
Abstract
Background:
Cardiopulmonary bypass causes detrimental effects on remote organs due to inflammatory response. One of these organs is kidney that is frequently affected by cardiac surgery. Acute kidney injury is a post-cardiopulmonary bypass complication, which may result in increased post-operative morbidity and mortality. Post-cardiopulmonary bypass inflammatory response may contribute to remote organ dysfunction. In the present study, we investigated the relation between cytokines including interleukin-6, interleukin-8, interleukin-10, and tumor necrosis factor-α, and renal function tests such as creatinine and blood urea nitrogen (BUN).
Methods:
In total, 91 patients between the ages of 4 and 60 months were enrolled for elective cardiac surgery with cardiopulmonary bypass after informed consent. Data regarding renal function tests and clinical outcomes were carefully recorded until 24 hours after admission to intensive care unit and analyzed.
Results:
Our findings support that there is a direct correlation between cytokines including interleukin-6, interleukin-8, interleukin-10, and tumor necrosis factor-α and cardiopulmonary bypass time, duration of operation, and intensive care unit stay. Longer cardiopulmonary bypass time was associated with higher interleukin-8 at cross-clamp removal and 24 hours post- intensive care unit as well as higher interleukin-10 at declamp time. Higher interleukin-6 at declamp time was directly correlated with higher post-operative BUN. Interleukin-8 level after anesthesia induction was directly correlated with intensive care unit stay duration. Higher blood interleukin-6 and tumor necrosis factor-α levels following 24 hours of admission to intensive care unit were associated with longer mechanical ventilation time.
Conclusion:
Higher circulatory pro-inflammatory cytokine level is associated with adverse outcomes such as increased intensive care unit stay and longer mechanical ventilation time in pediatric patients. It is also correlated with unfavorable biochemical parameter of renal function, BUN. Findings hint that proper control of the inflammatory response is vital for the control of unfavorable clinical and pathological outcomes.
Keywords
Introduction
Cardiopulmonary bypass (CPB) maintains blood supply to tissues during the cardiac operations and protects myocardial tissue against ischemic injury; 1 however, CPB is associated with ischemia/reperfusion (I/R) injury. Ischemia increases the rate of anaerobic metabolism and is associated with the coalescence of its metabolites in the affected tissue followed by enhanced reactive oxygen species and oxidative stress. These give rise to a systemic inflammatory response following the reperfusion, re-establishment of the blood flow in the ischemic tissue.2–7 Therefore, the plasma level of pro-inflammatory cytokines, released by white blood cells and the cells of the ischemic tissue, is increased. 8 The systemic inflammatory response causes changes in body temperature, activation of immune cells, and further release of inflammatory mediators. This inflammatory response can have detrimental effects on organs. The triggers for inducing the inflammation include not only I/R injury but also endotoxemia and surgical trauma among the others.9,10 Evidences suggest that increasing the level of interleukin (IL)-6 after CPB could be used as a predictor of post-operative infection 11 and implies a higher rate of tissue injury. 12 Most of the tissue injuries subsequent to CPB are result of the extravascular migration of activated neutrophils promoted by cytokine-mediated inflammatory response. 13 Acute systemic inflammation may cause remote organ dysfunction.14,15 One of the vital organs which is affected by post-CPB adverse biochemical changes is kidney. Acute kidney injury (AKI) is an important complication after cardiac surgery which increase morbidity. 16 This tissue is very sensitive to I/R injury and systemic inflammatory response.4,7,17 Uncontrolled damage to kidneys may cause temporary or irreversible kidney function loss. 17 Current approach of the determination and diagnosis of AKI depend on the serum level of creatinine. 18 Previous studies have demonstrated that increasing the levels of IL-1b, IL-6, IL-8, and tumor necrosis factor-α (TNF-α) are involved in the organ failure.19–24 In addition, it has been suggested that the plasma IL-6 and IL-10 levels are elevated in the acute phase of the inflammatory response after CPB and interact with the most frequently used biomarkers for peri- and post-operative renal complications. 25
In the present study, we investigated the trend of cytokines including IL-6, IL-8, IL-10, and TNF-α in pediatric CPB patients pre-operation (after anesthesia induction), post-cross-clamp removal, and 24 hours after admission to intensive care unit (ICU) and examined its correlation with renal function markers such as creatinine and blood urea nitrogen (BUN). Furthermore, we tested for the correlation between these cytokines, and the ICU stay, duration of mechanical ventilation, aortic cross-clamp time, pump time, and duration of operation in pediatric CPB patients.
Materials and methods
Study design
In a cross-sectional study, 91 pediatric patients candidate for elective surgical correction of congenital anomalies indicated for elective cardiac surgery with the CPB were enrolled after informed consent. Sampling strategy was based on convenient sampling from available pool of patients referring to the Rajaie Cardiovascular Medical and Research Center from the beginning of the December 2016 until the end of March 2017. All patients meeting the inclusion criteria were recruited provided informed consent. Study was conducted in compliance with the ethical codes of the Helsinki declaration on medical studies including human subjects. The study protocol was confirmed with Rajaie Cardiovascular Medical and Research Center Ethics Committee. Inclusion criteria were age between 4 and 60 months, informed consent of guardians, weight below or equal to 15 kg, candidate for CPB surgery, pump time between 80 and 180 minutes, and operation time between 240 and 360 minutes. Exclusion criteria were emergency surgery, pre-operative circulatory support with inotrope, and chronic systemic disease.
