36 scores of patient of Mechanical and Tissue valve groups before pregnancy (N = 265).
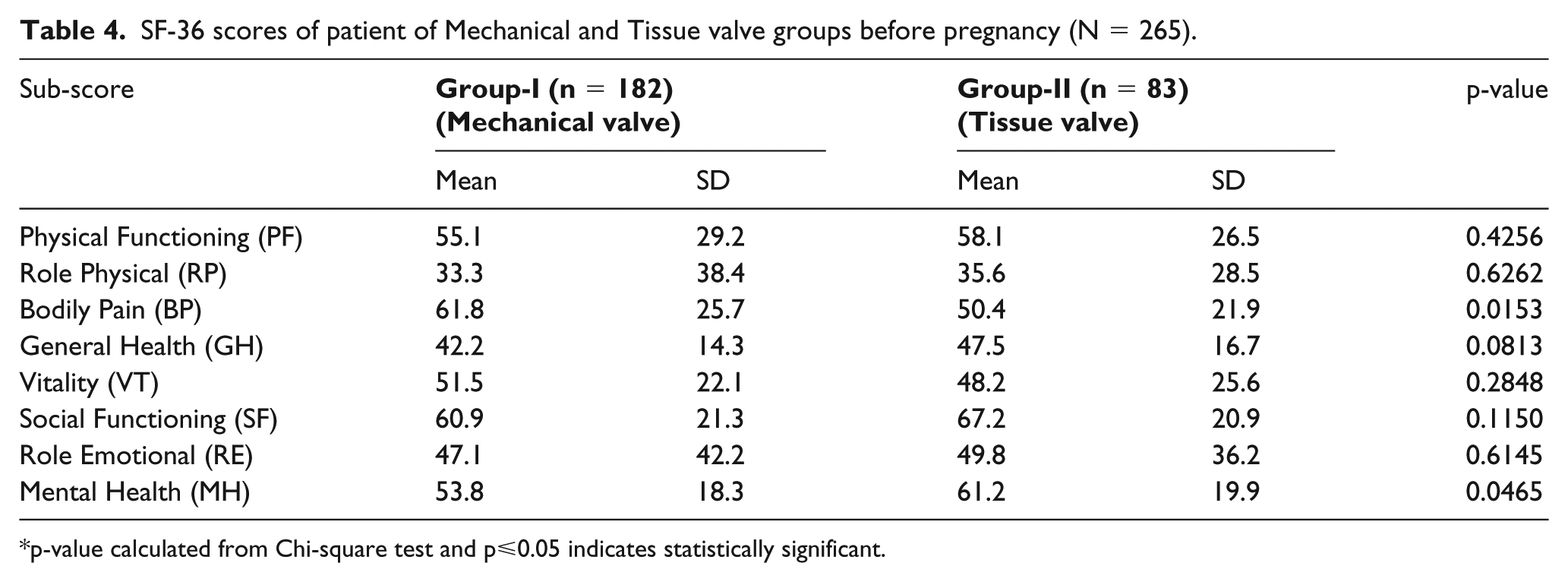
p-value calculated from Chi-square test and p⩽0.05 indicates statistically significant.
SF-36 scores differences between study groups before and after pregnancy.
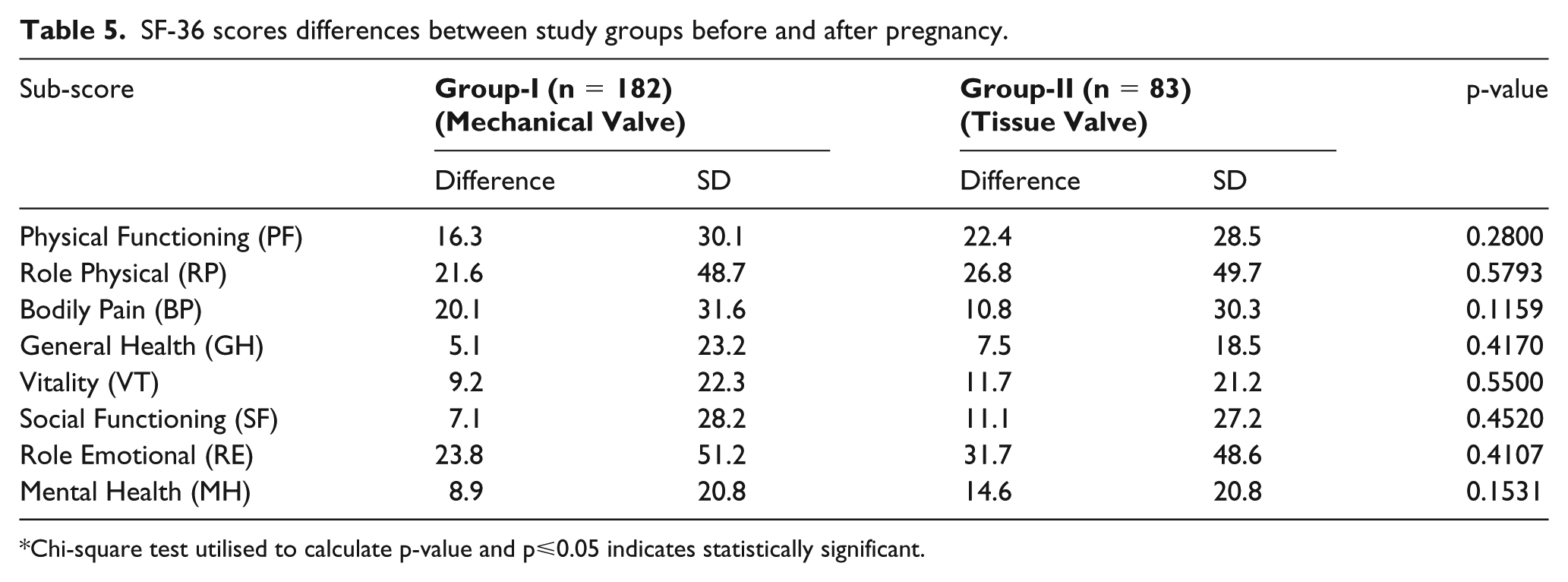
Chi-square test utilised to calculate p-value and p⩽0.05 indicates statistically significant.
