
Abstract
Background:
Cardiopulmonary bypass (CPB) during open-heart surgery triggers an inflammatory response that can cause significant morbidity and mortality. Human monocytes and regulatory T (Treg) cells are phenotypically and functionally heterogeneous and have been shown to play a significant role in the inflammatory dysfunction triggered by CPB. Glucocorticoids (GCs) have been widely administered for decades in patients undergoing CPB to reduce this inflammatory response. However, it has not been clearly established how routine prophylactic administration of glucocorticoids (GCs) affects monocyte and Treg subsets.
Methods:
Thirty-six patient who underwent heart surgery with CPB were randomly assigned to a methylprednisolone group (MG, N = 18; 500 mg in the CPB priming) and a non-methylprednisolone group (NMG, N = 18). The circulating monocyte and Treg subsets were analyzed by flow cytometry.
Results:
The MG and NMG groups had comparable percentages of monocyte subsets and similar expression levels of HLA-DR, CD86, CD64 and toll-like receptor 4 (TLR4). Remarkably, methylprednisolone increased the percentage of CD4+CD25+ Treg cells among CD4+ T cells in patients undergoing CPB, but did not increase the proportion of suppressive Treg cells, either resting or activated, in these patients undergoing CPB.
Conclusions:
Our results showed that prophylactic administration of methylprednisolone neither decreased the percentages and counts of inflammatory monocyte subsets nor did it induce the expansion of suppressive Treg cells in patients undergoing CPB. These results clarified the effects of GCs on cell-mediated immune responses and provided additional evidence in practice.
Trial registration:
Clinicaltrials.gov: NCT01296074. Registered 14 February 2011.
Keywords
Introduction
The exposure of a patient’s blood to the non-endothelial surface of the cardiopulmonary bypass (CPB) circuit during heart surgery leads to severe systemic and local inflammatory responses, which can cause a number of post-operative complications, including effusions, capillary leak syndrome and multiorgan failure.1,2 Gluco-corticoids (GCs), a class of corticosteroids that exhibit anti-inflammatory, anti-allergic and immunosuppressive properties,3,4 have been used routinely in the practice of prophylaxis against inflammatory responses in patients undergoing CPB.4–7 However, the correlation between glucocorticoid administration and the clinical prognosis remains inconclusive, which has led to a long-standing debate regarding the potential benefits and risks of glucocorticoid prophylaxis in patients undergoing CPB.4,7 To date, the randomized, double-blind, placebo-controlled trials studying the prophylactic administration of methylprednisolone have not demonstrated improved outcomes in patients undergoing cardiac surgery with CPB. 7 Thus, the mechanisms by which GCs can reduce inflammation and the immunological evidence need to be further studied.
A number of immune cells have been proven to play an important role in regulating CPB-induced immune responses. Human monocytes can traffic into injured tissues where they regulate local immune responses by acting as a key source of pro-inflammatory cytokines and functioning as precursors of macrophages and dendritic cells at the sites of tissue injury and inflammation. 8 Conversely, regulatory T cells (Tregs), a subset of T cells, play a critical role in modulating the immune system by suppressing T cell proliferation and cytokine production to prevent autoimmunity and excessive inflammatory responses. 9 Previous studies showed that GCs can inhibit the apoptosis of the anti-inflammatory monocyte subsets and can increase gene transcription of some anti-inflammatory mediators. 10 However, the available reports regarding the impact of GCs on Treg cells are contradictory. Several studies showed that administration of GCs induced the expansion of total Treg numbers by up-regulating transcription factor FoxP3 and their anti-inflammatory reaction.11–13 Conversely, Olsen and colleagues observed a decrease in Treg counts in a mouse model of asthma treated with GCs. 14
Interestingly, recent studies have demonstrated that both monocytes and regulatory T cells can be subdivided into phenotypically and functionally distinct subsets. 15 Human monocytes are classified into 3 subsets that exhibit different expression levels of surface markers and chemokine receptors: classic inflammatory CD14highCD16− monocytes, intermediate CD14highCD16+ monocytes and non-classical CD14lowCD16+ monocytes. The intermediate CD14highCD16+ monocytes exhibit a high capacity for production of tumor necrosis factor (TNF)-α and are more closely correlated with the pathogenesis of many inflammatory diseases.8,16,17 Human FoxP3+CD4+ Treg cells comprise 3 phenotypically and functionally distinct subpopulations: resting Treg cells (rTreg cells) and activated Treg cells (aTreg cells), both of which have been shown to be suppressive in vitro, and cytokine-secreting non-Treg cells, which exhibit limited immunosuppressive activity, but are capable of producing IL-2, IL-17 and IFN-γ.9,18,19
Building upon the notion of subsets of immunocytes, our previous studies explored whether CPB can induce dramatic changes in the subsets of monocytes and Treg cells. Importantly, we demonstrated that immature CD14lowCD16- monocytes contribute to the CPB-induced acute lung injury by generating their mature CD14highCD16+ descendants, a major subset of cells producing TNF-α. At the same time, we observed that CPB induced an increase in the numbers of both rTreg and aTreg cells in patients undergoing cardiac surgery with CPB, 19 which supported the idea that CPB triggers compensatory inhibitory mechanisms to temper the inflammatory responses.
However, the connection between prophylactic administration of GCs and the dynamic changes in the subsets of monocytes and Treg cells in patients undergoing CPB remains unclear. In the present study, we attempted to explore the effects of prophylactic administration of GCs on the dynamic changes of phenotypically and functionally different subpopulations of Treg cells and monocytes in the peripheral blood of patients undergoing CPB.
Materials and methods
Subjects
All participants in the study were enrolled at Beijing Anzhen Hospital, Capital Medical University. All human blood samples were collected after written informed consent was obtained and the study conformed to the tenets of the Declaration of Helsinki (the ethical approval number of our institution: 2009010). Thirty-six patients (15 males and 21 females, 21–75 years of age) who underwent cardiac surgery with CPB in 2012 were selected. Patients with infections, tumors, pregnancy or autoimmune disorders were excluded.
The participants were randomly organized into two groups: the methylprednisolone group (MG) and the non-methylprednisolone group (NMG), (N = 18/group). All patients in the MG group received methylprednisolone (500 mg) in the priming solution for CPB. The patients in the NMG group did not receive GCs before, during or after the operation.