Operation procedure
After pre-oxygenation (FiO2 = 1.0), anesthesia was induced by 10 μg/kg of fentanyl, 0.1 mg/kg of midazolam, and 0.15 mg/kg of pancuronium. Standard monitoring included pulse oximetry, ECG, non-invasive and invasive blood pressure and central venous pressures, nasopharyngeal temperature, and end-tidal CO2. Anesthesia was maintained using 0.5 μg kg−1 hour−1 of fentanyl, 1.0 μg kg−1 minute−1 of midazolam, and 0.1 mg/kg of pancuronium every 45 minutes. Ventilation was adjusted to maintain end-tidal CO2 (ETCO2) between 30 and 35 mmHg.
After induction of anesthesia, arterial and central venous line inserted via radial and right internal jugular vein, respectively. Heparin, 300 UI/kg was administered before aortic cannulation for an activated clotting time (ACT) above 480 seconds. CPB was established in a standard manner with the use of a roller pump and non-pulsatile flow (approximately between 2.5 and 3.0 L/m2 body surface area (BSA)/min according to blood pressure and body temperature). During CPB, hematocrit maintained between 25% and 30%. The target body temperature was 30°C. A hemofiltration circuit was used for common ultrafiltration in all patients.
Data collection
Anthropometric and clinical characteristics were registered for all the patients as well as the surgery parameters (length of the operation, of the CPB, of the aortic cross-clamping). CPB parameters were noted every 10 min and included mean arterial pressure, cardiac index, SvO2, and central temperature. Also, we explained acute renal disease (ARD) according to blood creatinine; increasing less than 25% shows no ARD, 26 increasing from 25% to 50% shows faint ARD, 27 increasing from 50% to 100% shows moderate ARD, 28 and increasing more than 100% shows severe ARD. The renal function impairment classification based on changes in the creatinine levels has been established26–28 and used in previous studies. 29 It should be noted that ARD was calculated by blood level of creatinine prior to surgery and 24-48 hours after operations.
Sampling times for drawing blood samples for cytokine measurement were (1) after induction of anesthesia and before skin incision, (2) 1 minute after releasing the cross-clamp, and (3) 24 hours after the surgery (ICU admission). TNF-α, IL-6, IL-8, and IL-10 cytokines were quantified in plasma for all these times using standard enzyme-linked immunosorbent assay (ELISA) method with a commercial EIA assay kit according to the manufacturer’s instructions (Biorbyt, UK). BUN and creatinine were measured at these times using standard blood chemistry analyzer at our clinical diagnostics laboratory. Pre-operative renal function was estimated using the formula of Cockcroft and Gault. 30 Variations of the plasma creatinine were used to appreciate renal function variations. Diuresis was registered at all the previously defined times until the second day after the surgery.
Statistical analysis
As the distribution was not normal for data (Shapiro–Wilk test), quantitative data were compared using the Kruskall–Wallis test and qualitative data using the Chi-square test (IBM SPSS version 24). Also, we used one-way analysis of variance (ANOVA) repeated measure for evaluating the changing plasma levels of cytokines, creatinine, and BUN. Correlation for all data was studied using linear regression. Data are expressed as mean ± SEM in each group. A p-value of less than 0.05 was considered statistically significant. We set α error at 0.05 and power (1 – β) at 0.8 for the analysis of data. Also, it should be noted that the post hoc power analysis of all statistical reports was more than 80% in this article.
Results
Patients enrolled for this study diagnosed with atrial septal defect (ASD), atrioventricular canal defect (AVCD), atrioventricular septal defect (AVSD), ventricular septal defect (VSD), and tetralogy of Fallot (TF). The mean age of the participants was 28.4 ± 1.92. In this article, we evaluated the creatinine, BUN, IL-6, IL-8, IL-10, and TNF-α at three times as previously described and the trend of each outcome over the time as well as the correlation between inflammatory markers and the renal function parameters were tested. The trends in the blood levels of creatinine and BUN at these times are presented in Figure 1. Statistical analysis demonstrated no significant differences between the measurements in these times in creatinine and BUN. As depicted in Figure 2, analysis demonstrated significant elevation of the cytokine levels from pre-operative measures into post-cross-clamp. The level of the four cytokines declined in the 24 hours post-ICU time compared with the post-cross-clamp time; however, it was slightly higher compared to the pre-operative amounts.
