
Abstract
Background:
Renal failure is a common occurrence in patients with refractory cardiogenic shock including those supported with veno-arterial extracorporeal membrane oxygenation. Prevalence and outcome of acute and chronic kidney failure in extracorporeal membrane oxygenation patients have not been well documented. In this study, we investigated the occurrence of acute and chronic kidney failure in veno-arterial extracorporeal membrane oxygenation patients as well as predictors for survival.
Methods:
This is a single center retrospective clinical study. We included adult patients with refractory cardiogenic shock who were supported by veno-arterial extracorporeal membrane oxygenation between 2008 and 2015. The primary endpoint of the study was acute kidney injury (KDIGO Stage 3) during extracorporeal membrane oxygenation and chronic kidney failure requiring renal replacement therapy, 30 and 90 days after extracorporeal membrane oxygenation. The secondary endpoint was in-hospital survival and 90-day survival.
Results:
A total of 196 veno-arterial extracorporeal membrane oxygenation patients were investigated. In total, 41.8% (82/196) patients had acute renal failure requiring continuous renal replacement therapy during extracorporeal membrane oxygenation. The 30- and 90-day survival was 55.1% (108/196) and 48.5% (95/196), respectively; 21.3% (23/108) and 11.6% (11/95) patients needed renal replacement therapy after 30 and 90 days, respectively. Predictors for KDIGO Stage 3 renal failure during extracorporeal membrane oxygenation were lactate (p = 0.026) and the number of blood units transfused during extracorporeal membrane oxygenation support (p = 0.000). A predictor for renal replacement therapy after 30 and 90 days was an elevated plasma-free hemoglobin level. The in-hospital survival was 54.6% (107/196). Serum lactate of less than 4.3 mmol/L, lower age, plasma-free hemoglobin of ⩽62 mg/dL, low number of blood units transfused during extracorporeal membrane oxygenation, and the use of an intra-aortic balloon pump were predictors for in-hospital and 90-day survival.
Introduction
As more and more studies show increased survival benefits with the use of extracorporeal membrane oxygenation (ECMO) support and other extracorporeal life support (ECLS),1–3 it is important to understand that these modalities of therapy for cardiogenic shock and cardiac arrest also bring new variables to the complexity of assessing mortality and morbidity.
Renal failure is a frequent problem in patients with refractory cardiogenic shock including patients supported with veno-arterial extracorporeal membrane oxygenation (VA-ECMO).4–6 Acute kidney injury (AKI) requiring renal replacement therapy (RRT) in patients with ECMO is associated with a significantly lower survival 7 , 8 and also with failure to wean from ECMO. 9 Renal dysfunction generally may be caused by the hemodynamic alterations associated with the baseline disease or ECMO itself may contribute to kidney injury through several mechanisms. 10 Defining predictors of renal dysfunction in these patients may help elucidate possible adverse effects of ECMO on the kidney. Detailed data about predictors for renal failure in VA-ECMO patients are sparse. The aim of this study was to evaluate possible predictors for acute and chronic renal failure in patients supported with VA-ECMO.
Methods
Patients
A total of 196 patients who received VA-ECMO for refractory cardiogenic shock between June 2008 and December 2015 at our institution were included in this retrospective single center study. Cardiac surgical patients were only included if they could be weaned off from cardiopulmonary bypass (CPB) and had to be placed on ECMO later after already being transferred to the intensive care unit (ICU). Patient data were obtained through the electronic medical record chart review (Cerner Corporation, Kansas City, MO, USA).
Severe AKI (KDIGO Stage 3) is defined as a ⩾300% rise in serum creatinine from baseline, an increase in serum creatinine to ⩾4.0 mg/dL or initiation of RRT. 11 In our study, all patients who fulfilled the KDIGO criteria for Stage 3 were supported with continuous renal replacement therapy (CRRT).
The study has been reviewed by our institutional ethics committee. The file number of the ethical committee approval is “STUDY00002125.”
Outcome variables
The primary outcome variable was acute and chronic kidney failure, evaluated as CRRT during ECMO and need for renal replacement 30 and 90 days after ECMO. In-hospital survival and survival after 90 days were evaluated as secondary outcome.