The procedures included mitral valve replacement (MVR) (14 patients), double (mitral and aortic) valve replacement (DVR) (18 patients) and aortic valve replacement (AVR) (4 patients). The range of perfusion time of all 36 patients was 54–188 minutes (average 112.4 ± 34.0 minutes). All patients were ultimately discharged.
CPB procedure
CPB consisted of a Type S III roller pump (Stöckert, Munich, Germany), a QUADROX oxygenator with Safeline coating and an arterial filter (both, Maquet, Jostra Medizintechnik AG, Hirrlingen, Germany) and a standard tubing set without coating (Kewei, Guangdong, China). The CPB circuit was primed routinely with approximately 800 ml of plasma expander (Gelofusion) and 400 ml of lactated Ringer’s solution, 0.25 g.kg−1 of mannitol (20%), 30 mEq of bicarbonate and 3 m.kg−1 heparin. After combined intravenous and inhalation anesthesia, conventional sternotomy and heparinization, patients undergoing CPB were cannulated and bypass was established. Open-heart surgery was performed under mild-to-moderate hypothermia (28–35°C). The blood flow index was 2.2-2.4 L/minute/m2 for adults at a temperature of 28°C or above. The Alpha-stat approach was used during the cardiac procedures in these patients. To protect the myocardium, high K+ blood cardioplegic solution (the ratio of blood to crystalloid cardioplegia mixed is 4:1) was perfused anterogradely through the root of the ascending aorta (AAo). Protamine was used to counteract heparin (1:1) after CPB.
Immunologic markers, absolute count calculation and flow cytometry analysis
Blood samples were collected at the indicated times: immediately before the operation (pre), immediately after the operation (0d) and once a day for 7 days post operation (1d, 2d, 3d, 4d, 5d, 6d, 7d). Antibodies used for flow cytometry analyses included FITC-, PE-, PerCP-, PerCP-Cy5.5 and APC-conjugated anti-human monoclonal antibodies against CD14, CD16, HLA-DR, CD86, CD64, TLR-4, CD4, CD25, CD45RA, all from Becton Dickinson (BD) Biosciences and BD Pharmingen (Palo Alto, CA, USA). BD Trucount Tubes (BD Biosciences), combined with specific antibodies (CD45/3/4/8 cocktail; BD Biosciences), were used to determine the absolute counts of leukocytes in the blood with flow cytometry, in accordance with the manufacturer’s instructions. The absolute numbers (cells per microliter) of leukocytes and T cells was determined by comparing cellular events to bead events. Data acquisition was performed on a FACSCalibur flow cytometer (BD) using CellQuest Software and the data were analyzed using FlowJo Software (Ashland, KY, USA).
Statistical analysis
Continuous variables are expressed as mean ± standard deviation (SD). The categorical data are conveyed as numbers or proportions. We compared independent continuous variables with two-tailed Student’s t tests or Mann–Whitney U tests, as appropriate. The data are presented as mean ± standard error of the mean (SEM) for percentages, as indicated. Differences in the peripheral blood between the two groups were analyzed using a two-way repeated measures ANOVA. If the data were not symmetric, then the Greenhouse–Geisser correction was applied. For all analyses, p<0.05 was considered statistically significant. All statistical calculations were performed with SPSS 19.0 (SPSS, Inc., Chicago, IL, USA).