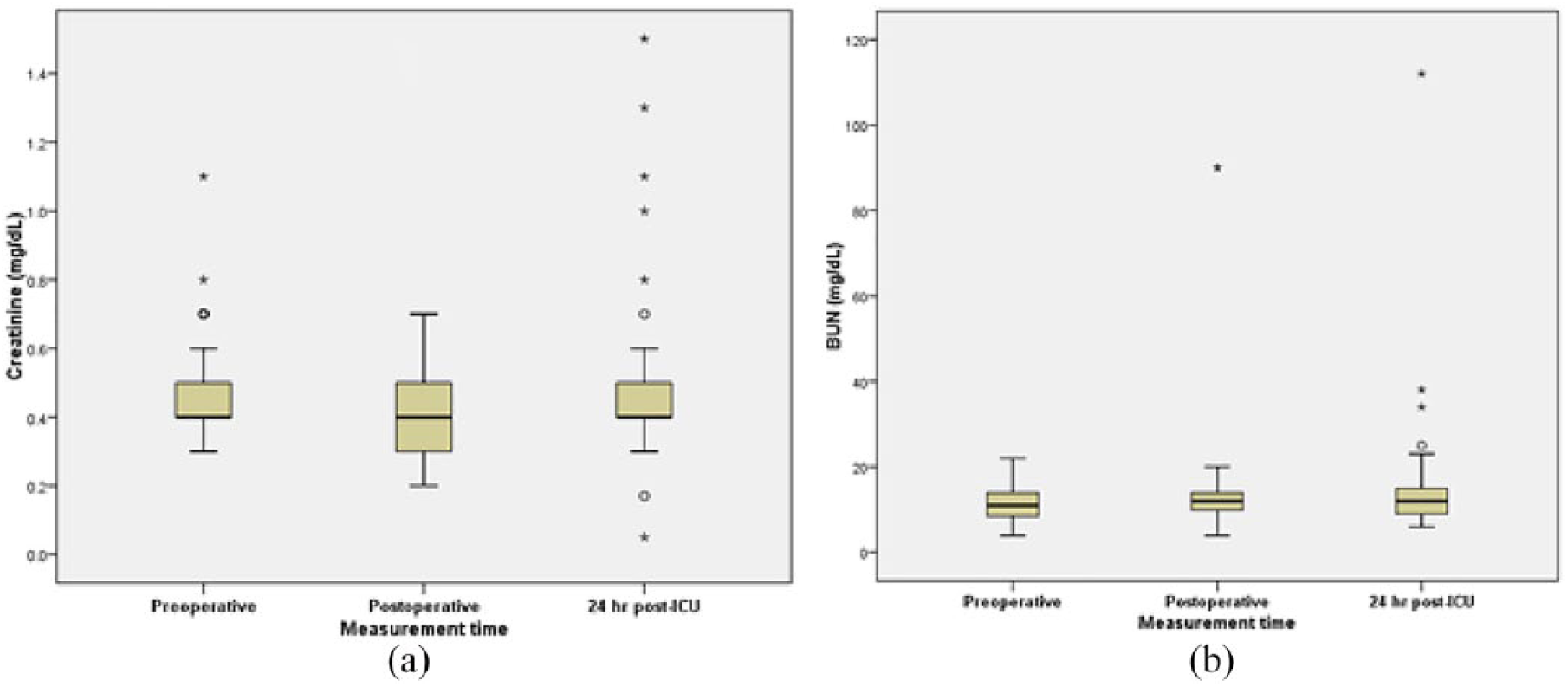
The plasma level of creatinine (a) and BUN (b) at pre-operation (before anesthesia induction), post-operation (ICU admission), and after 24 hours after ICU admission.
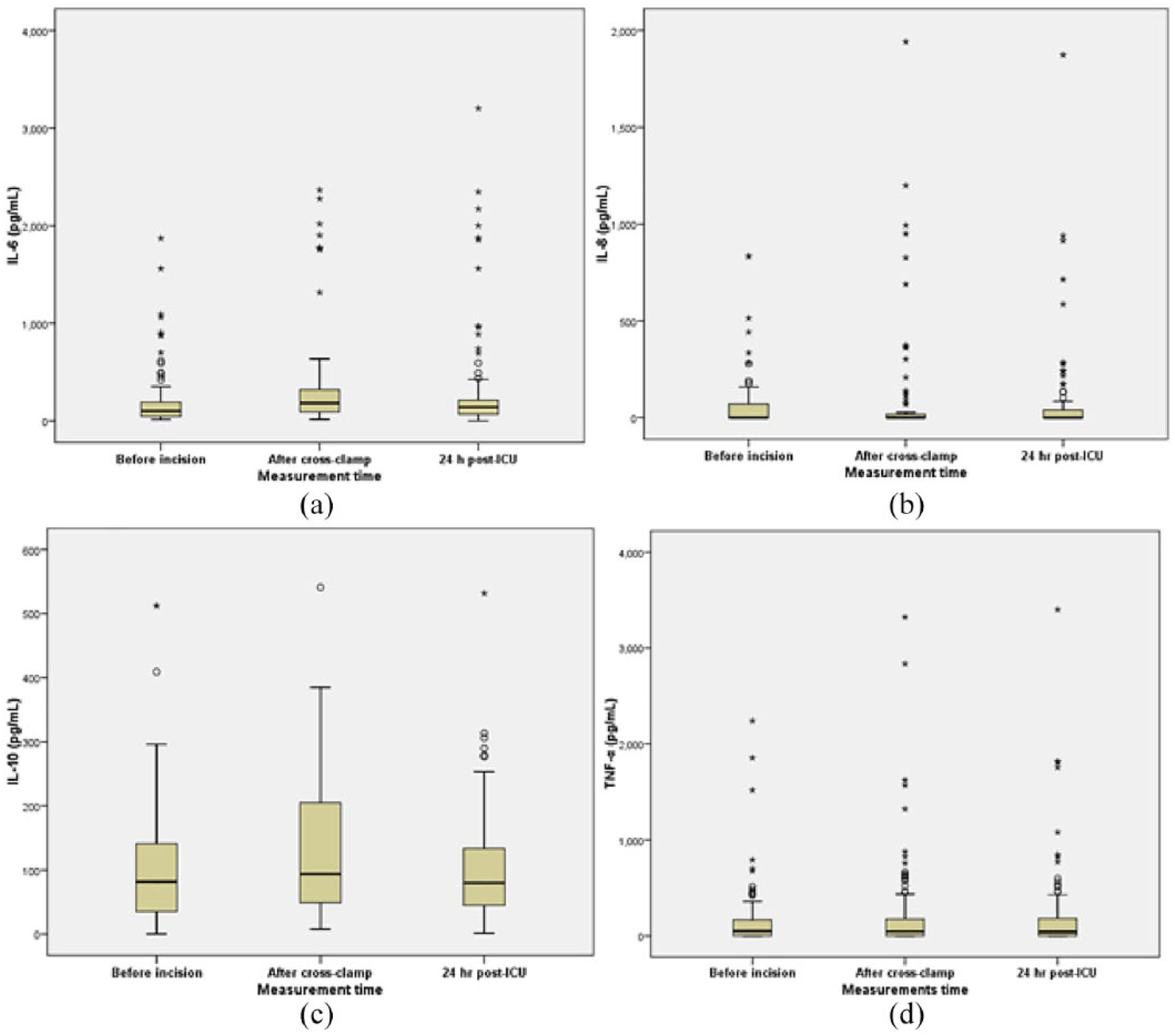
The plasma level of IL-6 (a), IL-8 (b), IL-10 (c), and TNF-α (d) at pre-operation (after anesthesia induction and before incision), post-declamp, and 24 hours after ICU admission.