Prespecified covariates included age, sex, body mass index (BMI), plasma-free hemoglobin levels, creatinine, serum lactate, hemoglobin, total bilirubin, number of blood units during ECMO, intra-aortic balloon pump (IABP), or Impella® as an additional intermediate heart device during ECMO. The baseline levels of creatinine, serum lactate, hemoglobin, and total bilirubin included in the study were collected either before or directly after ECMO cannulation. Values of plasma-free hemoglobin were checked twice daily during the entire ECMO run.
Statistical analyses
Results were reported as percentages for categorical variables, mean ± standard deviations for continuous variables that are evenly distributed, and/or medians and interquartile ranges (IQRs) for continuous variables that are unevenly distributed.
Categorical data were evaluated with Pearson’s χ2 test or with Fisher’s exact test.
Potential risk factors for survival and for kidney failure were analyzed with a univariate logistic regression. All continuous parameters were dichotomized at the 25th, 33rd, 50th, 66th, and 75th percentiles. The percentile value with the lowest p value was then used in the logistic regression. Multivariate logistic regression was performed with all predictors in which the univariate regression showed a p value of less than 0.05. All data were analyzed using SPSS, version 25.0 (IBM, Armonk, NY, USA). Statistical significance was defined as two-tailed p < 0.05.
ECMO circuit
ECMO circuits that were used consisted of a Quadrox oxygenator (Maquet Cardiovascular, Wayne, NJ, USA) and either a Rotaflow centrifugal pump (Maquet Cardiovascular) or a CentriMag centrifugal pump (Thoratec, Pleasanton, CA, USA). Both circuits were heparin coated. Except in patients where ECMO was placed under cardiopulmonary resuscitation (ECPR), a Swan–Ganz catheter was placed prior to ECMO cannulation. ECMO cannulation was considered in case of refractory cardiogenic shock with a cardiac index of less than 2.2 L/min/m2 despite support with two inotropes and signs of end-organ hypoperfusion (elevated serum lactate, low urine output, and ischemic hepatitis) and/or the presence of prolonged hypotension (systolic blood pressure <90 mm Hg or mean arterial pressure (MAP) <65 mm Hg).
Attending intensivists or attending cardiac surgeons performed ECMO placement. Patient or power of attorney was informed about the procedure and gave consent. Informed consent was waived only if patients’ capacity for consent was limited and the power of attorney was not accessible due to time limitation. In most of the patients, the ECMO was placed percutaneously by the intensivist. A distal perfusion cannula was placed routinely in the femoral artery. Weaning from ECMO was performed in patients who fulfilled our published institutional weaning criteria and passed an ECMO weaning trial consisting of decreasing and clamping ECMO flow while measuring cardiac output, cardiac index, MAP, and central venous pressure (CVP) and performing an echocardiography with measurement of the velocity time integral (VTI) and left ventricular ejection fraction (LVEF). 12
In case patients were supported with IABP before ECMO, the balloon pump was explanted either during ECMO implantation or during the first 24 hours after ECMO implantation (see below).
Blood units were transfused in case of low-flow of the ECMO circuit if the hemoglobin level was less than 10 mg/dL and in patients with stable hemodynamics if the hemoglobin was lower than 7-8 mg/dL.
Results
Study population
In total, 196 patients with VA-ECMO support were enrolled in this study (mean age: 56.7 years; standard deviation (SD): ±13.9 years; 69% male) and were evaluated for acute and chronic kidney failure and for in-hospital survival and mid-term survival (90 days). Patient’s characteristics at admission to our ICU are given in Table 1.
Characteristics of patients with VA-ECMO support after refractory cardiogenic shock (n = 196).