Results
Characteristics of patients undergoing CPB with and without methylprednisolone
Patients in the MG and NMG groups were well-matched and had a similar distribution of age, gender, etiology and surgery type. The percentage of younger adults (20-39 years) in MG and NMG group was, respectively, 11.11% (N = 2) and 16.67% (N = 3) (p = 0. 63). More than 80% of the primary pathology affecting patients was rheumatic heart disease and the incidences of atrial fibrillation were about 60% in both groups. There were no statistically significant differences between the MG and the NMG with respect to bypass time, cross-clamp time, length of intensive care unit (ICU) stay, duration of mechanical ventilation and length of hospital stay (Table 1).
Characteristics of patients undergoing CPB with and without methylprednisolone.
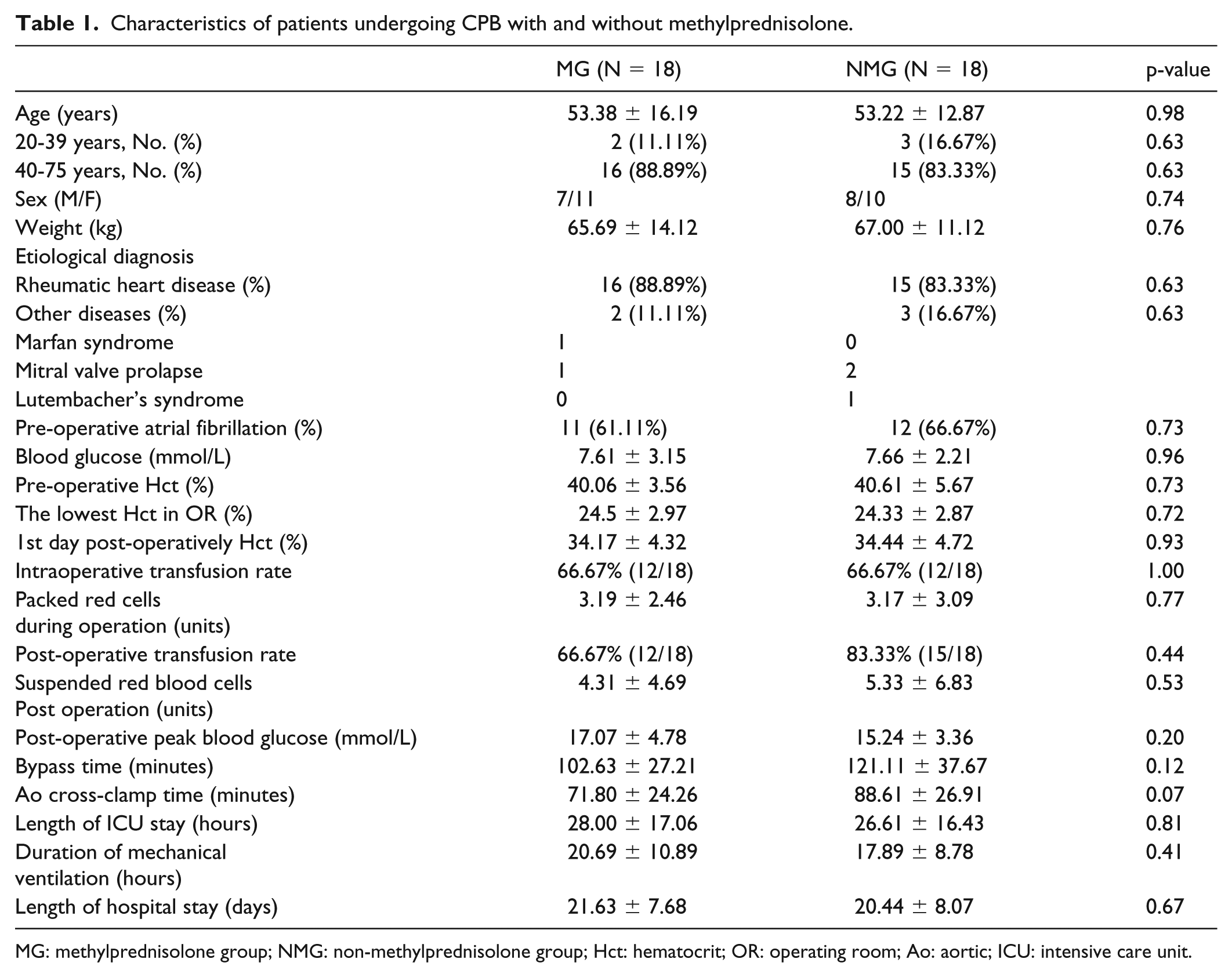
MG: methylprednisolone group; NMG: non-methylprednisolone group; Hct: hematocrit; OR: operating room; Ao: aortic; ICU: intensive care unit.
Prophylactic administration of methylprednisolone did not decrease the counts and percentages of inflammatory monocytes
To explore the effect of methylprednisolone on the monocytes of patients undergoing CPB, we analyzed the kinetic changes of the percentages and absolute numbers of monocytes by flow cytometry. In line with our previous studies, the proportion of monocytes among white blood cells rapidly decreased after CPB, then gradually returned to baseline levels within 5 days after the operation (Figure 1A). A slight decline in the monocyte count was observed after CPB, after which the count increased steadily to levels exceeding the baseline within 1 day post-CPB and remained two-times higher than the baseline levels for nearly a week after the surgery. There was no significant difference in the dynamic changes of the percentages and numbers of monocytes between the two groups (Figure 1B).
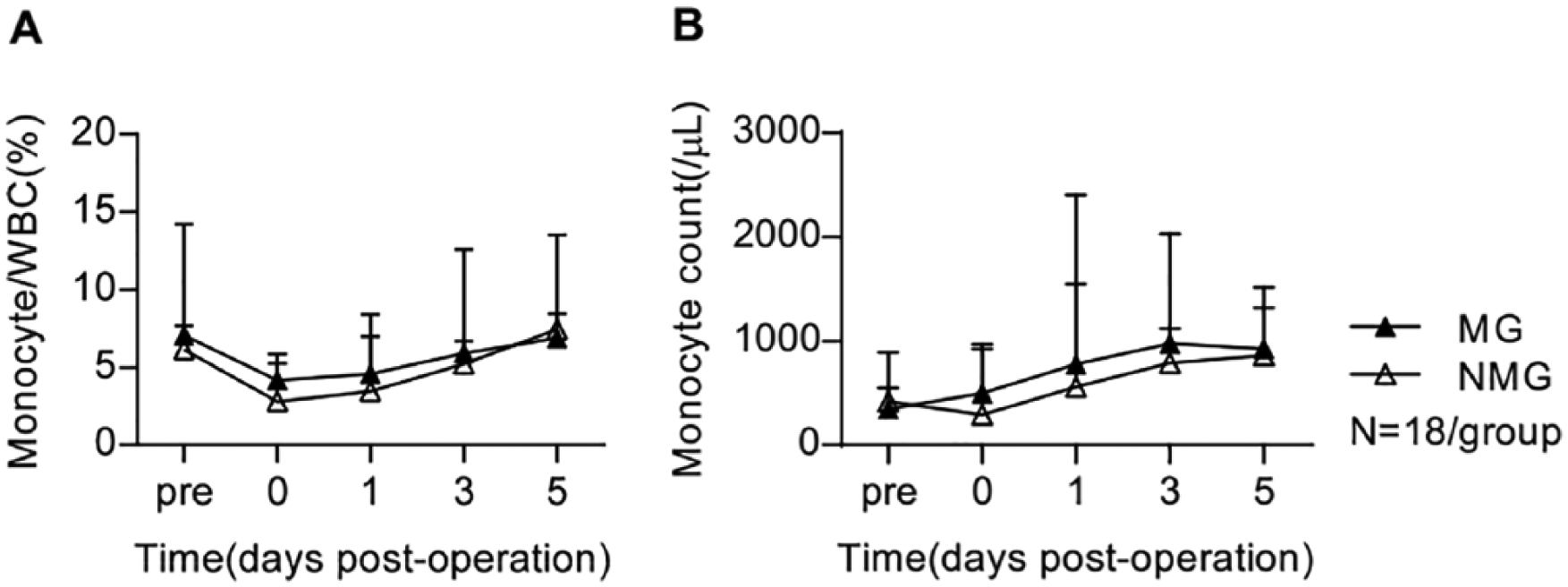
1A. Kinetic changes in the percentage of total monocytes among WBC in MG and NMG patients undergoing CPB.
Next, we divided circulating monocytes into 4 subpopulations: CD14lowCD16- (Mo0), CD14highCD16- (Mo1), CD14highCD16+ (Mo2) and CD14lowCD16+ (Mo3) (Figure 2A). 17 The percentage of immature Mo0 monocytes rapidly increased during the CPB process, then returned to the normal range within 5 days post operation; following a slight decrease during CPB, inflammatory Mo2 monocyte subsets rapidly increased in the peripheral blood after CPB. Nevertheless, methylprednisolone did not significantly change the percentages (Figure 2B-E) and numbers of monocyte subsets (Figure 3A-D) in patients undergoing CPB. Thus, these results indicated that prophylactic administration of methylprednisolone did not reduce significantly the percentages and counts of monocyte subsets, including inflammatory subsets.