The relation between the levels of age, cross-clamp time, mechanical ventilation duration, ICU stay, ultrafiltration on CPB, diuresis on CPB, and all three times of creatinine and BUN with IL-6 is examined and summarized in Table 1. A direct correlation was found between circulatory IL-6 values after cross-clamp removal and post-operative BUN and IL-6 after 24 hours of ICU admission and mechanical ventilation time (p > 0.05).
The demographic information of the patients recruited for studying the correlation of IL-6 at three times (pre-, post-declamp, and 24 hours after ICU admission) between factors.
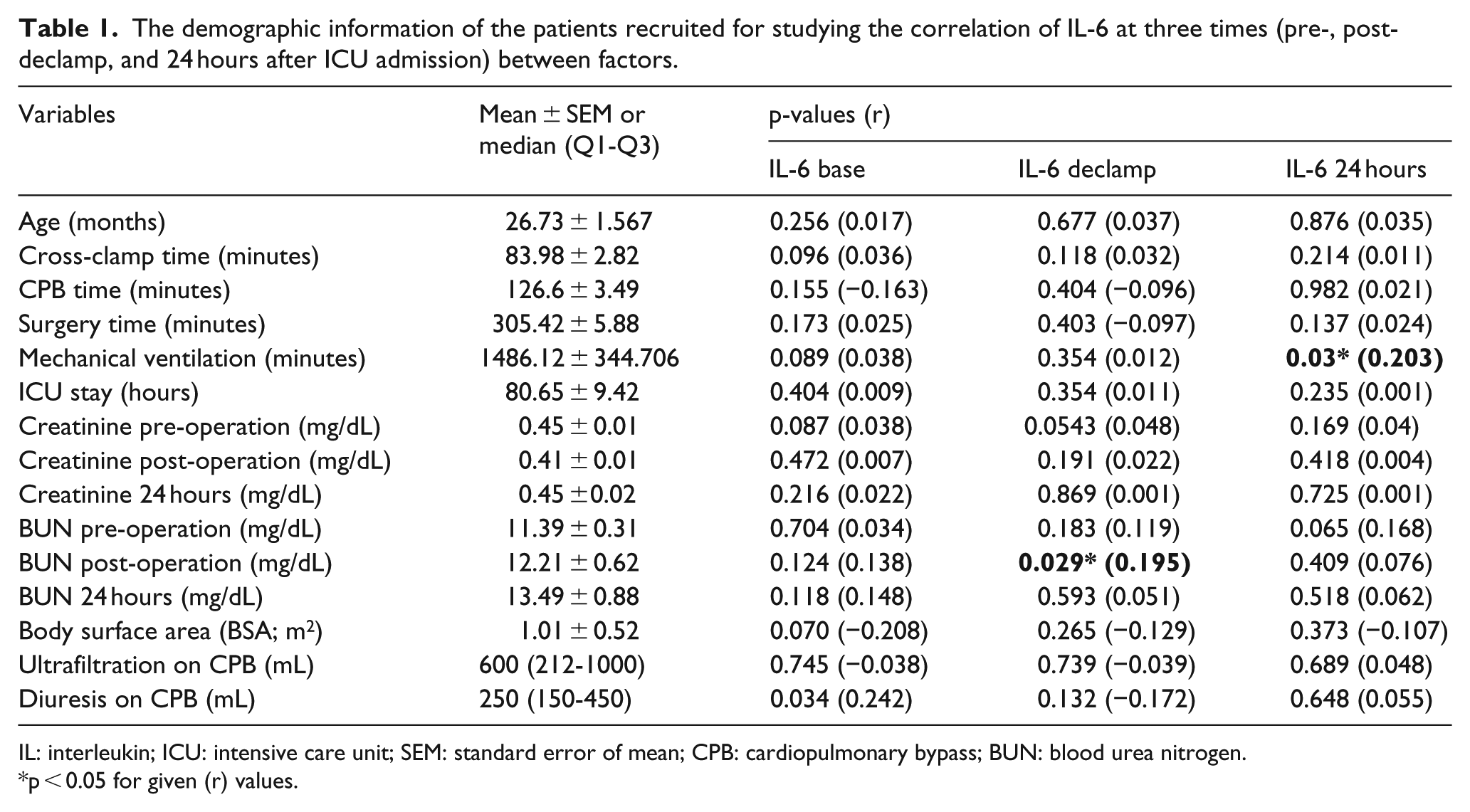
IL: interleukin; ICU: intensive care unit; SEM: standard error of mean; CPB: cardiopulmonary bypass; BUN: blood urea nitrogen.
*p < 0.05 for given (r) values.
The correlation between the levels of plasma IL-8 in three time points with factors such as age (p > 0.05), cross-clamp time (p > 0.05), mechanical ventilation duration (p > 0.05), surgery time (p > 0.05), ultrafiltration on CPB (p > 0.05), diuresis on CPB (p > 0.05), and all three times of creatinine and BUN (p > 0.05) is summarized in Table 2. Significant relationships were observed between CPB time and IL-8, in post-cross-clamp time and 24 hours after ICU admission (p < 0.05). This relationship was insignificant for pre-operative amounts of IL-8 (p > 0.05). Moreover, pre-operative circulatory IL-8 level was directly correlated with the length of ICU stay (p < 0.05).