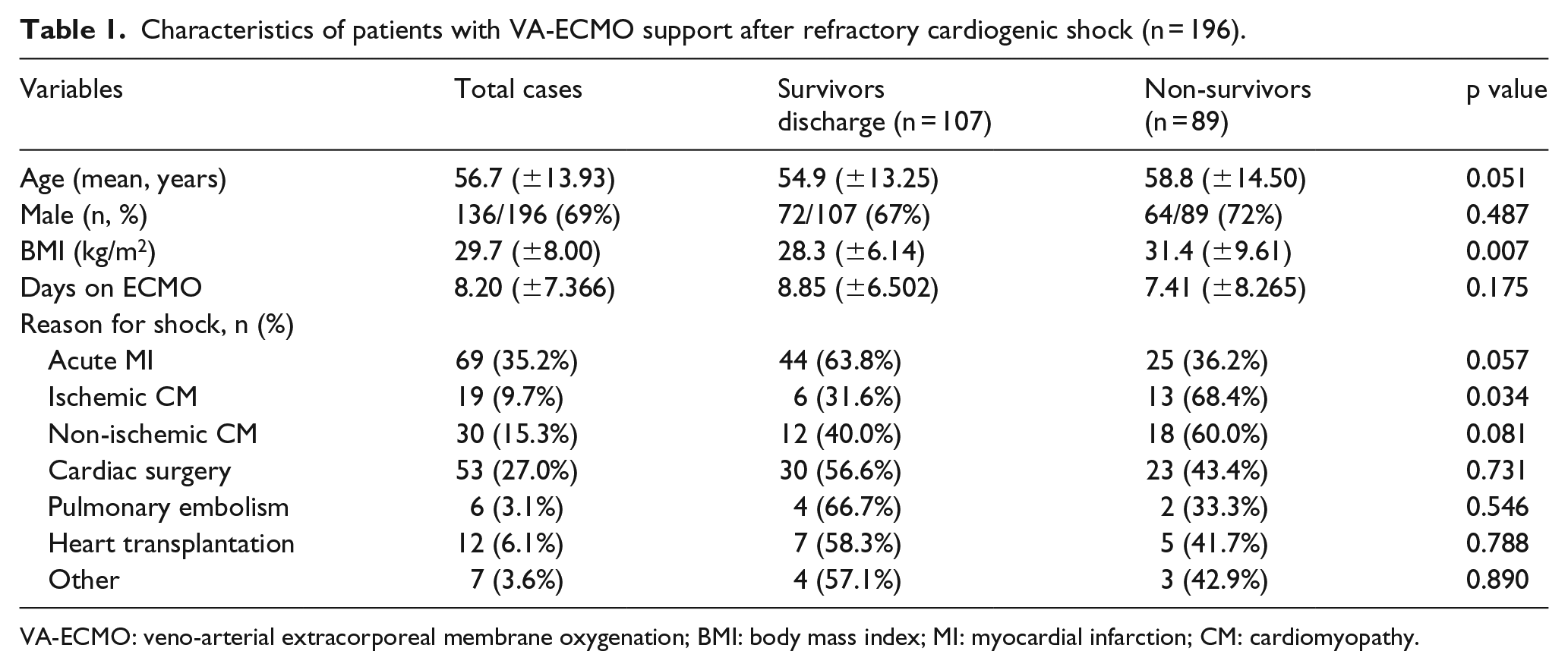
VA-ECMO: veno-arterial extracorporeal membrane oxygenation; BMI: body mass index; MI: myocardial infarction; CM: cardiomyopathy.
Patients’ outcomes
In-hospital survival and survival rate after 90 days were 54.6% (107/196) and 48.5% (95/196), respectively. Significant variables for in-hospital and 90-day survival were age ⩽65 years, initial lactate level less than 4.3 mmol/L, plasma-free hemoglobin less than 62 mg/dL, transfusion of less than 8 units of blood as well as the usage of an IABP before ECMO. Table 2 shows predictors for in-hospital and 90-day survival. The 30-day survival (55.1% (108/196)) was slightly different to the in-hospital survival.
Predictors for in-hospital and 90-day survival for patients on VA-ECMO.