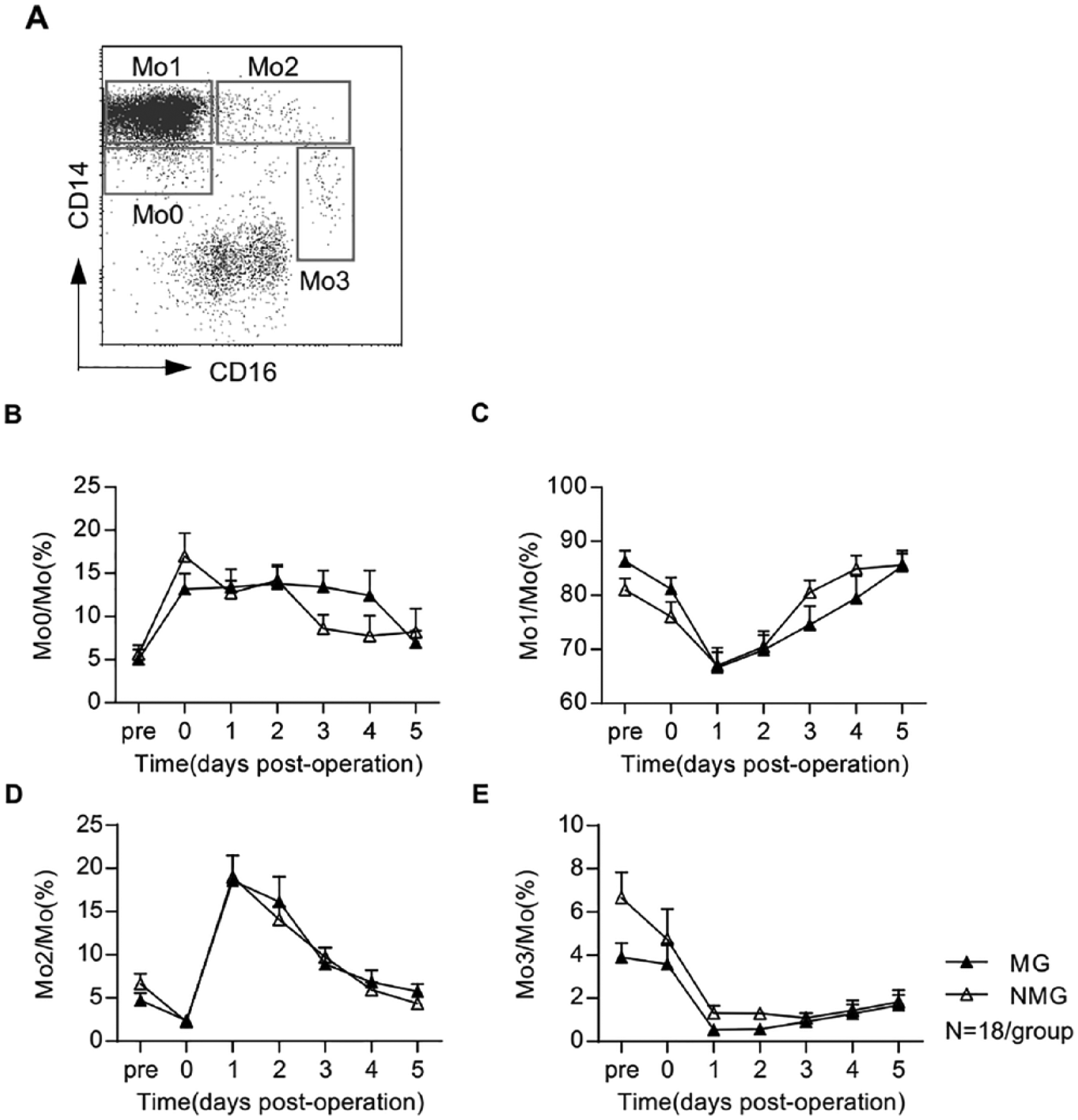
2A. Typical flow cytometry data of patients who underwent CPB.
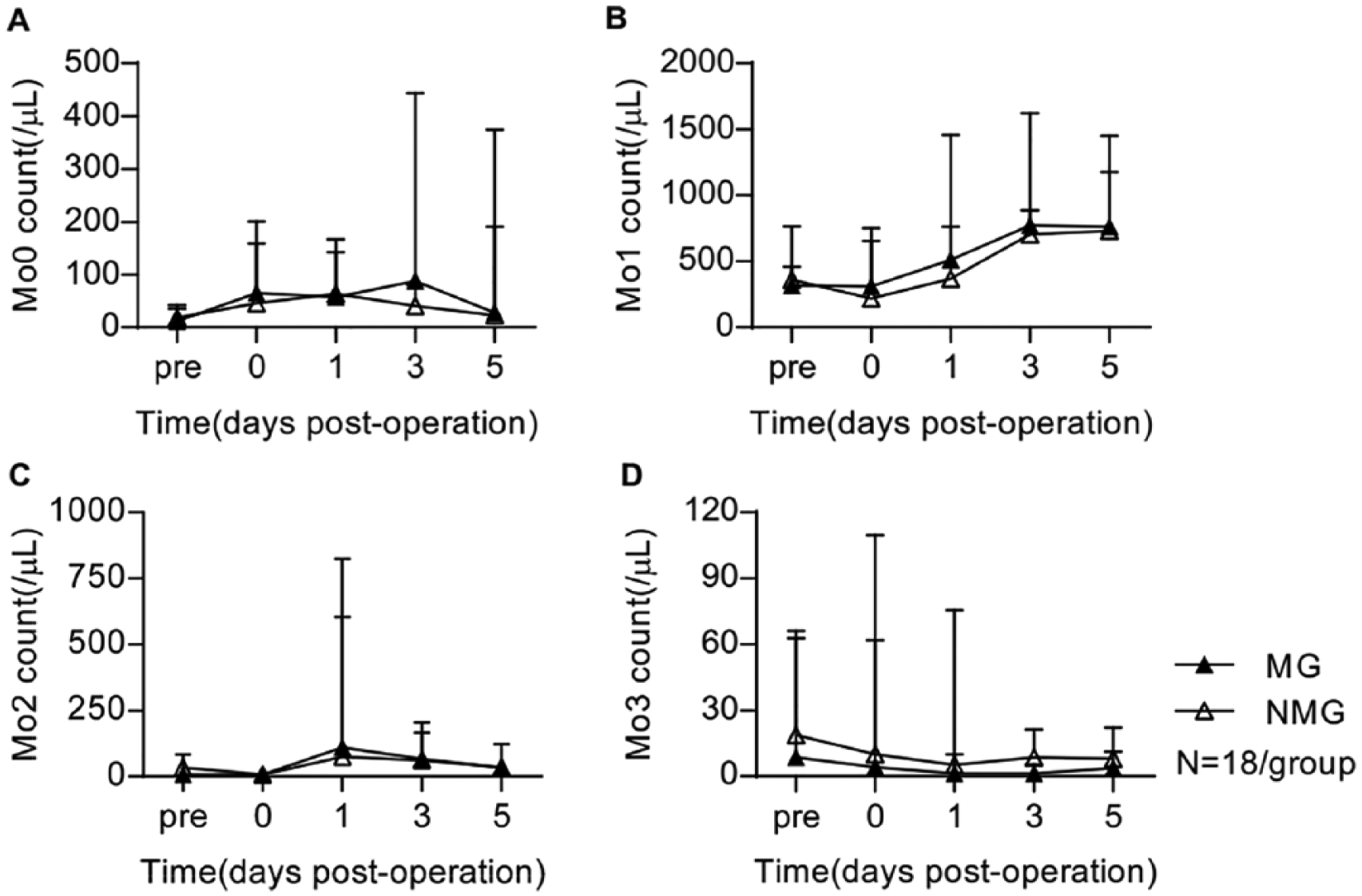
Kinetic changes in absolute counts of 4 monocyte subsets in MG and NMG patients undergoing CPB.
Prophylactic administration of methylprednisolone did not affect functional molecules expression on the monocyte subsets
We observed a decrease in the expression levels of HLA-DR, CD86, CD64 and