The correlation of IL-8 at three times (pre-, post-declamp, and 24 hours after ICU admission) between factors.
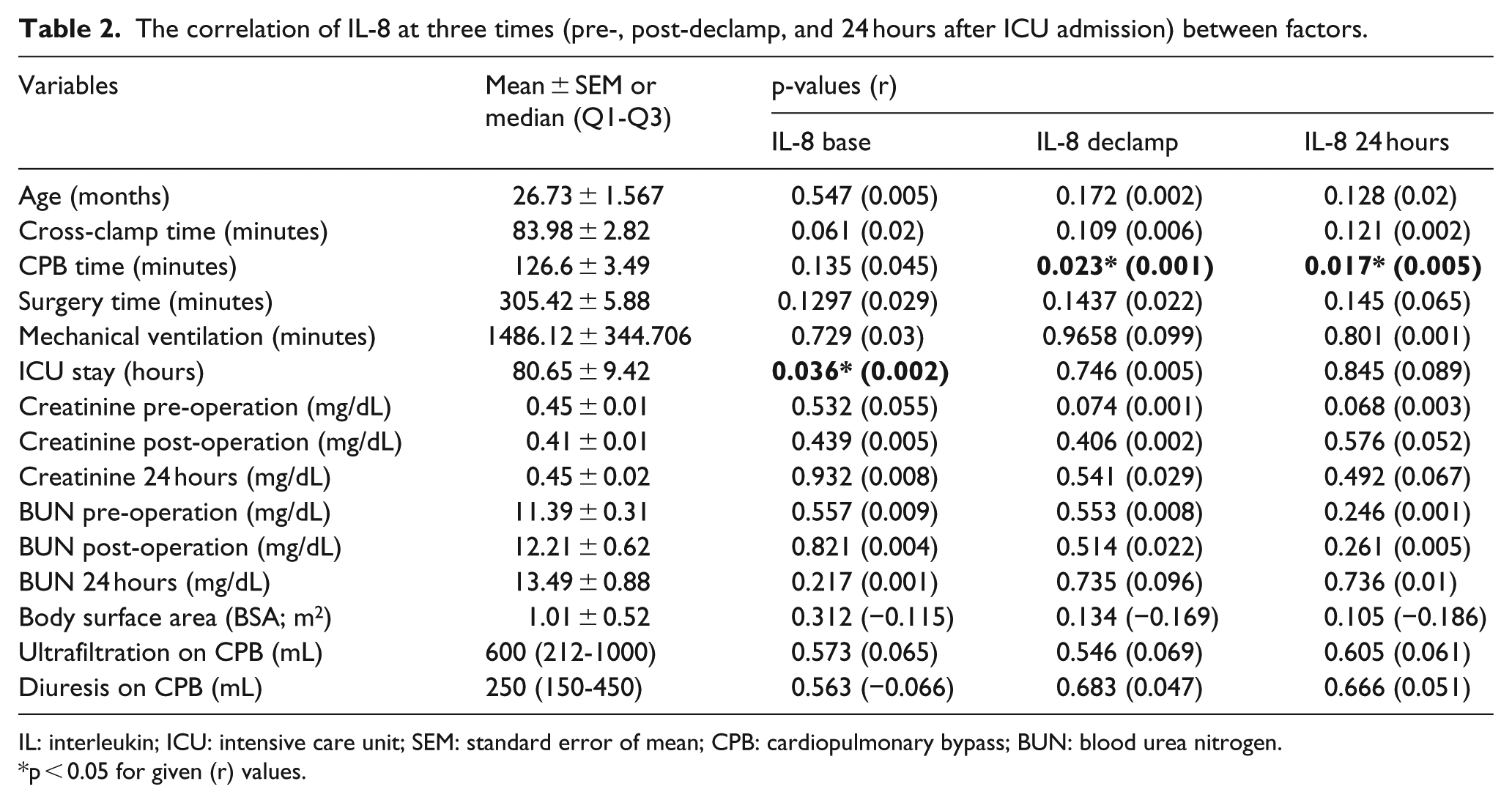
IL: interleukin; ICU: intensive care unit; SEM: standard error of mean; CPB: cardiopulmonary bypass; BUN: blood urea nitrogen.
*p < 0.05 for given (r) values.
This analysis was repeated for IL-10 and age (p > 0.05), cross-clamp time (p > 0.05), mechanical ventilation (p > 0.05), surgery time (p > 0.05), and ICU stay (p > 0.05) in correlated to all three times of creatinine and BUN (p > 0.05), ultrafiltration on CPB (p > 0.05), and diuresis on CPB (p > 0.05) in Table 3. However, we observed that there was significant relation between CPB time and IL-10 level on declamping time (p < 0.05).
The correlation of IL-10 at three times (pre-, post-declamp, and 24 hours after ICU admission) between factors.