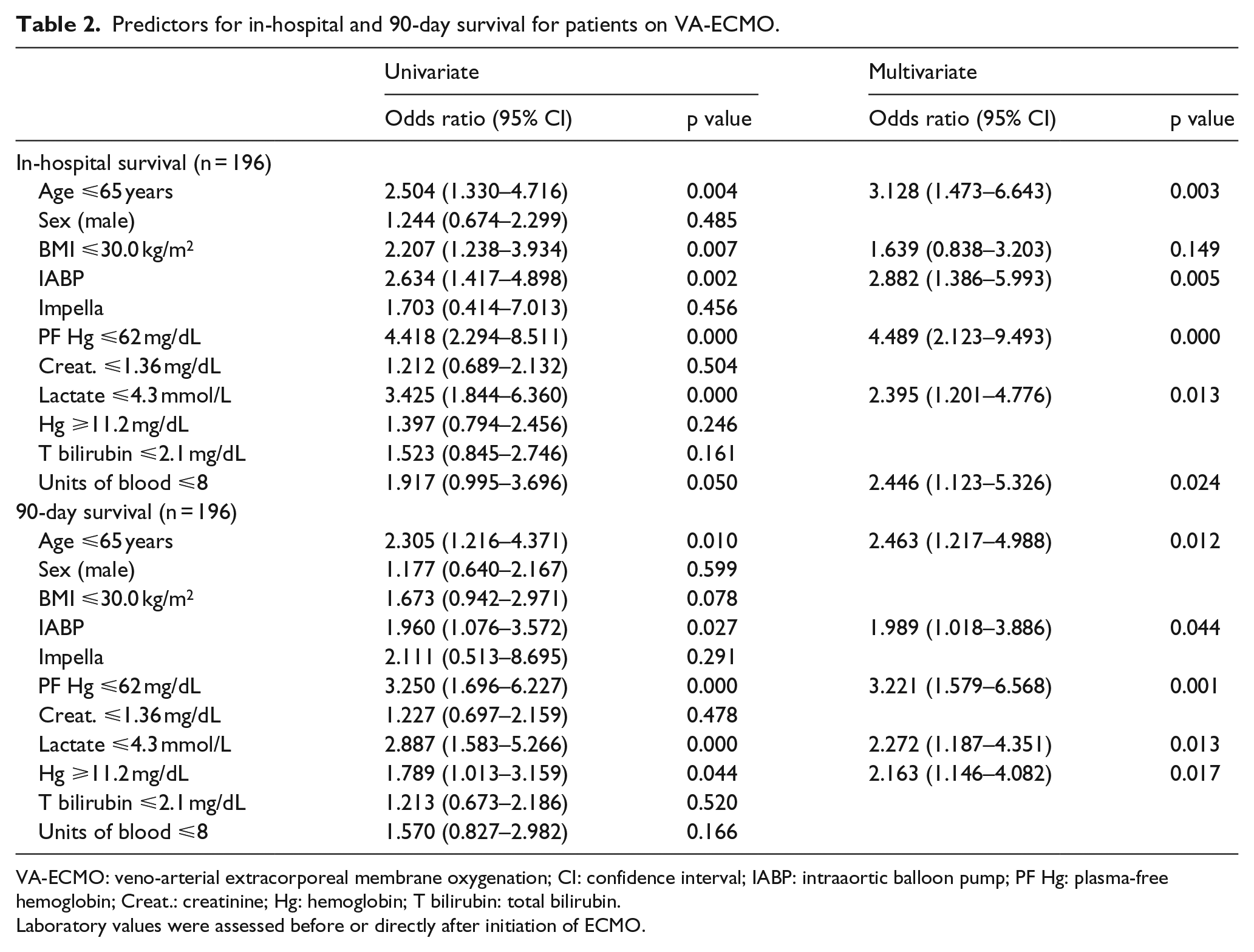
VA-ECMO: veno-arterial extracorporeal membrane oxygenation; CI: confidence interval; IABP: intraaortic balloon pump; PF Hg: plasma-free hemoglobin; Creat.: creatinine; Hg: hemoglobin; T bilirubin: total bilirubin.
Laboratory values were assessed before or directly after initiation of ECMO.
A total of 82 patients (41.8%) had an AKI (KDIGO Stage 3). In this cohort, every patient with AKI KDIGO Stage 3 was treated with CRRT. Twenty-three (21.3%) of the 108 patients who survived 30 days were on RRT 30 days after ECMO. Eleven (11.6%) of the 95 patients who survived 90 days required renal replacement therapy at this time. Significant predictors for acute renal failure and RRT requiring renal failure after 30 days were plasma-free hemoglobin levels and the number of blood units needed during ECMO. Plasma-free hemoglobin level was also a predictor for chronic kidney failure (requiring RRT) after 90 days. Table 3 shows the results of the multiregression analysis.