TLR-4 on 4 monocyte subsets after CPB. Moreover, patients in the MG and NMG groups showed comparable kinetic changes of the expression levels of HLA-DR (Figure 4A-D), CD86 (Supplementary Figure S1A-D), CD64 (Supplementary Figure S2A-D) and TLR-4 (Supplementary Figure S3A-D) on four monocyte subsets.
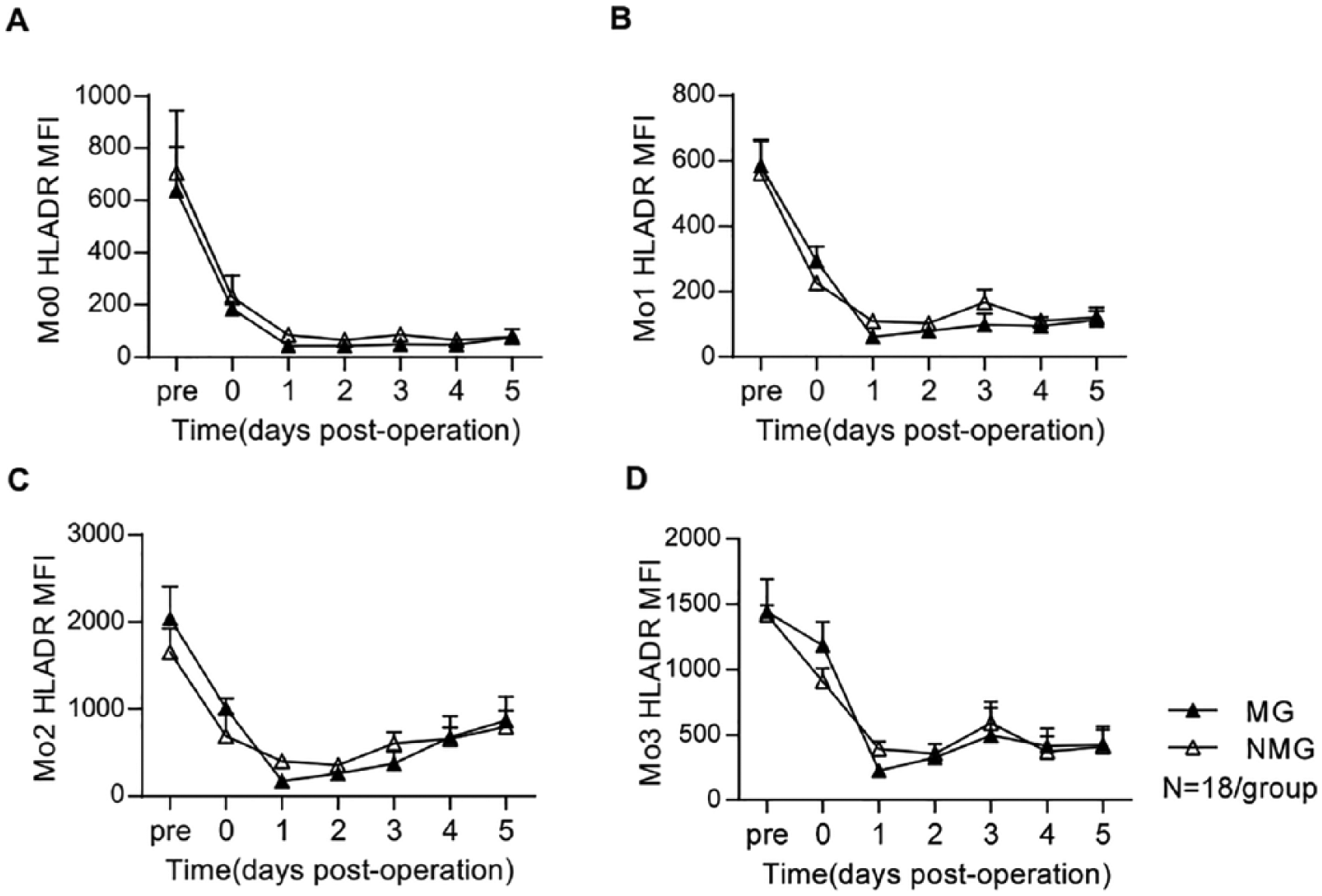
Dynamic changes in MFI of HLA-DR on 4 monocyte subsets in MG and NMG patients before and after CPB.