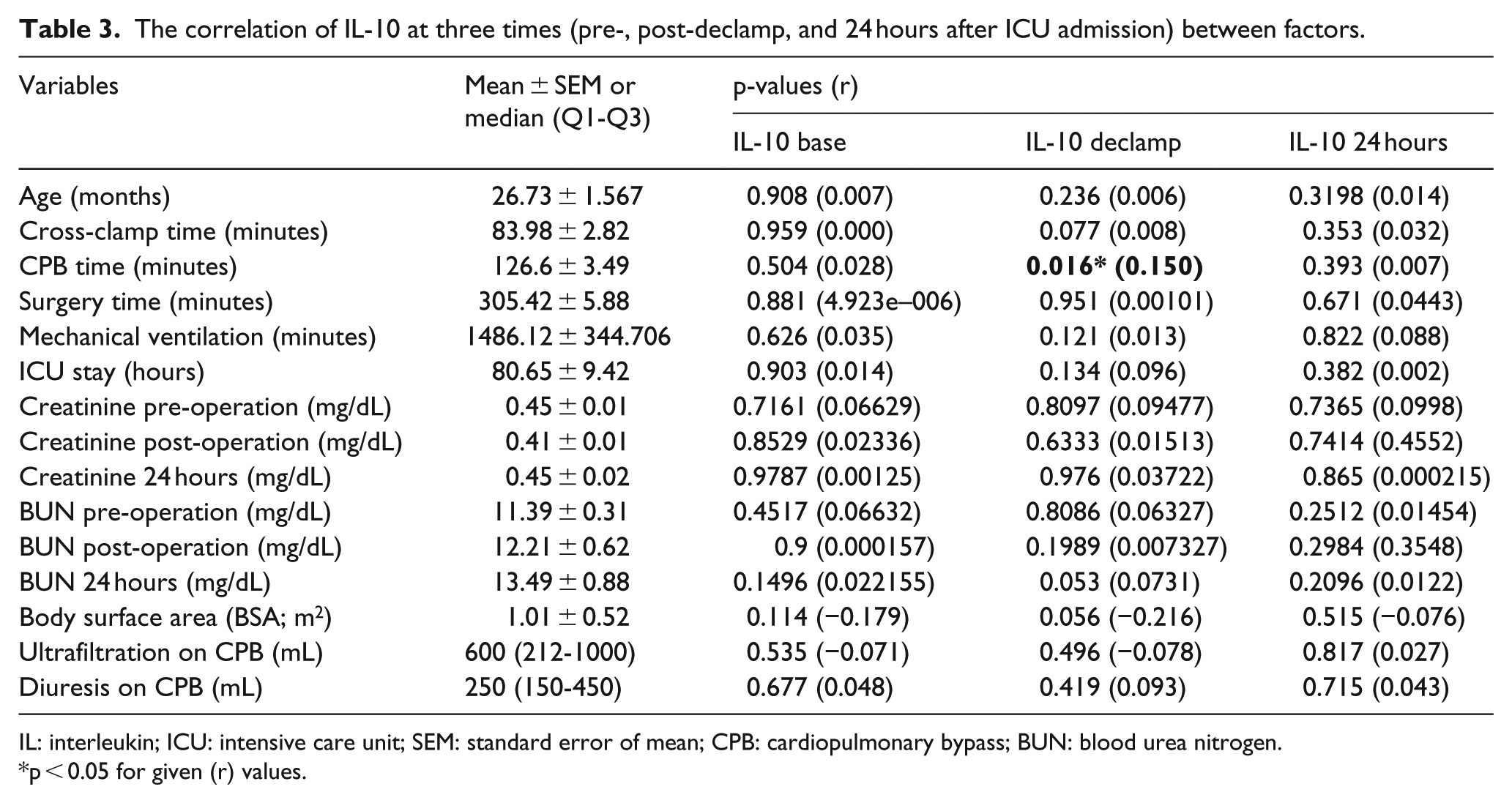
IL: interleukin; ICU: intensive care unit; SEM: standard error of mean; CPB: cardiopulmonary bypass; BUN: blood urea nitrogen.
*p < 0.05 for given (r) values.
Data obtained from correlation between TNF-α and age (p > 0.05), cross-clamp time (p > 0.05), CPB time (p > 0.05), surgery time (p > 0.05), and ICU stay (p > 0.05) in correlated to all three times of creatinine and BUN (p > 0.05), ultrafiltration on CPB (p > 0.05), and diuresis on CPB (p > 0.05) are briefly described in Table 4 and these parameters were not correlated. However, mechanical ventilation time was directly correlated with the TNF-α amounts in 24 hours after ICU admission (p < 0.05).
The correlation of TNF-α at three times (pre-, post-declamp, and 24 hours after ICU admission) between factors.
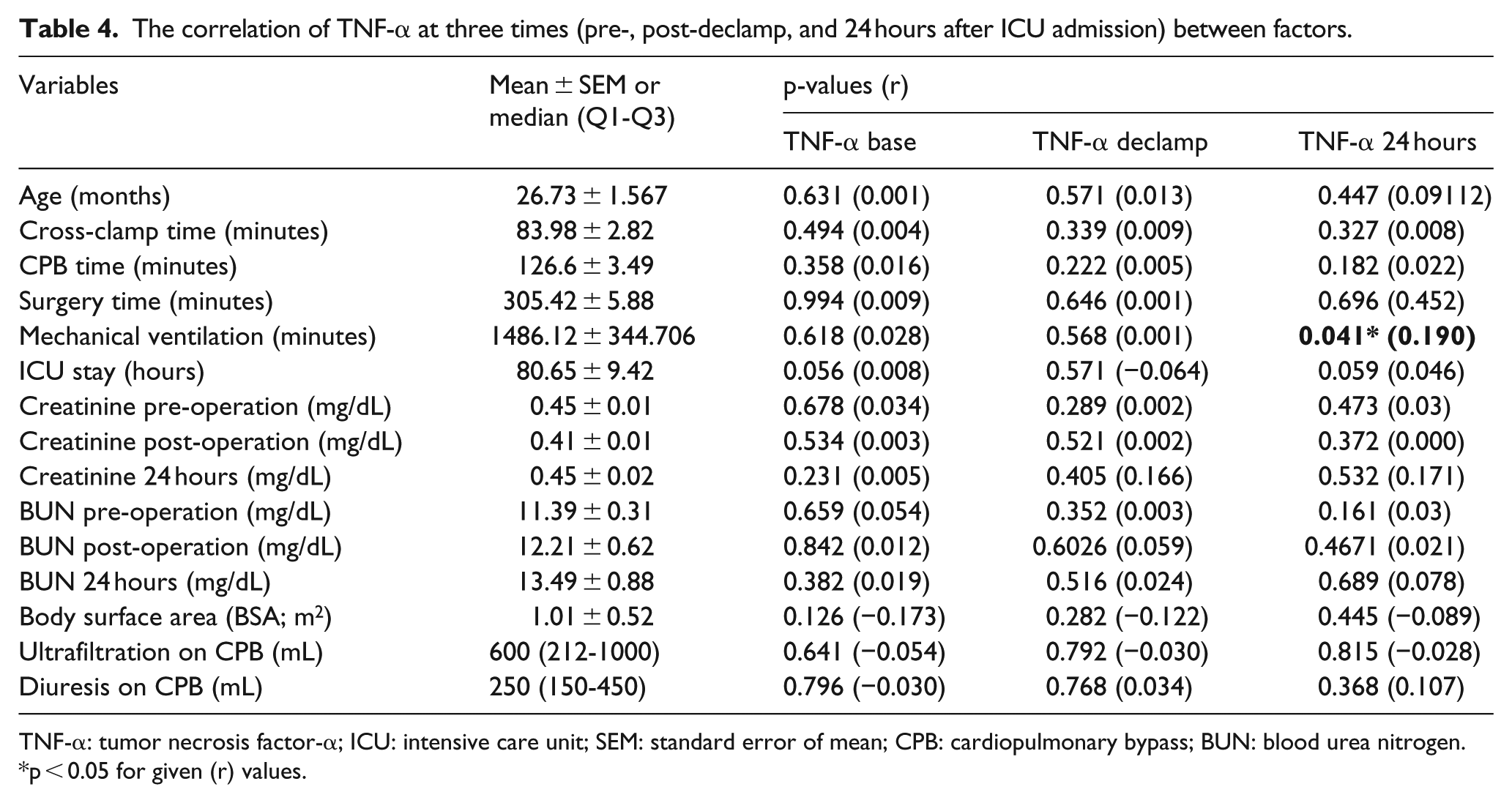