Discussion
The objective of this retrospective cohort study was to describe the occurrence of the maternal and foetal outcomes during pregnancy and immediately after delivery in women with prosthetic heart valves in order to adopt better counselling and treatment strategies. A total of 265 pregnancies with prosthetic heart valves were enrolled and were divided into two groups according to the type of heart valve; either mechanical or bioprosthetic. Approximately 74% of the pregnancies ended in live births and full-term baby was significantly higher in the bioprosthetic group in comparison to the mechanical valve group (p⩽0.05). Moreover, Group I patients had a higher incidence of maternal complications than Group II (p⩽0.05). In Group I, a total of 35.2% of the pregnancies were terminated in the first trimester - spontaneous miscarriage - and only 2.75% of babies developed warfarin embryopathy in the mechanical prosthetic group. Mean birth weight and APGAR score were found within normal values and the majority of the study patients were found in good health status during and after pregnancy. There was only 0.55% maternal mortality in the mechanical valve group.
Ashour et al. found pregnancy with mechanical valve replacement in 67% of a study population, which is concordance with other study results.5,8–11 Ayad et al. observed that approximately 15% of patients developed heart failure during pregnancy, which is similar to this study findings. 12 Moreover, Ayad et al. also found that about 52% pregnancies ended in healthy live births, 29% terminated in abortion and 2% were born with congenital anomalies, which is in concordance with other findings.7,10–12 However, in another study, Shannon et al. observed a maternal mortality rate of about 4% with prosthetic heart valve patients who required anticoagulation therapy, which is similar to other published articles.10,12,13 However, in another study by Ashour et al., they demonstrated that approximately 15% of the study population developed maternal complications, such as prosthetic valve thrombosis (8%), infective endocarditis (1%) and bleeding complications (1%), which is also supported by other findings.10,11–14 However, in this study, the incidence of thrombosis, infective endocarditis and haemorrhagic complications was higher in the mechanical valve group due to a lack of appropriate control of the coagulation profile.
In a study, Maxwell et al. have shown that the use of warfarin between 6 and 12 week’s gestational age results in a 6-10% risk of embryopathy, which is in concordance with our findings. 15 Moreover, several published articles observed that there is also an anticoagulant dose-dependent relationship with higher adverse effects, especially bleeding complications, miscarriage and embryopathy occurring at higher (>5 mg daily) doses.4,7,10–16
Chaitali and Kumar observed the outcome of pregnancy with prosthetic valve patients and demonstrated a mean birth weight of 2.72 ± 0.33 kg and APGAR score of 8.81, which is similar to this study findings. 17 Although Chaitali and Kumar found that caesarean section was done in 82% of the study population, Plesinac and Pilic observed the incidence was very low (20%) in their study.17,18 Furthermore, a study by Desai et al. shows that the cardiac patient who can tolerate caesarean section is likely to tolerate labour and vaginal delivery just as well, which is also similar to other published articles.19,20
This study assessed maternal characteristics to determine the possible causes of foetal loss and adverse pregnancy outcome with a prosthetic heart valve, especially with anticoagulation therapy. As a whole, cardiac complication was less in this study, but the rate of prosthetic valve thrombosis was higher in the mechanical prosthetic group, probably due to a lower threshold to maintain appropriate coagulation profile and irregular follow-up. Furthermore, pre-conceptual counselling of women with prosthetic heart valves to emphasize proper anticoagulation therapy and co-ordinated antenatal care may reduce the risk of maternal as well as foetal adverse outcomes.
Conclusion
Although pregnancies in women with prosthetic heart valves, especially mechanical valves, are at high risk for haemorrhagic complications, there is no specific contraindication for pregnancy in patients with good LV function and NYHA class I and II. Appropriate antenatal care, regular follow-up and standard coagulation profile results in favourable outcomes of pregnancy in women with a heart valve prosthesis.
Footnotes
Acknowledgements
I owe my heartfelt gratitude and indebtedness to (Late) Professor Dr. Md. Aftabuddin, Department of Cardiac Surgery, BSMMU, for his patience guidance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.