Prophylactic administration of methylprednisolone did not increase the suppressive aTreg and rTreg subsets
We investigated the kinetic changes in the proportion of Treg cells among CD4+ T cells in the MG and NMG groups. A slight decline of the total CD4+CD25+ Treg proportion was observed during the CPB process, after which the proportion gradually increased to levels exceeding the baseline within 2 to 3 days post-CPB. Remarkably, the proportion of CD4+CD25+ Treg among CD4+ T cells in the MG patients was higher than in the NMG patients within 1 to 2 days post-CPB (1 day post-CPB: 12.83 ± 2.03% vs. 7.36 ± 1.05%, p = 0.017; 2 days post-CPB: 12.55 ± 1.88% vs. 8.18 ± 0.69%, p = 0.029) (Figure 5A). These results indicated that methylprednisolone increased the proportion of total CD4+CD25+ Treg cells among CD4+ T cells in patients undergoing CPB.
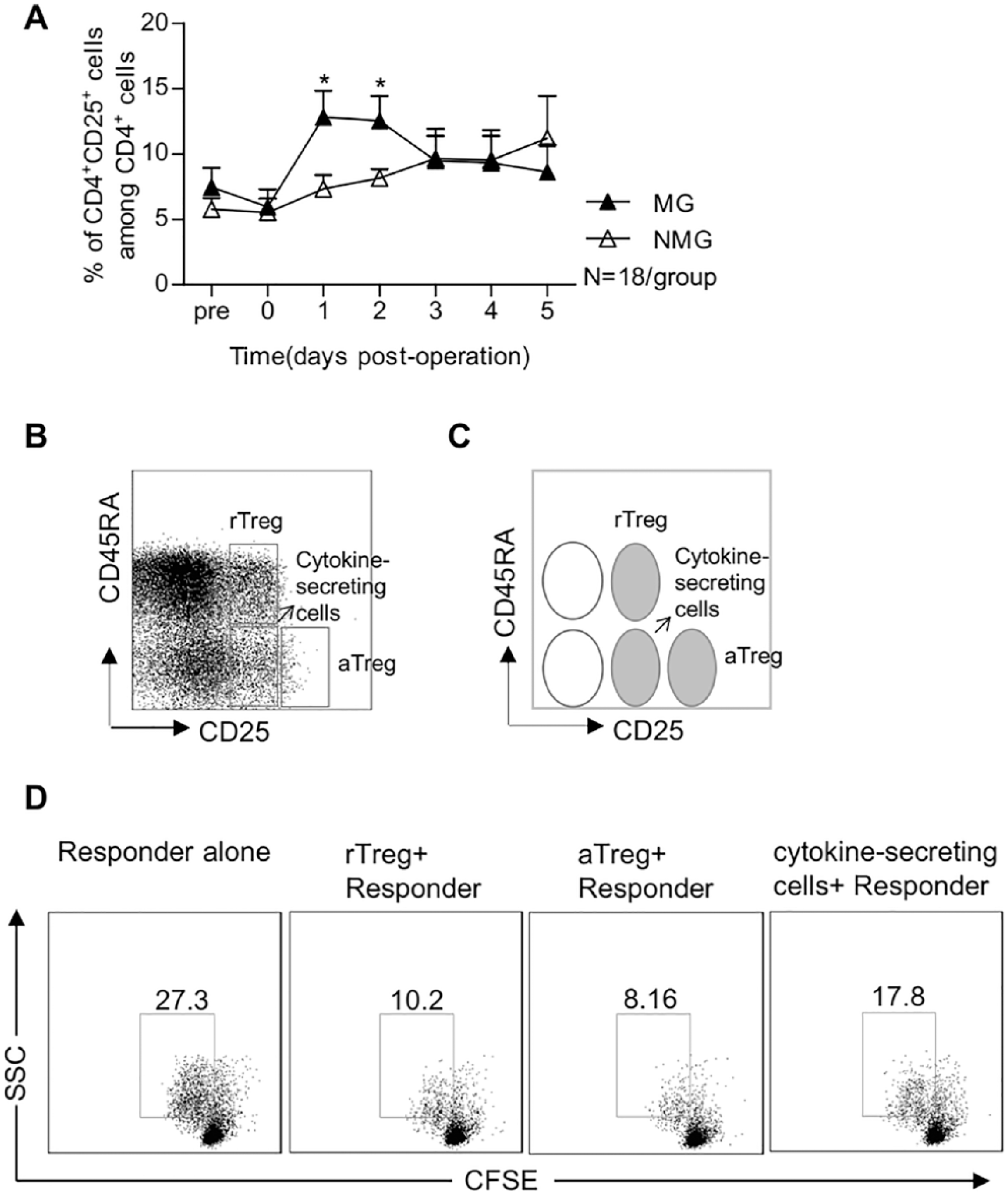
5A. Kinetic changes in the percentage of CD4+CD25+ Treg cells in the CD4+ T cells in MG and NMG patients before and after CPB.
Next, according to CD4/CD25/CD45RA/FoxP3 expression patterns, CD4+ CD25+/++ T cells were divided into 3 subpopulations: rTreg cells (CD45RA+CD25+), aTreg cells (CD45RA−CD25++) and cytokine-secreting non-Treg cells (CD45RA−CD25+, FrIII) (Figure 5B, C). Consistent with previous studies, both rTreg and aTreg were functionally suppressive, while cytokine-secreting non-Treg cells showed moderate suppressive capacity (Figure 5D). We did not find a significant difference in the percentages of aTreg and rTreg subpopulations between the MG and NMG groups (Figure 6A, B). Notably, following a slight and transient decrease, the percentage of cytokine-secreting non-Treg tended to increase within 2 to 3 days post-CPB. We observed an increase in the percentage of cytokine-secreting non-Treg cells among CD4+ T lymphocytes in the MG group compared with the NMG group (11.73 ± 1.49% in MG vs. 7.18 ± 0.91% in NMG, p = 0.016) at 2 days post-CPB (Figure 6C). Furthermore, we found that the (rTreg + aTreg):(Fr III) ratio was decreased in patients undergoing CPB assigned to the MG group compared with the ratio in the NMG group (Figure 6D). Thus, these results suggest that methylprednisolone did not increase the percentage of suppressive Treg cells (rTreg and aTreg) in patients undergoing CPB, but rather increased the percentage of pro-inflammatory cytokine-secreting non-Treg cells.