Predictors for acute renal failure in patients on VA-ECMO, for renal failure 30 days after VA-ECMO, for renal failure 90 days after VA-ECMO.
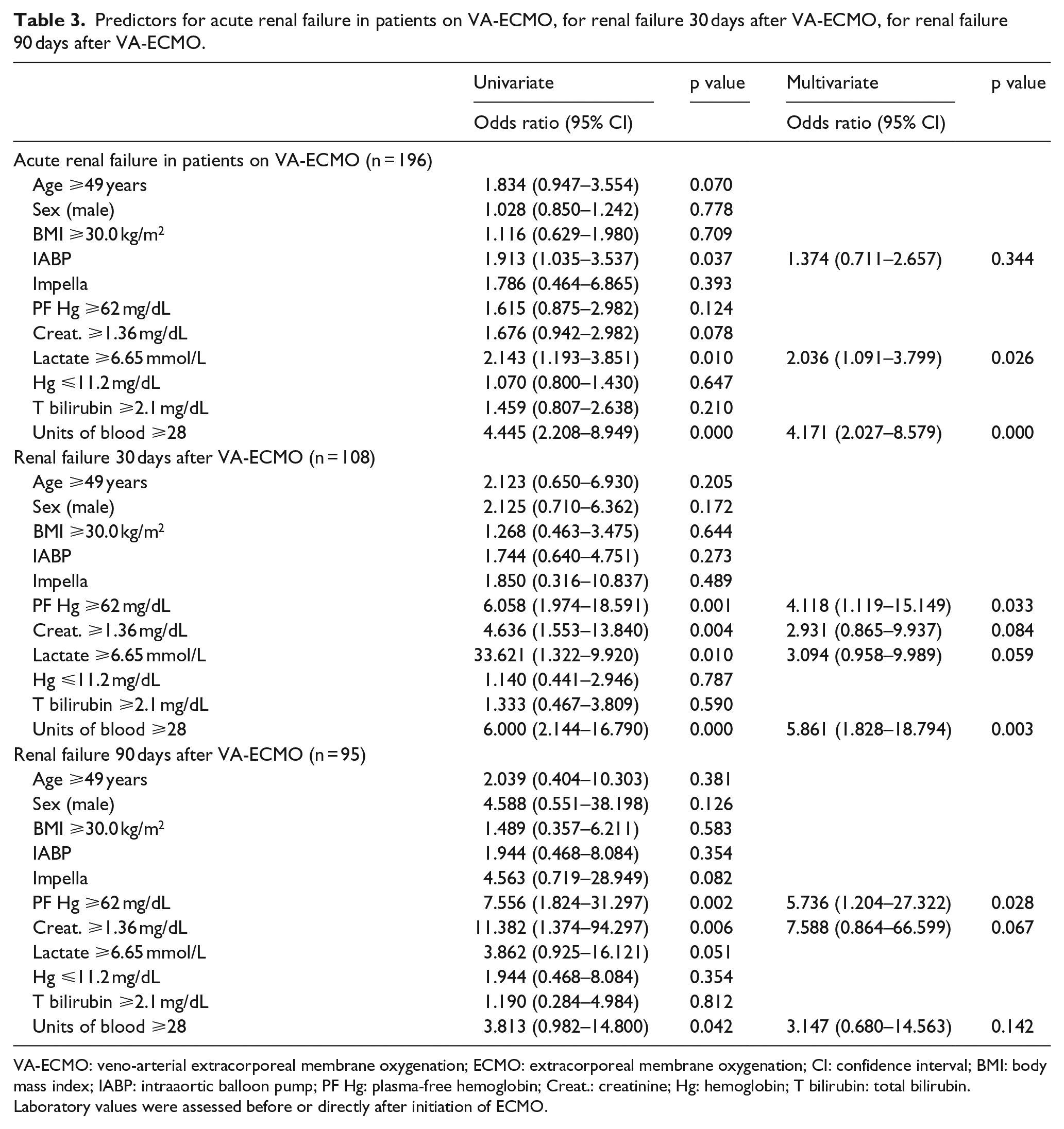
VA-ECMO: veno-arterial extracorporeal membrane oxygenation; ECMO: extracorporeal membrane oxygenation; CI: confidence interval; BMI: body mass index; IABP: intraaortic balloon pump; PF Hg: plasma-free hemoglobin; Creat.: creatinine; Hg: hemoglobin; T bilirubin: total bilirubin.