TNF-α: tumor necrosis factor-α; ICU: intensive care unit; SEM: standard error of mean; CPB: cardiopulmonary bypass; BUN: blood urea nitrogen.
*p < 0.05 for given (r) values.
Table 5 shows the rate of ARD according to serum creatinine; 85% of patients had no ARD, 6.25% mild ARD, 6.25% had moderate ARD, and 2.5% had severe ARD. Also, in this table, using Pearson chi-square, we tried to show the relation of multiple factors (after operation) with presentation of ARD. Analysis showed no relation between factors including IL-6, IL-8, IL-10, TNF-α, and BUN (p > 0.05).
The correlation between ARD groups, defined based on the changes in the circulatory creatinine, and the circulatory level of cytokines following operation.
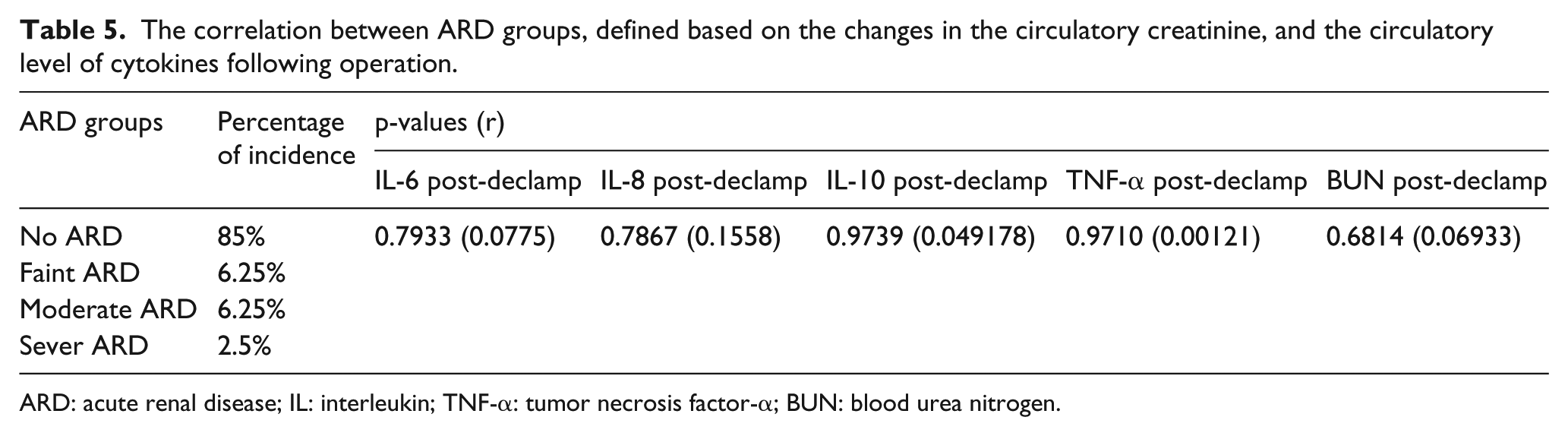
ARD: acute renal disease; IL: interleukin; TNF-α: tumor necrosis factor-α; BUN: blood urea nitrogen.