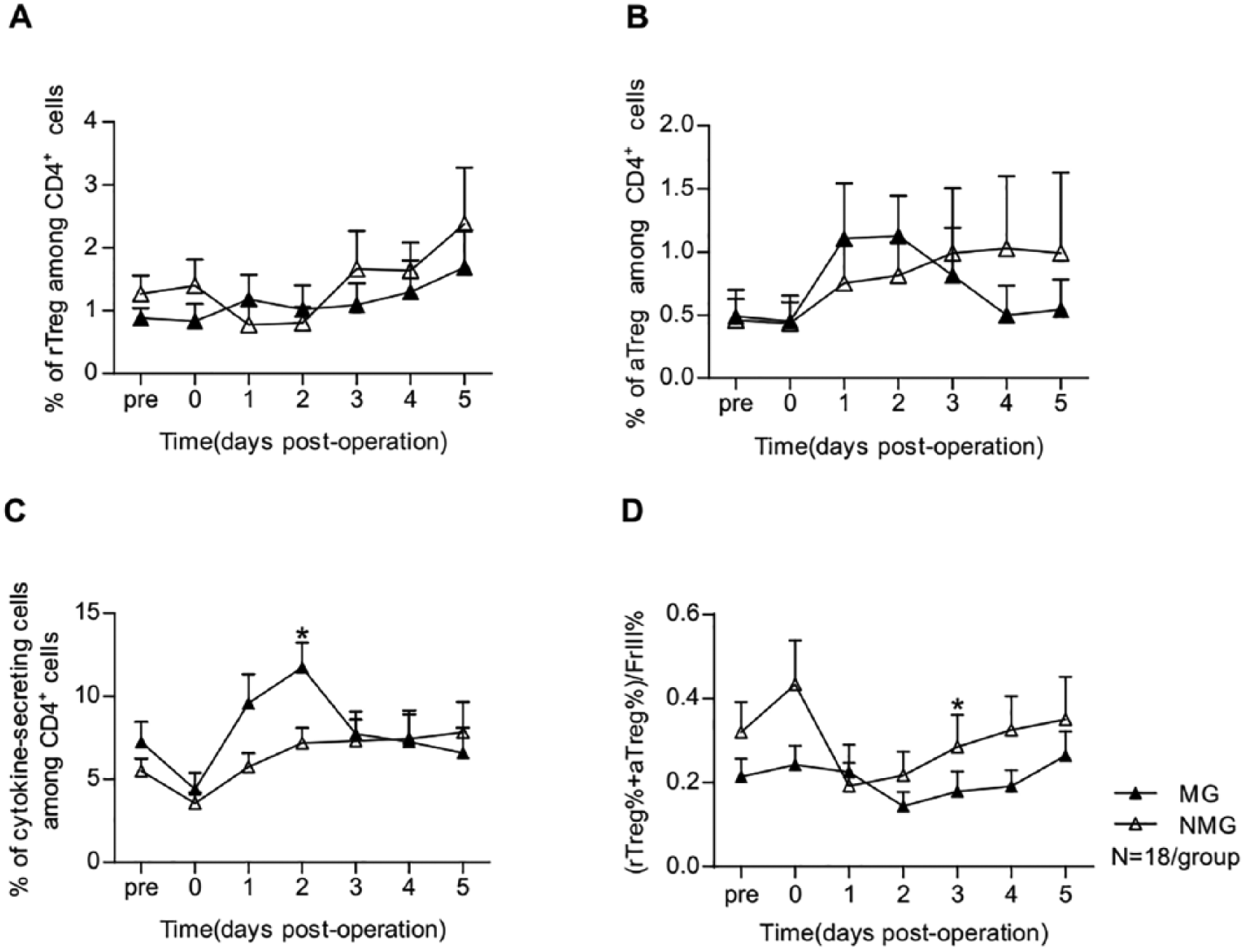
6A. Kinetic changes in the percentage of rTreg in the CD4+ T cells of MG and NMG patients before and after CPB.
Discussion
Known for their anti-inflammatory and immunosuppressive effects, GCs have been widely administered for decades in patients undergoing cardiac surgery to reduce the inflammatory response triggered by CPB. However, the pros and cons of glucocorticoid prophylaxis in patients undergoing open-heart surgery have been the subject of debate for many years. Our current study showed that prophylactic administration of methylprednisolone in patients undergoing CPB neither decreased the percentage and numbers of inflammatory monocyte subsets nor did it induce the expansion of suppressive Treg cells. These results help shed light on the effects of GCs on cell-mediated immune responses and provide additional evidence to be used in the evaluation of glucocorticoid prophylaxis in practice.
Earlier studies suggested that a low dose of GCs was as effective as a high dose of GCs in reducing the risk of atrial fibrillation and the duration of mechanical ventilation in adults undergoing cardiac surgery, while carrying a lower risk of side effects.20,21 Following the recommendations in these studies, most hospitals currently use low-dose GCs to curb CPB-induced inflammation. However, recent studies7,22,23 and meta-analyses 24 found no beneficial effect of corticosteroid prophylaxis on mortality and complications associated with cardiac surgery. Whitlock and colleagues 7 used a large pragmatic trial to show that low-dose methylprednisolone did not effectively reduce morbidity and mortality in patients undergoing heart surgery. In line with these findings, from the standpoint of immune subsets, our results do not support the routine use of methylprednisolone in patients undergoing CPB and it is not necessary to evaluate the effect of high-dose of GCs on immune subsets.