Laboratory values were assessed before or directly after initiation of ECMO.
Additional support devices
In total, 69 (35.2%) patients were supported with IABP before ECMO implantation. In 38 patients, IABP was removed at the time of ECMO implantation. In 31 patients, the balloon pump was withdrawn during the first 24 hours after ECMO implantation.
In nine cases (4.6%) the patients were supported with an Impella before ECMO implantation. In each of these cases, the Impella was removed during ECMO implantation. In two cases, an Impella was used as an additional device during ECMO to unload the left ventricle.
Discussion
Published reports on predictors of renal failure in ECMO patients are sparse. In our patient population, we found an acute kidney failure rate during VA-ECMO support of 41.8%, which is comparable with the reported rate of 43-52% in other publications.13–15 Possible etiologies for renal failure in ECMO patients include multiple pathophysiological mechanisms which chiefly lead to a reduction in renal oxygen delivery and/or to inflammatory damage. These mechanisms are generally a combination of causes due to patient-related variables as well as hemodynamic alterations associated with the baseline disease and the ECMO circuit. 10 In the context of these potential mechanisms we have chosen prespecified covariates for (1) patient characteristics including age, gender, and BMI, (2) disease-related parameters for hemolysis, anemia, red blood cell (RBC) transfusion, organic failure including prior elevated creatinine level, and (3) additional intermediate heart devices like IABP and Impella.
Predictors for renal failure
An extracorporeal circuit exposes blood to non-physiological surfaces and mechanical stress. This can result in activation of several enzyme cascades and lysis of RBCs. A combination of these events can cause the formation of reactive forms of oxygen such as hydrogen peroxide (H2O2). Hydrogen peroxide can react with hemoglobin to release redox active forms of iron which has the potential to be cytotoxic and may contribute to renal failure. 16 , 17 Hemolysis, documented by elevated level of plasma-free hemoglobin, was a predictor for chronic kidney disease in our cohort.
The number of RBC transfusion was significantly higher in patients with acute kidney failure. Interestingly it could not be found as a predictor for chronic renal failure. Intra- and perioperative blood product transfusions are independently associated with an increased risk of postoperative AKI in cardiac surgery patients.18–20 In general, two possible explanations for the impact of RBC transfusion on renal failure are conceivable: First, blood transfusion can increase hemolysis, caused by immunologic reaction due to different kinds of immunologic incompatibility between donor and recipient cell types. 21 Hemolysis can lead to significant renal sequelae. Lyu et al. 22 found an association between the hemolysis marker, plasma-free hemoglobin level, and acute renal failure during VA-ECMO support in a cohort of 84 patients. We also saw a significant elevated plasma-free hemoglobin level in patients with chronic kidney failure in our cohort. Second, erythrocytes undergo irreversible biochemical changes during storage and as a result can promote a pro-inflammatory state after transfusion. This can cause exacerbate tissue oxidative stress which in turn can cause AKI. 18 This was also described in patients undergoing cardiac surgery with CPB. 20 , 22 In our study, 53 (27.0%) patients were included who had cardiac surgery prior to ECMO placement. Cardiac surgery patients were only included in the study if they could be weaned off from CPB. There was neither a significant difference in the number of blood units received during ECMO nor any significant difference in kidney injury or mortality between the surgery patients and non-surgical patients in our study.
Lactate was a variable which showed to be a significant predictor for acute renal failure, but not for chronic kidney disease (30 and 90 days after ECMO). An elevated lactate as a parameter for end organ perfusion was expected to be a predictor for renal failure. The kidney is one of the most sensitive organs in case of malperfusion. 23
In the univariate analysis, an initially significant elevated creatinine prior to ECMO could be seen in our patients which later developed a chronic kidney injury but not in patients with AKI under ECMO treatment. The impact of a moderate elevated creatinine and therefore of less-severe kidney failure (KDIGO Stages 1 and 2) prior to ECMO might not have the same importance than for kidney recovery directly after the cardiogenic shock in the “post-acute stage” as for the long-term recovery of the kidney. However, the significance of the univariate analysis for lactate could not be confirmed in the multivariate analysis.