Discussion
In this study, we demonstrated relation between cytokines including IL-6, IL-8, IL-10, and TNF-α from one side, and CPB time, surgery time, and ICU stay from the other side. The circulatory levels of these cytokines regularly elevated after surgery and continued to remain high until 24 hours after the surgery. Therefore, they may offer a potential for the prognosis of post-surgical outcomes and also give an understanding of the pathogenesis of the related adverse outcomes. Beyond ischemia, reperfusion injury is a cause of myocardial damage consequent to surgery, which is related to raised cytokine response and increased tissue oxidative stress. 31
In the current study, we observed that the plasma levels of the IL-6, IL-8, IL-10, and TNF-α cytokines could correlate to CPB, mechanical ventilation, and ICU staying time. Also we investigated the relation between these cytokines and renal function. However, the analysis failed to show any significant correlation between these cytokines and plasma level of creatinine and BUN except for IL-6 at the declamp time. We found a direct correlation between IL-6 levels at 24 hours after ICU admission and mechanical ventilation time. This is presumably indicative of the adverse effects of the duration of mechanical ventilation time on inflammatory profile of the patients. Moreover, plasma IL-6 level after cross-clamp removal was directly correlated with the BUN level on ICU. This may hint a decrease in the renal function due to elevation of the IL-6 pro-inflammatory cytokine. According to the literature, pro-inflammatory cytokines could relate to the occurrence of adverse outcomes. For instance, pro-inflammatory cytokine IL-6 has been observed to be correlated with post-operative kidney dysfunction.32,33 Animal I/R paradigms demonstrated a key role of pro-inflammatory cytokines (IL-1b, IL-6, TNF-α) in the renal dysfunctions,34,35 particularly by increasing activation of the leukocytes and expressing intercellular adhesion molecule 1 (ICAM 1) adhesion molecule synthesis. TNF-α is associated with the development of glomerular injuries in the animal models.9,36 The most of the glomerulonephritis are correlated with monocytes and T lymphocyte infiltration. Increasing of the inflammatory cytokines that released from macrophages have been observed in the serum, and the urine of individual suffered from glomerulonephritis. It should be noted that IL-6 levels are related to the severity of the injuries. This evidence matched with past animal studies, illustrating the IL-6 as the proliferation factor for mesangial cells. 22 Another significant finding was the IL-6 level before incision and the diuresis volume during CPB. It appears that patients receiving higher amounts of volume expansion solutions have higher levels of IL-6 possibly. Since patients with higher levels of perioperative diuresis have probably received more infusions, they are presumably exposed to higher levels of infusion-related endotoxemia. 37
A weak direct correlation was observed between CPB time and the IL-8 levels at cross-clamp removal time and 24 hours after ICU admission. This reflects the fact that blood contact with non-physiological surfaces of the heart and lung machine and the related circuit is a major inflammation-inducing factor. 38 Moreover, IL-8 levels before incision is directly correlated with ICU stay in the study population.
In case of IL-10, only its circulatory level at the declamp time was found to be directly correlated with CPB time. Since elevation of the blood levels of IL-10 and other anti-inflammatory cytokines is a mechanism by which body responds to the inflammation, it is reasonable to presume that this elevation is a feedback to the elevation of inflammatory response and is responsible for the alleviation of the systemic inflammation. There are also evidence from in vivo preclinical studies confirming the correlation between these factors. Evidence from animal studies declared the effect of IL-10 in attenuating inflammation and renal failure of acute glomerulonephritis,33,39,40 cisplatin-induced nephrotoxicity,41–43 and ischemic damages.
TNF-α level at 24 hours after ICU admission was directly correlated with prolonged mechanical ventilation time. It has been reported that prolonged mechanical ventilation may have adverse effects on the lung and give rise to systemic inflammatory response due to stress and damage to the lung. Findings of the present study confirm this hypothesis. Also, the production of pro-inflammatory cytokines in the myocardium has been observed. Therefore, TNF-α seems like a main element of the post-ischemic myocardial dysfunction. During heart operation with CPB, the myocardium and its infiltrating lymphocytes are the main source of pro-inflammatory cytokines (TNF-α, IL-6, IL-8).22,23,28,44–47
Our findings also suggest that pro-inflammatory cytokines to be a consequence of the pre-operative variables and probable cause for alterations in the post-operative outcomes. For example, as observed in the current study, CPB duration is directly correlated with the circulatory level of IL-8 and IL-10 cytokines. On the other hand, there is a direct correlation between circulatory TNF-α and IL-6 cytokines levels 24 hours after operation and mechanical ventilation time. Also, results confirm that blood IL-8 levels following anesthesia induction is directly correlated with the duration of ICU stay. In sum, it appears that higher inflammation during and after operation is associated with adverse peri- and post-operative adverse outcomes.
In sum, findings of the current study illustrate the trends and correlates of the systemic inflammation in pediatrics undergoing CPB surgery and shed light on its association with a series of adverse events during this kind of operations. It highlights the importance of systemic inflammatory response during CPB in pediatrics and the necessity of prophylactic or therapeutic measures to prevent or alleviate it. Some of the prophylactic measures include reducing the use of transfusions, adequate cardioprotection through use of proper cardioplegic solutions, premedication with anti-inflammatory drugs, management strategies, such as hypothermia and early patient awakening to reduce the mechanical ventilation time, and the use of miniaturized circuits in CPB to reduce contact with non-self-non-physiological surfaces.3,48 Therapeutic strategies include those used to alleviate inflammation after it is induced. These comprise use of modified ultrafiltration (MUF) to remove cytokines, cytokine absorber, and anti-inflammatory post-medication such as corticoesteroids. 49
Conclusion
Higher level of circulatory pro-inflammatory cytokines is associated with adverse outcomes such as increased ICU stay and longer mechanical ventilation time in pediatric patients in CPB settings. It is also correlated with unfavorable biochemical parameter of renal function, BUN. Findings hint that proper control of the inflammatory response is vital for the control of unfavorable clinical and pathological outcomes in these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.