Monocytes, with their various phenotypic and functional subsets, play an important role in the pathophysiological process triggered by CPB, given their participation in both the inflammatory response and immunosuppression. 10 Previous studies have shown that GCs can modulate the mobilization of monocytes and delay their recovery after cardiac surgery. 25 Glucocorticoid therapy has demonstrated distinct effects on inflammatory monocytes. In patients with neuromyelitis optica, Zeng et al. reported that treatment with GCs can reduce the elevation of CD14+CD16++ monocytes, as well as inhibit IL-1β and TNF-α expression in CD14+CD16++ monocytes. 26 Liu B and colleagues showed that GCs promoted CD14++CD16+ enrichment in patients with autoimmune uveitis. 15 Corticosteroid administration repressed HLA-DR expression of monocytes in patients with burns. 27 In the current study, we observed that prophylactic administration of methylprednisolone did not affect the percentage of immature Mo0 subsets which migrated into the peripheral blood from the bone marrow and spleen. 17 In addition, we found that methylprednisolone prophylaxis did not affect the percentage of inflammatory Mo2 subsets nor did it affect the expression levels of HLA-DR, CD86, CD64 and TLR-4 of each monocyte subset.
As immune suppressor cells, Treg cells play an essential role in curbing excessive inflammation and autoimmunity by suppressing functional activity and proliferation of other immune cells.15,28 The previous study showed that CPB induced the expansion of rTreg and aTreg subsets. 19 GCs were shown to induce FoxP3+CD4+CD25+ Treg cell expansion in patients with myasthenia gravis and in an experimental autoimmune encephalomyelitis mouse model.12,13 On the contrary, short-term GCs therapy did not increase circulating Treg cell frequency in immunocompetent humans and mice 29 and it actually decreased Treg numbers and activity in asthma mouse models. 14 Thus, whether GCs can play an anti-inflammatory role by modulating Treg cells remained the subject of debate. However, recent evidence9,18,19 has indicated that human Treg cells are a heterogeneous population with three distinct subpopulations (suppressive rTreg and aTreg cells and cytokine-secreting non-Treg cells). In line with previous studies,12,13 we found that methylprednisolone increased the proportion of total CD4+CD25+ Treg cells in patients undergoing CPB. However, we revealed that prophylactic administration of methylprednisolone significantly increased the frequency of cytokine-secreting non-Treg cells among CD4+ T cells rather than expanding the suppressive rTreg and aTreg subsets. In addition, we demonstrated an imbalance between the anti- and pro-inflammatory subsets by measuring the (aTreg+rTreg):(Fr.III) ratio in patients undergoing CPB. The cytokine-secreting non-Treg population has limited suppressive activity, but can produce interleukin (IL-2, IL-17) and interferon (IFN-γ), 18 which play an important role in T-cell activation and pulmonary inflammation. Whether the increase in the relative frequency of the cytokine-secreting non-Treg cells is related to some clinical side effect of glucocorticoid administration, such as the prolonged duration of mechanical ventilation, and the potential mechanisms implicated in the development of side effects must be further studied.
There are several possible reasons why GCs did not take on an anti-inflammotory role by inhibiting inflammatory monocyte and expanding suppressive Treg cells in patients undergoing CPB. First, the effect of GCs on immune cells might be dose-dependent. The one-time low dose of GCs in our study might have been insufficient to balance the rapid, short and intense inflammatory reaction induced by CPB. 30 Furthermore, glucocorticoid physiology follows a biphasic dose-response curve, with GCs exerting immunostimulatory effects in low doses and suppressive effects in high doses.31,32 In the present study, we did not exclude the suppressive effects of high-dose GCs on immune subsets. Second, the timing of glucocorticoid administration might influence the effect of GCs on immune cells. In a rat model of delayed-type hypersensitivity, acute low-dose glucocorticoid administration before challenge actually enhanced inflammatory response. 33 In addition, all patients in the MG and NMG groups underwent valvular replacement (VR); the patients with coronary artery bypass grafting (CABG) and the patients with VR-CABG were not enrolled. The effect of GCs on each patient’s immune response is different, which might be caused by their respective primary diseases and/or age.
Despite the small sample size, the results from the present exploratory research suggested that the MG and NMG groups were similar in the patterns and the distribution of the immune subsets, which is sufficient to clarify the effects of GCs on monocyte and Treg subsets and provide additional evidence in practice. Additionally, the results of our research may not apply to the efficacy of other glucocorticoid regimens or the potential role of other inflammatory pathways that were not directly examined in this study.
Conclusions
Our study showed that one-time low-dose prophylactic administration of methylprednisolone in patients undergoing CPB during cardiac surgery did not exert the anticipated immunosuppressive effects implicated in regulating inflammatory monocytes and suppressive rTreg and aTreg cells. Thus, it is not recommended to routinely use methylprednisolone prophylaxis in patients with CPB. By exploring the effect of GCs on immune regulation, our study provided additional evidence to help re-evaluate the routine prophylactic administration of GCs in patients undergoing CPB.
Supplemental Material
supplementary_Figures – Supplemental material for The effect of methylprednisolone prophylaxis on inflammatory monocyte subsets and suppressive regulatory T cells of patients undergoing cardiopulmonary bypass
Supplemental material, supplementary_Figures for The effect of methylprednisolone prophylaxis on inflammatory monocyte subsets and suppressive regulatory T cells of patients undergoing cardiopulmonary bypass by Xing Hao, Junyan Han, Hui Zeng, Hong Wang, Guoli Li, Chunjing Jiang, Zhichen Xing, Yu Hao, Feng Yang and Xiaotong Hou in Perfusion
Footnotes
Acknowledgements
The authors would like to thank Miss Iulia Filip for providing writing and editing services. We are grateful to Dr. Gang Wan, a professor of statistics at Beijing Ditan Hospital, Capital Medical University, for his assistance in statistical analyses and data evaluation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the National Natural Science Foundation of China (No. 81071587 to Hui Zeng, No. 81270327 to Xiaotong Hou and No. 81470528 to Xiaotong Hou).
Summary of Author Contributions
X.H and JY.H: data and statistical analysis and manuscript preparation; H.Z and H.W: critical revision of article; Data collection by GL.L, CJ.J, ZC.X, Y.H and F.Y; Funding secured by H.Z and XT.H; XT.H: concept/design and critical revision of article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.