Predictors for survival
We found an in-hospital survival in our patient cohort of 54.6%, which was higher than the reported Extracorporeal Life Support Organization (ELSO) data 24 for VA-ECMO. In our cohort, 47 patients (24.0%) had ECMO placement during ECPR. The survival in patients with ECPR is known to be significantly lower than in other VA-ECMO patients. 3 ,25–27 A lower lactate level and lower age were predictors for survival after both, discharge and 90-day survival. Also in other studies, 28 , 29 lower lactate and age were reported as predictors for survival. We found an initial lactate value of more than 4.3 mmol/L being significant for higher mortality. The significant limit for age was 65 years for in-hospital survival and 90-day survival.
Hemolysis, documented by elevated plasma-free hemoglobin level, and transfusions of RBCs increased the mortality in our study. Omar et al. 13 also reported a high plasma-free hemoglobin level as a predictor for 90-day mortality. High levels of plasma-free hemoglobin lead to depletion of nitric oxide (NO) 30 , 31 and therefore can lead to increased systemic and pulmonary vascular resistance, increased thrombin formation, fibrin deposition, platelet aggregation, and finally can contribute to organ dysfunction and increased mortality. Furthermore, the released iron (Fe) from hemolysis can result in an overload of redox active iron leading to renal failure. 16 , 17
We found a significantly higher in-hospital survival and 90-day survival in patients supported with IABP, regardless if the IABP was directly explanted during ECMO implantation or if the ballon pump was continued for some time during the first 24 hours after ECMO implantation. The benefit of using IABP is discussed controversially. IABP did not confer any survival benefit in patients with cardiogenic shock complicating myocardial infarction. 32 A retrospective cohort study from the nationwide Japanese Diagnosis Procedure Combination national inpatient database investigated the impact of a combination support with IABP and VA-ECMO. In total, 1650 cardiogenic shock patients were divided into a group with IABP/VA-ECMO support and a group of VA-ECMO support alone. The 28-day mortality and in-hospital mortality in the IABP/VA-ECMO group was significantly lower. 33 It is conceivable that a combination support of IABP and ECMO may be of benefit. However, randomized controlled studies are required to confirm this mortality reducing effect of a combination support.
Transfusion of RBC during ECMO was found to be a predictor for mortality. Administration of packed RBCs especially to patients undergoing cardiac surgery was also associated with an increased mortality in other studies. 18 The mortality in our study was irrespective of prior cardiac surgery.
Limitations
The study is a single center study with limited numbers. Further limitation is the retrospective nature of the study. Although we excluded surgical patients who could not be weaned off from CPB directly after cardiac surgery, the cohort persists of both, cardiac surgery and non-cardiac surgery patients with refractory cardiogenic shock. However, we did not see a significant difference between cardiac surgery and non-cardiac surgery patients regarding kidney failure and survival.
Frequency and duration of significant hypotension before and during ECMO might play an additional role regarding development of kidney failure. In this study, all patients went on ECMO due to refractory cardiogenic shock often including significant low blood pressure. During ECMO treatment, patients were mostly managed to have a MAP of more than 65 mm Hg. However, the collected data set could not provide enough information about the exact duration of significant hypotension before and during ECMO which is an additional limitation in this study.
Conclusion
Elevated serum lactate and the amount of RBC transfusions were found to be predictors for AKI after VA-ECMO implantation while an elevated plasma-free hemoglobin level during ECMO was found to be a predictor for chronic renal failure.
Higher age, increased lactate, plasma-free hemoglobin levels, and the number of blood units could be confirmed as being predictors for mortality. The use of IABP was a predictor for survival in our VA-ECMO cohort.
Footnotes
Acknowledgements
This work was performed by the Heart and Vascular Institute of the Penn State Milton S. Hershey Medical Center (PA, USA).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.